
The Potential of Thyroid Hormone Therapy in Severe COVID-19: Rationale and Preliminary Evidence

 ,
,
Abstract
:1. Introduction
2. Tissue Hypoxia: A Unifying Pathophysiologic Mechanism in Myocardial Infarction, Sepsis and Severe COVID-19
3. TH and Tissue Hypoxia
3.1. Differential Effects of TH on Healthy and Injured Tissue
3.2. Potential Underlying Mechanisms of TH Effects on Tissue Hypoxia
3.3. TH as Potential Therapy for Tissue Hypoxia
4. The Role of TH in COVID-19
5. TH Therapy in Severe COVID-19: Preliminary Clinical Evidence
6. Conclusions
7. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Padhi, R.; Kabi, S.; Panda, B.N.; Jagati, S. Prognostic significance of nonthyroidal illness syndrome in critically ill adult patients with sepsis. Int. J. Crit. Illn. Inj. Sci. 2018, 8, 165–172. [Google Scholar] [PubMed]
- Chen, W.; Tian, Y.; Li, Z.; Zhu, J.; Wei, T.; Lei, J. Potential Interaction Between SARS-CoV-2 and Thyroid: A Review. Endocrinology 2021, 162, bqab004. [Google Scholar] [CrossRef] [PubMed]
- Johansson, P.I.; Stensballe, J.; Ostrowski, S.R. Shock induced endotheliopathy (SHINE) in acute critical illness—A unifying pathophysiologic mechanism. Crit. Care 2017, 21, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantos, C.; Mourouzis, I.; Cokkinos, D.V. Rebuilding the post-infarcted myocardium by activating ‘physiologic’ hypertrophic signaling pathways: The thyroid hormone paradigm. Heart Fail. Rev. 2010, 15, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Pantos, C.; Mourouzis, I. Thyroid hormone receptor α1 as a novel therapeutic target for tissue repair. Ann. Transl. Med. 2018, 6, 254. [Google Scholar] [CrossRef] [PubMed]
- Pantos, C.I.; Trikas, A.G.; Pisimisis, E.G.; Grigoriou, K.P.; Stougiannos, P.N.; Dimopoulos, A.K.; Linardakis, S.I.; Alexopoulos, N.A.; Evdoridis, C.G.; Gavrielatos, G.D.; et al. Effects of acute triiodothyronine treatment in patients with anterior myocardial infarction undergoing primary angioplasty: Evidence from a pilot randomized clinical trial (ThyRepair study). Thyroid 2022, 32, 714–724. [Google Scholar] [CrossRef]
- Mourouzis, I.S.; Lourbopoulos, A.I.; Trikas, A.G.; Tseti, I.K.; Pantos, C.I. Triiodothyronine prevents tissue hypoxia in experimental sepsis: Potential therapeutic implications. Intensive Care Med. Exp. 2021, 9, 17. [Google Scholar] [CrossRef]
- Pantos, C.; Kostopanagiotou, G.; Armaganidis, A.; Trikas, A.; Tseti, I.; Mourouzis, I. Triiodothyronine for the treatment of critically ill patients with COVID-19 infection: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 573. [Google Scholar] [CrossRef]
- Pantos, C.; Tseti, I.; Mourouzis, I. Use of triiodothyronine to treat critically ill COVID-19 patients: A new clinical trial. Crit. Care 2020, 24, 209. [Google Scholar] [CrossRef]
