
Association between Type 2 Diabetes and Classification of Periodontal Disease Severity in Japanese Men and Women: A Cross-Sectional Study


Abstract
:1. Introduction
2. Material and Methods
2.1. Design and Subjects
2.2. Assessment of ABL Using Oral Radiographs and Hs-CRP
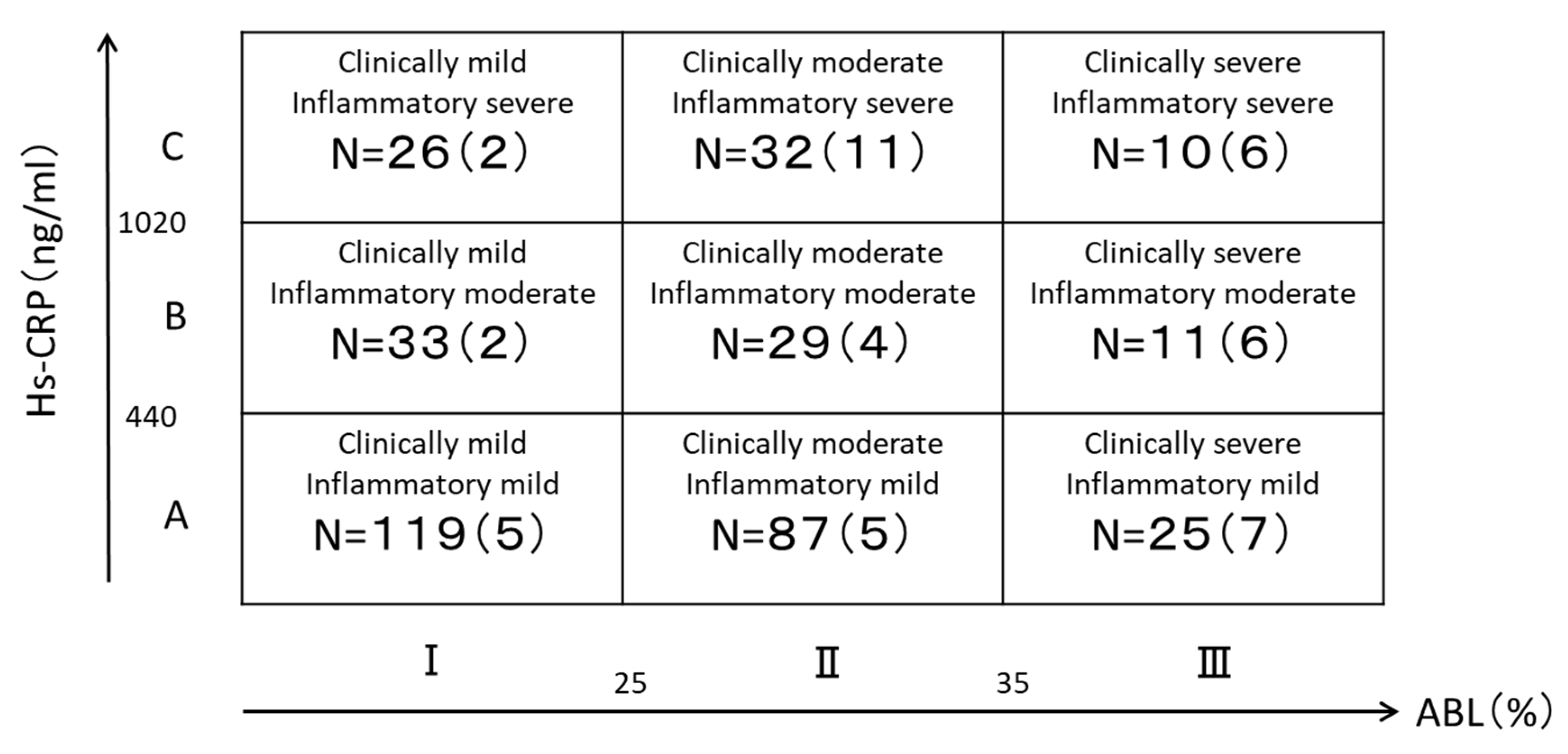
2.3. Classification of Periodontal Disease by Severity
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kidambi, S.; Patel, S.B. Diabetes mellitus: Considerations for dentistry. J. Am. Dent. Assoc. 2008, 139, 8S–18S. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wang, M.; Wang, X.; Qu, H.; Zhang, R.; Gu, J.; Wu, Y.; Ni, T.; Tang, W.; Li, Q. Relationship between periodontitis and microangiopathy in type 2 diabetes mellitus: A meta-analysis. J. Periodontal Res. 2021, 56, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Graziani, F.; Hasturk, H. Effects of periodontal disease on glycemic control, complications, and incidence of diabetes mellitus. Periodontology 2020, 83, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Blanco, J.; Buchalla, W.; Carvalho, J.C.; Dietrich, T.; Dörfer, C.; Eaton, K.A.; Figuero, E.; Frencken, J.E.; Graziani, F.; et al. Prevention and control of dental caries and periodontal diseases at individual and population level: Consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44 (Suppl. S18), S85–S93. [Google Scholar] [CrossRef] [PubMed]
- Meyle, J.; Chapple, I. Molecular aspects of the pathogenesis of periodontitis. Periodontology 2015, 69, 7–17. [Google Scholar] [CrossRef]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J. Clin. Periodontol. 2018, 45, 138–149. [Google Scholar] [CrossRef]
- IDF Diabetes Atlas. Ninth Edition 2019. Available online: https://www.diabetesatlas.org/upload/resources/material/20200302_133351_IDFATLAS9e-final-web.pdf (accessed on 1 May 2022).
- Eke, P.I.; Page, R.C.; Wei, L.; Thornton-Evans, G.; Genco, R.J. Update of the case definitions for population-based surveillance of periodontitis. J. Periodontol. 2012, 83, 1449–1454. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. S1), S159–S172. [Google Scholar] [CrossRef] [Green Version]
- Leroy, R.; Eaton, K.A.; Savage, A. Methodological issues in epidemiological studies of periodontitis--how can it be improved? BMC Oral Health 2010, 10, 8. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, F.; Yamazaki, K.; Nomura, Y.; Minabe, M.; Miyata, T.; Morita, M. Final report of Working Group on classification by severity of periodontal disease. The Periodontal Medicine Committee, the Japanese Society of Periodontology. J. Jpn. Soc. Periodontol. 2011, 53, 197–200. [Google Scholar]
