
Examine Race/Ethnicity Disparities in Perception, Intention, and Screening of Dementia in a Community Setting: Scoping Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.3. Collecting and Summarization
3. Results
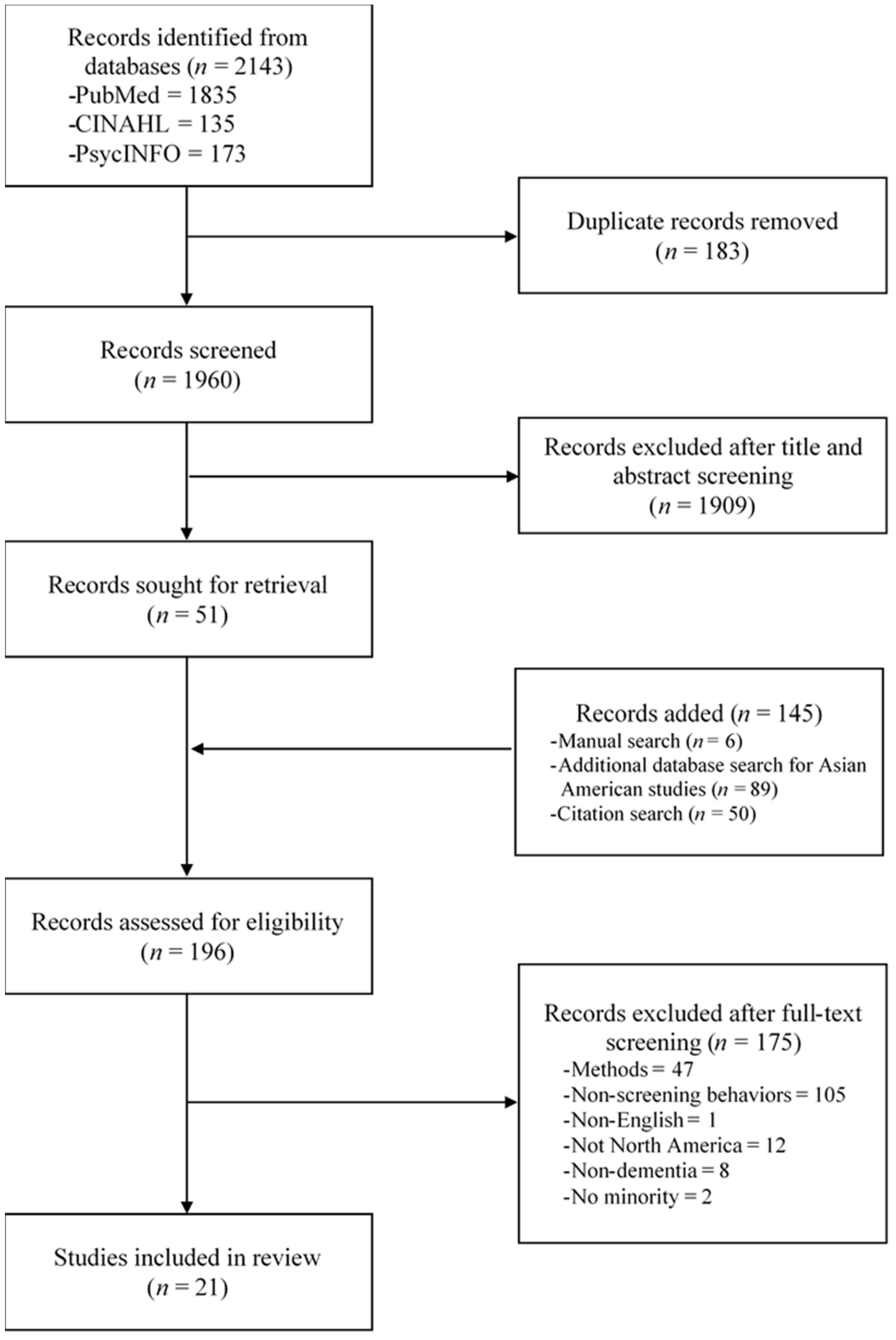
3.1. Search Results
3.2. Study Designs
3.3. Sample Characteristics
3.4. Theoretical Trends
3.5. ADRD Screening Behavior Is A Multidimensional Construct
3.6. Differences in ADRD Screening Behavior among Ethnicities
“He recalls that his mother’s doctor, who practices in Chinatown, said, ‘don’t expect too much… it is like a machine. After a long period of time, its parts will certainly be off or fall apart.’ The son denies that his mother has ever received a formal diagnosis of AD or dementia. He wishes that the doctor would ‘explain more’ and emphasized language barriers as a significant problem in getting care for his mother.”[42] (p. 140)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alzheimer’s Association. 2021 Alzheimer’s disease facts and figures. Alzheimers Dement. 2021, 17, 327–406. [Google Scholar] [CrossRef] [PubMed]
- Chodosh, J.; Petitti, D.B.; Elliott, M.; Hays, R.D.; Crooks, V.C.; Reuben, D.B.; Buckwalter, J.G.; Wenger, N. Physician recognition of cognitive impairment: Evaluating the need for improvement. J. Am. Geriatr. Soc. 2004, 52, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Kotagal, V.; Langa, K.M.; Plassman, B.L.; Fisher, G.G.; Giordani, B.J.; Wallace, R.B.; Burke, J.R.; Steffens, D.C.; Kabeto, M.; Albin, R.L.; et al. Factors associated with cognitive evaluations in the United States. Neurology 2015, 84, 64–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor Jr, D.H.; Østbye, T.; Langa, K.M.; Weir, D.; Plassman, B.L. The accuracy of Medicare claims as an epidemiological tool: The case of dementia revisited. J. Alzheimers Dis. 2009, 17, 807–815. [Google Scholar] [CrossRef] [Green Version]
- Dementias, Including Alzheimer’s Disease. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/dementias-including-alzheimers-disease/national-snapshot (accessed on 10 May 2022).
