
Association between Health Literacy and Prevalence of Obesity, Arterial Hypertension, and Diabetes Mellitus

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Issues
2.2. Statistical Analysis
3. Results
3.1. Morbidity and Nutritional Status of Study Patients
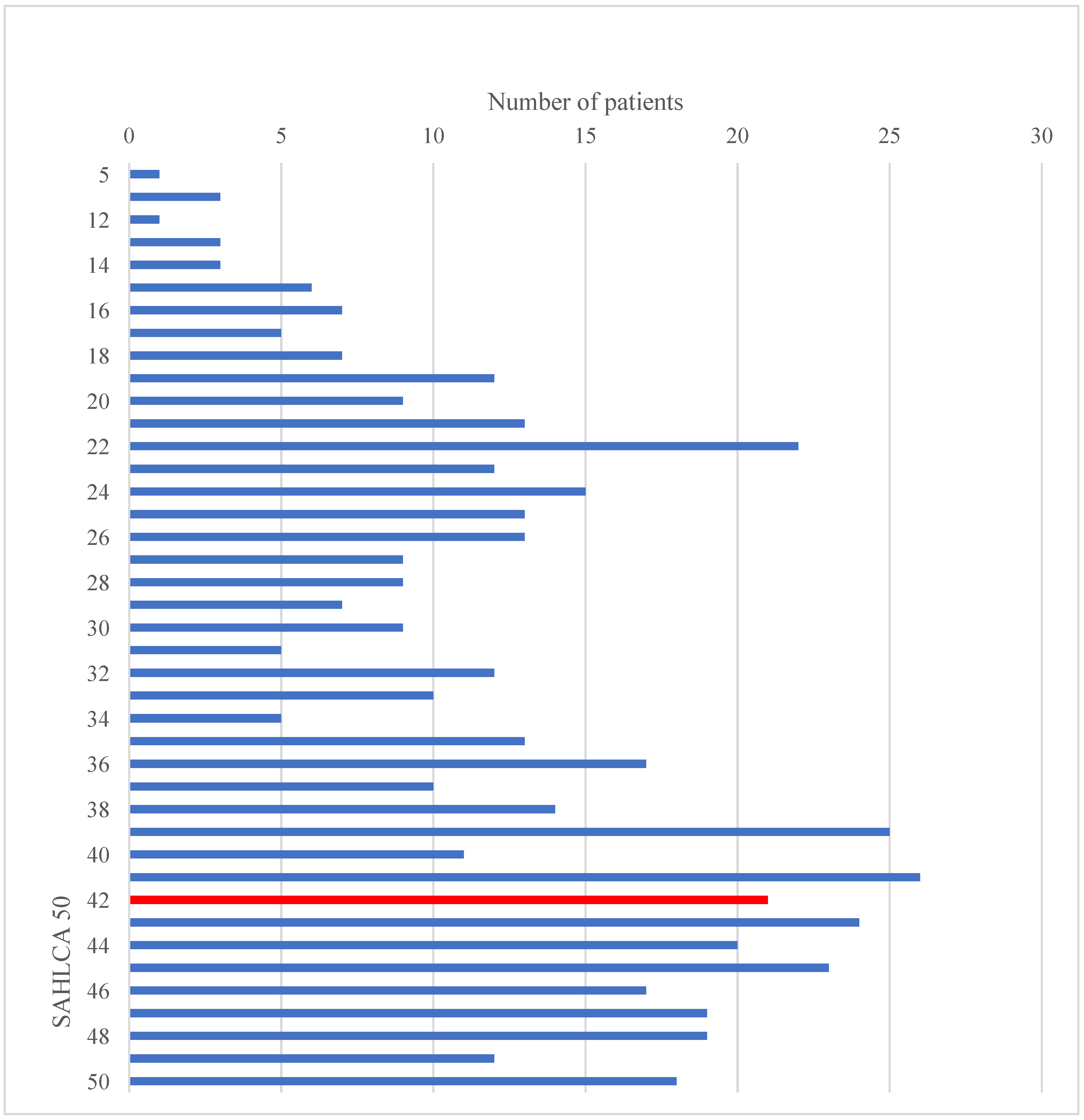
3.2. Health Literacy
3.3. Association between Health Literacy and Patient Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 5 April 2021).
- World Health Organization (WHO). Noncommunicable Diseases Progress Monitor 2020. Available online: https://www.who.int/publications/i/item/ncd-progress-monitor-2020 (accessed on 5 April 2021).