- Mahajan, A.; Tabassum, R.; Chavali, S.; Dwivedi, O.P.; Bharadwaj, M.; Tandon, N.; Bharadwaj, D. High-sensitivity C-reactive protein levels and type 2 diabetes in urban North Indians. J. Clin. Endocrinol. Metab. 2009, 94, 2123–2127. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, M.; Graziani, F.; D’Aiuto, F. Periodontal therapy and cardiovascular risk. Periodontology 2020, 83, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Parsegian, K.; Randall, D.; Curtis, M.; Ioannidou, E. Association between periodontitis and chronic kidney disease. Periodontology 2022, 89, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Kuraji, R.; Sekino, S.; Kapila, Y.; Numabe, Y. Periodontal disease-related nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: An emerging concept of oral-liver axis. Periodontology 2021, 87, 204–240. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.S.; Obst, C.; Zehaczek, S.; Geenen, C. Detection of bone loss with different X-ray techniques in periodontal patients. J. Periodontol. 2008, 79, 1141–1149. [Google Scholar] [CrossRef]
- Bassiouny, M.A.; Grant, A.A. The accuracy of the Schei ruler: A laboratory investigation. J. Periodontol. 1975, 46, 748–752. [Google Scholar] [CrossRef]
- Swets, J.A. Measuring the accuracy of diagnostic systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [Green Version]
- Demmer, R.T.; Desvarieux, M.; Holtfreter, B.; Jacobs, D.R., Jr.; Wallaschofski, H.; Nauck, M.; Völzke, H.; Kocher, T. Periodontal status and A1C change: Longitudinal results from the study of health in Pomerania (SHIP). Diabetes Care 2010, 33, 1037–1043. [Google Scholar] [CrossRef] [Green Version]
- Collin, H.L.; Uusitupa, M.; Niskanen, L.; Kontturi-Närhi, V.; Markkanen, H.; Koivisto, A.M.; Meurman, J.H. Periodontal findings in elderly patients with non-insulin dependent diabetes mellitus. J. Periodontol. 1998, 69, 962–966. [Google Scholar] [CrossRef]
- Saito, T.; Shimazaki, Y.; Kiyohara, Y.; Kato, I.; Kubo, M.; Iida, M.; Koga, T. The severity of periodontal disease is associated with the development of glucose intolerance in non-diabetics: The Hisayama study. J. Dent. Res. 2004, 83, 485–490. [Google Scholar] [CrossRef]
- Saremi, A.; Nelson, R.G.; Tulloch-Reid, M.; Hanson, R.L.; Sievers, M.L.; Taylor, G.W.; Shlossman, M.; Bennett, P.H.; Genco, R.; Knowler, W.C. Periodontal disease and mortality in type 2 diabetes. Diabetes Care 2005, 28, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shultis, W.A.; Weil, E.J.; Looker, H.C.; Curtis, J.M.; Shlossman, M.; Genco, R.J.; Knowler, W.C.; Nelson, R.G. Effect of periodontitis on overt nephropathy and end-stage renal disease in type 2 diabetes. Diabetes Care 2007, 30, 306–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soskolne, W.A.; Klinger, A. The relationship between periodontal diseases and diabetes: An overview. Ann. Periodontol. 2001, 6, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Demmer, R.T.; Jacobs, D.R., Jr.; Desvarieux, M. Periodontal disease and incident type 2 diabetes: Results from the First National Health and Nutrition Examination Survey and its epidemiologic follow-up study. Diabetes Care 2008, 31, 1373–1379. [Google Scholar] [CrossRef] [Green Version]
