
Effects of a Long-Term Monitored Exercise Program on Aerobic Fitness in a Small Group of Children with Cystic Fibrosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
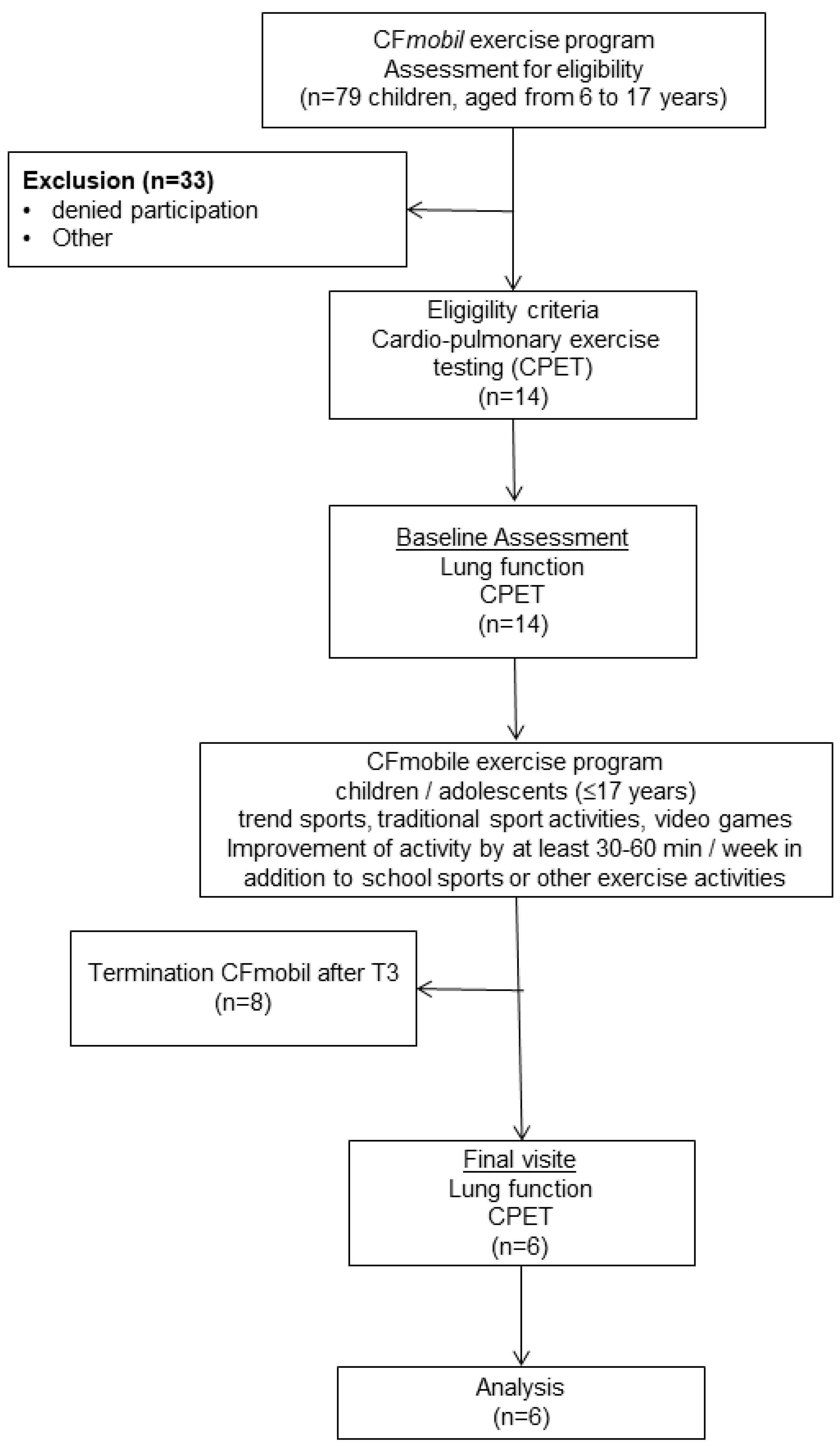
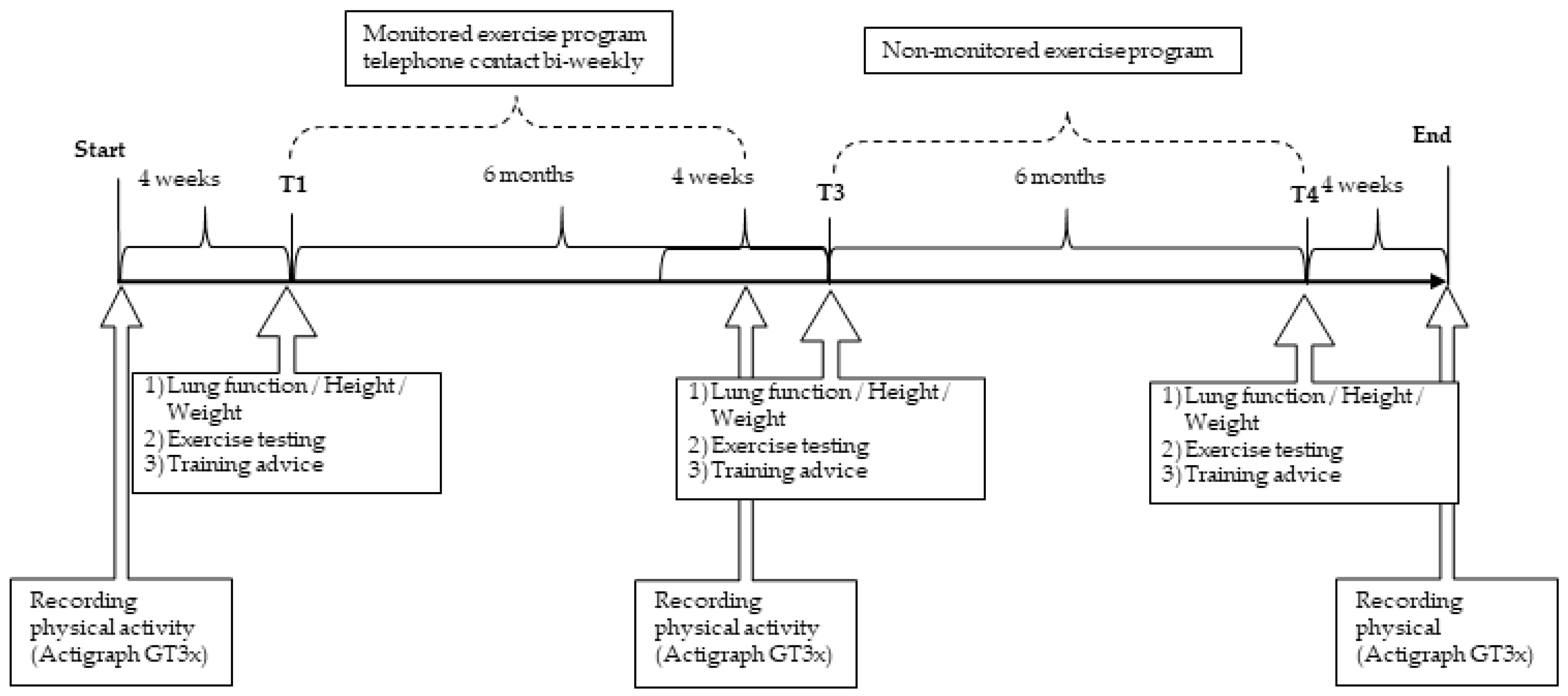
2.1. Study Design
2.2. Testing
2.3. Statistics
3. Results
3.1. Anthropometric Characteristics and Lung Function
3.2. Habitual Physical Activity
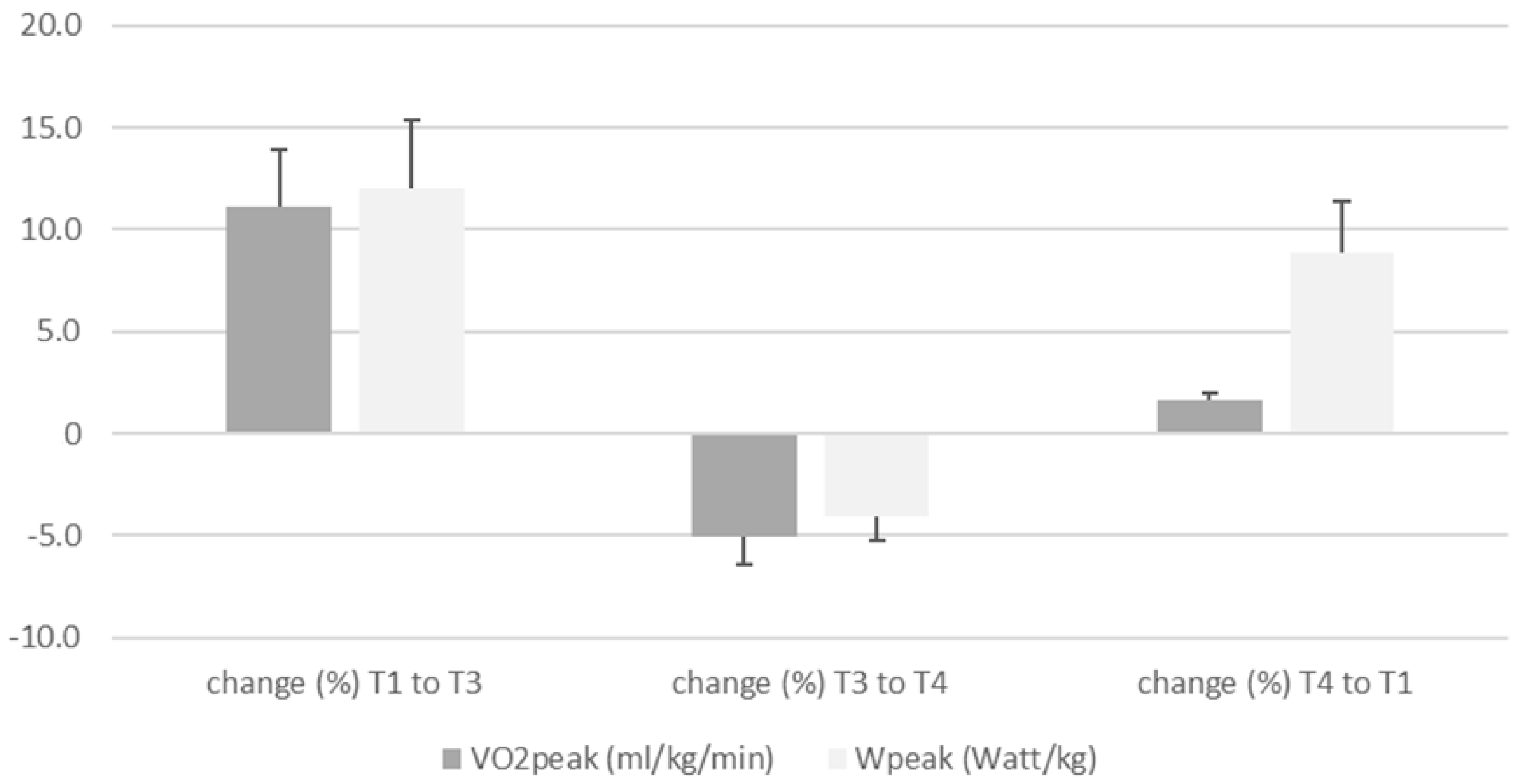
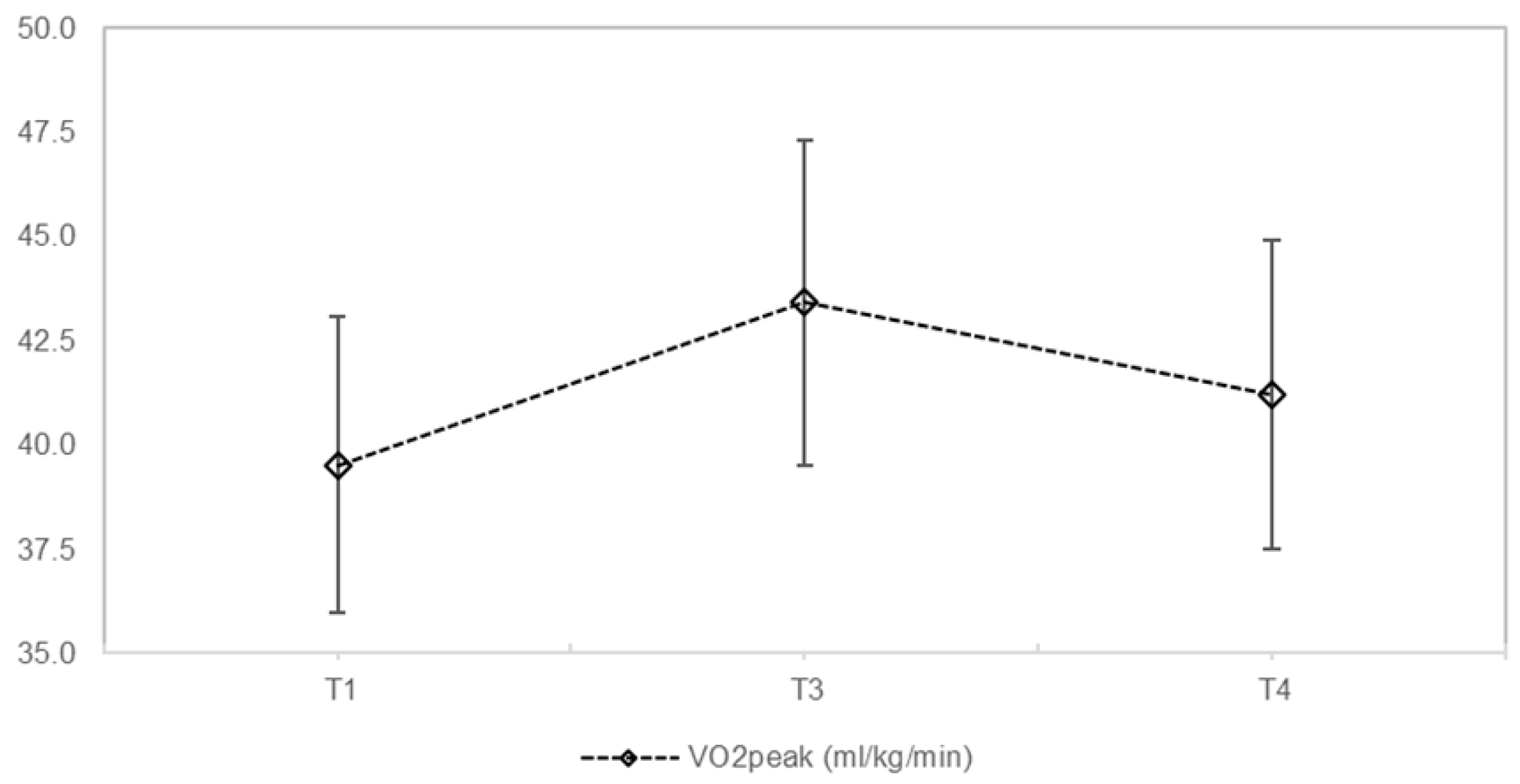
3.3. Exercise Capacity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bell, S.C.; Mall, M.A.; Gutierrez, H.; Macek, M.; Madge, S.; Davies, J.C.; Burgel, P.R.; Tullis, E.; Castaños, C.; Castellani, C.; et al. The future of cystic fibrosis care: A global perspective. Lancet. Respir. Med. 2020, 8, 65–124. [Google Scholar] [CrossRef] [Green Version]
- Elborn, J.S. Cystic fibrosis. Lancet (Lond. Engl.) 2016, 388, 2519–2531. [Google Scholar] [CrossRef]
- Jackson, A.D.; Daly, L.; Jackson, A.L.; Kelleher, C.; Marshall, B.C.; Quinton, H.B.; Fletcher, G.; Harrington, M.; Zhou, S.; McKone, E.F.; et al. Validation and use of a parametric model for projecting cystic fibrosis survivorship beyond observed data: A birth cohort analysis. Thorax 2011, 66, 674–679. [Google Scholar] [CrossRef] [Green Version]
- Castellani, C.; Duff, A.J.A.; Bell, S.C.; Heijerman, H.G.M.; Munck, A.; Ratjen, F.; Sermet-Gaudelus, I.; Southern, K.W.; Barben, J.; Flume, P.A.; et al. ECFS best practice guidelines: The 2018 revision. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2018, 17, 153–178. [Google Scholar] [CrossRef] [Green Version]
- Radtke, T.; Nevitt, S.J.; Hebestreit, H.; Kriemler, S. Physical exercise training for cystic fibrosis. Cochrane Database Syst. Rev. 2017, 11. [Google Scholar] [CrossRef]