- Chin, A.L.; Negash, S.; Hamilton, R. Diversity and disparity in dementia: The impact of ethnoracial differences in Alzheimer’s disease. Alzheimer Dis. Assoc. Disord. 2011, 25, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Gianattasio, K.Z.; Prather, C.; Glymour, M.M.; Ciarleglio, A.; Power, M.C. Racial disparities and temporal trends in dementia misdiagnosis risk in the United States. Alzheimers Dement. 2019, 5, 891–898. [Google Scholar] [CrossRef]
- Lang, L.; Clifford, A.; Wei, L.; Zhang, D.; Leung, D.; Augustine, G.; Danat, I.M.; Zhou, W.; Copeland, J.R.; Anstey, K.J.; et al. Prevalence and determinants of undetected dementia in the community: A systematic literature review and a meta-analysis. BMJ. Open 2017, 7, e011146. [Google Scholar] [CrossRef] [Green Version]
- Lines, L.M.; Wiener, J.M. Racial and Ethnic Disparities in Alzheimer’s Disease: A Literature Review. RTI International. 2014. Available online: https://aspe.hhs.gov/sites/default/files/migrated_legacy_files//138596/RacEthDis.pdf (accessed on 8 May 2022).
- Manly, J.J.; Avila, J.F.; Vonk, J.M.J.; Rentería, M.A.; Turney, I.C.; Lao, P.J.; Seblova, D.; Martinez, M.N.; Gutierrez, J.; Mayeux, R.; et al. Racial differences in cognitive resilience to parental history of AD and cognitive impairment: The offspring study. Alzheimers Dement. 2021, 17, e051874. [Google Scholar] [CrossRef]
- Special Committee on Aging United States Senate. 112th Congress 2d Session [Report 112–254]. Alzheimer’s Disease and Dementia: A Comparison of International Approaches. Available online: https://www.govinfo.gov/content/pkg/CRPT-112srpt254/pdf/CRPT-112srpt254.pdf (accessed on 8 May 2022).
- Cooper, C.; Tandy, A.R.; Balamurali, T.B.S.; Livingston, G. A systematic review and meta-analysis of ethnic differences in use of dementia treatment, care, and research. Am. J. Geriatr. Psychiatry 2010, 18, 193–203. [Google Scholar] [CrossRef]
- Livney, M.G.; Clark, C.M.; Karlawish, J.H.; Cartmell, S.; Negrón, M.; Nuñez, J.; Xie, S.X.; Entenza-Cabrera, F.; Vega, I.E.; Arnold, S.E. Ethnoracial differences in the clinical characteristics of Alzheimer’s disease at initial presentation at an urban Alzheimer’s disease center. Am. J. Geriatr. Psychiatry 2011, 19, 430–439. [Google Scholar] [CrossRef] [Green Version]
- National Plan to Address Alzheimer’s Disease: 2021 Update. Available online: https://aspe.hhs.gov/reports/national-plan-2021-update (accessed on 10 May 2022).
- Colby, S.L.; Ortman, J.M. Projections of the Size and Composition of the U.S. Population: 2014 to 2060, Current Population Reports, P25-1143; U.S. Census Bureau: Washington, DC, USA, 2014.
