
Relevant Strength Parameters to Allow Return to Running after Primary Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
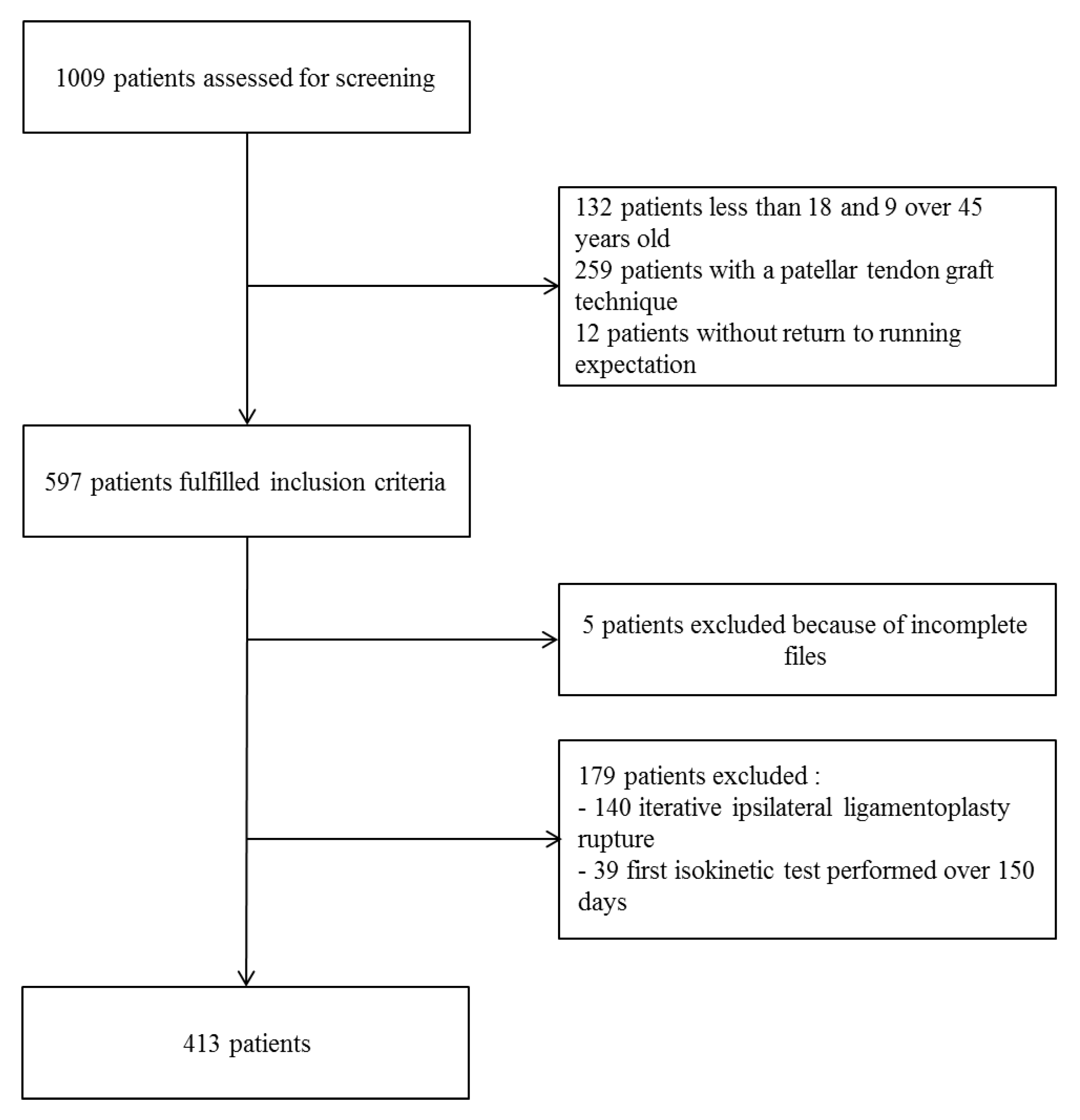
2.1. Participants
2.2. Surgical Procedure
2.3. Rehabilitation Protocol
- -
- Treatment of knee-swelling, edema, and pain by compression, icing, and non-steroidal anti-inflammatory drugs until complete swelling and heat resorption.
- -
- Limitation of standing and walking in order to limit knee-swelling and pain.
- -
- Full weight-bearing allowed with crutches.
