
Association between Social Integration, Social Exclusion, and Vaccination Behavior among Internal Migrants in China: A Cross-Sectional Study



Abstract
:1. Introduction
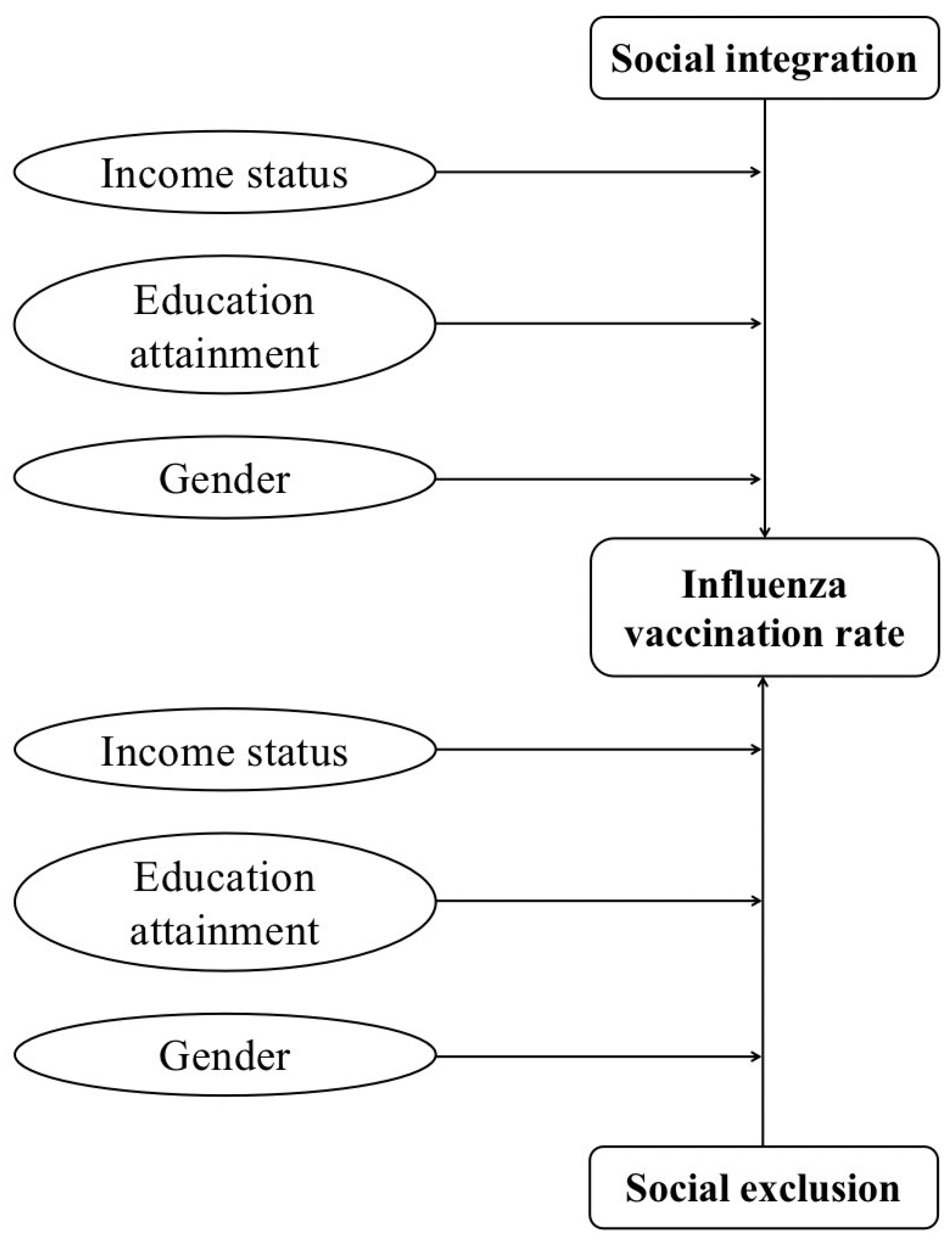
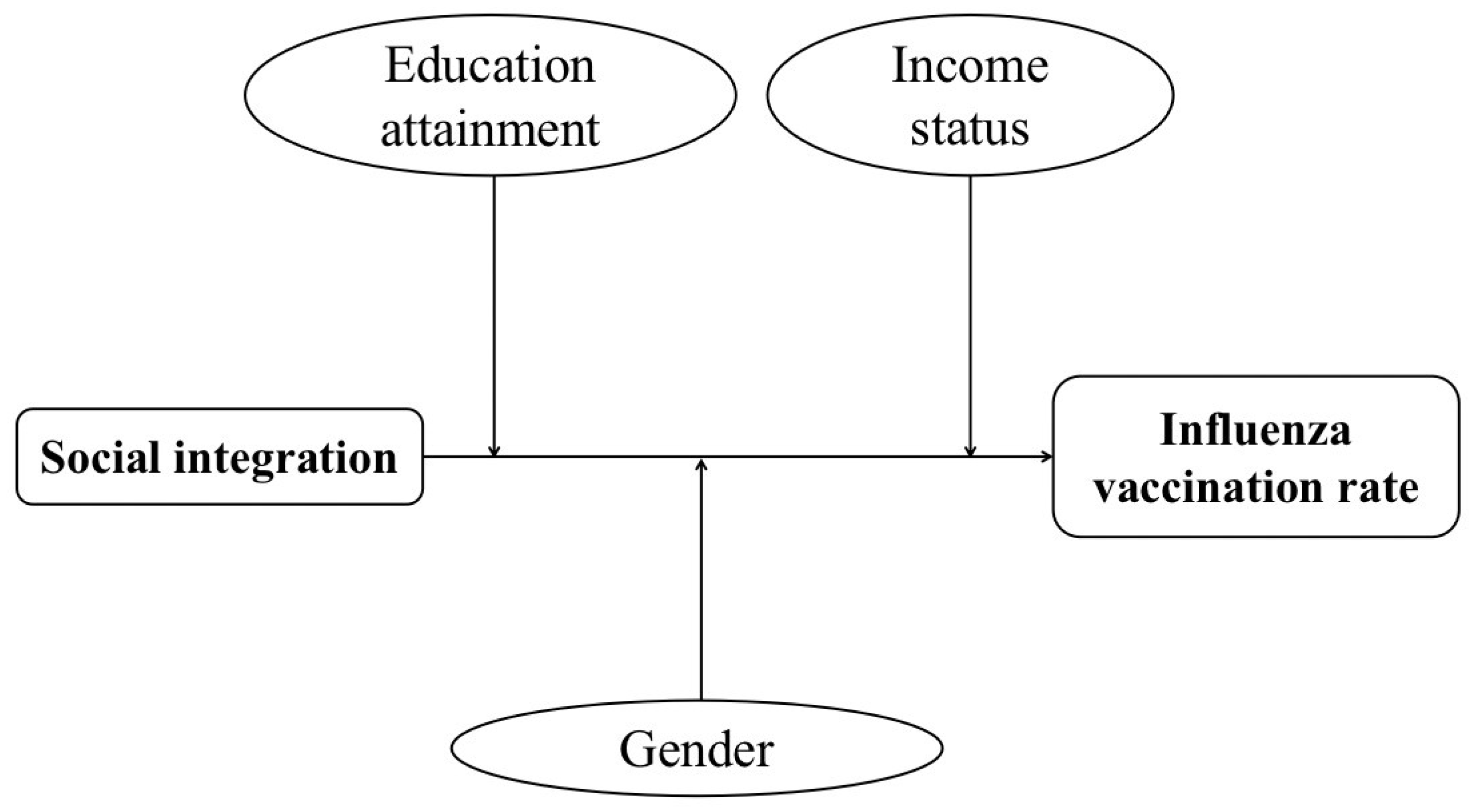
2. Conceptual Framework and Hypotheses
3. Materials and Methods
3.1. Sample
3.2. Measures
3.2.1. Influenza Vaccination Rate
3.2.2. Social Integration
3.2.3. Social Exclusion
3.2.4. Demographic Characteristics
3.2.5. Socioeconomic Characteristics
3.2.6. Health Characteristics
3.3. Statistical Analysis
4. Results
4.1. Basic Characteristics of the Respondents
4.2. The Association between Social Integration, Social Exclusion, and Influenza Vaccination Rate
4.2.1. Social Integration and Influenza Vaccination Rate
4.2.2. Social Exclusion and Influenza Vaccination Rate
4.2.3. Interactions and Influenza Vaccination Rate
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, J.; Zhu, J.; Wang, X.; Che, Y.; Bai, Y.; Liu, J. Sociodemographic disparities in the establishment of health records among 0.5 million migrants from 2014 to 2017 in China: A nationwide cross-sectional study. Int. J. Equity Health 2021, 20, 250. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Zhang, Q.; Chen, W.; Shi, J.; Han, S.; Song, X.; Xu, Y.; Ling, L. Association between social integration and health among internal migrants in ZhongShan, China. PLoS ONE 2016, 11, e0148397. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Zhang, Q.; Chen, W.; Ling, L. The social income inequality, social integration and health status of internal migrants in China. Int. J. Equity Health 2017, 16, 139. [Google Scholar] [CrossRef]
- Fang, H.; Yang, L.; Zhang, H.; Li, C.; Wen, L.; Sun, L.; Hanson, K.; Meng, Q. Strengthening health system to improve immunization for migrants in China. Int. J. Equity Health 2017, 16, 19. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.Y.; Matchar, D.B.; Clements, D.A.; Huber, J.; Hamilton, J.D.; Peterson, E.D. Economic analysis of influenza vaccination and antiviral treatment for healthy working adults. Ann. Intern. Med. 2002, 137, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Streefland, P.H. Public doubts about vaccination safety and resistance against vaccination. Health Policy 2001, 55, 159–172. [Google Scholar] [CrossRef]
- Tsutsui, Y.; Benzion, U.; Shahrabani, S.; Din, G.Y. A policy to promote influenza vaccination: A behavioral economic approach. Health Policy 2010, 97, 238–249. [Google Scholar] [CrossRef]
- Le, P.; Rothberg, M.B. Limited Focus in Evaluation of Vaccine Cost-effectiveness-Reply. JAMA Int. Med. 2018, 178, 1564. [Google Scholar] [CrossRef]
