1. Introduction
Alcohol Use Disorders (AUDs) constitute highly prevalent and disabling disorders with mean lifetime incidence reaching approximately 8.6% in all countries combined [
1]. A better grasp of etiological risk factors underlying AUDs could prove relevant to inform both prevention and intervention efforts [
2], whose ultimate aim is that of recovery. Notwithstanding, there has been ongoing debate concerning the conceptualization of improvements that define what exactly is meant by “recovery” in persons afflicted with AUDs. Given the heterogeneity of methods in how patients reduce or resolve alcohol-related problems, the characterizations thereof have become increasingly more nuanced over time, encompassing factors such as improved well-being and daily functioning, beyond the mere attainment of abstinence or low-risk drinking [
3]. However, a high relapse ratio and the extreme difficulty of remaining abstinent are still considered core characteristics of alcohol dependence [
4], with relapse being a crucial event occurring in numerous individuals on their path towards recovery from AUD [
5]. In this study, therefore, we sought to shed more light on the determinants and potential predictors of abstinence, considered a necessary condition and prerequisite of “sustained full remission” according to ICD-11 (lasting 1 to 12 months) [
6]. In addition, while there is evidence supporting the predictive role of various psychosocial underpinnings of AUDs, factors related to abstinence/relapse outcomes seem to have been less explored.
There has been a long and ongoing debate on the effect of personality-related factors on alcohol misuse cf. [
7,
8]. Proposed as the most comprehensive conceptualization of personality, the Five Factor model, consisting of five higher-order personality traits, including openness to experience, conscientiousness, extraversion, agreeableness and neuroticism [
9], is still amongst the most widely studied and applied in various conceptual frameworks. Considering this, available meta-analytic evidence suggests higher alcohol consumption in persons with low conscientiousness (responsible for self-control, flexibility, and adherence to social norms), low agreeableness (cooperativeness, kindness, and trust towards others), and high neuroticism (little emotional stability, proneness to anxiety, and sensitivity to negative emotions) [
10]. Next to low agreeableness (compliance and straightforwardness in particular), low conscientiousness (mostly deliberation and dutifulness) and high neuroticism (i.e., impulsiveness and angry hostility), another meta-analysis seems to also implicate certain facets of extraversion (i.e., excitement-seeking) as likely predictors of pathological alcohol use [
11], thus highlighting the associations between the two notions. Regarding facets related to alcohol abuse, past or present diagnoses thereof were found to be linked to low scores on “trust, achievement striving, self-discipline, and dutifulness” and high scores on “impulsiveness, vulnerability, and excitement-seeking” [
12]. Of note, although dimension and facet results across populations may vary, the Five Factor framework does demonstrate common personality characteristics among AUD patients. Likewise, specific personality factors (psychoticism and persistence) and facets (novelty-seeking and impulsiveness) have been shown to serve as usable predictors not only for the very diagnosis of AUD, but also for the risk of relapse in alcohol-dependent samples [
13], or to generally affect drinking outcomes [
14].
Proposed as a key predictor of treatment outcomes and a likely mechanism underlying success in attaining abstinence or drinking reductions in response to treatment, is the psychological construct of self-efficacy [
15]. Self-efficacy may be defined as one’s beliefs concerning their capacity to produce desired performance attainments [
16], determining how much effort and energy they will put into changing an undesired behavior [
16,
17,
18], and predictive of how persistent they will be in the case of initial failure. Of particular interest in alcohol use recovery is
abstinence self-efficacy, i.e., a belief that an individual will be able to abstain from partaking in the undesired activity that is (excessive) drinking [
19]. Given its theorized propensity to mediate behavior change and effective action, abstinence self-efficacy has been reported to also have an effect on alcohol use outcomes, such as predicting the time to first drink and the number of drinks on the first drinking day in individuals who fail to maintain abstinence after treatment [
5]. There is evidence of higher self-efficacy scores in abstainers relative to those who relapsed [
20] and findings suggesting that greater self-efficacy at discharge from treatment may predict abstinence [
21,
22,
23]. There is also further evidence reaffirming the role of self-efficacy in predicting AUD outcomes [
24], and findings to support links between self-efficacy and abstinence with increases in self-efficacy found to lower the likelihood of relapse [
25].