- Dekker, N.A.M.; Veerhoek, D.; Koning, N.J.; van Leeuwen, A.L.I.; Elbers, P.W.G.; van den Brom, C.E.; Vonk, A.B.A.; Boer, C. Postoperative microcirculatory perfusion and endothelial glycocalyx shedding following cardiac surgery with cardiopulmonary bypass. Anaesthesia 2019, 74, 609–618. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.L.; De Backer, D. Microvascular dysfunction as a cause of organdysfunction in severe sepsis. Crit. Care 2005, 9 (Suppl. S4), S9–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakr, Y.; Dubois, M.J.; De Backer, D.; Creteur, J.; Vincent, J.L. Persistent microcirculatory alterations are associated with organ failure and death in patients with septic shock. Crit. Care Med. 2004, 32, 1825–1831. [Google Scholar] [CrossRef]
- Konijnenberg, L.S.F.; Damman, P.; Duncker, D.J.; Kloner, R.A.; Nijveldt, R.; van Geuns, R.M.; Berry, C.; Riksen, N.P.; Escaned, J.; van Royen, N. Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction. Cardiovasc. Res. 2020, 116, 787–805. [Google Scholar] [CrossRef]
- van Kranenburg, M.; Magro, M.; Thiele, H.; de Waha, S.; Eitel, I.; Cochet, A.; Cottin, Y.; Atar, D.; Buser, P.; Wu, E.; et al. Prognostic value of microvascular obstruction and infarct size, as measured by CMR in STEMI patients. JACC Cardiovasc. Imaging 2014, 7, 930–939. [Google Scholar] [CrossRef] [PubMed]
- Kanoore Edul, V.S.; Caminos Eguillor, J.F.; Ferrara, G.; Estenssoro, E.; Siles, D.S.P.; Cesio, C.E.; Dubin, A. Microcirculation alterations in severe COVID-19 pneumonia. J. Crit. Care 2021, 61, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Sloop, G.D.; Pop, G.A.; Weidman, J.J.; Cyr, J.A. The Detrimental Role of Elevated Blood Viscosity in Patients With COVID-19. J. Cardiol. Ther. 2021, 8, 976–980. [Google Scholar]
- Johansson, P.I.; Stensballe, J.; Rasmussen, L.S.; Ostrowski, S.R. A high admission syndecan-1 level, a marker of endothelial glycocalyx degradation, is associated with inflammation, protein C depletion, fibrinolysis, and increased mortality in trauma patients. Ann. Surg. 2011, 254, 194–200. [Google Scholar] [CrossRef]
- Johansen, M.E.; Johansson, P.I.; Ostrowski, S.R.; Bestle, M.H.; Hein, L.; Jensen, A.L.; Soe-Jensen, P.; Andersen, M.H.; Steensen, M.; Mohr, T.; et al. Profound endothelial damage predicts impending organ failure and death in sepsis. Semin. Thromb. Hemost. 2015, 41, 16–25. [Google Scholar] [CrossRef]
- Zhang, D.; Li, L.; Chen, Y.; Ma, J.; Yang, Y.; Aodeng, S.; Cui, Q.; Wen, K.; Xiao, M.; Xie, J.; et al. Syndecan-1, an indicator of endothelial glycocalyx degradation, predicts outcome of patients admitted to an ICU with COVID-19. Mol. Med. 2021, 27, 151. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
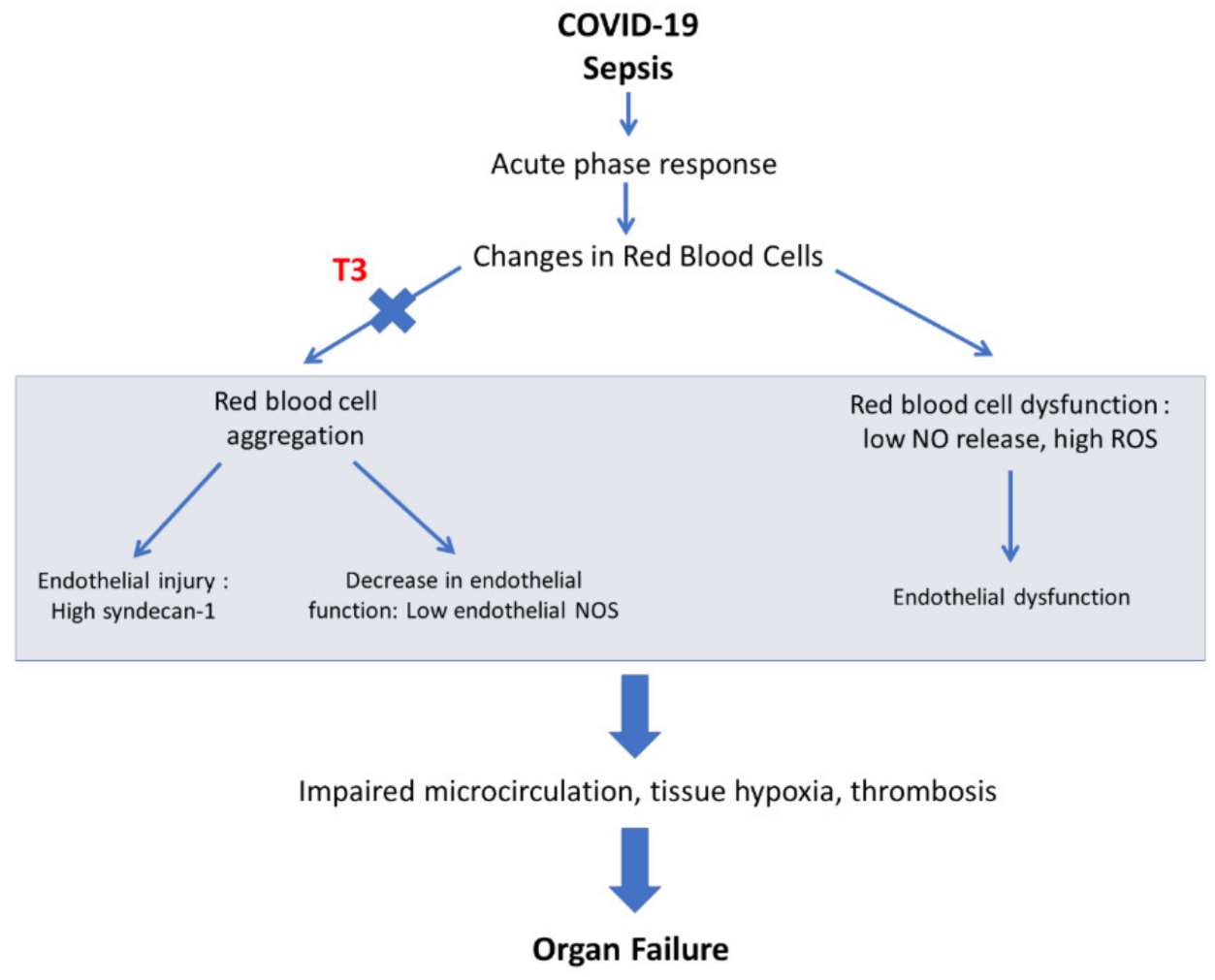
- Baskurt, O.K.; Yalcin, O.; Ozdem, S.; Armstrong, J.K.; Meiselman, H.J. Modulation of endothelial nitric oxide synthase expression by red blood cell aggregation. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H222–H229. [Google Scholar] [CrossRef] [Green Version]
