
The Assessment of Early Server Childhood Caries Status in Abandoned Institutionalized Children

 and
and
Abstract
:1. Introduction
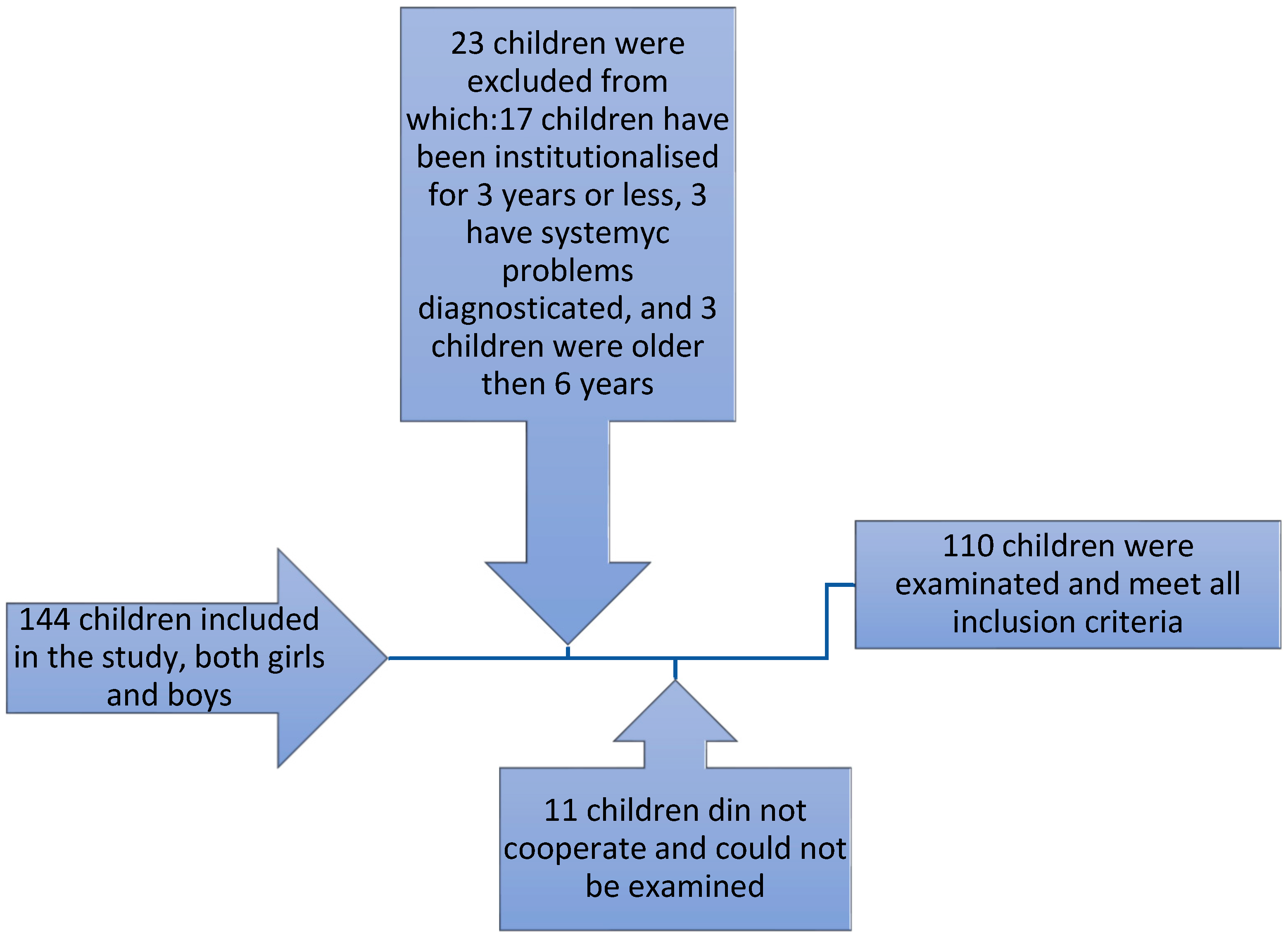
2. Materials and Methods
2.1. Study Design
2.2. Clinical Examination and Assessment
2.3. Statistical Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenthal, E.A. Mandate to End Placement of Children in Institutions and Orphanages: The Duty of Governments and Donors to Prevent Segregation and Torture. February 2017. Available online: https://ssrn.com/abstract=3271306 (accessed on 22 September 2018).
