
Effectiveness of Two Stress Reduction Interventions in Patients with Chronic Diabetic Foot Ulcers (PSY-DFU): Protocol for a Longitudinal RCT with a Nested Qualitative Study Involving Family Caregivers


Abstract
:1. Background
2. Methods
2.1. Objectives
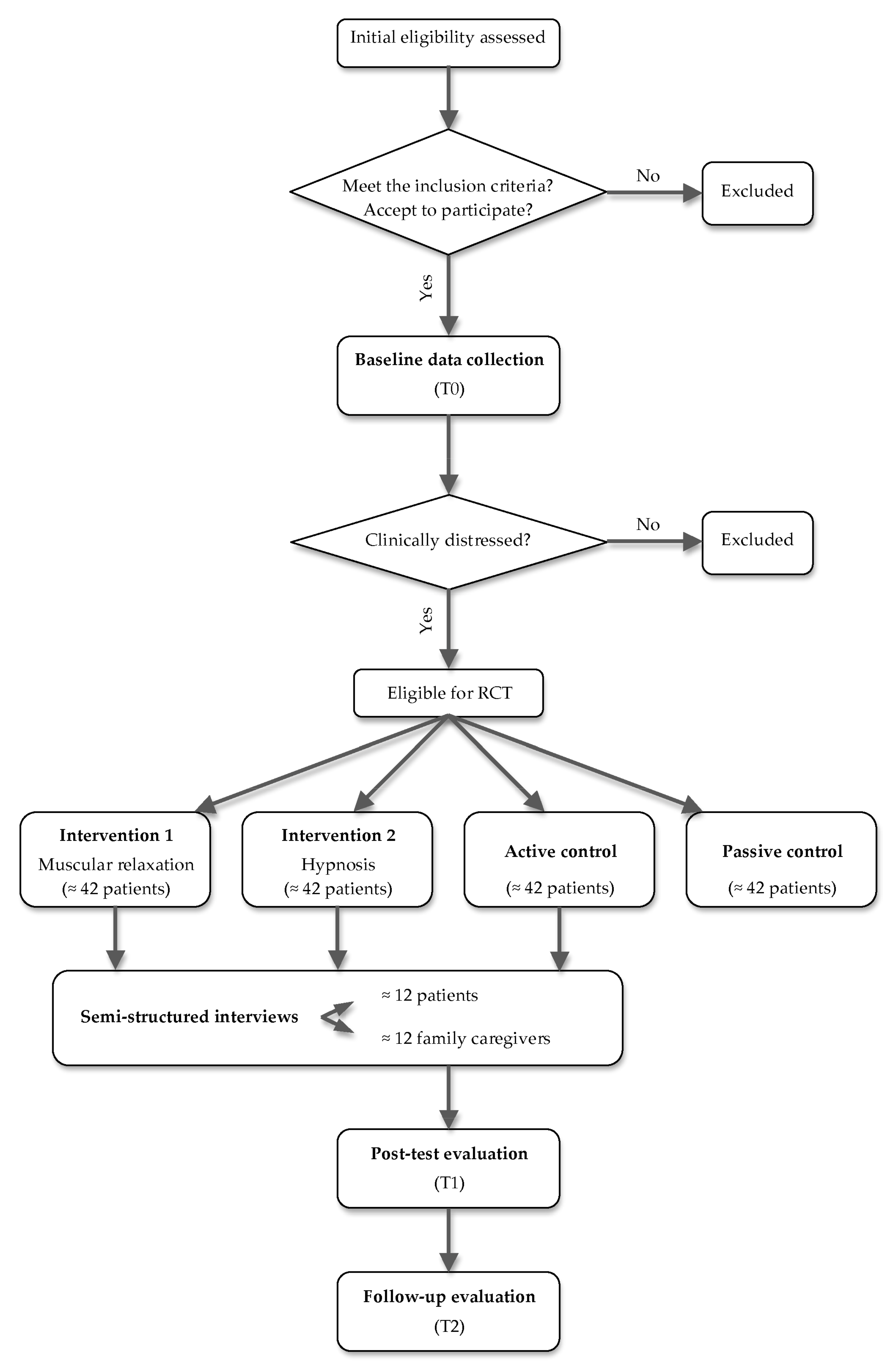
- Assess the effectiveness of a muscle relaxation intervention with guided imagery (TG1) compared to hypnosis with guided imagery (TG2) versus a neutral guided imagery placebo (ACG) and a group that does not receive any psychological intervention (PCG) regarding DFU healing, physiological indicators of healing prognosis, and QoL in patients with clinical distress and a chronic DFU.