- Babulal, G.M.; Quiroz, Y.T.; Albensi, B.C.; Arenaza-Urquijo, E.; Astell, A.J.; Babiloni, C.; Bahar-Fuchs, A.; Bell, J.; Bowman, G.L.; Brickman, A.M.; et al. Perspectives on ethnic and racial disparities in Alzheimer’s disease and related dementia: Update and areas in immediate need. Alzheimers Dement. 2019, 15, 292–312. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Padovani, A.; Scheltens, P.; Rossi, A.; Dell’Agnello, G. Timely diagnosis for Alzheimer’s disease: A literature review on benefits and challenges. J. Alzheimers Dis. 2016, 49, 617–631. [Google Scholar] [CrossRef] [Green Version]
- Ford, M.E.; Kelly, P.A. Conceptualizing and categorizing race and ethnicity in health services research. Health Serv. Res. 2005, 40, 1658–1675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, L.K.; Welter, E.; Leverenz, J.; Lerner, A.J.; Udelson, N.; Kanetsky, C.; Sajatovic, M. A systematic review of dementia-related stigma research: Can we move the stigma dial? Am. J. Geriatr. Psychiatry 2018, 26, 316–331. [Google Scholar] [CrossRef] [PubMed]
- Marin, S.; Kelly, S.; Khan, A.; Cullum, S.; Dening, T.; Rait, G.; Fox, C.; Katona, C.; Cosco, T.; Brayne, C.; et al. Attitudes and preferences towards screening for dementia: A systematic review of the literature. BMC Geriatr. 2015, 15, 66. [Google Scholar]
- Sagbakken, M.; Spilker, R.S.; Nielsen, T.R. Dementia and immigrant groups: A qualitative study of challenges related to identifying, assessing, and diagnosing dementia. BMC Health Serv. Res. 2018, 18, 910. [Google Scholar] [CrossRef]
- Quiroz, Y.T.; Solis, M.; Aranda, M.P.; Arbaje, A.I.; Arroyo-Miranda, M.; Cabrera, L.Y.; Carrasquillo, M.M.; Corrada, M.M.; Crivelli, L.; Diminich, E.D.; et al. Addressing the disparities in dementia risk, early detection and care in Latino populations: Highlights from the second Lationos & Alzheimer’s symposium. Alzheimers Dement. 2022, 1–10. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Fawcett, J.; Kim, D.; Yang, J.H. Correlates of hepatitis B virus-related stigmatization experienced by Asians: A scoping review of literature. Asia Pac. J. Oncol. Nurs. 2016, 3, 324–334. [Google Scholar] [CrossRef]
- Lim, S.; Chong, S.; Min, D.; Mohaimin, S.; Roberts, T.; Trinh-Shevrin, C.; Kwon, S.C. Alzheimer’s disease screening tools for Asian Americans: A scoping review. J. Appl. Gerontol. 2021, 40, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Pham, M.T.; Rajić, A.; Greig, J.D.; Sargeant, J.M.; Papadopoulos, A.; McEwen, S.A. A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Res. Synth. Methods 2014, 5, 371–385. [Google Scholar] [CrossRef] [PubMed]
- Clark, P.C.; Kutner, N.G.; Goldstein, F.C.; Peterson-Hazen, S.; Garner, V.; Zhang, R.; Bowles, T. Impediments to timely diagnosis of Alzheimer’s disease in African Americans. J. Am. Geriatr. Soc. 2005, 53, 2012–2017. [Google Scholar] [CrossRef] [PubMed]
- Holsinger, T.; Boustani, M.; Abbot, D.; Williams, J.W. Acceptability of dementia screening in primary care patients. Int. J. Geriatr. Psychiatry 2011, 26, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Fowler, N.R.; Boustani, M.A.; Frame, A.; Perkins, A.J.; Monahan, P.; Gao, S.; Sachs, G.A.; Hendrie, H.C. Impact of patients’ perceptions on dementia screening in primary care. J. Am. Geriatr. Soc. 2012, 60, 1037–1043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, N.R.; Perkins, A.J.; Turchan, H.A.; Frame, A.; Monahan, P.; Gao, S.; Boustani, M.A. Older primary care patients’ attitudes and willingness to screen for dementia. J. Aging Res. 2015, 2015, 423265. [Google Scholar] [CrossRef] [PubMed]
- Savva, G.M.; Arthur, A. Who has undiagnosed dementia? A cross-sectional analysis of participants of the Aging, Demographics and Memory Study. Age Ageing 2015, 44, 642–647. [Google Scholar] [CrossRef] [Green Version]
- Casado, B.L.; Hong, M.; Lee, S.E. Attitudes toward Alzheimer’s care-seeking among Korean Americans: Effects of knowledge, stigma, and subjective norm. Gerontologist 2018, 58, e25–e34. [Google Scholar] [CrossRef] [Green Version]