- Stockwell, M.S.; Fiks, A.G. Utilizing health information technology to improve vaccine communication and coverage. Hum. Vaccines Immunother. 2013, 9, 1802–1811. [Google Scholar] [CrossRef] [Green Version]
- Leidner, A.J.; Murthy, N.; Chesson, H.W.; Biggerstaff, M.; Stoecker, C.; Harris, A.M.; Acosta, A.; Dooling, K.; Bridges, C.B. Cost-effectiveness of adult vaccinations: A systematic review. Vaccine 2019, 37, 226–234. [Google Scholar] [CrossRef]
- Wang, Q.; Yue, N.; Zheng, M.; Wang, D.; Duan, C.; Yu, X.; Zhang, X.; Bao, C.; Jin, H. Influenza vaccination coverage of population and the factors influencing influenza vaccination in mainland China: A meta-analysis. Vaccine 2018, 36, 7262–7269. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Atkins, K.E.; Feng, L.; Pang, M.; Zheng, Y.; Liu, X.; Cowling, B.J.; Yu, H. Seasonal influenza vaccination in China: Landscape of diverse regional reimbursement policy, and budget impact analysis. Vaccine 2016, 34, 5724–5735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Atkins, K.E.; Feng, L.; Baguelin, M.; Wu, P.; Yan, H.; Lau, E.; Wu, J.T.K.; Liu, Y.; Cowling, B.J.; et al. Cost-effectiveness of introducing national seasonal influenza vaccination for adults aged 60 years and above in mainland China: A modelling analysis. BMC Med. 2020, 18, 90. [Google Scholar] [CrossRef] [PubMed]
- McQuestion, M.J.; Quijano Calle, A.; Drasbek, C.; Harkins, T.; Sagastume, L.J. Social integration and health behavioral change in San Luis, Honduras. Health Educ. Behav. 2010, 37, 694–708. [Google Scholar] [CrossRef] [PubMed]
- Uchino, B.N.; Landvatter, J.; Zee, K.; Bolger, N. Social Support and Antibody Responses to Vaccination: A Meta-Analysis. Ann. Behav. Med. 2020, 54, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Huang, Y.; Zhang, W. Residential segregation and perceptions of social integration in Shanghai, China. Urban. Stud. 2017, 55, 1484–1503. [Google Scholar] [CrossRef]
- Qin, L.; Chen, C.P.; Wang, W.; Chen, H. How migrants get integrated in urban China-The impact of health insurance. Soc. Sci. Med. 2021, 272, 113700. [Google Scholar] [CrossRef]
- O’Reilly, C.A.; Caldwell, D.F.; Barnett, W.P. Work Group Demography, Social Integration, and Turnover. Adm. Sci. Q. 1989, 34, 21–37. [Google Scholar]
- Zhou, J.; Zhou, J.; Zhang, H.; Zhang, J. Social Integration as Mediator and Age as Moderator in Social Capital Affecting Mental Health of Internal Migrant Workers: A Multi-Group Structural Equation Modeling Approach. Front. Public Health 2022, 10, 865061. [Google Scholar] [CrossRef]