- GBD 2013 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Padwal, R.; Straus, S.E.; McAlister, F.A. Cardiovascular risk factors and their effects on the decision to treat hypertesion: Evidence-based review. BMJ 2001, 322, 977–980. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular disease: Risk factor, paradox, and impact of weight loss. J. Am. Col. Cardiol. 2009, 53, 1925–1932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Lim, D.H.; Kim, Y. Classification and Prediction on the Effects of Nutritional Intake on Overweight/Obesity, Dyslipidemia, Hypertension and Type 2 Diabetes Mellitus Using Deep Learning Model: 4–7th Korea National Health and Nutrition Examination Survey. Int J. Environ. Res. Public Health 2021, 18, 5597. [Google Scholar] [CrossRef]
- Piché, M.E.; Tchernof, A.; Després, J.P. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ. Res. 2020, 126, 1477–1500. [Google Scholar] [CrossRef]
- Stefan, N.; Häring, H.U.; Schulze, M.B. Metabolically healthy obesity: The low-hanging fruit in obesity treatment? Lancet Diabetes Endocrinol. 2018, 6, 249–258. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Kasperczyk, S.; Osadnik, T.; Pawlas, N. oxidative stress in association with metabolic health and obesity in young adults. Oxid. Med. Cell. Longev. 2021, 2021, 9987352. [Google Scholar] [CrossRef]
- Stanek, A.; Brożyna-Tkaczyk, K.; Myśliński, W. Oxidative Stress Markers among Obstructive Sleep Apnea Patients. Oxid Med. Cell Long. 2021, 2021, 9681595. [Google Scholar] [CrossRef]
- Stanek, A.; Brożyna-Tkaczyk, K.; Myśliński, W. The role of obesity-induced perivascular adipose tissue (PVAT) dysfunction in vascular homeostasis. Nutrients 2021, 13, 3843. [Google Scholar] [CrossRef]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Hrabak Žerjavić, V.; Kralj, V.; Dika, Ž.; Jelaković, B. Epidemiology of hypertension, stroke and myocardial infarction in Croatia. Medix 2010, 16, 102–107. [Google Scholar]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- IDF. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation IDF: Brussels, Belgium, 2017; Available online: http://www.diabetesatlas.org/across-the-globe.html (accessed on 15 April 2021).
- Croatian Institute of Public Health. World Diabetes Day 2019. Available online: https://www.hzjz.hr/aktualnosti/svjetski-dan-secerne-bolesti-2019 (accessed on 15 April 2021).
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aune, D.; Sen, A.; Prasad, M.; Norat, T.; Janszky, I.; Tonstad, S.; Romundstad, P.; Vatten, L.J. BMI and all-cause mortality: Systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants. BMJ 2016, 353, i2156. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.-C.; Li, C.-L.; Qi, J.-Y.; Huang, L.-N.; Shi, D.; Du, S.-S.; Liu, L.-Y.; Feng, R.-N.; Sun, C.-H. Relationships of dietary histidine and obesity in Northern Chinese adults, an internet-based cross-sectional study. Nutrients 2016, 8, 420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of Obesity in the United States, 2009-2010. NCHS Data Brief 2012, 82, 1–8. [Google Scholar]
- World Health Organization Data and Statistics. Available online: https://www.euro.who.int/en/health-topics/noncommunicable-diseases/obesity/data-and-statistics (accessed on 12 April 2021).
- Croatian Institute of Public Health. Department of Physical Health Promotion. Available online: https://www.hzjz.hr/sluzba-promicanje-zdravlja/odjel-za-prevenciju-debljine (accessed on 10 August 2021).