- Iffrig, E.; Oakley, J.; Fibben, K.; Sakurai, Y.; Esper, A.M.; Lam, W. Severe COVID-19 Is an Acquired Red Cell Disease- Potential Mechanisms Underlying Endothelialitis. Am. J. Respir. Crit. Care Med. 2021, 203, A4470. [Google Scholar]
- Baskurt, O.K.; Temiz, A.; Meiselman, H.J. Red blood cell aggregation in experimental sepsis. J. Lab. Clin. Med. 1997, 130, 183–190. [Google Scholar] [CrossRef]
- Li, C.; Wang, Y.; Zhang, Q.; Wang, L.; Li, K.; Yang, X. Incorporating the erythrocyte sedimentation rate for enhanced accuracy of the global registry of acute coronary event score in patients with ST-segment elevated myocardial infarction: A retrospective cohort study. Medicine 2020, 99, e22523. [Google Scholar] [CrossRef] [PubMed]
- Nader, E.; Nougier, C.; Boisson, C.; Poutrel, S.; Catella, J.; Martin, F.; Charvet, J.; Girard, S.; Havard-Guibert, S.; Martin, M.; et al. Increased blood viscosity and red blood cell aggregation in patients with COVID-19. Am. J. Hematol. 2022, 97, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Brugnara, C. The Erythrocyte, a Novel Disease-Mediator for COVID-19 Vasculopathy? JACC Basic Transl. Sci. 2022, 7 Pt 1, 205–206. [Google Scholar] [CrossRef]
- Mahdi, A.; Collado, A.; Tengbom, J.; Jiao, T.; Wodaje, T.; Johansson, N.; Farnebo, F.; Färnert, A.; Yang, J.; Lundberg, J.O.; et al. Erythrocytes Induce Vascular Dysfunction in COVID-19. JACC Basic Transl. Sci. 2022, 7 Pt 1, 193–204. [Google Scholar] [CrossRef]
- Xi, Y.; Kim, T.; Brumwell, A.N.; Driver, I.H.; Wei, Y.; Tan, V.; Jackson, J.R.; Xu, J.; Lee, D.K.; Gotts, J.E.; et al. Local lung hypoxia determines epithelial fate decisions during alveolar regeneration. Nat. Cell Biol. 2017, 19, 904–914. [Google Scholar] [CrossRef]
- Wibowo, A.; Pranata, R.; Akbar, M.R.; Purnomowati, A.; Martha, J.W. Prognostic performance of troponin in COVID-19: A diagnostic meta-analysis and meta-regression. Int. J. Infect. Dis. 2021, 105, 312–318. [Google Scholar] [CrossRef]
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Gal Oz, A.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of Cardiac Manifestations in COVID-19: A Systematic Echocardiographic Study. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef]
- Vanderhaeghen, T.; Vandewalle, J.; Libert, C. Hypoxia-inducible factors in metabolic reprogramming during sepsis. FEBS J. 2020, 287, 1478–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbesen, P.; Eckardt, K.U.; Ciampor, F.; Pettersen, E.O. Linking measured intercellular oxygen concentration to human cell functions. Acta Oncol. 2004, 43, 598–600. [Google Scholar] [CrossRef] [PubMed]
- Lourbopoulos, A.I.; Mourouzis, I.S.; Trikas, A.G.; Tseti, I.K.; Pantos, C.I. Effects of Thyroid Hormone on Tissue Hypoxia: Relevance to Sepsis Therapy. J. Clin. Med. 2021, 10, 5855. [Google Scholar] [CrossRef]
- Colgan, S.P.; Furuta, G.T.; Taylor, C.T. Hypoxia and Innate Immunity: Keeping Up with the HIFsters. Annu. Rev. Immunol. 2020, 38, 341–363. [Google Scholar] [CrossRef] [Green Version]