- Ware, N.C.; Hopper, K.; Tugenberg, T.; Dickey, B.; Fisher, D. Connectedness and citizenship: Redefining social integration. Psychiatr. Serv. 2007, 58, 469–474. [Google Scholar] [CrossRef]
- Berkman, L.F.; Glass, T.; Brissette, I.; Seeman, T.E. From social integration to health: Durkheim in the new millennium. Soc. Sci. Med. 2000, 51, 843–857. [Google Scholar] [CrossRef]
- Li, T.C.; Chu, C.C.; Meng, F.C.; Li, Q.; Mo, D.; Li, B.; Tsai, S.-B. Will Happiness Improve the Psychological Integration of Migrant Workers? Int. J. Environ. Res. Public Health 2018, 15, 900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apospori, E.; Millar, J. The Dynamics of Social Exclusion in Europe; Edward Elgar Publications: London, UK, 2003. [Google Scholar]
- Atkinson, A.B. Social exclusion, poverty and unemployment. In Exclusion, Employment and Opportunity; Atkinson, A.B., Hills, J., Eds.; CASE Paper Number 4; Centre for Analysis of Social Exclusion: London, UK, 1998. [Google Scholar]
- Pantazis, C.; Gordon, D.; Levitas, R. Poverty and Social Exclusion in Britain. Bristol Policy Press 2006, 1, 6. [Google Scholar]
- Feng, Z.; Jones, K.; Phillips, D.R. Social exclusion, self-rated health and depression among older people in China: Evidence from a national survey of older persons. Arch. Gerontol. Geriatr. 2019, 82, 238–244. [Google Scholar] [CrossRef]
- Sacker, A.; Ross, A.; MacLeod, C.A.; Netuveli, G.; Windle, G. Health and social exclusion in older age: Evidence from Understanding Society, the UK household longitudinal study. J. Epidemiol. Commun. Health 2017, 71, 681–690. [Google Scholar] [CrossRef]
- Weyers, S.; Dragano, N.; Möbus, S.; Beck, E.M.; Stang, A.; Möhlenkamp, S.; Jöckel, K.H.; Erbel, R.; Siegrist, J. Poor social relations and adverse health behaviour: Stronger associations in low socioeconomic groups? Int. J. Public Health 2010, 55, 17–23. [Google Scholar] [CrossRef]
- He, J.; He, L.; Zhou, W.; Nie, X.; He, M. Discrimination and Social Exclusion in the Outbreak of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 2933. [Google Scholar] [CrossRef] [Green Version]
- Grossman, M. The Demand for Health-A Theoretical and Empirical Investigation; National Bureau of Economic Research: New York, NY, USA, 1972. [Google Scholar]
- Grossman, M. On the Concept of Health Capital and the Demand for Health. J. Political Econ. 1972, 80, 223–255. [Google Scholar] [CrossRef] [Green Version]
- Grossman, M. The Human Capital Model. In Handbook of Health Economics; JP Newhouse: Amsterdam, The Netherlands, 2000; Volume 1, pp. 347–408. [Google Scholar]
- Toyama, M.; Fuller, H.R.; Owino, J. Longitudinal Implications of Social Integration for Age and Gender Differences in Late-Life Physical Functioning. Int. J. Aging Hum. Dev. 2022, 94, 169–192. [Google Scholar] [CrossRef]