- Quick, V.M.; McWilliams, R.; Byrd-Bredbenner, C. Fatty, fatty, two-by-four: Weight-teasing history and disturbed eating in young adult women. Am. J. Public Health 2013, 103, 508–515. [Google Scholar] [CrossRef]
- Wang, H.; Steffen, L.M.; Zhou, X.; Harnack, L.; Luepker, R.V. Consistency between increasing trends in added-sugar intake and body mass index among adults: The Minnesota heart survey, 1980–1982 to 2007–2009. Am. J. Public Health 2013, 103, 501–507. [Google Scholar] [CrossRef]
- Block, J.P.; Scribner, R.A.; DeSalvo, K.B. Fast food, race/ethnicity, and income: A geographic analysis. Am. J. Prevent Med. 2004, 27, 211–217. [Google Scholar] [CrossRef]
- Corral, I.; Landrine, H.; Hao, Y.; Zhao, L.; Mellerson, J.L.; Cooper, D.L. Residential segregation, health behavior and overweight/obesity among a national sample of African American adults. J. Health Psychol. 2012, 17, 371–378. [Google Scholar] [CrossRef]
- Ma, Y.; Hébert, J.R.; Manson, J.E.; Balasubramanian, R.; Liu, S.; Lamonte, M.J.; Bird, C.E.; Ockene, J.K.; Qiao, Y.; Olendzki, B.; et al. Determinants of racial/ethnic disparities in incidence of diabetes in postmenopausal women in the U.S.: The women’s health initiative 1993–2009. Diabetes Care 2012, 35, 2226–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Liu, M.; Tsilimingras, D.; Schiffrin, E.L. Racial disparities in cardiovascular risk factors among diagnosed hypertensive subjects. J. Am. Soc. Hypertens. 2011, 5, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Dehal, A.; Garrett, T.; Tedders, S.H.; Arroyo, C.; Afriyie-Gyawu, E.; Zhang, J. Body mass index and death rate of colorectal cancer among a national cohort of U.S. adults. Nutr. Cancer. 2011, 63, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Rahmawati, R.; Bajorek, B. Understanding untreated hypertension from patients’ point of view: A qualitative study in rural Yogyakarta province, Indonesia. Chronic Illn. 2018, 14, 228–240. [Google Scholar] [CrossRef]
- AbuAlreesh, A.; Alburikan, K.A. Health literacy among patients with poor understanding of prescription drug label instructions in Saudi Arabia. Saudi Pharm. J. 2019, 27, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health Literacy in Europe: Comparative Results of the European Health Literacy Survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [Green Version]
- Lovrić, B.; Jovanović, T.; Jakovljević, P. Adolescents’ Health Literacy. Holistic Approach to the Patient, Conference Proceedings, International Scientific Conference. Food Health Dis. 2018, 10, 9–10. Available online: https://hrcak.srce.hr/clanak/319057 (accessed on 19 April 2022).
- Brangan, S.; Ivanišić, M.; Rafaj, G.; Rowlands, G. Health literacy of hospital patients using a linguistically validated Croatian version of the Newest Vital Sign screening test (NVS-HR). PLoS ONE 2018, 13, e0193079. [Google Scholar] [CrossRef] [Green Version]
- Placento, H.; Lovrić, B.; Gvozdanović, Z.; Farčić, N.; Jovanović, T.; Jovanović, J.T.; Zibar, L.; Prlić, N.; Mikšić, Š.; Jovanović, N.B.; et al. Croatian version of the Short Assessment of Health Literacy for Spanish Adults (SAHLSA-50): Cross-cultural adaptation and psychometric evaluation. Healthcare 2022, 10, 111. [Google Scholar] [CrossRef]
- Lee, S.-Y.D.; Bender, D.E.; Ruiz, R.E.; Cho, Y.I. Development of an easy-to-use Spanish Health Literacy Test. Health Serv. Res. 2006, 41, 1392–1412. [Google Scholar] [CrossRef] [Green Version]
- Berlančić, T.; Kuharić, M.; Janković, D.; Milić, J.; Badak, K.; Zibar, L. Croatian translation and linguistic adaptation of the Short Assessment of Health Literacy for Spanish Adults (SAHLSA-50). Southeast. Eur. Med. J. SEEMEDJ 2020, 4, 121–128. [Google Scholar] [CrossRef]
- Armitage, P.; Berry, G. Statistical Methods in Medical Research; WileyBlackwell: Hoboken, NJ, USA, 2001. [Google Scholar]
- MedCalc Software Ltd.: Ostend, Belgium, 2020. Available online: https://www.medcalc.org (accessed on 12 April 2021).