- Gruber, W.; Orenstein, D.M.; Braumann, K.M.; Beneke, R. Interval exercise training in cystic fibrosis-effects on exercise capacity in severely affected adults. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2014, 13, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Paranjape, S.M.; Barnes, L.A.; Carson, K.A.; von Berg, K.; Loosen, H.; Mogayzel, P.J., Jr. Exercise improves lung function and habitual activity in children with cystic fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2012, 11, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Hebestreit, H.; Kieser, S.; Junge, S.; Ballmann, M.; Hebestreit, A.; Schindler, C.; Schenk, T.; Posselt, H.G.; Kriemler, S. Long-term effects of a partially supervised conditioning programme in cystic fibrosis. Eur. Respir J. 2010, 35, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Kriemler, S.; Kieser, S.; Junge, S.; Ballmann, M.; Hebestreit, A.; Schindler, C.; Stussi, C.; Hebestreit, H. Effect of supervised training on FEV1 in cystic fibrosis: A randomised controlled trial. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2013, 12, 714–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruber, W.; Stehling, F.; Olivier, M.; Dillenhoefer, S.; Koerner-Rettberg, C.; Sutharsan, S.; Taube, C.; Mellies, U.; Welsner, M. Effects of a long-term exercise program on motor performance in children and adolescents with CF. Pediatric Pulmonol. 2020, 55, 3371–3380. [Google Scholar] [CrossRef]
- Hebestreit, H.; Kieser, S.; Rudiger, S.; Schenk, T.; Junge, S.; Hebestreit, A.; Ballmann, M.; Posselt, H.G.; Kriemler, S. Physical activity is independently related to aerobic capacity in cystic fibrosis. Eur. Respir. J. 2006, 28, 734–739. [Google Scholar] [CrossRef]