- Understand the perspectives of patients and family caregivers on the efficacy of TG1 and TG2 interventions versus ACG sessions for DFU healing.
Primary Specific Aims
2.2. Study Design
2.3. Participant Recruitment and Selection Criteria
2.4. Randomization
3. Outcomes and Measures
3.1. Participant Timeline
3.2. Characteristics of Patients
3.2.1. Sociodemographic Characteristics
3.2.2. Clinical Information
3.3. Measures of Primary Outcomes
3.3.1. Degree of DFU Healing
3.3.2. Physiological Indicators of Healing Prognosis
3.3.3. Impact of the DFU on QoL
3.3.4. Physical and Mental QoL
3.4. Measures of Secondary Outcomes
3.4.1. Perceived Stress
3.4.2. Psychological Morbidity
3.4.3. DFU Representations
3.5. Other Outcome Measures
3.5.1. Health Literacy
3.5.2. Blood Pressure
3.5.3. Heart Rate
3.5.4. Time to Complete Wound Healing
3.5.5. Time to Favorable Healing Prognosis
3.6. Qualitative Assessment
4. Interventions
4.1. Trial Arms
4.1.1. Intervention Groups
4.1.2. Control Groups
4.2. Adherence to the Treatment Plan
5. Statistical Analysis
5.1. Sample Size
5.2. Data Analysis
6. Ethics
7. Discussions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, J.; Ren, Z.H.; Qiang, H.; Wu, J.; Shen, M.; Zhang, L.; Lyu, J. Trends in the incidence of diabetes mellitus: Results from the Global Burden of Disease Study 2017 and implications for diabetes mellitus prevention. BMC Public Health 2020, 20, 1415. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Basel, Switzerland, 2013; Available online: https://diabetesatlas.org/ (accessed on 28 December 2021).
- Pendsey, S.P. Understanding diabetic foot. Int. J. Diabetes Dev. Ctries. 2010, 30, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Jajoo, S.; Shukla, S.; Acharya, S. Educating patients of diabetes mellitus for diabetic foot care. J. Fam. Med. Prim. Care 2020, 9, 367–373. [Google Scholar]
- Hingorani, A.; LaMuraglia, G.M.; Henke, P.; Meissner, M.H.; Loretz, L.; Zinszer, K.M.; Driver, V.R.; Frykberg, R.; Carman, T.L.; Marston, W.; et al. The management of diabetic foot: A clinical practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine. J. Vasc. Surg. 2016, 63, 3S–21S. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis. Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef]
- Polikandrioti, M.; Vasilopoulos, G.; Koutelekos, I.; Panoutsopoulos, G.; Gerogianni, G.; Babatsikou, F.; Zartaloudi, A.; Toulia, G. Quality of Life in Diabetic Foot Ulcer: Associated Factors and the Impact of Anxiety/Depression and Adherence to Self-Care. Int. J. Low. Extrem. Wounds 2020, 19, 165–179. [Google Scholar] [CrossRef]
- Westby, M.; Norman, G.; Vedhara, K.; Game, F.; Cullum, N. Systematic Review or Meta-analysis Psychosocial and behavioural prognostic factors for diabetic foot ulcer development and healing: A systematic review. Diabet. Med. 2020, 37, 1244–1255. [Google Scholar] [CrossRef]
- Jiang, F.H.; Liu, X.; Yu, H.R.; Qian, Y.; Chen, H.L. The Incidence of Depression in Patients With Diabetic Foot Ulcers: A Systematic Review and Meta-Analysis. Int. J. Low. Extrem. Wounds 2020, 19, 165–179. [Google Scholar] [CrossRef]
- Dias, Â.; Ferreira, G.; Vilaça, M.; Pereira, M.G. Quality of Life in Patients with Diabetic Foot Ulcer: A Cross-Sectional Study. Adv. Skin Wound Care 2022. accepted. [Google Scholar]
- Iversen, M.M.; Tell, G.S.; Espehaug, B.; Midthjell, K.; Graue, M.; Rokne, B.; Berge, L.I.; Østbye, T. Is depression a risk factor for diabetic foot ulcers? 11-years follow-up of the Nord-Trøndelag Health Study (HUNT). J. Diabetes Complicat. 2015, 29, 20–25. [Google Scholar] [CrossRef]
- House, S.L. Psychological Distress and Its Impact on Wound Healing. J. Wound Ostomy Cont. Nurs. 2015, 42, 38–41. [Google Scholar] [CrossRef]