- IBM Corp. IBM SPSS Statistics for Windows; IBM Corp.: Armonk, NY, USA, 2017; Available online: https://hadoop.apache.org (accessed on 19 April 2021).
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. ESC Scientific Document Group, 2018 ESC/ESH Guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 1, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- IDF. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation IDF: Brussels, Belgium, 2019; Available online: https://www.diabetesatlas.org/en (accessed on 7 April 2021).
- Bailey, S.C.; Brega, A.G.; Crutchfield, T.M.; Elasy, T.; Herr, H.; Kaphingst, K.; Karter, A.J.; Moreland-Russell, S.; Osborn, C.Y.; Pignone, M.; et al. Update on Health Literacy and Diabetes. Diabetes Educ. 2014, 40, 581–604. [Google Scholar] [CrossRef]
- Cavanaugh, K.L. Health literacy in diabetes care: Explanation, evidence and equipment. Diab. Manag. 2011, 1, 191–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullah, A.; Liew, S.M.; Salim, H.; Ng, C.J.; Chinna, K. Prevalence of limited health literacy among patients with type 2 diabetes mellitus: A systematic review. PLoS ONE 2019, 7, e0216402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLeod, S.; Musich, S.; Gulyas, S.; Cheng, Y.; Tkatch, R.; Cempellin, D.; Bhattarai, G.R.; Hawkins, K.; Yeh, C.S. The impact of inadequate health literacy on patient satisfaction, healthcare utilization, and expenditures among older adults. Geriatr. Nurs. 2017, 38, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Geboers, B.; de Winter, A.F.; Spoorenberg, S.L.; Wynia, K.; Reijneveld, S.A. The association between health literacy and self-management abilities in adults aged 75 and older, and its moderators. Qual. Life Res. 2016, 25, 2869–2877. [Google Scholar] [CrossRef] [Green Version]
- Mancuso, J.M. Impact of health literacy and patient trust on glycemic control in an urban USA population. Nurs. Health Sci. 2010, 12, 94–104. [Google Scholar] [CrossRef]
- DeWalt, D.A.; Boone, R.S.; Pignone, M.P. Literacy and its relationship with self-efficacy, trust, and participation in medical decision making. Am. J. Health Behav. 2007, 31, 27–35. [Google Scholar] [CrossRef]
- McCray, A.T. Promoting health literacy. J. Am. Med. Inform. Assoc. 2005, 12, 152–163. [Google Scholar] [CrossRef] [Green Version]
- Tarekegne, F.E.; Padyab, M.; Schröders, J.; Stewart Williams, J. Sociodemographic and behavioral characteristics associated with self-reported diagnosed diabetes mellitus in adults aged 50+ years in Ghana and South Africa: Results from the WHO-SAGE wave 1. BMJ Open Diabetes Res. Care 2018, 2, e000449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, X.-y.; Lin, J.; Gu, W.-w. Risk factors and therapies in vascular diseases: An umbrella review of updated systematic reviews and meta-analyses. J. Cell. Physiol. 2019, 234, 8221–8232. [Google Scholar] [CrossRef] [PubMed]
- Igel, L.I.; Saunders, K.H.; Fins, J.J. Why weight? An analytic review of obesity management, diabetes prevention, and cardiovascular risk reduction. Curr. Atheroscler. Rep. 2018, 21, 39. [Google Scholar] [CrossRef] [PubMed]
- Cripps, C.; Roslin, M. Endoluminal treatments for obesity and related hypertension: Updates, review, and clinical perspective. Curr. Hypertens. Rep. 2016, 18, 79. [Google Scholar] [CrossRef]
- Eurostat. Over Half of Adults in the EU Are Overweight. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20210721-2 (accessed on 12 August 2021).