- Dozier, M.; Zeanah, C.H.; Wallin, A.R.; Shauffer, C. Institutional Care for Young Children: Review of Literature and Policy Implications. Soc. Issues Policy Rev. 2012, 6, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkowitz, R.J. Causes, treatment and prevention of early childhood caries: A microbiologic perspective. J. Can. Dent. Assoc. 2003, 69, 304–307. [Google Scholar] [PubMed]
- De Castilho, A.R.F.; Mialhe, F.L.; Barbosa, T.D.S.; Puppin-Rontani, R.M. Influence of family environment on children’s oral health: A systematic review. J. Pediatr. 2013, 89, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Fan, C.; Wang, W.; Xu, T.; Zheng, S. Risk factors of early childhood caries among children in Beijing: A case-control study. BMC Oral Health 2016, 16, 98. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Qingming, Z.; Jinhua, W.; Jun, D.; Hechuan, Z.; Songlin, H.; Lina, D. Investigation on deciduous dental caries among preschool children in Chongqing city. West China J. Stomatol. 2014, 32, 472–475. [Google Scholar] [CrossRef]
- Bratthall, D.; Petersson, G.H. Cariogram—A multifactorial risk assessment model for a multifactorial disease. Community Dent. Oral Epidemiol. 2005, 33, 256–264. [Google Scholar] [CrossRef]
- Gao, X.; Di Wu, I.; Lo, E.C.M.; Chu, C.H.; Hsu, C.-Y.S.; Wong, M.C.M. Validity of caries risk assessment programmes in preschool children. J. Dent. 2013, 41, 787–795. [Google Scholar] [CrossRef]
- Maheswari, S.U.; Raja, J.; Kumar, A.; Seelan, R.G. Caries management by risk assessment: A review on current strategies for caries prevention and management. J. Pharm. Bioallied Sci. 2015, 7, 320–324. [Google Scholar] [CrossRef]
- Yoon, R.K.; Smaldone, A.M.; Edelstein, B.L. Early childhood caries screening tools: A comparison of four approaches. J. Am. Dent. Assoc. 2012, 143, 756–763. [Google Scholar] [CrossRef]
- Holgerson, P.L.; Twetman, S.; Stecksen-Blicks, C. Validation of an age-modified caries risk assessment program (Cariogram) in preschool children. Acta Odontol. Scand. 2009, 67, 106–112. [Google Scholar] [CrossRef]
- Gao, X.-L.; Hsu, C.-Y.; Xu, Y.; Hwarng, H.; Loh, T.; Koh, D. Building Caries Risk Assessment Models for Children. J. Dent. Res. 2010, 89, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Petersson, G.H.; Isberg, P.-E.; Twetman, S. Caries risk assessment in school children using a reduced Cariogram model without saliva tests. BMC Oral Health 2010, 10, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iida, H.; Auinger, P.; Billings, R.J.; Weitzman, M. Association between Infant Breastfeeding and Early Childhood Caries in the United States. Pediatrics 2007, 120, e944–e952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenblatt, A.; Zarzar, P. Breast-feeding and early childhood caries: An assessment among Brazilian infants. Int. J. Paediatr. Dent. 2004, 14, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Willing, M.C.; Marazita, M.L.; Wendell, S.; Warren, J.; Broffitt, B.; Smith, B.; Busch, T.; Lidral, A.C.; Levy, S.M. Genetic and Environmental Factors Associated with Dental Caries in Children: The Iowa Fluoride Study. Caries Res. 2012, 46, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, N.; Mathiba, O.P.; Mulder, R. Oral status of HIV-infected children aged 12 years or younger who attended a Paediatric Infectious Diseases Clinic in Cape Town. Clin. Exp. Dent. Res. 2020, 6, 75–81. [Google Scholar] [CrossRef]
- ElKarmi, R.; Aljafari, A.; Eldali, H.; Hosey, M.T. Do expectant mothers know how early childhood caries can be prevented? A cross-sectional study. Eur. Arch. Paediatr. Dent. 2019, 20, 595–601. [Google Scholar] [CrossRef]