- Amjad, H.; Roth, D.L.; Sheehan, O.C.; Lyketsos, C.G.; Wolff, J.L.; Samus, Q.M. Underdiagnosis of dementia: An observational study of patterns in diagnosis and awareness in US older adults. J. Gen. Intern. Med. 2018, 33, 1131–1138. [Google Scholar] [CrossRef] [Green Version]
- Harrawood, A.; Fowler, N.R.; Perkins, A.J.; LaMantia, M.A.; Boustani, M.A. Acceptability and results of dementia screening among older adults in the United States. Curr. Alzheimer Res. 2018, 15, 51–55. [Google Scholar] [CrossRef]
- Park, J.; Tolea, M.; Besser, L.; Galvin, J. Intention to be screened for Alzheimer’s disease in nondemented older adults: Integrated Behavioral Model and self-efficacy as mediation effect. J. Hum. Behav. Soc. Environ. 2020, 30, 778–796. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.; Daly, A.T.; Olchanski, N.; Cohen, J.T.; Neumann, P.J.; Faul, J.D.; Fillit, H.M.; Freund, K.M. Dementia diagnosis disparities by race and ethnicity. Med. Care 2021, 59, 679–686. [Google Scholar] [CrossRef]
- Tsoy, E.; Kiekhofer, R.E.; Guterman, E.L.; Tee, B.L.; Windon, C.C.; Dorsman, K.A.; Lanata, S.C.; Rabinovici, G.D.; Miller, B.L.; Kind, A.J.H.; et al. Assessment of racial/ethnic disparities in timeliness and comprehensiveness of dementia diagnosis in California. JAMA Neurol. 2021, 78, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Wiese, L.K.; Galvin, J.E.; Williams, C.L. Rural stakeholder perceptions about cognitive screening. Aging Ment. Health 2019, 23, 1616–1628. [Google Scholar] [CrossRef] [PubMed]
- Wiese, L.K.; Williams, I.; Williams, C.L.; Galvin, J.E. Discerning rural Appalachian stakeholder attitudes toward memory screening. Aging Ment. Health 2021, 25, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.L.; Tappen, R.M.; Rosselli, M.; Keane, F.; Newlin, K. Willingness to be screened and tested for cognitive impairment: Cross-cultural comparison. Am. J. Alzheimers Dis. Other Demen. 2010, 25, 160–166. [Google Scholar] [CrossRef]
- Hinton, L.; Franz, C.; Friend, J. Pathways to dementia diagnosis: Evidence for cross-ethnic differences. Alzheimer Dis. Assoc. Disord. 2004, 18, 134–144. [Google Scholar] [CrossRef]
- Hugh, T.; Tyler, K.; Danner, D.; Carter, A. African American caregivers: An exploration of pathways and barriers to a diagnosis of Alzheimer’s disease for a family member with dementia. Dementia 2009, 8, 95–116. [Google Scholar] [CrossRef]
- Leung, K.K.; Finlay, J.; Silvius, J.L.; Koehn, S.; McCleary, L.; Cohen, C.A.; Hum, S.; Garcia, L.; Dalziel, W.; Emerson, V.F.; et al. Pathways to diagnosis: Exploring the experiences of problem recognition and obtaining a dementia diagnosis among Anglo-Canadian. Health Soc. Care Community 2011, 19, 372–381. [Google Scholar] [CrossRef]
- Koehn, S.; McCleary, L.; Garcia, L.; Spence, M.; Jarvis, P.; Drummond, N. Understanding Chinese-Canadian pathways to a diagnosis of dementia through a critical-constructionist lens. J. Aging Res. 2012, 26, 44–54. [Google Scholar] [CrossRef]
- McCleary, L.; Persaud, M.; Hum, S.; Pimlott, N.J.G.; Cohen, C.A.; Koehn, S.; Leung, K.K.; Dalziel, W.B.; Kozak, J.; Emerson, V.F.; et al. Pathways to dementia diagnosis among South Asian Canadians. Dementia 2013, 12, 769–789. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.J.; McCleary, L.; Emerson, V.; Léopoldoff, H.; Dalziel, W.; Drummond, N.; Cohen, C.; Koehn, S.; Silvius, J. The pathway to diagnosis of dementia for Francophones living in a minority situation. Gerontologist 2013, 54, 964–975. [Google Scholar] [CrossRef] [PubMed]
- Doàn, L.N.; Takata, Y.; Sakuma, K.K.; Irvin, V.L. Trends in clinical research including Asian American, Native Hawaiian, and Pacific Islander participants funded by the US National Institutes of Health, 1992 to 2018. JAMA Netw. Open 2019, 2, e197432. [Google Scholar] [CrossRef] [PubMed]
- NIA and the National Plan to Address Alzheimer’s Disease. Available online: https://www.nia.nih.gov/about/nia-and-national-plan-address-alzheimers-disease (accessed on 8 May 2022).