- Kamatham, S.; Trak, J.; Alzouhayli, S.; Fehmi, Z.; Rahoui, N.; Sulieman, N.; Khoury, Z.; Fehmi, O.; Rakine, H.; El-Masri, D.; et al. Characteristics and distribution of obesity in the Arab American population of southeastern Michigan. BMC Public Health 2020, 20, 1685. [Google Scholar] [CrossRef]
- Toçi, E.; Burazeri, G.; Kamberi, H.; Toçi, D.; Roshi, E.; Jerliu, N.; Bregu, A.; Brand, H. Health literacy and body mass index: A population-based study in a South-Eastern European country. J. Public Health 2021, 43, 123–130. [Google Scholar] [CrossRef]
- Gurgel do Amaral, M.S.; Reijneveld, S.A.; Geboers, B.; Navis, G.J.; Winter, A.F. Low health literacy is associated with the onset of CKD during the life course. J. Am. Soc. Nephrol. JASN 2021, 32, 1436–1443. [Google Scholar] [CrossRef]
- Al-Ruthia, Y.S.; Balkhi, B.; AlGhadeer, S.; Mansy, W.; AlSanawi, H.; AlGasem, R.; AlMutairi, L.; Sales, I. Relationship between health literacy and body mass index among Arab women with polycystic ovary syndrome. Saudi Pharm. J. SPJ 2017, 25, 1015–1018. [Google Scholar] [CrossRef]
- Lam, L.T.; Yang, L. Is low health literacy associated with overweight and obesity in adolescents: An epidemiology study in a 12–16 years old population, Nanning, China, 2012. Arch. Public Health 2014, 1, 11. [Google Scholar] [CrossRef] [Green Version]
- Moghaddam, R.; Mokhtari Lakeh, N.; Rahebi, S.M.; Leili, E.K. Health literacy and its relationship with body mass index. J. Holist. Nurs. Midwifery 2019, 29, 130–136. [Google Scholar] [CrossRef]
- Vozikis, A.; Drivas, K.; Milioris, K. Health literacy among university students in Greece: Determinants and association with self-perceived health, health behaviours and health risks. Arch. Public Health 2014, 72, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esna Ashari, F.; Pirdehghan, A.; Rajabi, F.; Sayarifard, A.; Ghadirian, L.; Rostami, N.; Pirdehghan, M. The study of health literacy of staff about risk factors of chronic diseases in 2014. Avicenna J. Clin. Med. 2015, 22, 248–254. [Google Scholar]
- Zhang, F.; Or, P.; Chung, J. How different health literacy dimensions influences health and well-being among men and women: The mediating role of health behaviours. Health Expect. 2021, 24, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, D.; Berens, E.; Vogt, D.; Gille, S.; Griese, L.; Klinger, J.; Hurrelmann, K. Health literacy in Germany: Findings of a representative follow-up survey. Dtsch. Arztebl. Int. 2021, 118, 723–729. [Google Scholar] [CrossRef]
- Santos, H.C.; Varnum, M.E.W.; Grossmann, I. Global increases in individualism. Psychol. Sci. 2017, 28, 1228–1239. [Google Scholar] [CrossRef] [Green Version]
- Marconcin, P.; Matos, M.G.; Ihle, A.; Ferrari, G.; Gouveia, É.R.; López-Flores, M.; Peralta, M.; Marques, A. Trends of healthy lifestyles among adolescents: An analysis of more than half a million participants from 32 countries between 2006 and 2014. Front. Pediatr. 2021, 25, 645074. [Google Scholar] [CrossRef]
- Lim, S.; Beauchamp, A.; Dodson, S.; O’Hara, J.; McPhee, C.; Fulton, A.; Wildey, C.; Osborne, R.H. Health literacy and fruit and egetable intake in rural Australia. Public Health Nutr. 2017, 20, 2680–2684. [Google Scholar] [CrossRef] [Green Version]