- Dahlberg, L.; McKee, K.J.; Fritzell, J.; Heap, J.; Lennartsson, C. Trends and gender associations in social exclusion in older adults in Sweden over two decades. Arch. Gerontol. Geriatr. 2020, 89, 104032. [Google Scholar] [CrossRef]
- Jo, E.B.; Kwon, R.H.; Jung, M. Contextual effects of social integration and disintegration on health status: Evidence from South Korea. BMC Public Health 2020, 20, 940. [Google Scholar] [CrossRef] [PubMed]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef] [PubMed]
- Mamelund, S.E.; Shelley-Egan, C.; Rogeberg, O. The association between socioeconomic status and pandemic influenza: Protocol for a systematic review and meta-analysis. Syst. Rev. 2019, 8, 5. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior-A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Zhu, Z.; Guo, M.; Petrovsky, D.V.; Dong, T.; Hu, Y.; Wu, B. Age and regional disparity in HIV education among migrants in China: Migrants population dynamic monitoring survey, 2014-2015. Int. J. Equity Health 2019, 18, 104. [Google Scholar] [CrossRef] [Green Version]
- Nie, P.; Ma, W.; Sousa-Poza, A. The relationship between smartphone use and subjective well-being in rural China. Electron. Commer. Res. 2021, 21, 983–1009. [Google Scholar] [CrossRef]
- Olson, J.A.; Sandra, D.A.; Colucci, É.S.; Al Bikaii, A.; Chmoulevitch, D.; Nahas, J.; Veissière, S.P. Smartphone addiction is increasing across the world: A meta-analysis of 24 countries. Comput. Hum. Behav. 2022, 129, 107138. [Google Scholar] [CrossRef]
- Wang, Z.; Wu, Q.; Ming, J. The Relationship Between Homeownership and the Utilization of Local Public Health Services Among Rural Migrants in China: A Nationwide Cross-Sectional Study. Front. Public Health. 2020, 8, 589038. [Google Scholar] [CrossRef]
- Tyner, A.; Ren, Y. The hukou system, rural institutions, and migrant integration In China. J. East. Asian Stud. 2016, 16, 331–348. [Google Scholar] [CrossRef] [Green Version]
- Pickett, K.E.; Wilkinson, R.G. Income inequality and health: A causal review. Soc. Sci. Med. 2015, 128, 316–326. [Google Scholar] [CrossRef]
- Aalto, A.M.; Uutela, A.; Kangas, T. Health behaviour, social integration, perceived health and dysfunction. A comparison between patients with type I and II diabetes and controls. Scand. J. Soc. Med. 1996, 24, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef] [PubMed]