- Morey, J.N.; Boggero, I.A.; Scott, A.B.; Segerstrom, S.C. Current Directions in Stress and Human Immune Function. Curr. Opin. Psychol. 2015, 5, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Seiler, A.; Fagundes, C.P.; Christian, L.M. The Impact of Everyday Stressors on the Immune System and Health. In Stress Challenges and Immunity in Space; Choukèr, A., Ed.; Springer: Cham, Switzerland, 2020; pp. 71–92. [Google Scholar]
- Basu, S.; Goswami, A.G.; David, L.E.; Mudge, E. Psychological Stress on Wound Healing: A Silent Player in a Complex Background. Int. J. Low. Extrem. Wounds 2022, 15347346221077517. [Google Scholar] [CrossRef] [PubMed]
- Janakiram, N.B.; Valerio, M.S.; Goldman, S.M.; Dearth, C.L. The Role of the Inflammatory Response in Mediating Functional Recovery Following Composite Tissue Injuries. Int. J. Mol. Sci. 2021, 22, 13552. [Google Scholar] [CrossRef] [PubMed]
- Biggar, K.K.; Storey, K.B. Functional impact of microRNA regulation in models of extreme stress adaptation. J. Mol. Cell Biol. 2018, 10, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Petkovic, M.; Sørensen, A.E.; Leal, E.C.; Carvalho, E.; Dalgaard, L.T. Mechanistic Actions of microRNAs in Diabetic Wound Healing. Cells 2020, 9, 2228. [Google Scholar] [CrossRef]
- Hilliard, M.E.; Yi-Frazier, J.P.; Hessler, D.; Butler, A.M.; Anderson, B.J.; Jaser, S. Stress and A1c Among People with Diabetes Across the Lifespan. Curr. Diab. Rep. 2016, 16, 67. [Google Scholar] [CrossRef] [Green Version]
- Christman, A.; Selvin, E.; Margolis, D.; Lazarus, G.; Garza, L. Hemoglobin A1c is a Predictor of Healing Rate In Diabetic Wounds. J. Investig. Dermatol. 2011, 131, 2121–2127. [Google Scholar] [CrossRef] [Green Version]
- Fesseha, B.K.; Abularrage, C.J.; Hines, K.F.; Sherman, R.; Frost, P.; Langan, S.; Canner, J.; Likes, K.C.; Hosseini, S.M.; Jack, G.; et al. Association of Hemoglobin A1c and Wound Healing in Diabetic Foot Ulcers. Diabetes Care 2018, 41, 1478–1485. [Google Scholar] [CrossRef] [Green Version]
- Hussain, N.; Said, A. Mindfulness-Based Meditation Versus Progressive Relaxation Meditation: Impact on Chronic Pain in Older Female Patients With Diabetic Neuropathy. J. Evid. Based Integr. Med. 2019, 24, 2515690X19876599. [Google Scholar] [CrossRef] [Green Version]
- Paschali, A.A.; Peppou, L.E.; Benroubi, M. Relaxation training significantly reduced blood glucose levels in patients with type 1 diabetes mellitus. Hormones 2020, 19, 215–222. [Google Scholar] [CrossRef]
- Pombeiro, I.; Moura, J.; Pereira, M.G.; Carvalho, E. Stress-Reducing Psychological Interventions as Adjuvant Therapies for Diabetic Chronic Wounds. Curr. Diabetes Rev. 2021, 18, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Rice, B.I.; Kalker, A.; Schindler, J.; Dixon, R.M. Effect of biofeedback-assisted relaxation training on foot ulcer healing. J. Am. Podiatr. Med. Assoc. 2001, 91, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Deswita, D.; Sahar, J.; Mulyono, S. Impact of coaching and self-hypnosis intervention on blood glucose levels of older adults in Indonesia. Enferm. Clin. 2019, 29, 146–150. [Google Scholar] [CrossRef]
- Ratner, H.; Gross, L.; Casas, J.; Castells, S. A Hypnotherapeutic Approach to the Improvement of Compliance in Adolescent Diabetics. Am. J. Clin. Hypn. 1990, 32, 154–159. [Google Scholar] [CrossRef]
- Rodrigues, F.; Oliveira, C.; Silva, C.F.; D’Almeida, A. Psychotherapy with Hypnosis in glycemia in patients with type 1 Diabetes Mellitus. Eur. Proc. Soc. Behav. Sci. 2017, XXII, 76–88. [Google Scholar]
- Xu, Y.; Cardeña, E. Hypnosis as an Adjunct Therapy in the Management of Diabetes. Int. J. Clin. Exp. Hypn. 2007, 56, 63–72. [Google Scholar] [CrossRef]