- Boustedt, K.; Dahlgren, J.; Twetman, S.; Roswall, J. Tooth brushing habits and prevalence of early childhood caries: A prospective cohort study. Eur. Arch. Paediatr. Dent. 2020, 21, 155–159. [Google Scholar] [CrossRef] [Green Version]
- George, A.; Lang, G.; Johnson, M.; Ridge, A.; de Silva, A.M.; Ajwani, S.; Bhole, S.; Blinkhorn, A.; Dahlen, H.; Ellis, S.; et al. The evaluation of an oral health education program for midwives in Australia. Women Birth 2016, 29, 208–213. [Google Scholar] [CrossRef]
- Cui, T.; Xu, Q.; Wu, Y.; Yang, X.; Sun, H. Longitudinal Follow-up Survey of Effects of Oral Comprehensive Healthcare Measures on Early Childhood Caries. Oral Health Prev. Dent. 2020, 18, 197–203. [Google Scholar] [CrossRef]
- Ahovuo-Saloranta, A.; Forss, H.; Walsh, T.; Nordblad, A.; Mäkelä, M.; Worthington, H.V. Pit and fissure sealants for preventing dental decay in permanent teeth. Cochrane Database Syst. Rev. 2017, 7, CD001830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Bernabe, E.; Pitts, N.; Zheng, S.; Gallagher, J.E. Dental caries thresholds among adolescents in England, Wales, and Northern Ireland, 2013 at 12, and 15 years: Implications for epidemiology and clinical care. BMC Oral Health 2021, 21, 137. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, P.A.; Sheiham, A. Grouping of tooth surfaces by susceptibility to caries: A study in 5–16 year-old children. BMC Oral Health 2004, 4, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, M.R.; Sayadizadeh, M.; Raeisi Estabragh, S.; Ghannadan, K.; Malek-Mohammadi, M. Dental caries status and its related factors in Iran: A meta-analysis. J. Dent. 2020, 21, 158–176. [Google Scholar]
- Mahboobi, Z.; Pakdaman, A.; Yazdani, R.; Azadbakht, L.; Shamshiri, A.R.; Babaei, A. Caries incidence of the first permanent molars according to the Caries Assessment Spectrum and Treatment (CAST) index and its determinants in children: A cohort study. BMC Oral Health 2021, 21, 259. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P.J.; Kelly, S.A. Effect on Caries of Restricting Sugars Intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habibian, M.; Roberts, G.; Lawson, M.; Stevenson, R.; Harris, S. Dietary habits and dental health over the first 18 months of life. Community Dent. Oral Epidemiol. 2001, 29, 239–246. [Google Scholar] [CrossRef]
- Dixit, L.P.; Shakya, A.; Shrestha, M.; Shrestha, A. Dental caries prevalence, oral health knowledge and practice among indigenous Chepang school children of Nepal. BMC Oral Health 2013, 13, 20. [Google Scholar] [CrossRef] [Green Version]
- Stein, C.; Cunha-Cruz, J.; Hugo, F.N. Is dietary pattern a mediator of the relationship between socioeconomic status and dental caries? Clin. Oral Investig. 2021, 25, 5441–5447. [Google Scholar] [CrossRef]
- Iasonos, A.; Schrag, D.; Raj, G.V. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Casanova-Rosado, J.F.; Casanova-Rosado, A.J.; Minaya-Sanchez, M. Self-Reported Dental Caries by Mexican Elementary and Middle-School Schoolchildren in the Context of Socioeconomic Indicators: A National Ecological Study. Children 2021, 8, 289. [Google Scholar] [CrossRef] [PubMed]
- Elamin, A.; Garemo, M.; Gardner, A. Dental caries and their association with socioeconomic characteristics, oral hygiene practices and eating habits among preschool children in Abu Dhabi, United Arab Emirates—The NOPLAS project. BMC Oral Health 2018, 18, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Y.-T.; Zhu, C.; Xu, W.; Lu, H.-X.; Ye, W. A study about oral health-related quality of life among 11–14-year-old children in Shanghai municipality. Shanghai J. Stomatol. 2015, 24, 345–350. [Google Scholar]