- Leng, A.; Maitland, E.; Wang, S.; Nicholas, S.; Liu, R.; Wang, J. Individual preferences for COVID-19 vaccination in China. Vaccine 2021, 39, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Diaz, M.; Barrionuevo-Rosas, L.; Herrero, R.; Bray, F.; Bosch, F.X.; de Sanjosé, S.; Castellsagué, X. Global estimates of human papillomavirus vaccination coverage by region and income level: A pooled analysis. Lancet Glob. Health 2016, 4, e453–e463. [Google Scholar] [CrossRef] [Green Version]
- Fellmeth, G.; Rose-Clarke, K.; Zhao, C.; Busert, L.K.; Zheng, Y.; Massazza, A.; Sonmez, H.; Eder, B.; Blewitt, A.; Lertgrai, W.; et al. Health impacts of parental migration on left-behind children and adolescents: A systematic review and meta-analysis. Lancet 2018, 392, 2567–2582. [Google Scholar] [CrossRef] [Green Version]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef]
- Luyten, J.; Beutels, P. The Social Value of Vaccination Programs: Beyond Cost-Effectiveness. Health Aff. 2016, 35, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Omoniyi, O.S.; Williams, I. Realist Synthesis of the International Theory and Evidence on Strategies to Improve Childhood Vaccination in Low- and Middle-Income Countries: Developing Strategies for the Nigerian Healthcare System. Int. J. Health Policy Manag. 2020, 9, 274–285. [Google Scholar] [CrossRef] [Green Version]
- Cherian, T.; Morales, K.F.; Mantel, C.; Lambach, P.; Independent Expert Advisory Group (IEAG) for Health Worker Influenza Vaccination. Factors and considerations for establishing and improving seasonal influenza vaccination of health workers: Report from a WHO meeting, 16–17 January, Berlin, Germany. Vaccine 2019, 37, 6255–6261. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) | Got Vaccinated | |||
|---|---|---|---|---|---|
| N (%) | OR | 95% CI | p-Value | ||
| Total | 12,476 (100) | 1414 (11.33) | |||
| Demographic characteristics | |||||
| Gender | 1.018 | 0.91–1.14 | 0.753 | ||
| Male | 6393 (51.24) | 719 | |||
| Female | 6083 (48.76) | 695 | |||
| Age | 0.673 | 0.60–0.75 | 0.000 *** | ||
| ≤30 | 4627 (37.09) | 644 | |||
| 31–40 | 4090 (32.78) | 473 | |||
| 41–50 | 2727 (21.86) | 219 | |||
| >50 | 1032 (8.27) | 78 | |||
| Marital status | 0.703 | 0.62–0.80 | 0.000 *** | ||
| Single | 2317 (18.57) | 335 | |||
| Married | 10,159 (81.43) | 1079 | |||
| Region | 1.028 | 0.89–1.19 | 0.707 | ||
| Rural | 10,341 (82.89) | 1167 | |||
| Urban | 2135 (17.11) | 247 | |||
| Socioeconomic characteristics | |||||
| Education attainment | 1.5445 | 1.38–1.73 | 0.000 *** | ||
| Middle school or below | 6941 (55.63) | 651 | |||
| High school | 3235 (25.93) | 446 | |||
| Three-year technical college | 1494 (11.97) | 205 | |||
| University or above | 806 (6.46) | 112 | |||
| Social security card | 1.208 | 1.08–1.35 | 0.001 ** | ||