- Gruber, W.; Orenstein, D.M.; Braumann, K.M. Do responses to exercise training in cystic fibrosis depend on initial fitness level? Eur. Respir J. 2011, 38, 1336–1342. [Google Scholar] [CrossRef] [Green Version]
- Cox, N.S.; Holland, A.E. Current perspectives of physical activity in cystic fibrosis. Expert Rev. Respir. Med. 2019, 13, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Hebestreit, H.; Hulzebos, E.H.J.; Schneiderman, J.E.; Karila, C.; Boas, S.R.; Kriemler, S.; Dwyer, T.; Sahlberg, M.; Urquhart, D.S.; Lands, L.C.; et al. Cardiopulmonary Exercise Testing Provides Additional Prognostic Information in Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2019, 199, 987–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nixon, P.A.; Orenstein, D.M.; Kelsey, S.F.; Doershuk, C.F. The prognostic value of exercise testing in patients with cystic fibrosis. N. Engl. J. Med. 1992, 327, 1785–1788. [Google Scholar] [CrossRef]
- Vendrusculo, F.M.; Heinzmann-Filho, J.P.; Da Silva, J.S.; Perez Ruiz, M.; Donadio, M.V.F. Peak Oxygen Uptake and Mortality in Cystic Fibrosis: Systematic Review and Meta-Analysis. Respir. Care 2019, 64, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Rovedder, P.M.; Flores, J.; Ziegler, B.; Casarotto, F.; Jaques, P.; Barreto, S.S.; Dalcin Pde, T. Exercise programme in patients with cystic fibrosis: A randomized controlled trial. Respir. Med. 2014, 108, 1134–1140. [Google Scholar] [CrossRef] [Green Version]
- Urquhart, D.; Sell, Z.; Dhouieb, E.; Bell, G.; Oliver, S.; Black, R.; Tallis, M. Effects of a supervised, outpatient exercise and physiotherapy programme in children with cystic fibrosis. Pediatric Pulmonol. 2012, 47, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Selvadurai, H.C.; Blimkie, C.J.; Meyers, N.; Mellis, C.M.; Cooper, P.J.; van Asperen, P.P. Randomized controlled study of in-hospital exercise training programs in children with cystic fibrosis. Pediatric Pulmonol. 2002, 33, 194–200. [Google Scholar] [CrossRef]