- McGloin, H.; Devane, D.; McIntosh, C.D.; Winkley, K.; Gethin, G. Psychological interventions for treating foot ulcers, and preventing their recurrence, in people with diabetes. Cochrane Database Syst. Rev. 2021, 2017, CD012835. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.; Altman, D.; Laupacis, A.; Gøtzsche, P.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.C.; Moher, D.; the CONSORT group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar]
- Pais-Ribeiro, J.; Silva, I.; Ferreira, T.; Martins, A.; Meneses, R.; Baltar, M. Validation study of a Portuguese version of the Hospital Anxiety and Depression Scale. Psychol. Health Med. 2007, 12, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Trigo, M.; Canudo, N.; Branco, F.; Silva, D. Estudo das propriedades psicométricas da Perceived Stress Scale (PSS) na população Portuguesa [Psychometric proprieties of the Perceived Stress Scale (PSS) in Portuguese population]. Psychologica 2010, 53, 353–378. [Google Scholar] [CrossRef]
- Van Rijnsoever, F.J. (I Can’t get no) saturation: A simulation and guidelines for sample sizes in qualitative research. PLoS ONE 2017, 12, e0181689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Shin, W. How to Do Random Allocation (Randomization). Clin. Orthop. Surg. 2014, 6, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Spieth, P.M.; Kubasch, A.S.; Penzlin, A.I.; Illigens, B.M.; Barlinn, K.; Siepmann, T. Randomized controlled trials—A matter of design. Neuropsychiatr. Dis. Treat. 2016, 12, 1341–1349. [Google Scholar]
- Bonnet, J.; Sultan, A. Narrative Review of the Relationship Between CKD and Diabetic Foot Ulcer. Kidney Internat. Rep. 2022, 7, 381–388. [Google Scholar] [CrossRef]
- Hinchliffe, R.J.; Forsythe, R.O.; Apelqvist, J.; Boyko, E.J.; Fitridge, R.; Hong, J.P.; Katsanos, K.; Mills, J.L.; Nikol, S.; Reekers, J.; et al. Guidelines on diagnosis, prognosis, and management of peripheral artery disease in patients with foot ulcers and diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36, e3276. [Google Scholar] [CrossRef]
- Chuan, F.; Tang, K.; Jiang, P.; Zhou, B.; He, X. Reliability and validity of the perfusion, extent, depth, infection and sensation (PEDIS) classification system and score in patients with diabetic foot ulcer. PLoS ONE 2015, 10, e0124739. [Google Scholar] [CrossRef]
- Marques, J.M. Adaptação Cultural e Validação Para a População Portuguesa de um Instrumento de Monitorização de Feridas Crónicas—Escala RESVECH 2.0 [Cultural Adaptation and Validation of a Monitoring Chronic Wounds Instrument into Portuguese Population: RESVECH 2.0 Scale]. Master’s Thesis, Instituto de Ciências da Saúde da Universidade Católica, Porto, Portugal, 16 November 2016. [Google Scholar]
- Health & Family Research Group (GISEF). Manuscript in Preparation; GISEF: Braga, Portugal, 2022. [Google Scholar]
- Ferreira, P.L.; Ferreira, L.N.; Pereira, L.N. Medidas sumário física e mental de estado de saúde para a população portuguesa [Physical and mental summary measures of health state for the Portuguese population]. Rev. Port. De Saude Publ. 2012, 30, 163–171. [Google Scholar]
- Figueiras, M.; Marcelino, D.; Claudino, A.; Cortes, M.; Maroco, J.; Weinman, J. Patients’ illness schemata of hypertension: The role of beliefs in the choice of treatment. Psychol. Health 2010, 25, 507–517. [Google Scholar] [CrossRef]
- Paiva, D.; Silva, S.; Severo, M.; Ferreira, P.; Santos, O.; Lunet, N.; Azevedo, A. Cross-cultural adaptation and validation of the health literacy assessment tool METER in the Portuguese adult population. Patient Educ. Couns. 2014, 97, 269–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Direção-Geral de Saúde, DGS [General Health Direction, Portugal]. Circular Normativa Nº: 05/PNPCD: Pé Diabético, Programa Nacional de Prevenção e Controlo da Diabetes [Normative Circular Nº: 05/PNPCD: Diabetic Foot, National Diabetes Prevention and Control Program]. Available online: http://www.dgs.pt/?cr=15718 (accessed on 20 December 2021).