In addition, there is a paucity of evidence on whether there are relationships between personality and self-efficacy in AUD patients, and, if so, whether those may be affected by comorbid depressive symptomatology. Given the high incidence of mood dysregulation in clinical samples [
26], this may be considered a research priority. Depression is frequently associated with at-risk drinking cf. [
27], both being highly prevalent phenomena, with approximately 280 million adults suffering from depressive disorders [
28], 20% of whom meet the diagnostic criteria for AUD [
29]. A role of negative emotionality underpinning addiction pathology [
30], as well as associations between depressive symptomatology and failures in drinking control have been previously demonstrated [
31]. Given the outbreak of the COVID-19 pandemic, whose aftermath has led to the severe deterioration of various aspects of mental health [
32], including depression and substance use disorders, the urgency to identify the links between them warrants prompt investigation.
In light of the harmful effects of compulsive alcohol use on human functioning and the mitigated success of AUD-targeted therapies to date, with relapse rates for substance use disorders reaching 50% [
33], the exploration of their likely underpinnings is both timely and valid. Should specific contributors to altering their outcomes be identified, treatment programs could be optimized to better suit individual patient needs. As described above, previous research found both factors (personality traits and facets and self-efficacy) to be individually linked to alcohol use and/or abstinence/relapse rates. However, no study has investigated how they may interact to affect the risk of relapse. To this end, we sought to examine (i) the effect of personality-related factors, alcohol self-efficacy, and depressive symptoms on attaining abstinence as our primary objective, and to analyze (ii) the potential interactions between the three investigated factors and (iii) their changes over time in a treatment-seeking AUD population as our two secondary objectives.
2. Methods
Fifty-one Polish male (
n = 44; 86.3%) and female (
n = 7; 13.7%) alcohol rehabilitation center inpatients, aged 25 to 62 years (
M = 41.69,
SD = 8.91), were enrolled to participate in an international study on the effect of modern technologies on enhancing treatment as usual (TAU) in the therapy of AUDs (for more information see [
34]). As part of this project, upon screening for eligibility, they were subjected to a baseline interview with the use of the Mini-International Neuro-psychiatric Interview (MINI) for DSM-5 and invited to complete a questionnaire set, including the International Personality Item Pool (IPIP-50), the Alcohol Abstinence Self-Efficacy Scale (AASE) and the Beck Depression Inventory (BDI-II). Following TAU, at a two-month follow-up, forty-five participants (39 males and 6 females) completed a survey concerning post-treatment outcomes, including data regarding abstinence/relapse.
TAU was designed to last for 2 months and include mainly psychological CBT interventions, delivered via individual and group sessions. The treatment consisted of psycho-education, functional analysis of drinking situations, development and practice of coping strategies, problem-solving, and homework. Add-on interventions included tablet-assisted or virtual-reality-based approach/avoidance training programmes (AATP), each consisting of six sessions distributed over the period of 2 weeks and administered to 33 randomly selected participants (31 of whom provided information on abstinence at follow-up). The administered treatment had no effect on the results of the current study. Prior to enrolment, all patients provided their written informed consent to participate.
The eligibility criteria included: (1) written consent to participate in the study; (2) age ≥ 18 years; (3) completed detoxification (if needed); (4) no other SUDs; and (5) no severe psychiatric or neurological comorbidity or terminal somatic illness.
The baseline assessment was conducted with the use of the Mini-International Neuro-psychiatric Interview (MINI) for DSM-5, a structured interview assessing the 17 most prevalent psychiatric diagnoses through a set of yes/no questions [
35,
36].
A personality assessment was performed with the use of the 50-item International Personality Item Pool—a self-report personality questionnaire developed by Goldberg [
37] to measure the Big Five personality traits, as expressed in Costa and McCrae’s [
38] revised NEO personality inventory (NEO-PI-R). The tool is reported to have good validity and reliability (International Personality Item Pool, 2001).
Abstinence efficacy was assessed at two separate time points (baseline and discharge) with the 40-item Alcohol Abstinence Self-Efficacy Scale (AASE), consisting of subject ratings of the temptation to drink/confidence to abstain from alcohol use across 20 different high-risk situations. AASE was reported to demonstrate a solid subscale structure and strong reliability and validity. The scale comprises four five-item subscales labeled
negative affect,
social positive,
physical and other concerns, and
withdrawal and urges. The tool demonstrated no substantive gender differences [
39].