- Welsner, M.; Gruber, W.; Sutharsan, S.; Taube, C.; Olivier, M.; Mellies, U.; Koerner-Rettberg, C.; Dillenhöfer, D.; Stehling, F. Trainability of Health-Related and Motor Performance Fitness in Adults with Cystic Fibrosis within a 12-Month Partially Supervised Exercise Program. Pulm. Med. 2021, 2021, 5581812. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Swisher, A.K.; Hebestreit, H.; Mejia-Downs, A.; Lowman, J.D.; Gruber, W.; Nippins, M.; Alison, J.; Schneiderman, J. Exercise and Habitual Physical Activity for People with Cystic Fibrosis: Expert Consensus, Evidence-Based Guide for Advising Patients. Cardiopulm Phys. J. 2015, 1, 1–14. [Google Scholar] [CrossRef]
- Strath, S.J.; Kaminsky, L.A.; Ainsworth, B.E.; Ekelund, U.; Freedson, P.S.; Gary, R.A.; Richardson, C.R.; Smith, D.T.; Swartz, A.M. Guide to the assessment of physical activity: Clinical and research applications: A scientific statement from the American Heart Association. Circulation 2013, 128, 2259–2279. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Godfrey, S.; Mearns, M. Pulmonary function and response to exercise in cystic fibrosis. Arch. Dis. Child. 1971, 46, 144–151. [Google Scholar] [CrossRef] [Green Version]
- Hebestreit, H.; Arets, H.G.; Aurora, P.; Boas, S.; Cerny, F.; Hulzebos, E.H.; Karila, C.; Lands, L.C.; Lowman, J.D.; Swisher, A.; et al. Statement on Exercise Testing in Cystic Fibrosis. Respir. Int. Rev. Thorac. Dis. 2015, 90, 332–351. [Google Scholar] [CrossRef]
- Cooper, C.B.; Storer, T. Exercise Testing and Interpretation. A Practical Approach; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- Godfrey, S. Exercise Testing in Children. Applications in HEALTH and Disease; WB Saunders: Philadelphia, PA, USA, 1974. [Google Scholar]