- -
- Use of knee brace until full active knee extension was achieved.
- -
- Progressive recovery of knee range of motion with special care for preserving full active knee extension throughout the process.
- -
- Stop using crutches when the gait is well-balanced after proprioception exercises.
- -
- Possibility of driving a car or returning to professional sedentary activities when walking without crutches was achieved.
- -
- Return to cycling when knee range of motion was at least 0 to 120 degrees of knee flexion. A progressive protocol was given to all patients: cycling was practiced 3 times a week from 15 min to 90 min sessions over a 2-month period until the first isokinetic test.
2.4. Isokinetic Evaluation Procedure
2.5. Follow-Up
2.6. Decision-Making Process to Allow a Return to Running
- -
- If the Q-LSI at 60°/s was ≥60%, an RTR was allowed at moderate intensity (70% of maximum heart rate) 3 times a week from 15 to 30 min continuous sessions in the first month. In the second month, 3 sessions were proposed: 2 sessions of 1 to 2 min interval training at up to 85% of maximal heart rate, and one session with 10 × 50 to 100 m progressive acceleration. A written program was given to the participants and they were encouraged to buy a heart rate monitor to self-monitor their running intensity.
- -
- If the Q-LSI was <60% but >50%, an RTR was not allowed and only cycling was prescribed. If the Q-LSI was <50%, only swimming, including breaststroke, was allowed. Physiotherapy care was prescribed only if the total knee range of motion was not achieved.
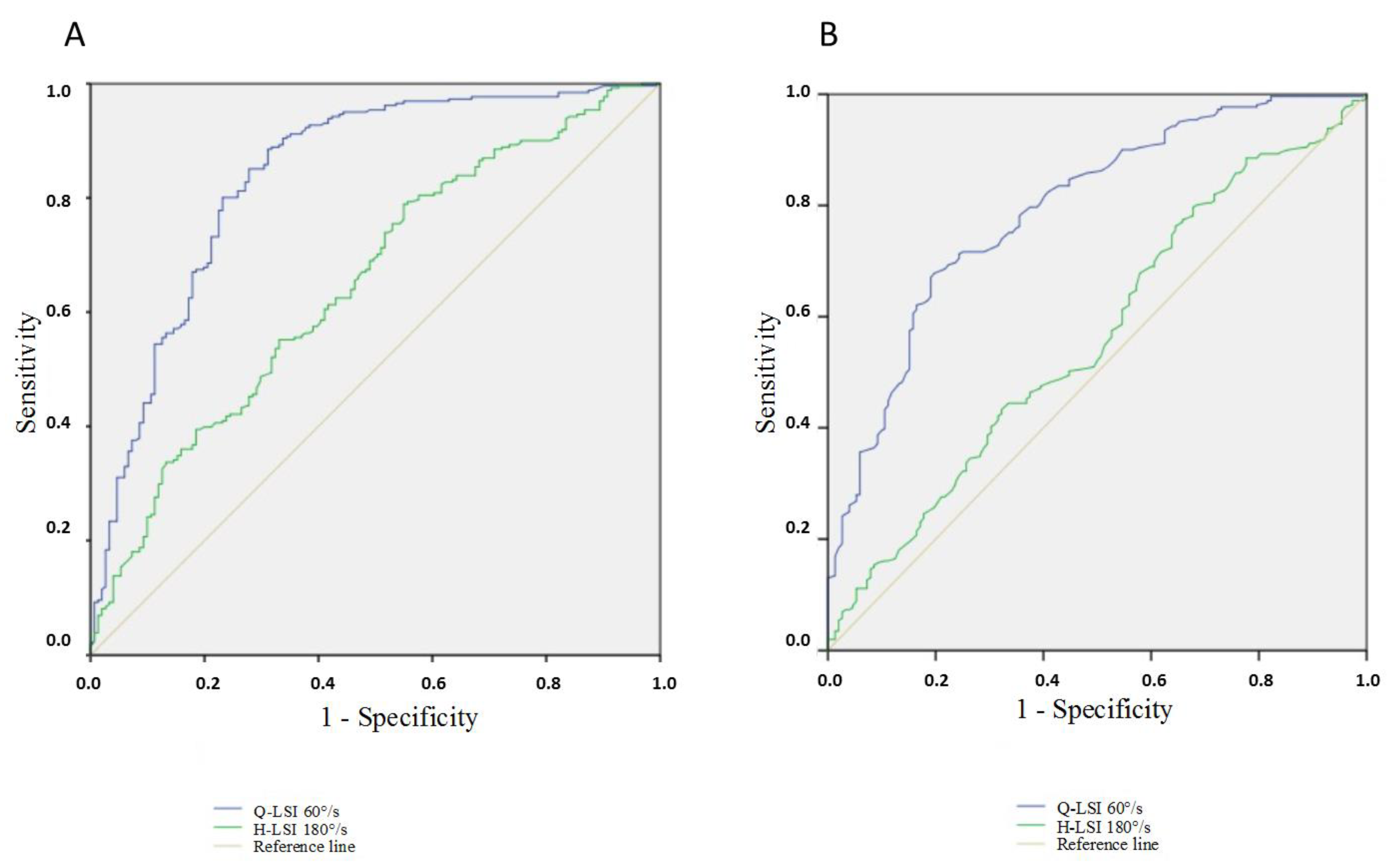
2.7. Statistical Analyses
3. Results
3.1. Comparison of the Return-to-Running and the No-Return-to-Running Populations
3.2. Univariate Analysis
3.3. Multivariate Analysis: Wald Logistic Regression
3.3.1. First Model Taking into Account Patients as Unit (Limb Symmetry Indexes)
3.3.2. Second Model Taking into Account Limbs (Operated/Contralateral) as Unit of Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, S.B.; Sekiya, J.K. Allograft Safety in Anterior Cruciate Ligament Reconstruction. Clin. Sports Med. 2007, 26, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Purnell, M.L.; Larson, A.I.; Clancy, W. Anterior Cruciate Ligament Insertions on the Tibia and Femur and Their Relationships to Critical Bony Landmarks Using High-Resolution Volume-Rendering Computed Tomography. Am. J. Sports Med. 2008, 36, 2083–2090. [Google Scholar] [CrossRef] [PubMed]
- Noyes, F.R. Noyes’ Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Quatman, C.E.; Quatman-Yates, C.C.; Hewett, T.E. A “plane” Explanation of Anterior Cruciate Ligament Injury Mechanisms: A Systematic Review. Sports Med. Auckl. NZ 2010, 40, 729–746. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Holme, I. Risk Factors for Sports Injuries—A Methodological Approach. Br. J. Sports Med. 2003, 37, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fifty-Five per Cent Return to Competitive Sport Following Anterior Cruciate Ligament Reconstruction Surgery: An Updated Systematic Review and Meta-Analysis Including Aspects of Physical Functioning and Contextual Factors. Br. J. Sports Med. 2014, 48, 1543–1552. [Google Scholar] [CrossRef] [Green Version]