- Taylor, G.W.; Burt, B.A.; Becker, M.P.; Genco, R.J.; Shlossman, M.; Knowler, W.C.; Pettitt, D.J. Severe periodontitis and risk for poor glycemic control in patients with non-insulin-dependent diabetes mellitus. J. Periodontol. 1996, 67, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, V.E.; Kornman, K.S.; Beck, J.D.; Genco, R.; Goldfine, A.; Libby, P.; Offenbacher, S.; Ridker, P.M.; Van Dyke, T.E.; Roberts, W.C. The American Journal of Cardiology and Journal of Periodontology Editors’ Consensus: Periodontitis and atherosclerotic cardiovascular disease. Am. J. Cardiol. 2009, 104, 59–68. [Google Scholar] [CrossRef]
- Nakarai, H.; Yamashita, A.; Takagi, M.; Adachi, M.; Sugiyama, M.; Noda, H.; Katano, M.; Yamakawa, R.; Nakayama, K.; Takumiya, H.; et al. Periodontal disease and hypertriglyceridemia in Japanese subjects: Potential association with enhanced lipolysis. Metabolism 2011, 60, 823–829. [Google Scholar] [CrossRef]
- Nakajima, T.; Honda, T.; Domon, H.; Okui, T.; Kajita, K.; Ito, H.; Takahashi, N.; Maekawa, T.; Tabeta, K.; Yamazaki, K. Periodontitis-associated up-regulation of systemic inflammatory mediator level may increase the risk of coronary heart disease. J. Periodontal Res. 2010, 45, 116–122. [Google Scholar] [CrossRef]
- Arima, H.; Kubo, M.; Yonemoto, K.; Doi, Y.; Ninomiya, T.; Tanizaki, Y.; Hata, J.; Matsumura, K.; Iida, M.; Kiyohara, Y. High-sensitivity C-reactive protein and coronary heart disease in a general population of Japanese: The Hisayama study. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1385–1391. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, F.; Taniguchi, A.; Iwamoto, Y.; Soga, Y.; Fukushima, M.; Nagasaka, S.; Nakai, Y.; Murayama, Y. Porphyromonas gingivalis infection is associated with elevated C-reactive protein in nonobese Japanese type 2 diabetic subjects. Diabetes Care 2002, 25, 1888. [Google Scholar] [CrossRef] [Green Version]
- Dewake, N.; Ishioka, Y.; Uchida, K.; Taguchi, A.; Higashi, Y.; Yoshida, A.; Yoshinari, N. Association between Carotid Artery Calcification and Periodontal Disease Progression in Japanese Men and Women: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 3365. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Type 2 Diabetes (N = 48) | Non-Diabetic (N = 324) | p-Value | |
|---|---|---|---|