- Orenstein, D. Assessment of exercise pulmonary function. In Pediatric Laboratory Exercise Testing; Rowland, T., Ed.; Human Kinetics: Champaign, IL, USA, 1993; pp. 141–163. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Rowland, T. Developmental Exercise Physiology; Human Kinetics: Champaign, IL, USA, 1996. [Google Scholar]
- Hommerding, P.X.; Baptista, R.R.; Makarewicz, G.T.; Schindel, C.S.; Donadio, M.V.; Pinto, L.A.; Marostica, P.J. Effects of an educational intervention of physical activity for children and adolescents with cystic fibrosis: A randomized controlled trial. Respir. Care 2015, 60, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Denford, S.; Mackintosh, K.A.; McNarry, M.A.; Barker, A.R.; Williams, C.A. Promotion of physical activity for adolescents with cystic fibrosis: A qualitative study of UK multi disciplinary cystic fibrosis teams. Physiotherapy 2020, 106, 111–118. [Google Scholar] [CrossRef]
- Schindel, C.S.; Hommerding, P.X.; Melo, D.A.S.; Baptista, R.R.; Marostica, P.J.C.; Donadio, M.V.F. Physical exercise recommendations improve postural changes found in children and adolescents with cystic fibrosis: A randomized controlled trial. J. Pediatrics 2015, 166, 710–716.e2. [Google Scholar] [CrossRef]
- Denford, S.; van Beurden, S.; O’Halloran, P.; Williams, C. Barriers and facilitators to physical activity among children, adolescents, and young adults with cystic fibrosis: A systematic review and thematic synthesis of qualitative research. BMJ Open 2020, 10, e035261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denford, S.; Mackintosh, K.A.; McNarry, M.A.; Barker, A.R.; Williams, C.A. Enhancing intrinsic motivation for physical activity among adolescents with cystic fibrosis: A qualitative study of the views of healthcare professionals. BMJ Open 2019, 9, e028996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bierlaagh, M.C.; Muilwijk, D.; Beekman, J.M.; van der Ent, C.K. A new era for people with cystic fibrosis. Eur. J. Pediatrics 2021, 180, 2731–2739. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants (n = 6) | |||||
|---|---|---|---|---|---|
| Mean ± SD T1 | Mean ± SD T3 | Mean ± SD T4 | Chi-Quadrat | p-Value | |
| Age (years) | 11.3 ± 3.3 | ||||
| Height (cm) | 143.6 ± 10.3 | 146.2 ± 13.0 | 147.6 ± 11.7 * | 9.652 | 0.008 |
| Weight (kg) | 38.2 ± 10.0 | 38.5 ± 9.8 | 40.2 ± 10.8 | 4.261 | 0.119 |
| BMI | 18.2 ± 2.5 | 17.8 ± 2.4 | 18.0 ± 2.4 | 0.933 | 0.627 |
| ppFEV1 | 102.5 ± 13.1 | 104.0 ± 8.7 | 92.3 ± 9.4 * | 6.333 | 0.042 |
| ppFVC | 94.0 ± 13.7 | 95.3 ± 7.5 | 94.0 ± 11.1 | 0.333 | 0.846 |
| Steps/day | 10,791 ± 2103 | 10,835 ± 1072 | 10,298 ± 1905 | 1.600 | 0.449 |
| Sedentary intensity (<1.5 METs) min/day | 821.0 ± 116.7 | 724.0 ± 96.2 | 744.0 ± 107.9 | 2.800 | 0.247 |
| Light intensity (1.5–3 METs) min/day | 416.2 ± 71.6 | 442.0 ± 61.2 | 397.7 ± 75.6 | 0.737 | 0.692 |
| Moderate-to-vigorous intensity (3–5.9 METs) min/day | 107.3 ± 80.7 | 116.6 ± 66.3 | 97.3 ± 69.9 | 2.632 | 0.268 |
| Vigorous intensity (>6 METs) min/day | 16.3 ± 11.0 | 18.6 ± 14.3 | 16.8 ± 11.0 | 3.500 | 0.174 |
| TG (n = 6) | |||||
|---|---|---|---|---|---|
| Mean ± SD T1 | Mean ± SD T3 | Mean ± SD T4 | Chi-Quadrat | p-Value | |
| VO2peak (mL/kg/min) | 39.5 ± 8.7 | 43.4 ± 9.3 | 41.2 ± 7.1 | 1.600 | 0.449 |
| VO2peak (%pred) | 88.6 ± 18.6 | 95.0 ± 18.2 | 91.0 ± 17.6 | 2.211 | 0.331 |
| BR (%) | 68.9 ± 17.0 | 74.3 ± 13.8 | 78.8 ± 11.8 | 0.400 | 0.819 |
| Wpeak (Watt/kg) | 2.9 ± 0.8 | 3.2 ± 0.6 | 3.1 ± 0.6 | 2.666 | 0.264 |
| Wpeak(%pred) | 95.5 ± 26.3 | 107.3 ± 22.8 | 104.0 ± 26.3 | 2.311 | 0.311 |