- Schaper, N.; van Netten, J.; Apelqvist, J.; Bus, S.; Hinchliffe, R.; Lipsky, B.; International Working Group on the Diabetic Foot [IWGDF] Editorial Board. Practical Guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36, e3266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegel, H. An Eye-Roll Test for Hypnotizability. Am. J. Clin. Hypn. 1972, 15, 25–28. [Google Scholar] [CrossRef]
- Sakpal, T.V. Sample size estimation in clinical trial. Perspect. Clin. Res. 2010, 1, 67–69. [Google Scholar] [PubMed]
- Ferreira, G.; Faria, S.; Carvalho, A.; Pereira, M.G. Relaxation Intervention to Improve Diabetic Foot Ulcer Healing: Results from a Pilot Randomized Controlled Study. Submitted.


{kind=link}
| TIMEPOINTS | Enrollment | Allocation | Pos-Allocation | Follow-Up | ||
|---|---|---|---|---|---|---|
| T0 | T0 | T1 | 2 Weeks after T1 | T2 | ||
| Eligibility | X | |||||
| Informed consent | X | |||||
| Allocation | X | |||||
| INTERVENTIONS |  | |||||
| PMR + GI (TG1) | ||||||
| H + GI (TG2) | ||||||
| Control groups |  | |||||
| Active (ACG) | ||||||
| Passive (PCG) | ||||||
| ASSESSMENTS | ||||||
| Sociodemographic data | X | |||||
| Health literacy | X | |||||
| Clinical data (PEDIS) | X | X | X | |||
| DFU evolution/healing a | X | X | X | |||
| Impact of DFU on QoL | X | X | X | |||
| Mental and physical QoL | X | X | X | |||
| Perceived stress | X | X | X | |||
| Psychological morbidity | X | X | X | |||
| DFU representations a | X | X | X | |||
| Blood pressure b | X | X | X | |||
| Heart rate b | X | X | X | |||
| Biochemical parameter | X | X | X | |||
| Inflammatory markers | X | X | X | |||
| Angiogenic markers | X | X | X | |||
| miRNAs | X | X | X | |||
| Immune cells | X | X | X | |||
| Semi-structured interviews | X | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, M.G.; Vilaça, M.; Carvalho, E. Effectiveness of Two Stress Reduction Interventions in Patients with Chronic Diabetic Foot Ulcers (PSY-DFU): Protocol for a Longitudinal RCT with a Nested Qualitative Study Involving Family Caregivers. Int. J. Environ. Res. Public Health 2022, 19, 8556. https://doi.org/10.3390/ijerph19148556
Pereira MG, Vilaça M, Carvalho E. Effectiveness of Two Stress Reduction Interventions in Patients with Chronic Diabetic Foot Ulcers (PSY-DFU): Protocol for a Longitudinal RCT with a Nested Qualitative Study Involving Family Caregivers. International Journal of Environmental Research and Public Health. 2022; 19(14):8556. https://doi.org/10.3390/ijerph19148556
Chicago/Turabian StylePereira, M. Graça, Margarida Vilaça, and Eugenia Carvalho. 2022. "Effectiveness of Two Stress Reduction Interventions in Patients with Chronic Diabetic Foot Ulcers (PSY-DFU): Protocol for a Longitudinal RCT with a Nested Qualitative Study Involving Family Caregivers" International Journal of Environmental Research and Public Health 19, no. 14: 8556. https://doi.org/10.3390/ijerph19148556
APA StylePereira, M. G., Vilaça, M., & Carvalho, E. (2022). Effectiveness of Two Stress Reduction Interventions in Patients with Chronic Diabetic Foot Ulcers (PSY-DFU): Protocol for a Longitudinal RCT with a Nested Qualitative Study Involving Family Caregivers. International Journal of Environmental Research and Public Health, 19(14), 8556. https://doi.org/10.3390/ijerph19148556