- Bradford, A.; Kunik, M.E.; Schulz, P.; Williams, S.P.; Singh, H. Missed and delayed diagnosis of dementia in primary care: Prevalence and contributing factors. Alzheimer Dis. Assoc. Disord. 2009, 23, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Romano, R.R.; Carter, M.A.; Anderson, A.R.; Monroe, T.B. An integrative review of system-level factors influencing dementia detection in primary care. J. Am. Assoc. Nurse Pract. 2020, 32, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Elliott, K.S.; Di Minno, M. Unruly grandmothers, ghosts and ancesters: Chinese elders and the importance of culture in dementia evaluations. J. Cross Cult. Gerontol. 2006, 21, 157–177. [Google Scholar] [CrossRef]
- Sentell, T.; Braun, K. Low health literacy, limited english proficiency, and health status in asians, latinos, and other racial/ethnic groups in California. J. Health Commun. 2012, 17 (Suppl. S3), 82–99. [Google Scholar] [CrossRef] [Green Version]
- Angel, J.L.; Angel, R.J. Minority group status and healthful aging: Social structure still matters. Am. J. Public Health. 2006, 96, 1152–1159. [Google Scholar] [CrossRef]
- Osborn, R.; Doty, M.M.; Moulds, D.; Sarnak, D.O.; Shah, A. Older Americans Were Sicker and Faced More Financial Barriers to Health Care than Counterparts in Other Countries. Health Aff. 2017, 36, 2123–2132. [Google Scholar] [CrossRef] [Green Version]
- Jones, R.S.; Chow, T.W.; Gatz, M. Asian Americans and Alzheimer’s disease: Assimilation, culture, and beliefs. J. Aging Stud. 2006, 20, 11–25. [Google Scholar] [CrossRef]
- Roche, M.; Higgs, P.; Aworinde, J.; Cooper, C. A Review of Qualitative Research of Perception and Experiences of Dementia Among Adults from Black, African, and Caribbean Background: What and Whom Are We Researching? Gerontology 2021, 61, e195–e208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Judge, D.; Roberts, J.; Khandker, R.; Ambegaonkar, B.; Black, C.M. Physician Perceptions about the Barriers to Prompt Diagnosis of Mild Cognitive Impairment and Alzheimer’s Disease. Int. J. Alzheimers Dis. 2019, 21, 3637954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsan, M.; Wanamaker, M. Tuskegee and the Health of Black Men. Q. J. Econ. 2018, 133, 407–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsan, M.; Owen Garrick, O.; Graziani, G. Does Diversity Matter for Health? Experimental Evidence From Oakland. Am. Econ. Rev. 2019, 109, 4071–4111. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| References | Study Location/ Recruitment Sites/ Age Range | Design/Population/ Sample Size | Ethnicity/Race/ Language | Key Findings |
|---|---|---|---|---|
| Clark et al. (2005) [28] | U.S. Community-based clinics (urban and suburban) | Cohort study Patients with probable AD and primary family caregivers n = 79 units | African Americans | Time from noticing first AD signs to recognition
Time from recognition to physician consultation:
Longer delay in recognition associated with longer delay in physician consultation |
| Holsinger et al. (2011) [29] | U.S. 2 sites: Clinics and community-based clinics (urban) ≥50 years | Cross-sectional study Patients presenting for primary care appointments n = 345 | White vs. minority Site 1 (n = 152): White 73% Site 2 (n = 193): White 57% | Majority accepted screening After exposing various potential risks and benefits, more accepted screening. No difference between white and minority |
| Fowler et al. (2012) [30] | U.S. Community-based clinics (urban) ≥65 years | Cross-sectional study Patients with no dementia receiving primary care n = 554 | White 41.5%, African Americans 56.5% Other 1.4% | Majority willing to screen; 12.7% screened positive Refusal rates did not vary with ethnicity, education, other SES. Odds of refusal higher in older age groups |
| Fowler et al. (2015) [31] | U.S. 2 sites Clinic (urban) and community-based clinics (urban and suburban) ≥65 years | Cross-sectional study Patients with no dementia receiving primary care n = 400 | Site 1 (n = 278): White 78.1%, African American 20.9%, Other 1.1% Site 2 (n = 122): White 96.7%, African American 2.5%, Other 0.8% English | Site 1: No difference in acceptance and refusal between White and African Americas Site 2: only one African American participant No differences in refusal between two sites Perceptions about the benefits of screening associated with acceptance of screening No effect of sociodemographic data except education predicted acceptance |
| Savva et al. (2015) [32] | U.S. Nationwide ≥71 years | Cross-sectional study Patients with dementia Data source: ADAMS substudy from HRS 2000–2002 waves n = 307 | White 73%, Non-White 27% English or Spanish | 121 informants reported prior diagnosis Grater CDC rate associated with prior diagnosis Race or nursing home residency no link with prior diagnosis Aged <90 years or married women associated with prior diagnosis. ¾ undiagnosed have mild dementia |
| Casado et al. (2017) [33] | U.S. Community (community outreach, local business sites, flyers, newsletters, social media) ≥40 years | Cross-sectional survey Adults n = 234 | Korean Americans English or Korean | 20.7% reported having experience with caring for someone with AD. Attitude scores were slightly more positive toward AD specialists (mean = 55.92 ± 7.40) than toward PCPs (mean = 54.24 ± 9.82). |