| HFpeak (b/min) | 184.8 ± 13.1 | 183.3 ± 14.3 | 183.0 ± 17.1 | 0.609 | 0.738 |
| HFpeak (%/peak) | 94.8 ± 6.7 | 94.0 ± 7.4 | 93.8 ± 8.8 | 0.609 | 0.738 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gruber, W.; Stehling, F.; Blosch, C.; Dillenhoefer, S.; Olivier, M.; Koerner-Rettberg, C.; Sutharsan, S.; Mellies, U.; Taube, C.; Welsner, M. Effects of a Long-Term Monitored Exercise Program on Aerobic Fitness in a Small Group of Children with Cystic Fibrosis. Int. J. Environ. Res. Public Health 2022, 19, 7923. https://doi.org/10.3390/ijerph19137923
Gruber W, Stehling F, Blosch C, Dillenhoefer S, Olivier M, Koerner-Rettberg C, Sutharsan S, Mellies U, Taube C, Welsner M. Effects of a Long-Term Monitored Exercise Program on Aerobic Fitness in a Small Group of Children with Cystic Fibrosis. International Journal of Environmental Research and Public Health. 2022; 19(13):7923. https://doi.org/10.3390/ijerph19137923
Chicago/Turabian StyleGruber, Wolfgang, Florian Stehling, Christopher Blosch, Stefanie Dillenhoefer, Margarete Olivier, Cordula Koerner-Rettberg, Sivagurunathan Sutharsan, Uwe Mellies, Christian Taube, and Matthias Welsner. 2022. "Effects of a Long-Term Monitored Exercise Program on Aerobic Fitness in a Small Group of Children with Cystic Fibrosis" International Journal of Environmental Research and Public Health 19, no. 13: 7923. https://doi.org/10.3390/ijerph19137923
APA StyleGruber, W., Stehling, F., Blosch, C., Dillenhoefer, S., Olivier, M., Koerner-Rettberg, C., Sutharsan, S., Mellies, U., Taube, C., & Welsner, M. (2022). Effects of a Long-Term Monitored Exercise Program on Aerobic Fitness in a Small Group of Children with Cystic Fibrosis. International Journal of Environmental Research and Public Health, 19(13), 7923. https://doi.org/10.3390/ijerph19137923