- Gazmararian, J.A.; Baker, D.W.; Williams, M.V.; Parker, R.M.; Scott, T.L.; Green, D.C.; Fehrenbach, S.N.; Ren, J.; Koplan, J.P. Health literacy among medicare enrollees in a managed care organization. JAMA 1999, 281, 545–551. [Google Scholar] [CrossRef] [Green Version]
- Saunders, C.; Palesy, D.; Lewis, J. Systematic review and conceptual framework for health literacy training in health professions education. Health Prof. Educ. 2019, 5, 13–29. [Google Scholar] [CrossRef]
- Kaper, M.S.; de Winter, A.F.; Bevilacqua, R.; Giammarchi, C.; McCusker, A.; Sixsmith, J.; Koot, J.A.R.; Reijneveld, S.A. Positive outcomes of a comprehensive health literacy communication training for health professionals in three European countries: A multi-centre pre-post intervention study. Int. J. Environ. Res. Public Health 2019, 16, 3923. [Google Scholar] [CrossRef] [Green Version]
- Harzheim, L.; Lorke, M.; Woopen, C.; Jünger, S. Health literacy as communicative action—A qualitative study among persons at risk in the context of predictive and preventive medicine. Int. J. Environ. Res. Public Health 2020, 17, 1718. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Guo, Y. The effect of socio-economic status on health information literacy among urban older adults: Evidence from western China. Int. J. Environ. Res. Public Health 2021, 18, 3501. [Google Scholar] [CrossRef] [PubMed]
- Gvozdanović, Z.; Farčić, N.; Šimić, H.; Buljanović, V.; Gvozdanović, L.; Katalinić, S.; Pačarić, S.; Gvozdanović, D.; Dujmić, Ž.; Miškić, B.; et al. The impact of education, COVID-19 and risk factors on the quality of life in patients with type 2 diabetes. Int. J. Environ. Res. Public Health 2021, 18, 2332. [Google Scholar] [CrossRef] [PubMed]
- Finbråten, H.S.; Guttersrud, Ø.; Nordström, G.; Pettersen, K.S.; Trollvik, A.; Wilde-Larsson, B. Explaining variance in health literacy among people with type 2 diabetes: The association between health literacy and health behaviour and empowerment. BMC Public Health 2020, 20, 161. [Google Scholar] [CrossRef] [PubMed]
- Rondia, K.; Adriaenssens, J.; Van Den Broucke, S.; Kohn, L. Health Literacy: What Lessons Can Be Learned from the Experiences of Other Countries? Available online: https://kce.fgov.be/sites/default/files/atoms/files/KCE_322_Health_Literacy_Report.pdf (accessed on 10 August 2021).
- Berkman, N.D.; Dewalt, D.A.; Pignone, M.P.; Sheridan, S.L.; Lohr, K.N.; Lux, L.; Sutton, S.F.; Swinson, T.; Bonito, A.J. Literacy and health outcomes: Summary. In AHRQ Evidence Report Summaries; Evidence Report/Technology Assessment No. 87; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2004. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11942 (accessed on 15 August 2021).
- Cost of Non-Communicable Diseases in the EU. Available online: https://knowledge4policy.ec.europa.eu/health-promotion-knowledge-gateway/cost-non-communicable-diseases-eu_e (accessed on 10 August 2021).


{kind=link}
| Associated Disease | n (%) |
|---|---|
| Arterial hypertension | 262 (52.4) |
| T2DM | 132 (26.4) |
| Arterial hypertension and T2DM | 110 (22) |
| Either arterial hypertension or T2DM | 174 (34.8) |
| Neither arterial hypertension nor T2DM | 216 (43.2) |