- Ardern, C.L.; Glasgow, P.; Schneiders, A.; Witvrouw, E.; Clarsen, B.; Cools, A.; Gojanovic, B.; Griffin, S.; Khan, K.M.; Moksnes, H.; et al. 2016 Consensus Statement on Return to Sport from the First World Congress in Sports Physical Therapy, Bern. Br. J. Sports Med. 2016, 50, 853–864. [Google Scholar] [CrossRef] [Green Version]
- Kyritsis, P.; Bahr, R.; Landreau, P.; Miladi, R.; Witvrouw, E. Likelihood of ACL Graft Rupture: Not Meeting Six Clinical Discharge Criteria before Return to Sport Is Associated with a Four Times Greater Risk of Rupture. Br. J. Sports Med. 2016, 50, 946–951. [Google Scholar] [CrossRef]
- Pires, N.J.; Lay, B.S.; Rubenson, J. Joint-Level Mechanics of the Walk-to-Run Transition in Humans. J. Exp. Biol. 2014, 217, 3519–3527. [Google Scholar] [CrossRef] [Green Version]
- Takeda, K.; Hasegawa, T.; Kiriyama, Y.; Matsumoto, H.; Otani, T.; Toyama, Y.; Nagura, T. Kinematic Motion of the Anterior Cruciate Ligament Deficient Knee during Functionally High and Low Demanding Tasks. J. Biomech. 2014, 47, 2526–2530. [Google Scholar] [CrossRef]
- Stearns, K.M.; Pollard, C.D. Abnormal Frontal Plane Knee Mechanics during Sidestep Cutting in Female Soccer Athletes after Anterior Cruciate Ligament Reconstruction and Return to Sport. Am. J. Sports Med. 2013, 41, 918–923. [Google Scholar] [CrossRef]
- Petersen, W.; Taheri, P.; Forkel, P.; Zantop, T. Return to Play Following ACL Reconstruction: A Systematic Review about Strength Deficits. Arch. Orthop. Trauma Surg. 2014, 134, 1417–1428. [Google Scholar] [CrossRef] [PubMed]
- Lewek, M.; Rudolph, K.; Axe, M.; Snyder-Mackler, L. The Effect of Insufficient Quadriceps Strength on Gait after Anterior Cruciate Ligament Reconstruction. Clin. Biomech. 2002, 17, 56–63. [Google Scholar] [CrossRef]
- Rambaud, A.J.M.; Ardern, C.L.; Thoreux, P.; Regnaux, J.-P.; Edouard, P. Criteria for Return to Running after Anterior Cruciate Ligament Reconstruction: A Scoping Review. Br. J. Sports Med. 2018, 52, 1437–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dauty, M.; Edouard, P.; Menu, P.; Mesland, O.; Fouasson-Chailloux, A. Isokinetic Quadriceps Symmetry Helps in the Decision to Return to Running after Anterior Cruciate Ligament Reconstruction. Ann. Phys. Rehabil. Med. 2021, 65, 101543. [Google Scholar] [CrossRef]
- Iwame, T.; Matsuura, T.; Okahisa, T.; Katsuura-Kamano, S.; Wada, K.; Iwase, J.; Sairyo, K. Quadriceps Strength to Body Weight Ratio Is a Significant Indicator for Initiating Jogging after Anterior Cruciate Ligament Reconstruction. Knee 2021, 28, 240–246. [Google Scholar] [CrossRef]