| Amjad et al. (2018) [34] | U.S. Nationwide ≥65 years | Cross-sectional observational study Patients with probable dementia or proxy Data source: NHATS n = 585 | Non-Hispanic White, non-Hispanic Black, Hispanic or other non-Hispanic (Asian, Pacific Islander, and Native American) | 39.5% undiagnosed Among diagnosed, 31% of those persons or their proxies were unaware of diagnosis. Undiagnosed persons likely to be non-White and lower education. But OR was statistically significant only for Hispanic/other non-White race Majority of older adults with dementia either undiagnosed or unaware of the diagnosis |
| Harrawood et al. (2018) [35] | U.S. 3 sites: clinic (urban) and community-based clinics (urban and suburban) ≥65 years | Cross-sectional study Patients with no dementia receiving primary care n = 954 | African American 42.4% (n = 317): Site 1 (n = 280), Site 2 (n = 35), Site 3 (n = 2) | 21.6% refused screening 78.4% agreed to be screened 10.2% screened positive: 11.7% African American; 9.0% White and other Older age (>75 years) low education, and perceived problem with memory associated with screening positive but no effect from race and research sites. |
| Gianattasio et al. (2019) [7] | U.S. Nationwide ≥70 years | Longitudinal study Patients with dementia Data source: HRS biannual interviews with participants or proxy linked with Medicare claims n = 4647–5201 (2000 to 2010, 6 observations) | Non-Hispanic White: 91–93%, Non-Hispanic Black: 7–9% English or Spanish | Whites were “correctly diagnosed” Blacks were “underdiagnosed” Black had double the risk of underdiagnosed compare with White at all 6 waves Risk of over diagnosed increased over time in both groups |
| Park et al. (2020) [36] | U.S. Community (urban, suburban, and rural) >50 years | Cross-sectional study Individuals with no dementia n = 1043 | White 82.7%, Black/African American 11.6%, Hispanic 1.2%, Asian 0.6%, Native Hawaiian/Pacific Islander 0.3%, American Indian 0.8% English | In terms of demographic difference, female and participants with long-term care insurance have greater intention to screen but no mention about the effect of race. Younger age, higher level of perceived barriers, perceived benefit, higher social support and self-efficacy associated with increased intention |
| Lin et al. (2021) [37] | U.S. Nationwide ≥70 years | Prospective cohort study Patients with probable dementia Data source: HRS 2000–2014 linked with Medicare and Medicaid n = 3966 | Non-Hispanic White 80.8%, non-Hispanic Black 11.9%, Hispanic 7.3% English or Spanish | A higher proportion of Blacks and Hispanics had a missed/delayed clinical dementia diagnosis compared with White (46%, s = 54% vs. 41%) Blacks and Hispanics had a poorer cognitive function and more functional limitations than White when received dementia diagnosis.
|
| Tsoy et al. (2021) [38] | U.S. Statewide | Retrospective cross-sectional study Patients with no prior dementia or MCI Data source: California CMS claims 2013–2015 n = 10,472 | White 74.6%, Black 3.9%, Hispanic 12.0%, Asian 9.5% | Incident MCI diagnosis 23.3% White, 18.28% Black, 12.3% Asian, 15.8% Hispanic Timeliness of diagnosis Asian, Blacks, and Hispanic less likely to receive an incident diagnosis of MCI vs. dementia than White Estimated mean marginal effects of race/ethnicity on incident diagnosis of MCI were −11.0% for Asian, −6.6% for Hispanic, and −5.6% for Black |
| Wiese et al. (2019) [39] | U.S. Local service organizations, physician offices, church councils, senior center (rural) | Mixed methods Stakeholders -Social workers, healthcare administrators, nurses, nurses’ aides, physician, ministers, clerical worker, kitchen aids, farmworkers, auto mechanic, church worker n = 21 | Non-Hispanic White (n = 5): professionals 4, layperson 1 African American (n = 11): professionals 9, laypersons 2 Afro-Caribbean (n = 2): professional 1, layperson 1 Hispanic American (n = 2): professional 1, layperson 1 English | 81%: willing to screening annually if they developed memory problems or AD 85% of those previously screened would want to know if they were at higher risk of AD. |
| Wiese et al. (2021) [40] | U.S. Local city hall, senior centers, healthcare clinics, faith-based organizations (rural) | Mixed methods Stakeholders -Senior center administrators, senior center volunteer staffs, health clinic administrators, law enforcement officers, emergency medical technicians, physicians, nurse practitioners, nurses, paid caregivers, family caregivers, residents n = 22 | White (n = 21), African American (n = 1) English | 100%: willing to screening 82%: agreeable to blood testing 86%: agreeable to pictures of head or brain to detect dementia All would want their provider to screen them annually for memory problems |
| Williams et al. (2010) [41] | U.S. Churches, senior centers, health fair (announcements and flyers) | Mixed method Open-ended questions A part memory screening study of 793 community dwelling older adults n = 119 | African American (n = 26) Afro-Caribbean (n = 31) European American (n = 29) Hispanic American (n = 33) English or Spanish | More African Americans recruited from churches than Hispanic and European American 89% valued the screening 92% would recommend screening to others 39% would seek professional help if they screened positive. More Hispanic Americans (70%) planned to seek help than did than European Americans (35%), African Americans (31%), or Afro-Caribbean (16%). |