| Characteristic | Median (Interquartile Range) |
|---|---|
| Body weight (kg) | 80 (70–90) |
| Body height (cm) | 170 (163–175) |
| Body mass index (BMI) (kg/m2) | 27.44 (24.45–31.02) |
| Nutritional status: | n (%) |
| Underweight (BMI ≤ 18.5 kg/m2) | 6 (1.2) |
| Normal weight (18.5 ≤ BMI ≤ 24.9 kg/m2) | 140 (28) |
| Overweight (25.0 ≤ BMI ≤ 29.9 kg/m2) | 196 (39.2) |
| Obesity I (30.0 ≤ BMI ≤ 34.9 kg/m2) | 108 (21.6) |
| Obesity II (35.0 ≤ BMI ≤ 39.9 kg/m2) | 26 (5.2) |
| Obesity III (BMI ≥ 40.0 kg/m2) | 24 (4.8) |
| Characteristic | Median (Interquartile Range) SAHLCA-50 | p | |
|---|---|---|---|
| Gender: | |||
| Male | 36 (25–42) | † Difference = 3 95% CI = 1–4 | 0.004 * |
| Female | 39 (26–5) | ||
| Age group (years): | |||
| <30 | 44 (39–47) | H test = 123.4 df = 4 | <0.001 ‡ § |
| 31–40 | 44 (39–48) | ||
| 41–50 | 43 (34–46) | ||
| 51–60 | 41 (36–44) | ||
| ≥61 | 28 (22–39) | ||
| Level of education: | |||
| Incomplete elementary school | 22 (18–26) | H test = 246.1 df = 4 | <0.001 ‡ †† |
| Elementary school | 26 (22–34) | ||
| High school | 41 (36–45) | ||
| College | 45 (41–48) | ||
| University degree or higher | 47 (44–49) | ||
| Employment status: | |||
| Employed | 43 (38–47) | H test = 113.3 df = 3 | <0.001 ‡ §§ |
| Unemployed | 41 (33–45) | ||
| Occasionally employed | 43 (33–45) | ||
| Retired | 28 (22–39) |
| Characteristic | n (%) | p * | ||
|---|---|---|---|---|
| Adequate Health Literacy (n = 173) (42–50 points) | Inadequate Health Literacy (n = 327) (0–41 points) | Total | ||
| Gender: | ||||
| Male | 55 (26) | 156 (74) | 211 (42) | 0.001 |
| Female | 118 (41) | 171 (59) | 289 (58) | |
| Age group (years): | ||||
| <30 | 43 (64) | 24 (36) | 67 (13) | <0.001 |
| 31–40 | 34 (63) | 20 (37) | 54 (11) | |
| 41–450 | 21 (60) | 14 (40) | 35 (7) | |
| 51–460 | 25 (38) | 41 (62) | 66 (13) | |
| ≥61 | 50 (18) | 228 (82) | 278 (56) | |
| Place of residence: | ||||
| Rural | 72 (25) | 221 (75) | 293 (59) | <0.001 |
| Urban | 101 (49) | 106 (51) | 207 (41) | |
| Level of education: | ||||
| Incomplete elementary school | 1 (1) | 81 (99) | 82 (16) | <0.001 |
| Elementary school | 6 (6) | 100 (94) | 106 (21) | |
| High school | 111 (45) | 133 (55) | 244 (49) | |
| College | 21 (72) | 8 (28) | 29 (6) | |
| University and higher | 34 (87) | 5 (13) | 39 (8) | |
| Employment status: | ||||
| Employed | 82 (60) | 55 (40) | 137 (27) | <0.001 |
| Unemployed | 37 (44) | 47 (56) | 84 (17) | |
| Occasionally employed | 3 (75) | 1 (25) | 4 (1) | |
| Retired | 51 (19) | 224 (81) | 275 (55) | |
| Characteristic | n (%) | p * | ||
|---|---|---|---|---|
| Adequate Health Literacy (42–50 points) | Inadequate Health Literacy (0–41 points) | Total | ||
| Arterial hypertension (AH): | ||||
| Yes | 108 (45) | 130 (55) | 238 (48) | <0.001 |
| No | 65 (25) | 197 (75) | 262 (52) | |
| Type 2 diabetes mellitus (T2DM): | ||||
| No | 145 (39) | 223 (61) | 368 (74) | <0.001 |
| Yes | 28 (21) | 104 (79) | 132 (26) | |
| AH/T2DM: | ||||
| Both | 23 (21) | 87 (79) | 110 (22) | <0.001 |
| Either AH or T2DM | 47 (27) | 127 (73) | 174 (35) | |
| Neither | 103 (48) | 113 (52) | 216 (43) | |
| Nutritional status: | ||||
| Underweight | 2 (33) | 4 (67) | 6 (1) | 0.7 † |