- Galvan-Pena, S.; O’Neill, L.A. Metabolic reprograming in macrophage polarization. Front. Immunol. 2014, 5, 420. [Google Scholar] [PubMed] [Green Version]
- Jahani, M.; Dokaneheifard, S.; Mansouri, K. Hypoxia: A key feature of COVID-19 launching activation of HIF-1 and cytokine storm. J. Inflamm. 2020, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Liu, W.; Li, X.; Zhao, P.; Shereen, M.A.; Zhu, C.; Huang, S.; Liu, S.; Yu, X.; Yue, M.; et al. HIF-1alpha promotes SARS-CoV-2 infection and aggravates inflammatory responses to COVID-19. Signal Transduct. Target Ther. 2021, 6, 308. [Google Scholar] [CrossRef]
- Pantos, C.; Mourouzis, I. Translating thyroid hormone effects into clinical practice: The relevance of thyroid hormone receptor alpha1 in cardiac repair. Heart Fail. Rev. 2015, 20, 273–282. [Google Scholar] [CrossRef]
- Chen, J.; Ortmeier, S.B.; Savinova, O.V.; Nareddy, V.B.; Beyer, A.J.; Wang, D.; Gerdes, A.M. Thyroid hormone induces sprouting angiogenesis in adult heart of hypothyroid mice through the PDGF-Akt pathway. J. Cell Mol. Med. 2012, 16, 2726–2735. [Google Scholar] [CrossRef]
- Bloise, F.F.; Santos, A.T.; de Brito, J.; de Andrade, C.B.V.; Oliveira, T.S.; de Souza, A.F.P.; Fontes, K.N.; Silva, J.D.; Blanco, N.; Silva, P.L.; et al. Sepsis Impairs Thyroid Hormone Signaling and Mitochondrial Function in the Mouse Diaphragm. Thyroid 2020, 30, 1079–1090. [Google Scholar] [CrossRef]
- Pantos, C.; Mourouzis, I.; Saranteas, T.; Brozou, V.; Galanopoulos, G.; Kostopanagiotou, G.; Cokkinos, D.V. Acute T3 treatment protects the heart against ischemia-reperfusion injury via TRalpha1 receptor. Mol. Cell. Biochem. 2011, 353, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Pantos, C.; Mourouzis, I.; Saranteas, T.; Clave, G.; Ligeret, H.; Noack-Fraissignes, P.; Renard, P.Y.; Massonneau, M.; Perimenis, P.; Spanou, D.; et al. Thyroid hormone improves postischaemic recovery of function while limiting apoptosis: A new therapeutic approach to support hemodynamics in the setting of ischaemia-reperfusion? Basic Res. Cardiol. 2009, 104, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Lieder, H.R.; Braczko, F.; Gedik, N.; Stroetges, M.; Heusch, G.; Kleinbongard, P. Cardioprotection by post-conditioning with exogenous triiodothyronine in isolated perfused rat hearts and isolated adult rat cardiomyocytes. Basic Res. Cardiol. 2021, 116, 27. [Google Scholar] [CrossRef] [PubMed]
- Kleinbongard, P.; Kuthan, P.; Eickelmann, C.; Jakobs, P.; Altschmied, J.; Haendeler, J.; Ruhparwar, A.; Thielmann, M.; Heusch, G. Triiodothyronine improves contractile recovery of human atrial trabeculae after hypoxia/reoxygenation. Int. J. Cardiol 2022. online ahead of print. [Google Scholar] [CrossRef]
- Ferreyra, C.; O’Valle, F.; Osorio, J.M.; Moreno, J.M.; Rodriguez, I.; Vargas, F.; Osuna, A. Effect of preconditioning with triiodothyronine on renal ischemia/reperfusion injury and poly(ADP-ribose) polymerase expression in rats. Transpl. Proc. 2009, 41, 2073–2075. [Google Scholar] [CrossRef]