Depressive symptoms were measured at two separate time points, i.e., baseline and discharge (pre- and post-treatment) with the Beck Depression Inventory (BDI-II), a 21-item self-report and a commonly applied psychometric scale enabling assessment of the severity of depression. The tool shows good reliability (Pearson
r = 0.86) and internal consistency values (α = 0.91) [
40].
5. Discussion
In this study, we investigated the postulated effect of personality-related factors, alcohol abstinence self-efficacy, and depressive symptomatology on post-therapy abstinence attainment in a treatment-seeking AUD population.
Against our initial expectations, none of the analyzed factors, i.e., personality traits, facets of alcohol abstinence self-efficacy, or depressive symptoms proved individually significant for abstinence, as reported by our sample at the two-month follow-up. This means that personality profiles, although seemingly significant for the development of AUDs c.f. [
10,
11], do not necessarily need to predict primary treatment outcomes in terms of relapse/abstinence attainment. Although there is evidence for the links between higher order personality factors (i.e., high neuroticism and low conscientiousness) and relapse rates at a 12 months post-treatment follow-up, postulated to remain in line with previous findings [
47], and thus supporting the use of the Five Factor framework in alcohol-dependent cohorts, such findings are not reported across all research in AUD samples. Hence, elsewhere, Foulds et al. [
48] demonstrate that the use of personality instruments other than Cloninger’s Temperament and Personality Questionnaire (TPQ) or Temperament and Character Inventory (TCI), may lack consistency in reporting findings on the links between personality variables and treatment outcomes. This remains in line with the results of Arnau et al. [
49], who report associations between TCI scales, adherence to treatment, and relapse rates in alcoholic outpatients. In their study on the effect of personality on treatment outcomes, Muller et al. [
13] used five different personality assessment tools (NEO 5-Factor Inventory, Temperament and Character Inventory, Eysenck Personality Questionnaire, Eysenck Impulsiveness–Venturesomeness–Empathy Scale and Sensation-Seeking Scale) to find that relapsed patients scored higher in psychoticism, novelty seeking, and impulsiveness, and lower in persistence, none of which are described within the Five Factor framework. This, alongside our results, raises an important question as to whether the use of instruments measuring personality factors according to the Five Factor theory is warranted in alcohol-dependent samples, or perhaps other theoretical models and corresponding tools are a better alternative in both research and practical approaches to predicting treatment outcomes. It can also be noted that as personality is known to affect behavior in a variety of ways, and the effect of personality-related factors on treatment outcomes can occur through mediation, the effect of potential mediating variables is definitely worthy of further investigation.
Likewise, and against our expectations or available evidence cf. [
50], our results suggest no links between alcohol abstinence self-efficacy and abstinence/relapse rates. This suggests that the set of beliefs our patients hold concerning their capacity to refrain from drinking did not relate to their actual ability to do so as manifested behaviorally post-treatment. One way to interpret such a result could be that a likely phenomenon prevalent across our sample is low self-awareness reflected in the limited ability to generate a realistic self-report. More specifically, the participants might be prone to construing a particular self-image that is in fact an illusion of being capable of coping with emerging urges, which is to serve as a means to maintain their fragile self-esteem. This, in turn, could imply deficits within metacognitive processes, i.e., little awareness of their actual behavioral tendencies and/or an unrealistic representation of their true functioning c.f. [
51]. Such meta-cognitive bias could be another way to account for the observed lack of consistency within self-reported vs experimental outcomes.
Similarly, contrary to existing research suggesting that depression symptoms are a significant predictor of addiction treatment outcomes [
52,
53,
54,
55], our findings indicate no relationship between depressive symptomatology and post-therapy abstinence status. (Sub)clinical depression symptoms can develop following acute and prolonged withdrawal from chronic substance misuse. Whether alcohol use precedes depressive symptoms or users reach for it to “self-medicate” and thus alleviate pre-existing depression symptoms, the inability to attain abstinence appears to be significantly connected with depression symptoms [
56]. In our sample, however, the self-reported level of depressive symptoms/subjective emotional distress recorded either at the beginning of or after treatment did not affect whether or not they were going to be capable of controlling the temptation to drink emerging at any time between discharge and a two-month follow-up. This may therefore indicate the potential existence of other factors confounding the elsewhere-postulated relationship between depressive symptoms and abstinence/relapse rates, which makes controlling for other demographic and/or treatment-related variables a good research direction in the future.