| Have | 6433 (51.56) | 788 | |||
| Do not have | 6043 (48.44) | 626 | |||
| Income status | 0.725 | 0.65–0.81 | 0.000 *** | ||
| High income | 7166 (57.44) | 683 | |||
| Characteristics | N (%) | Got vaccinated | |||
| N (%) | OR | 95%CI | p-Value | ||
| Middle income | 1684 (13.50) | 233 | |||
| Low income | 3636 (29.06) | 498 | |||
| Characteristics about health | |||||
| Health status | 1.414 | 0.90–2.22 | 0.1134 | ||
| Healthy | 12,224 (97.98) | 1393 | |||
| Unhealthy | 252 (2.02) | 21 | |||
| Hypertension | 0.498 | 0.35–0.72 | 0.000 *** | ||
| Yes | 523 (4.19) | 32 | |||
| No | 11,953 (95.81) | 1382 | |||
| Type 2 diabetes mellitus(T2DM) Yes | 124 (0.99) | 9 | 0.610 | 0.31–1.20 | 0.127 |
| No | 12,352 (99.01) | 1045 | |||
| Establishment of health record Yes | 3925 (31.46) | 512 | 1.272 | 1.13–1.43 | 0.000 *** |
| No | 8551(68.54) | 902 | |||
| The awareness of basic public health services program | 1.360 | 1.206–1.533 | 0.000 *** | ||
| Yes | 7961 (63.81) | 988 | |||
| No | 4515 (36.19) | 426 | |||
| Model 1 | Model 2 | Model 3 | |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Social integration | 1.106 ** (1.02, 1.20) | 1.142 ** (1.04, 1.22) | |
| Social exclusion | 1.011 (0.90, 1.13) | 1.062 (1.00, 1.13) | |
| Demographic characteristics | |||
| Gender (Female) | |||
| Male | 2.046 (0.96, 4.37) | 1.056 (0.71, 1.57) | 3.408 * (0.95, 4.35) |
| Age (≤30) | |||
| 31–40 | 0.881 (0.77, 1.01) | 0.884 (0.77, 1.02) | 0.880 (0.76, 1.01) |
| 41–50 | 0.611 *** (0.51, 0.73) | 0.610 *** (0.51, 0.73) | 0.609 *** (0.51, 0.73) |
| >50 | 0.550 *** (0.42, 0.72) | 0.555 *** (0.42, 0.73) | 0.550 *** (0.42, 0.72) |
| Marital status (Single) | |||
| Married | 0.871 (0.75, 1.01) | 0.873 (0.75, 1.01) | 0.868 (0.75, 1.01) |
| Region (Rural) | |||
| Urban | 0.909 (0.78, 1.06) | 0.924 (0.79, 1.08) | 0.914 (0.78, 1.07) |
| Socioeconomic characteristics | |||
| Education attainment (middle school or below) | |||
| High school | 0.563 (0.23, 1.37) | 2.030 ** (1.26, 3.26) | 0.561 (0.23, 1.37) |
| Three-year technical college | 1.230 (0.38, 3.94) | 1.478 (0.80, 2.73) | 1.214 (0.38, 3.88) |
| University or above | 0.664 (0.14, 3.23) | 1.565 (0.71, 3.44) | 0.663 (0.14, 3.24) |
| Social security card (do not have) | |||
| have | 1.125 * (1.00, 1.26) | 1.130 * (1.01, 1.27) | 1.129 * (1.00, 1.27) |
| Income status (low) | |||
| Middle | 1.438 (0.42, 4.92) | 0.890 (0.46, 1.71) | 1.398 (0.41, 4.79) |
| High | 1.869 (0.79, 4.44) | 0.426 *** (0.28. 0.66) | 1.797 (0.75, 4.28) |
| Characteristics about health | |||
| Health status (unhealthy) | |||
| Healthy | 1.023 (0.64, 1.64) | 1.025 (0.64, 1.64) | 1.034 (0.65, 1.65) |