- Sutter, P.M.; Thulin, G.; Stromski, M.; Ardito, T.; Gaudio, K.M.; Kashgarian, M.; Siegel, N.J. Beneficial effect of thyroxin in the treatment of ischemic acute renal failure. Pediatr. Nephrol. 1988, 2, 1–7. [Google Scholar] [CrossRef]
- Ferreyra, C.; Vargas, F.; Rodriguez-Gomez, I.; Perez-Abud, R.; O’Valle, F.; Osuna, A. Preconditioning with triiodothyronine improves the clinical signs and acute tubular necrosis induced by ischemia/reperfusion in rats. PLoS ONE 2013, 8, e74960. [Google Scholar] [CrossRef] [Green Version]
- Friederich-Persson, M.; Persson, P.; Fasching, A.; Hansell, P.; Nordquist, L.; Palm, F. Increased kidney metabolism as a pathway to kidney tissue hypoxia and damage: Effects of triiodothyronine and dinitrophenol in normoglycemic rats. Adv. Exp. Med. Biol. 2013, 789, 9–14. [Google Scholar]
- Sivertsson, E.; Friederich-Persson, M.; Persson, P.; Nangaku, M.; Hansell, P.; Palm, F. Thyroid hormone increases oxygen metabolism causing intrarenal tissue hypoxia; a pathway to kidney disease. PLoS ONE 2022, 17, e0264524. [Google Scholar] [CrossRef]
- Geist, D.; Hones, G.S.; Gassen, J.; Kerp, H.; Kleinbongard, P.; Heusch, G.; Fuhrer, D.; Moeller, L.C. Noncanonical Thyroid Hormone Receptor alpha Action Mediates Arterial Vasodilation. Endocrinology 2021, 162, bqab099. [Google Scholar] [CrossRef]
- Pantos, C.; Mourouzis, I.; Cokkinos, D.V. Thyroid hormone and cardiac repair/regeneration: From Prometheus myth to reality? Can. J. Physiol. Pharmacol. 2012, 90, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Forini, F.; Nicolini, G.; Iervasi, G. Mitochondria as key targets of cardioprotection in cardiac ischemic disease: Role of thyroid hormone triiodothyronine. Int. J. Mol. Sci. 2015, 16, 6312–6336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantos, C.I.; Malliopoulou, V.A.; Mourouzis, I.S.; Karamanoli, E.P.; Paizis, I.A.; Steimberg, N.; Varonos, D.D.; Cokkinos, D.V. Long-term thyroxine administration protects the heart in a pattern similar to ischemic preconditioning. Thyroid 2002, 12, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Pantos, C.; Mourouzis, I.; Galanopoulos, G.; Gavra, M.; Perimenis, P.; Spanou, D.; Cokkinos, D.V. Thyroid hormone receptor alpha1 downregulation in postischemic heart failure progression: The potential role of tissue hypothyroidism. Horm. Metab. Res. 2010, 42, 718–724. [Google Scholar] [CrossRef]
- Mourouzis, I.; Mantzouratou, P.; Galanopoulos, G.; Kostakou, E.; Roukounakis, N.; Kokkinos, A.D.; Cokkinos, D.V.; Pantos, C. Dose-dependent effects of thyroid hormone on post-ischemic cardiac performance: Potential involvement of Akt and ERK signalings. Mol. Cell. Biochem. 2012, 363, 235–243. [Google Scholar] [CrossRef]
- Ranasinghe, A.M.; Quinn, D.W.; Pagano, D.; Edwards, N.; Faroqui, M.; Graham, T.R.; Keogh, B.E.; Mascaro, J.; Riddington, D.W.; Rooney, S.J.; et al. Glucose-insulin-potassium and tri-iodothyronine individually improve hemodynamic performance and are associated with reduced troponin I release after on-pump coronary artery bypass grafting. Circulation 2006, 114 (Suppl. S1), I245–I250. [Google Scholar] [CrossRef] [Green Version]