- Dauty, M.; Menu, P.; Garraud, T.; Mesland, O.; Berlivet, T.; Metayer, B.; Fouasson-Chailloux, A. Jumper’s Knee Mechanical Consequences in Professional Basketball Players: The “Camel’s Back Curve”. Eur. J. Appl. Physiol. 2019, 119, 735–742. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Bizzini, M.; Rampinini, E.; Cereda, F.; Maffiuletti, N.A. Reliability of Isokinetic Strength Imbalance Ratios Measured Using the Cybex NORM Dynamometer. Clin. Physiol. Funct. Imaging 2008, 28, 113–119. [Google Scholar] [CrossRef]
- Tegner, Y.; Lysholm, J. Rating Systems in the Evaluation of Knee Ligament Injuries. Clin. Orthop. 1985, 198, 43–49. [Google Scholar] [CrossRef]
- Deeks, J. When Can Odds Ratios Mislead? Odds Ratios Should Be Used Only in Case-Control Studies and Logistic Regression Analyses. BMJ 1998, 317, 1155–1156, author reply 1156–1157. [Google Scholar] [CrossRef]
- Stoltzfus, J.C. Logistic Regression: A Brief Primer. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2011, 18, 1099–1104. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Statistics Notes: Diagnostic Tests 3: Receiver Operating Characteristic Plots. BMJ 1994, 309, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youden, W.J. Index for Rating Diagnostic Tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal Cut-Point and Its Corresponding Youden Index to Discriminate Individuals Using Pooled Blood Samples. Epidemiol. Camb. Mass 2005, 16, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Dauty, M.; Menu, P.; Mesland, O.; Fouasson-Chailloux, A. Arthrogenic Muscle Inhibition and Return to Sport after Arthrofibrosis Complicating Anterior Cruciate Ligament Surgery. Eur. J. Sport Sci. 2021, 22, 627–635. [Google Scholar] [CrossRef]
- Lepley, A.S.; Pietrosimone, B.; Cormier, M.L. Quadriceps Function, Knee Pain, and Self-Reported Outcomes in Patients with Anterior Cruciate Ligament Reconstruction. J. Athl. Train. 2018, 53, 337–346. [Google Scholar] [CrossRef] [Green Version]
- Zwolski, C.; Schmitt, L.C.; Quatman-Yates, C.; Thomas, S.; Hewett, T.E.; Paterno, M.V. The Influence of Quadriceps Strength Asymmetry on Patient-Reported Function at Time of Return to Sport after Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2015, 43, 2242–2249. [Google Scholar] [CrossRef]
- Rice, D.A.; McNair, P.J. Quadriceps Arthrogenic Muscle Inhibition: Neural Mechanisms and Treatment Perspectives. Semin. Arthritis Rheum. 2010, 40, 250–266. [Google Scholar] [CrossRef]
- Knurr, K.A.; Kliethermes, S.A.; Stiffler-Joachim, M.R.; Cobian, D.G.; Baer, G.S.; Heiderscheit, B.C. Running Biomechanics Before Injury and 1 Year After Anterior Cruciate Ligament Reconstruction in Division I Collegiate Athletes. Am. J. Sports Med. 2021, 49, 2607–2614. [Google Scholar] [CrossRef]
- Goerger, B.M.; Marshall, S.W.; Beutler, A.I.; Blackburn, J.T.; Wilckens, J.H.; Padua, D.A. Anterior Cruciate Ligament Injury Alters Preinjury Lower Extremity Biomechanics in the Injured and Uninjured Leg: The JUMP-ACL Study. Br. J. Sports Med. 2015, 49, 188–195. [Google Scholar] [CrossRef]