| Age (years) | 62.6 ± 9.8 | 51.8 ± 11.4 | <0.001 |
| Sex | |||
| Male | 39 (15.5) | 213 (84.5) | 0.032 |
| Female | 9 (7.5) | 111 (92.5) | |
| BMI (kg/m2) | 25.1 ± 4.2 | 22.9 ± 3.6 | 0.001 |
| Smoking | |||
| Yes | 12 (17.1) | 58 (82.9) | 0.239 |
| No | 36 (11.9) | 266 (88.1) | |
| Number of teeth | 22.2 ± 5.3 | 25.7 ± 3.9 | <0.001 |
| ABL (%) | 34.3 ± 11.7 | 25.6 ± 7.5 | <0.001 |
| Ⅰ | 9 (5.1) | 169 (94.9) | <0.001 |
| Ⅱ | 20 (13.5) | 128 (86.5) | |
| Ⅲ | 19 (41.3) | 27 (58.7) | |
| Hs-CRP (ng/mL) | 1269.4 ± 1690.2 | 587.5 ± 966.4 | <0.001 |
| A | 17 (7.4) | 214 (92.6) | <0.001 |
| B | 12 (16.4) | 61 (83.6) | |
| C | 19 (27.9) | 49 (72.1) | |
| Classification of periodontal disease severity | |||
| ⅠA | 5 (4.2) | 114 (95.8) | <0.001 |
| ⅠB | 2 (6.1) | 31 (93.9) | |
| ⅠC | 2 (7.7) | 24 (92.3) | |
| ⅡA | 5 (5.7) | 82 (94.3) | |
| ⅡB | 4 (13.8) | 25 (86.2) | |
| ⅡC | 11 (34.4) | 21 (65.6) | |
| ⅢA | 7 (28.0) | 18 (72.0) | |
| ⅢB | 6 (54.5) | 5 (45.5) | |
| ⅢC | 6 (60.0) | 4 (40.0) | |
| Odds Ratio | 95%CI | p-Value | |
|---|---|---|---|
| Age (years) | 1.082 | 1.042–1.124 | <0.001 |
| BMI (kg/m2) | 1.175 | 1.061–1.301 | 0.002 |
| Classification of periodontal disease severity | |||
| ⅠA (reference) | 1.000 | ||
| ⅠB | 1.132 | 0.196–6.535 | 0.890 |
| ⅠC | 0.831 | 0.141–4.948 | 0.839 |
| ⅡA | 0.955 | 0.254–3.590 | 0.946 |
| ⅡB | 2.100 | 0.489–9.023 | 0.319 |
| ⅡC | 3.582 | 0.988–12.986 | 0.052 |
| ⅢA | 5.108 | 1.346–19.381 | 0.017 |
| ⅢB | 9.626 | 1.950–47.528 | 0.005 |
| ⅢC | 12.386 | 2.464–62.276 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dewake, N.; Iwasaki, Y.; Taguchi, A.; Udagawa, N.; Yoshinari, N. Association between Type 2 Diabetes and Classification of Periodontal Disease Severity in Japanese Men and Women: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 8134. https://doi.org/10.3390/ijerph19138134
Dewake N, Iwasaki Y, Taguchi A, Udagawa N, Yoshinari N. Association between Type 2 Diabetes and Classification of Periodontal Disease Severity in Japanese Men and Women: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(13):8134. https://doi.org/10.3390/ijerph19138134
Chicago/Turabian StyleDewake, Nanae, Yukiko Iwasaki, Akira Taguchi, Nobuyuki Udagawa, and Nobuo Yoshinari. 2022. "Association between Type 2 Diabetes and Classification of Periodontal Disease Severity in Japanese Men and Women: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 13: 8134. https://doi.org/10.3390/ijerph19138134
APA StyleDewake, N., Iwasaki, Y., Taguchi, A., Udagawa, N., & Yoshinari, N. (2022). Association between Type 2 Diabetes and Classification of Periodontal Disease Severity in Japanese Men and Women: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(13), 8134. https://doi.org/10.3390/ijerph19138134