- Ntari, L.; Mantzouratou, P.; Katsaouni, A.; Pantos, C.; Kollias, G.; Mourouzis, I. Changes in Thyroid Hormone Signaling Mediate Cardiac Dysfunction in the Tg197 Mouse Model of Arthritis: Potential Therapeutic Implications. J. Clin. Med. 2021, 10, 5512. [Google Scholar] [CrossRef]
- Pantos, C.; Xinaris, C.; Mourouzis, I.; Kokkinos, A.D.; Cokkinos, D.V. TNF-alpha administration in neonatal cardiomyocytes is associated with differential expression of thyroid hormone receptors: A response prevented by T3. Horm. Metab. Res. 2008, 40, 731–734. [Google Scholar] [CrossRef]
- Baldelli, R.; Nicastri, E.; Petrosillo, N.; Marchioni, L.; Gubbiotti, A.; Sperduti, I.; Di Giacinto, P.; Rizza, L.; Rota, F.; Franco, M.; et al. Thyroid dysfunction in COVID-19 patients. J. Endocrinol. Investig. 2021, 44, 2735–2739. [Google Scholar] [CrossRef]
- Lui, D.T.W.; Lee, C.H.; Chow, W.S.; Lee, A.C.H.; Tam, A.R.; Fong, C.H.Y.; Law, C.Y.; Leung, E.K.H.; To, K.K.W.; Tan, K.C.B.; et al. Thyroid Dysfunction in Relation to Immune Profile, Disease Status, and Outcome in 191 Patients with COVID-19. J. Clin. Endocrinol. Metab. 2021, 106, e926–e935. [Google Scholar] [CrossRef]
- Vassiliadi, D.A.; Ilias, I.; Pratikaki, M.; Jahaj, E.; Vassiliou, A.G.; Detsika, M.; Ampelakiotou, K.; Koulenti, M.; Manolopoulos, K.N.; Tsipilis, S.; et al. Thyroid hormone alterations in critically and non-critically ill patients with SARS-CoV-2 infection. Endocr. Connect. 2021, 10, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Jevalikar, G.; Sharma, R.; Farooqui, K.J.; Mahendru, S.; Dewan, A.; Bhudiraja, S.; Mithal, A. Low FT3 is an independent marker of disease severity in patients hospitalized for COVID-19. Endocr. Connect. 2021, 10, 1455–1462. [Google Scholar] [CrossRef]
- Gao, W.; Guo, W.; Guo, Y.; Shi, M.; Dong, G.; Wang, G.A.; Ge, Q.; Zhu, J.; Zhou, X. Thyroid hormone concentrations in severely or critically ill patients with COVID-19. J. Endocrinol. Investig. 2021, 44, 1031–1040. [Google Scholar] [CrossRef]
- Schwarz, Y.; Percik, R.; Oberman, B.; Yaffe, D.; Zimlichman, E.; Tirosh, A. Sick Euthyroid Syndrome on Presentation of Patients With COVID-19: A Potential Marker for Disease Severity. Endocr. Pract. 2021, 27, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Mehmet Güven, H.G. The prognostic impact of thyroid disorders on the clinical severity of COVID-19: Results of single-centre pandemic hospital. Int. J. Clin. Pract. 2021, 75, e14129. [Google Scholar]
- Chen, M.; Zhou, W.; Xu, W. Thyroid Function Analysis in 50 Patients with COVID-19: A Retrospective Study. Thyroid 2021, 31, 38–11. [Google Scholar] [CrossRef]
- Campi, I.; Bulgarelli, I.; Dubini, A.; Perego, G.B.; Tortorici, E.; Torlasco, C.; Torresani, E.; Rocco, L.; Persani, L.; Fugazzola, L. The spectrum of thyroid function tests during hospitilization for SARS-CoV-2 infection. Eur. J. Endocrinol. 2021, 184, 699–709. [Google Scholar] [CrossRef]