- Sigward, S.M.; Chan, M.-S.M.; Lin, P.E.; Almansouri, S.Y.; Pratt, K.A. Compensatory Strategies That Reduce Knee Extensor Demand During a Bilateral Squat Change From 3 to 5 Months Following Anterior Cruciate Ligament Reconstruction. J. Orthop. Sports Phys. Ther. 2018, 48, 713–718. [Google Scholar] [CrossRef]
- Boggess, G.; Morgan, K.; Johnson, D.; Ireland, M.L.; Reinbolt, J.A.; Noehren, B. Neuromuscular Compensatory Strategies at the Trunk and Lower Limb Are Not Resolved Following an ACL Reconstruction. Gait Posture 2018, 60, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Di Stasi, S.L.; Logerstedt, D.; Gardinier, E.S.; Snyder-Mackler, L. Gait Patterns Differ Between ACL-Reconstructed Athletes Who Pass Return-to-Sport Criteria and Those Who Fail. Am. J. Sports Med. 2013, 41, 1310–1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmieri-Smith, R.M.; Lepley, L.K. Quadriceps Strength Asymmetry after Anterior Cruciate Ligament Reconstruction Alters Knee Joint Biomechanics and Functional Performance at Time of Return to Activity. Am. J. Sports Med. 2015, 43, 1662–1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiemstra, L.A.; Webber, S.; MacDonald, P.B.; Kriellaars, D.J. Contralateral Limb Strength Deficits after Anterior Cruciate Ligament Reconstruction Using a Hamstring Tendon Graft. Clin. Biomech. Bristol Avon 2007, 22, 543–550. [Google Scholar] [CrossRef]
- Urbach, D.; Nebelung, W.; Becker, R.; Awiszus, F. Effects of Reconstruction of the Anterior Cruciate Ligament on Voluntary Activation of Quadriceps Femoris a Prospective Twitch Interpolation Study. J. Bone Jt. Surg. Br. 2001, 83, 1104–1110. [Google Scholar] [CrossRef]
- Chung, K.S.; Ha, J.K.; Yeom, C.H.; Ra, H.J.; Lim, J.W.; Kwon, M.S.; Kim, J.G. Are Muscle Strength and Function of the Uninjured Lower Limb Weakened After Anterior Cruciate Ligament Injury? Two-Year Follow-up after Reconstruction. Am. J. Sports Med. 2015, 43, 3013–3021. [Google Scholar] [CrossRef]
- Wellsandt, E.; Failla, M.; Snyder-Mackler, L. Limb Symmetry Indexes Can Overestimate Knee Function after ACL Injury. J. Orthop. Sports Phys. Ther. 2017, 47, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Dauty, M.; Tortellier, L.; Rochcongar, P. Isokinetic and Anterior Cruciate Ligament Reconstruction with Hamstrings or Patella Tendon Graft: Analysis of Literature. Int. J. Sports Med. 2005, 26, 599–606. [Google Scholar] [CrossRef]
- Perumal, S.; Thiyagarajan, K.A.; Prakash, A.; Arumugam, S. Evaluation of Regeneration of Semitendinosus Tendon Using Ultrasound Imaging and Isokinetic Strength Testing after Graft Harvest for Arthroscopic Anterior Cruciate Ligament Reconstruction. J. Orthop. 2020, 21, 340–344. [Google Scholar] [CrossRef]
- Fouasson-Chailloux, A.; Menu, P.; Mesland, O.; Dauty, M. Strength Assessment after Proximal Hamstring Rupture: A Critical Review and Analysis. Clin. Biomech. 2020, 72, 44–51. [Google Scholar] [CrossRef]