| Hinton et al. (2004) [42] | U.S. Community (urban) (Physician referrals, Alzheimer’s Association, newspaper advertisements, etc.) Caregiver to patient ≥50 years | Qualitative Study In-depth interview A part of Survey Study: 33% of 117 family caregivers to community dwelling dementia patients -Wife, daughters, sons, others n = 39 | African American (n = 10) Chinese American (n = 14) Anglo European-American (n = 15) English or three Chinese dialects (Mandarin, Cantonese, and Toisanese) | Help-seeking was most often initiated by family members or formal care providers Lack of a final diagnosis: more commonly reported by Chinese Americans compared with Anglos and African Americans Fragmentation in the referral process was common across all groups. Four general types of pathways to diagnosis: Smooth pathways/fragmented pathways/crisis pathways/dead-ended pathways |
| Hugh et al. (2009) [43] | U.S. Community (urban and rural) (A dementia outreach partnership) | Qualitative study Face-to-face semi-structured interview Health belief model Family caregivers of dementia patients -Daughters, spouses, sons, siblings n = 17 | African American | Not knowledgeable about AD prior to their family diagnosed Knew that there is no known cure and expected a continued decline Almost half attributed a change in cognition was normal, age-related memory loss Some caregivers received support or resistance from other family member A supportive social network facilitated a diagnosis. Perplexing behavior and an increasing loss of ability are seen as cues to action |
| Leung et al. (2011) [44] | Canada Community and clinic (urban) (Alzheimer’s Society, posters) Patients: >55 years | Qualitative study Semi-structured interview Dyads of patients with dementia and family caregivers -Caregivers: wives, daughter, son-in-law, husband n = 6 dyads (7 caregivers) | Anglo-Canadian English | Symptom recognition to a dementia diagnosis 2–4 years Demented patients noticing memory difficulties earlier than careers but perceived as ambiguous and normalized or attributed to current health problem Diagnosis process was multiple visits and interactions with health professionals, obtained as more severe cognitive deficit emerged |
| Koehn et al. (2012) [45] | Canada Community (urban) (Chinese Resource Center of Alzheimer’s Society) | Qualitative study Semi-structured interview A Help-seeking Model Dyads of patients with probable dementia and their careers -Caregivers: wives, husband, daughter n = 10 dyads | Chinese Canadian Cantonese or Mandarin | The average pre-diagnosis interval: 1.5 years Caregivers and patients reported a diversity of experiences regarding the early symptoms of the patients’ cognitive deficit. Normalized of early symptoms Decision to seek care was made by family member, either spouse or consulted with adult children Two diagnosed done during acute care admission The role of family caregivers was more influenced by structural factors than by traditional Chinese cultural norms about family responsibilities and filial piety. 60% of the dyads experienced delays in diagnosis because Chinese family doctors dismissed the caregivers’ appraisals of the patients’ symptoms. Gender-based power imbalance between female family caregivers and male Chinese Canadian physicians |
| McCleary et al. (2012) [46] | Canada Community (urban) (Adult daycare center and flyers to community health center, local Alzheimer’s Society) Patient: >70 years | Descriptive qualitative study Semi-structured interview Dyads of patients with dementia and either one or two of their family careers -Caregivers: wives, daughters, daughter-in-law, husband, son, son-in-law n = 6 dyads | South Asian-Canadian English, Hindi, or Tamil | Early signs of dementia were seen as normal that are related to the aging process or patients’ personality characteristics. Seek attention when dementia symptoms were worsened after episodes Health seeking was delayed up to four years, even with significant dementia symptoms Safety concerns, new symptoms, treatment for other health problem influenced the recognition of a health problem |
| Garcia et al. (2013) [37] | Canada Clinic setting (a memory disorder clinic) Patients: >60 years | Qualitative study Semi-structured interview Dyads of patients with dementia and family or friends -Caregivers: spouses, daughters n = 7 dyads | French-speaking Canadian French | Estimated first suspicion of a problem to an official diagnosis: 1–7 years Not easy to identify signs and symptoms Lack of knowledge about the importance of the changes they were experiencing. No single symptoms sufficient to alert participants Preferentially sought from francophone Recognition to consultation with family physician from 4 months to 6 years. All final diagnoses were made by specialists, but family physicians clearly suspected dementia Variety of reasons for the delay. |
| Dimensions | Definitions | Findings: Empirical Statements | Measures/ Example Items |
|---|---|---|---|