- Gong, J.; Wang, D.K.; Dong, H.; Xia, Q.S.; Huang, Z.Y.; Zhao, Y.; Chen, X.; Yuan, F.; Li, J.B.; Lu, F.E. Prognostic significance of low TSH concentration in patients with COVID-19 presenting with non-thyroidal illness syndrome. BMC Endocr. Disord. 2021, 21, 111. [Google Scholar] [CrossRef]
- Lang, S.; Liu, Y.; Qu, X.; Lu, R.; Fu, W.; Zhang, W.; Wang, H.; Hong, T. Association between Thyroid Function and Prognosis of COVID-19: A Retrospective Observational Study. Endocr. Res. 2021, 46, 170–177. [Google Scholar] [CrossRef]
- Ballesteros Vizoso, M.A.; Castilla, A.F.; Barceló, A.; Raurich, J.M.; Argente del Castillo, P.; Morell-García, D.; Velasco, J.; Pérez-Bárcena, J.; Llompart-Pou, J.A. Thyroid Disfunction in Critically Ill COVID-19 Patients. Relationship with In-Hospital Mortality. J. Clin. Med. 2021, 10, 5057. [Google Scholar] [CrossRef]
- Chen, Y.; Li, X.; Dai, Y.; Zhang, J. The Association Between COVID-19 and Thyroxine Levels: A Meta-Analysis. Front. Endocrinol. 2021, 12, 779692. [Google Scholar] [CrossRef] [PubMed]
- Muller, I.; Cannavaro, D.; Dazzi, D.; Covelli, D.; Mantovani, G.; Muscatello, A.; Ferrante, E.; Orsi, E.; Resi, V.; Longari, V.; et al. SARS-CoV-2-related atypical thyroiditis. Lancet Diabetes Endocrinol. 2020, 8, 739–741. [Google Scholar] [CrossRef]
- Rotondi, M.; Coperchini, F.; Ricci, G.; Denegri, M.; Croce, L.; Ngnitejeu, S.T.; Villani, L.; Magri, F.; Latrofa, F.; Chiovato, L. Detection of SARS-CoV-2 receptor ACE-2 mRNA in thyroid cells: A clue for COVID-19-related subacute thyroiditis. J. Endocrinol. Investig. 2021, 44, 1085–1090. [Google Scholar] [CrossRef] [PubMed]
- Samuels, M.H.; McDaniel, P.A. Thyrotropin levels during hydrocortisone infusions that mimic fasting-induced cortisol elevations: A clinical research center study. J. Clin. Endocrinol. Metab. 1997, 82, 3700–3704. [Google Scholar] [CrossRef]
- Nicoloff, J.T.; Fisher, D.A.; Appleman, M.D., Jr. The role of glucocorticoids in the regulation of thyroid function in man. J. Clin. Investig. 1970, 49, 1922–1929. [Google Scholar] [CrossRef] [Green Version]
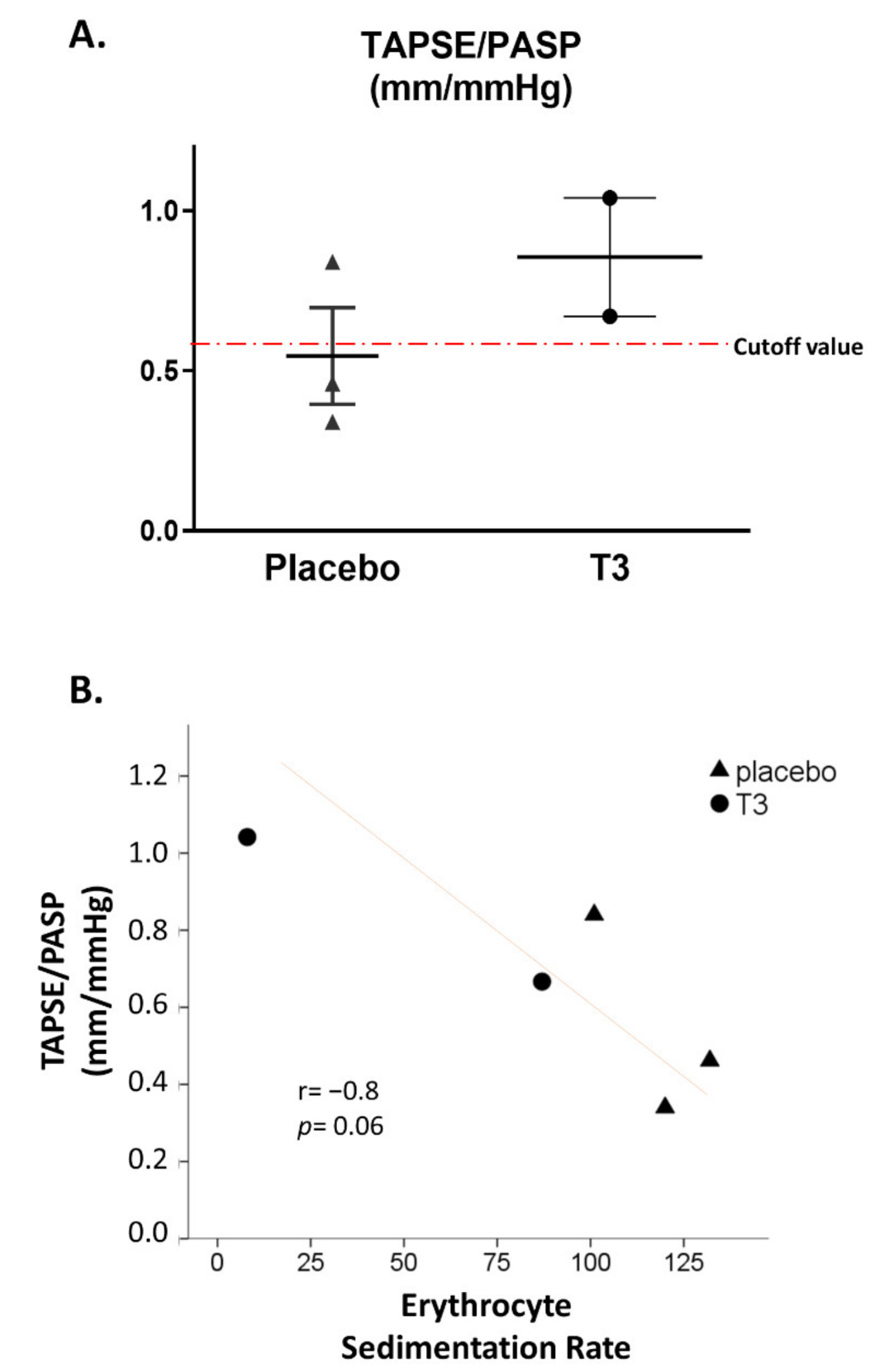
- Pantos, C.; Apostolaki, V.; Kokkinos, L.; Trikas, A.; Mourouzis, I. Acute triiodothyronine treatment and red blood cell sedimentation rate (ESR) in critically ill COVID-19 patients: A novel association? Clin. Hemorheol. Microcirc. 2021, 79, 485–488. [Google Scholar] [CrossRef]
- Paternoster, G.; Bertini, P.; Innelli, P.; Trambaiolo, P.; Landoni, G.; Franchi, F.; Scolletta, S.; Guarracino, F. Right Ventricular Dysfunction in Patients With COVID-19: A Systematic Review and Meta-analysis. J. Cardiothorac. Vasc. Anesth. 2021, 35, 3319–3324. [Google Scholar] [CrossRef]