- Kitaguchi, T.; Tanaka, Y.; Takeshita, S.; Tsujimoto, N.; Kita, K.; Amano, H.; Kinugasa, K.; Tachibana, Y.; Natsuume, T.; Horibe, S. Importance of Functional Performance and Psychological Readiness for Return to Preinjury Level of Sports 1 Year after ACL Reconstruction in Competitive Athletes. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2020, 28, 2203–2212. [Google Scholar] [CrossRef] [PubMed]
- Fouasson-Chailloux, A.; Crenn, V.; Louguet, B.; Grondin, J.; Menu, P.; Dauty, M. Therapeutic Patient Education after Anterior Cruciate Ligament Reconstruction: Evaluation of the Knowledge and Certitudes with a Self-Report Questionnaire. Healthcare 2022, 10, 934. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.J.; Browning, W.M.; Urband, C.E.; Kluczynski, M.A.; Bisson, L.J. A Systematic Summary of Systematic Reviews on the Topic of the Anterior Cruciate Ligament. Orthop. J. Sports Med. 2016, 4, 2325967116634074. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Total Population n = 413 | RTR n = 261 | NRTR n = 152 | p | |
|---|---|---|---|---|
| Sex, n (%) | 0.824 * | |||
| 123 (29.8) | 79 | 44 | |
| 290 (70.2) | 182 | 108 | |
| Mean age, years ± SD | 26.2 ± 6.3 | 26.1 ± 6.4 | 26.4 ± 6.2 | 0.677 |
| Mean weight, kg ± SD | 73.0 ±13.0 | 73.3 ± 13.6 | 72.6 ± 11.9 | 0.618 |
| Mean height, cm ± SD | 173.9 ± 9.0 | 173.9 ± 10.0 | 173.9 ± 7.7 | 0.963 |
| Delay ACL tear to surgery, days ± SD | 197.2 ± 295.5 | 212 ± 284 | 173 ± 317 | 0.206 |
| Delay surgery to isokinetic test, days ± SD | 124.9 ± 20.2 | 125 ± 20.8 | 124 ± 19.3 | 0.899 |
| Meniscal procedure, n (%) | 0.522 * | |||
| 50 (12.1) | 31 (11.9%) | 18 (11.8%) | |
| 39 (9.5) | 24 (9.1%) | 15 (9.9%) | |
| 15 (3.6) | 8 (3.1%) | 8 (5.3%) | |
| 104 (25.2) | 63 (24.1) | 41 (27.0) | |
| No meniscal procedure | 309 (74.8) | 198 (75.9) | 111 (73.0) | |
| Type of reeducation, n (%) | 0.218 * | |||
| 239 (57.9) | 157 (60.2) | 82 (53.9) | |
| 174 (42.1) | 104 (39.8) | 70 (46.1) |
| RTR | NRTR | Mean Difference | CI95% | p | |
|---|---|---|---|---|---|
| Clinical features: | |||||
| Mean Lysholm score | 94.40 | 89.50 | −4.90 | [−6.80; −3.00] | <0.001 |
| Isokinetic parameters: | |||||
| QS/BW 60°/s | |||||
| 2.06 | 1.38 | −0.68 | [−0.81; −0.55] | <0.001 |
| 2.75 | 2.59 | −0.15 | [−0.32; 0.02] | 0.08 |
| QS/BW 180°/s | |||||
| 1.44 | 1.04 | −0.40 | [−0.49; −0.31] | <0.001 |
| 1.79 | 1.68 | −0.10 | [−0.21; 0.004] | 0.060 |
| HS/BW 60°/s/kg | |||||
| 1.25 | 1.05 | −0.20 | [−0.29; −0.11] | <0.001 |
| 1.50 | 1.42 | −0.08 | [−0.17; 0.02] | 0.114 |
| HS/BW 180°/s/kg | |||||
| 0.93 | 0.79 | −0.14 | [−0.21; −0.08] | <0.001 |
| 1.10 | 1.04 | −0.06 | [−0.13; 0.01] | 0.098 |
| Q-LSI 60°/s, % | 74.80 | 53.60 | −21.20 | [−24.3; −18.2] | <0.001 |
| Q-LSI 180°/s, % | 80.30 | 62.40 | −17.90 | [−20.9; −14.8] | <0.001 |
| H-LSI 60°/s, % | 84.00 | 73.70 | −10.30 | [−13.3; −7.4] | <0.001 |
| H-LSI 180°/s, % | 85.20 | 75.50 | −9.70 | [−13.1; −6.3] | <0.001 |
| H/Q 60°/s | |||||
| 0.63 | 0.82 | 0.19 | [0.14–0.25] | <0.001 |