| Hypertension | 0.683 (0.47, 1.00) | 0.674 * (0.46, 0.99) | 0.680 * (0.46, 0.99) |
| T2DM | 0.909 (0.45, 1.84) | 0.919 (0.45, 1.86) | 0.913 (0.45, 1.84) |
| Health record | 1.106 (0.97, 1.37) | 1.121 (0.99, 1.27) | 1.112 (0.98, 1.26) |
| The awareness of basic public health services | 1.200 ** (1.05, 1.01) | 1.219 ** (1.09, 1.39) | 1.208 ** (1.06, 1.38) |
| Interactions | |||
| Gender * Social integration | 0.936 (0.87, 1.01) | 0.913 * (0.84, 0.99) | |
| Gender * Social exclusion | 0.996 (0.90, 1.11) | 0.932 (0.83, 1.05) | |
| Income status * Social integration (low income) | |||
| Middle income | 0.962 (0.85, 1.09) | 0.954 (0.83, 1.10) | |
| High income | 0.899 * (0.83, 0.98) | 0.911 (0.93, 1.00) | |
| Income status * Social exclusion (low income) | |||
| Middle income | 1.008 (0.85, 1.19) | 0.976 (0.80, 1.18) | |
| High income | 1.104 (0.98, 1.24) | 1.033 (0.90, 1.18) | |
| Education attainment * Social integration | |||
| High school | 1.093 * (1.00, 1.19) | 1.078 (0.98, 1.19) | |
| Three-year technical college | 1.003 (0.90, 1.12) | 0.989 (0.86, 1.13) | |
| University or above | 1.063 (0.92, 1.24) | 1.063 (0.89, 1.27) | |
| Education attainment * Social exclusion | |||
| High school | 0.903 (0.80, 1.02) | 0.962 (0.83, 1.11) | |
| Three-year technical college | 0.962 (0.82, 1.13) | 0.957 (0.78, 1.17) | |
| University or above | 0.945 (0.76, 1.17) | 0.996 (0.77, 1.28) | |
| P for the model | 0.000 *** | 0.000 *** | 0.000 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Bai, Y.; Zhu, J.; Wang, X.; Che, Y.; Liu, J. Association between Social Integration, Social Exclusion, and Vaccination Behavior among Internal Migrants in China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 7915. https://doi.org/10.3390/ijerph19137915
Wang J, Bai Y, Zhu J, Wang X, Che Y, Liu J. Association between Social Integration, Social Exclusion, and Vaccination Behavior among Internal Migrants in China: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(13):7915. https://doi.org/10.3390/ijerph19137915
Chicago/Turabian StyleWang, Jun, Yang Bai, Jingmin Zhu, Xueyao Wang, Yue Che, and Jue Liu. 2022. "Association between Social Integration, Social Exclusion, and Vaccination Behavior among Internal Migrants in China: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 13: 7915. https://doi.org/10.3390/ijerph19137915
APA StyleWang, J., Bai, Y., Zhu, J., Wang, X., Che, Y., & Liu, J. (2022). Association between Social Integration, Social Exclusion, and Vaccination Behavior among Internal Migrants in China: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(13), 7915. https://doi.org/10.3390/ijerph19137915