- Wang, H.-N.; Wang, Y.; Zhang, H.; Mao, Y.-M.; Dong, H.; Hua, M.; Jiang, Y.-W.; Zhang, Y. Early childhood caries and its related risk factors in 1296 children aged 3 to 5 years old in Shanghai. Shanghai J. Stomatol. 2020, 29, 174–178. [Google Scholar]
- Heaton, B.; Cherng, S.T.; Sohn, W. Complex Systems Model of Dynamic Mechanisms of Early Childhood Caries Development. J. Dent. Res. 2020, 99, 537–543. [Google Scholar] [CrossRef]
- Stoica, A.M.; Stoica, O.E.; Vlad, R.E.; Pop, A.M.; Monea, M. Correlation between Oral Self-Harm and Ethnicity in Institutionalized Children. Children 2021, 8, 2. [Google Scholar] [CrossRef]
- Duangthip, D.; Chen, K.J.; Gao, S.S.; Lo, E.C.M.; Chu, C.H. Managing Early Childhood Caries with Atraumatic Restorative Treatment and Topical Silver and Fluoride Agents. Int. J. Environ. Res. Public Health 2017, 14, 1204. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatric Dentistry Council on Clinical Affairs. Policy on Early Childhood Caries (ECC): Unique Challenges and Treatment Options. Pediatric. Dent. 2016, 38, 55–56. [Google Scholar]



{kind=link}
{kind=link}
| Total 110 | 5 Years Old | 6 Years Old |
|---|---|---|
| Girls 52 (47.27%) | 23 (20.90%) | 29 (26.36%) |
| Boys 58 (52.72%) | 30 (27.27%) | 28 (25.46%) |
| No. of Incisors Affected/Child | Children | % of Total |
|---|---|---|
| 0 | 64 | 58.2% |
| 2 | 11 | 10.0% |
| 4 | 23 | 20.9% |
| 6 | 9 | 8.2% |
| 8 | 3 | 2.7% |
| No. of Canines Affected/Child | Children | % of Total |
|---|---|---|
| 0 | 68 | 61.8% |
| 2 | 39 | 35.5% |
| 4 | 3 | 2.7% |
| No. of Molars Affected/Child | Children | % of Total |
|---|---|---|
| 0 | 7 | 6.4% |
| 2 | 14 | 12.7% |
| 3 | 31 | 28.2% |
| 4 | 32 | 29.1% |
| 5 | 10 | 9.1% |
| 6 | 3 | 2.7% |
| 8 | 13 | 11.8% |
| Dmft | Children | % of Total | Cumulative % |
|---|---|---|---|
| 0 | 7 | 6.5% | 6.5% |
| 2 | 7 | 6.5% | 13.1% |
| 3 | 12 | 11.2% | 24.3% |
| 4 | 12 | 11.2% | 35.5% |
| 5 | 10 | 9.3% | 44.9% |
| 6 | 13 | 12.1% | 57.0% |
| 7 | 9 | 8.4% | 65.4% |
| 8 | 15 | 14.0% | 79.4% |
| 9 | 10 | 9.3% | 88.8% |
| 12 | 6 | 5.6% | 94.4% |
| 14 | 3 | 2.8% | 97.2% |
| 20 | 3 | 2.8% | 100.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoica, O.E.; Esian, D.; Bud, A.; Stoica, A.M.; Beresescu, L.; Bica, C.I. The Assessment of Early Server Childhood Caries Status in Abandoned Institutionalized Children. Int. J. Environ. Res. Public Health 2022, 19, 8632. https://doi.org/10.3390/ijerph19148632
Stoica OE, Esian D, Bud A, Stoica AM, Beresescu L, Bica CI. The Assessment of Early Server Childhood Caries Status in Abandoned Institutionalized Children. International Journal of Environmental Research and Public Health. 2022; 19(14):8632. https://doi.org/10.3390/ijerph19148632
Chicago/Turabian StyleStoica, Oana Elena, Daniela Esian, Anamaria Bud, Alexandra Mihaela Stoica, Liana Beresescu, and Cristina Ioana Bica. 2022. "The Assessment of Early Server Childhood Caries Status in Abandoned Institutionalized Children" International Journal of Environmental Research and Public Health 19, no. 14: 8632. https://doi.org/10.3390/ijerph19148632
APA StyleStoica, O. E., Esian, D., Bud, A., Stoica, A. M., Beresescu, L., & Bica, C. I. (2022). The Assessment of Early Server Childhood Caries Status in Abandoned Institutionalized Children. International Journal of Environmental Research and Public Health, 19(14), 8632. https://doi.org/10.3390/ijerph19148632