| Normal weight | 51 (36) | 89 (64) | 140 (28) | |
| Overweight | 71 (36) | 125 (64) | 196 (39) | |
| Obesity | 49 (31) | 109 (69) | 158 (32) | |
| Total | 173 (100) | 327 (100) | 500 (100) | |
| Characteristic | ß | Wald | p | OR | 95% Cl |
|---|---|---|---|---|---|
| Gender (M) | 0.67 | 11.59 | <0.001 | 1.96 | 1.33–2.88 |
| Age group (years): | |||||
| 31–40 | 0.05 | 0.02 | 0.89 | 1.05 | 0.50–2.22 |
| 41–50 | 0.18 | 0.17 | 0.68 | 1.19 | 0.52–2.77 |
| 51–60 | 1.08 | 8.98 | 0.003 | 2.94 | 1.45–5.95 |
| ≥61 | 2.10 | 49.4 | <0.001 | 8.17 | 4.55–14.68 |
| Place of residence (city) | −1.07 | 30.5 | <0.001 | 0.34 | 0.23–0.50 |
| Level of education: | |||||
| College education | 0.95 | 2.25 | 0.13 | 2.59 | 0.75–8.97 |
| High school education | 2.09 | 17.89 | <0.001 | 8.15 | 3.08–21.5 |
| Elementary school | 4.73 | 55.10 | <0.001 | 113.3 | 32.5–395.18 |
| Incomplete elementary school | 6.31 | 32.07 | <0.001 | 550.8 | 62.01–4892.6 |
| Employment status: | |||||
| Unemployed | 0.64 | 5.18 | 0.02 | 1.89 | 1.09–3.28 |
| Part-time employee | −0.69 | 0.36 | 0.55 | 0.49 | 0.05–4.90 |
| Retired | 1.87 | 64.9 | <0.001 | 6.54 | 4.14–10.34 |
| Arterial hypertension (yes) | 0.92 | 22.8 | <0.001 | 2.52 | 1.72–3.67 |
| Type 2 diabetes (yes) | 0.88 | 13.7 | <0.001 | 2.42 | 1.51–3.85 |
| AH/T2DM | |||||
| Both diseases | 1.24 | 20.8 | <0.001 | 3.45 | 2.03–5.87 |
| Pne of the diseases | 0.90 | 17.0 | <0.001 | 2.46 | 1.61–3.78 |
| Nutrition (obese) | |||||
| Underweight | 0.13 | 0.02 | 0.88 | 1.14 | 0.20–6.36 |
| Normal weight | −0.01 | 0.001 | 0.97 | 0.99 | 0.63–1.56 |
| Obesity | 0.23 | 1.06 | 0.30 | 1.26 | 0.81–1.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lovrić, B.; Placento, H.; Farčić, N.; Lipič Baligač, M.; Mikšić, Š.; Mamić, M.; Jovanović, T.; Vidić, H.; Karabatić, S.; Cviljević, S.; et al. Association between Health Literacy and Prevalence of Obesity, Arterial Hypertension, and Diabetes Mellitus. Int. J. Environ. Res. Public Health 2022, 19, 9002. https://doi.org/10.3390/ijerph19159002
Lovrić B, Placento H, Farčić N, Lipič Baligač M, Mikšić Š, Mamić M, Jovanović T, Vidić H, Karabatić S, Cviljević S, et al. Association between Health Literacy and Prevalence of Obesity, Arterial Hypertension, and Diabetes Mellitus. International Journal of Environmental Research and Public Health. 2022; 19(15):9002. https://doi.org/10.3390/ijerph19159002
Chicago/Turabian StyleLovrić, Božica, Harolt Placento, Nikolina Farčić, Metka Lipič Baligač, Štefica Mikšić, Marin Mamić, Tihomir Jovanović, Hrvoje Vidić, Sandra Karabatić, Sabina Cviljević, and et al. 2022. "Association between Health Literacy and Prevalence of Obesity, Arterial Hypertension, and Diabetes Mellitus" International Journal of Environmental Research and Public Health 19, no. 15: 9002. https://doi.org/10.3390/ijerph19159002
APA StyleLovrić, B., Placento, H., Farčić, N., Lipič Baligač, M., Mikšić, Š., Mamić, M., Jovanović, T., Vidić, H., Karabatić, S., Cviljević, S., Zibar, L., Vukoja, I., & Barać, I. (2022). Association between Health Literacy and Prevalence of Obesity, Arterial Hypertension, and Diabetes Mellitus. International Journal of Environmental Research and Public Health, 19(15), 9002. https://doi.org/10.3390/ijerph19159002