| 0.55 | 0.55 | 0.00 | [−0.02; 0.02] | 0.933 |
| H/Q 180°/s | |||||
| - Operated limb | 0.67 | 0.79 | 0.13 | [0.08; 0.17] | < 0.001 |
| - Contralateral limb | 0.62 | 0.63 | 0.00 | [−0.02; 0.03] | 0.668 |
| Complications | Total Population, n (%) | RTR, n (%) | NRTR, n (%) |
|---|---|---|---|
| None | 274 (66.3) | 205 (78.6) * | 69 (45.4) * |
| Arthrofibrosis | 40 (9.7) | 6 (2.3) * | 34 (22.4) * |
| Anterior knee pain | 26 (6.3) | 17 (6.5) * | 26 (17.1) * |
| Postero-internal knee pain | 39 (9.4) | 25 (9.6) | 14 (9.2) |
| Knee joint swelling | 28 (6.8) | 5 (1.9) | 6 (3.9) |
| Knee Infection | 6 (1.5) | 3 (1.1) | 3 (2.0) |
| Prediction | B | Wald | ORs | CI95% | p |
|---|---|---|---|---|---|
| Step 1: | |||||
| Q-LSI 60°/s | 8.57 | 93.2 | 52057 | [1291–49,627] | <0.001 |
| Constant | −5.27 | 75.3 | 0.005 | <0.001 | |
| Step 2: | |||||
| Q-LSI 60°/s | 8.57 | 93.2 | 52057 | [1291–49,627] | <0.001 |
| H-LSI 180°/s | 2.65 | 10.8 | 14.11 | [2.90–68] | 0.001 |
| Constant | −7.13 | 67.0 | 0.001 | <0.001 |
| Prediction | B | Wald | ORs | CI95% | p |
|---|---|---|---|---|---|
| Step 1: | |||||
| QS/BW 60°/s on operated limb | 1.63 | 64.0 | 5.1 | [3.41–7.58] | <0.001 |
| Constant | −2.19 | 41.3 | 0.1 | <0.001 | |
| Step 2: | |||||
| QS/BW 60°/s on operated leg | 1.63 | 64.0 | 5.1 | [3.41–7.58] | <0.001 |
| QS/BW 60°/s on contralateral limb | −2.25 | 54.8 | 0.1 | [0.06–0.19] | 0.001 |
| Constant | −0.07 | 0.03 | 0.9 | 0.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grondin, J.; Crenn, V.; Gernigon, M.; Quinette, Y.; Louguet, B.; Menu, P.; Fouasson-Chailloux, A.; Dauty, M. Relevant Strength Parameters to Allow Return to Running after Primary Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft. Int. J. Environ. Res. Public Health 2022, 19, 8245. https://doi.org/10.3390/ijerph19148245
Grondin J, Crenn V, Gernigon M, Quinette Y, Louguet B, Menu P, Fouasson-Chailloux A, Dauty M. Relevant Strength Parameters to Allow Return to Running after Primary Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft. International Journal of Environmental Research and Public Health. 2022; 19(14):8245. https://doi.org/10.3390/ijerph19148245
Chicago/Turabian StyleGrondin, Jérôme, Vincent Crenn, Marie Gernigon, Yonis Quinette, Bastien Louguet, Pierre Menu, Alban Fouasson-Chailloux, and Marc Dauty. 2022. "Relevant Strength Parameters to Allow Return to Running after Primary Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft" International Journal of Environmental Research and Public Health 19, no. 14: 8245. https://doi.org/10.3390/ijerph19148245
APA StyleGrondin, J., Crenn, V., Gernigon, M., Quinette, Y., Louguet, B., Menu, P., Fouasson-Chailloux, A., & Dauty, M. (2022). Relevant Strength Parameters to Allow Return to Running after Primary Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft. International Journal of Environmental Research and Public Health, 19(14), 8245. https://doi.org/10.3390/ijerph19148245