| Noticing symptoms | Noticing first signs and symptoms | “I heard the word, but I did not pay much attention to it” Usually normalized or attribute to other health problems. (Hugh et al. 2009) [43] | “The first ADRD symptoms were observed” (Clark et al. 2005) [28] |
| Recognizing a problem | Recognize the signs and symptoms as problems | Multiples signs and symptoms, more cognitive and behavior changes, symptoms getting worse and increasing loss of ability. (McCleary et al. 2013) [46] | “Caregiver’s recognition that a problem existed” (Clark et al. 2005) [28] |
| Accepting Screen | Acknowledging that there is a problem that needs to change | Accumulation of subtle changes including issues with hygiene, finance, or safety in combination with forgetfulness; Consider harm and benefit of screening. (Garcia et al. 2013) [47] | Modified SAPH * “I would like to know if I have a problem with my memory that may indicate that I’m developing dementia” (Holsinger et al. 2011) [29] |
| Intending Screen | Intention or willingness undergo screen | “No critical event either physical or cognitive symptoms to trigger their desire to seek care” “Concerns safety is cue” (Leung et al. 2011) [44] | “Plan to screen for AD at some point in life” “Plan to screen for AD in the next year” “Plan to screen for AD after the participant reaches a certain age” “Plan to screen for AD in the presence of symptoms for AD” (Park et al. 2020) [36] |
| Action | Taking actions to assess the symptoms | Diagnosis process was multiple visits and interactions with health professionals. (Leung et al. 2011) [44] | Ever participated in screen procedures “Patients completed the MMSE, CSI-D, or TICS” (Harrawood et al. 2018) [35] |
| Integrating with time | Timeliness of receiving a clinical diagnosis; Delays in diagnosis of ADRD | Delays due to not only the trajectory of the disease and patients’ personality but also to the types of caregivers. (Koehn et al. 2012) [45] There was no single common pathway from recognition to action. (McCleary et al. 2013) [46] | “The first observed ADRD symptoms to first physician visit” (Clark et al. 2005) [28] |
| Non-Hispanic Black vs. White | ||||
|---|---|---|---|---|
| Subgroups | Findings | |||
| Reference | Outcome | Value | Reference Group (Non-Hispanic White) | |
| Non-Hispanic Black | Fowler et al. (2015) [31] | Accepted screening | ||
| Urban hospital | 60.3% | 63.1% | ||
| Network of urban and suburban hospitals and outpatient care centers | 66.3% | 63.6% | ||
| Folwer et al. (2012) [30] | Undergo screening | 89.5% | 90.4% | |
| Harrawood et al. (2018) [35] | Screened positive for dementia | 11.7% | 9% † | |
| Lin et al., (2021) [37] | Dementia diagnosis without delay | 54.5% | 59.3% | |
| Missed or delayed dementia diagnosis | 45.5% | 40.8% | ||
| Amjad et al. (2018) [34] | Undiagnosed vs. diagnosed dementia | Adjusted OR 1.26 ‡ | - | |
| Unaware vs. aware of dementia diagnosis | Adjusted OR 0.73 ‡ | |||
| Gianattasio et al. (2019) [7] | Underdiagnosed | Adjusted PR 1.35–2.33 | - | |
| Hinton et al. (2004) [42] | Lack of a final diagnosis | 20% | 7% | |
| Latino/Hispanic vs. White | ||||
| Subgroups | Findings | |||
| Reference | Outcome | Value | Reference group (Non-Hispanic White) | |
| Hispanic | Lin et al. (2021) [37] | Dementia diagnosis without delay | 45.8% | 59.3% |
| Missed or delayed dementia diagnosis | 54.2% | 40.8% | ||
| Amjad et al. (2018) [34] | Undiagnosed vs. diagnosed dementia | Adjusted OR 2.48 | - | |
| Unaware vs. aware of dementia diagnosis | Adjusted OR 0.87 ‡ | - | ||
| Asian vs. White | ||||
| Subgroup | Findings | |||
| Reference | Outcome | Value | Reference group (Non-Hispanic White) | |
| Chinese | Hinton et al. (2004) [42] | Lack of a final diagnosis | 43% | 7% |
| Other vs. White | ||||
| Subgroup | Findings | |||
| Reference | Outcome | Value | Reference group (Non-Hispanic White) | |
| Other | Fowler et al. (2015) [31] | Accepted screening | ||
| Urban hospital | 33.3% | 63.1% | ||
| Network of urban and suburban hospitals and outpatient care centers | 100% | 63.6% | ||
| Fowler et al. (2012) [30] | Undergo screening | 87.5% | 90.4% | |
| Non-White | Savva et al. (2015) [32] | Prior diagnosis of dementia (weighted) | 48% | 41.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Kim, D.; Lee, H. Examine Race/Ethnicity Disparities in Perception, Intention, and Screening of Dementia in a Community Setting: Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 8865. https://doi.org/10.3390/ijerph19148865
Lee S, Kim D, Lee H. Examine Race/Ethnicity Disparities in Perception, Intention, and Screening of Dementia in a Community Setting: Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(14):8865. https://doi.org/10.3390/ijerph19148865
Chicago/Turabian StyleLee, SangA, Deogwoon Kim, and Haeok Lee. 2022. "Examine Race/Ethnicity Disparities in Perception, Intention, and Screening of Dementia in a Community Setting: Scoping Review" International Journal of Environmental Research and Public Health 19, no. 14: 8865. https://doi.org/10.3390/ijerph19148865
APA StyleLee, S., Kim, D., & Lee, H. (2022). Examine Race/Ethnicity Disparities in Perception, Intention, and Screening of Dementia in a Community Setting: Scoping Review. International Journal of Environmental Research and Public Health, 19(14), 8865. https://doi.org/10.3390/ijerph19148865