- D’Alto, M.; Marra, A.M.; Severino, S.; Salzano, A.; Romeo, E.; De Rosa, R.; Stagnaro, F.M.; Pagnano, G.; Verde, R.; Murino, P.; et al. Right ventricular-arterial uncoupling independently predicts survival in COVID-19 ARDS. Crit. Care 2020, 24, 670. [Google Scholar] [CrossRef]
- Bursi, F.; Santangelo, G.; Barbieri, A.; Vella, A.M.; Toriello, F.; Valli, F.; Sansalone, D.; Carugo, S.; Guazzi, M. Impact of Right Ventricular-Pulmonary Circulation Coupling on Mortality in SARS-CoV-2 Infection. J. Am. Heart Assoc. 2022, 11, e023220. [Google Scholar] [CrossRef]
- Contou, D.; Cally, R.; Sarfati, F.; Desaint, P.; Fraisse, M.; Plantefeve, G. Causes and timing of death in critically ill COVID-19 patients. Crit. Care 2021, 25, 79. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Survivors (n = 8) | Non-Survivors (n = 10) | Sign. (p) | |
|---|---|---|---|
| Age (years) | 64.4 (8.7) | 68.1 (12.1) | 0.47 |
| Gender (Male/Female) | 4/4 | 6/4 | 0.67 |
| Co-morbidities | 75% (6/8) | 100% (10/10) | 0.18 |
| Dexamethasone treatment | 100% (8/8) | 80% (8/10) | 0.47 |
| P/F ratio * | 152 (71) | 114 (43) | 0.17 |
| Lactate (mmol/L) | 0.95 (0.33) | 2.35 (3.1) | 0.23 |
| D-Dimers (ng/mL) | 1563 (1403) | 2443 (2869) | 0.41 |
| Fibrinogen (mg/dL) | 315 (329) | 471 (28) | 0.4 |
| WBC (cells × 103) * | 11.85 (5.57) | 13.84 (6.77) | 0.51 |
| Troponin (pg/mL) | 188 (451) | 445 (704) | 0.41 |
| Total T3 (ng/mL) * | 0.46 (0.09) | 0.44 (0.12) | 0.73 |
| Total T4 (μg/dL) * | 7.53 (1.0) | 5.27 (2.1) | 0.027 |
| TSH (μIU/mL) * | 1.0 (1.33) | 0.28 (0.32) | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mourouzis, I.; Apostolaki, V.; Trikas, A.; Kokkinos, L.; Alexandrou, N.; Avdikou, M.; Giannoulopoulou, M.; Vassi, A.; Tseti, I.; Pantos, C. The Potential of Thyroid Hormone Therapy in Severe COVID-19: Rationale and Preliminary Evidence. Int. J. Environ. Res. Public Health 2022, 19, 8063. https://doi.org/10.3390/ijerph19138063
Mourouzis I, Apostolaki V, Trikas A, Kokkinos L, Alexandrou N, Avdikou M, Giannoulopoulou M, Vassi A, Tseti I, Pantos C. The Potential of Thyroid Hormone Therapy in Severe COVID-19: Rationale and Preliminary Evidence. International Journal of Environmental Research and Public Health. 2022; 19(13):8063. https://doi.org/10.3390/ijerph19138063
Chicago/Turabian StyleMourouzis, Iordanis, Vassiliki Apostolaki, Athanasios Trikas, Leonidas Kokkinos, Natassa Alexandrou, Maria Avdikou, Myrto Giannoulopoulou, Aimilia Vassi, Ioulia Tseti, and Constantinos Pantos. 2022. "The Potential of Thyroid Hormone Therapy in Severe COVID-19: Rationale and Preliminary Evidence" International Journal of Environmental Research and Public Health 19, no. 13: 8063. https://doi.org/10.3390/ijerph19138063
APA StyleMourouzis, I., Apostolaki, V., Trikas, A., Kokkinos, L., Alexandrou, N., Avdikou, M., Giannoulopoulou, M., Vassi, A., Tseti, I., & Pantos, C. (2022). The Potential of Thyroid Hormone Therapy in Severe COVID-19: Rationale and Preliminary Evidence. International Journal of Environmental Research and Public Health, 19(13), 8063. https://doi.org/10.3390/ijerph19138063