Apart from investigating the effect of personality, alcohol self-efficacy, and depressive symptomatology on post-treatment ability to abstain from alcohol use in recovering AUD patients, we also sought to analyze the potential interactions between them, as well as their changes in time as two secondary objectives of the current study. Hence, even though we found no meaningful evidence for the effect of either one of the three investigated factors on post-therapy abstinence, certain other findings are definitely worthy of expanding on.
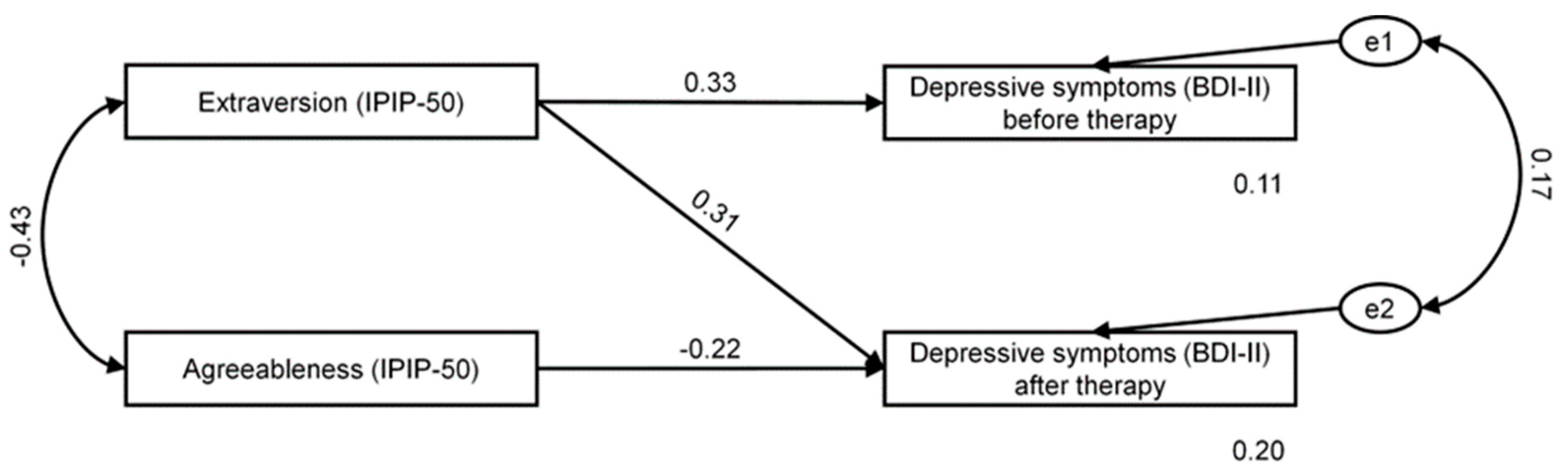
Perhaps somewhat surprisingly, we found extraversion to be significantly linked with depressive symptoms before and after therapy, and to predict their level at admission. In addition, depressive symptomatology at discharge was also negatively correlated with agreeableness. Given that previous findings tended to consider extraversion to be a factor that is generally protective against depression, highlighting its strong negative links to depressive symptoms and diagnoses [
57,
58], our results seem all the more unexpected. Nevertheless, one way they can be accounted for is through the consideration of the fact that more extraverted and socially-inclined individuals may experience more profound negative consequences of social isolation and other restrictions inpatient treatment is known to entail. Secondary outcomes of social distancing may assume the form of negative emotional states such as feelings of loneliness, frustration, concern, or boredom. These, however, do not need to affect all patients in a universal manner. Indeed, it has been proposed that extraversion, a factor involving sociability, assertiveness and high energy levels [
9,
59], could moderate the relationship between measure stringency and mental health problems e.g., [
59,
60,
61,
62,
63]. Hence, although research to date is scarce and yields conflicting results [
64,
65,
66,
67], there are likely disadvantages to being an extravert in situations where severe restrictions and social distancing are in place (or even anticipated), as they inhibit their natural urges for social engagement [
68], pleasure and excitement [
69], or new and exciting surroundings [
70]. Incidentally, our findings are in keeping with research which demonstrates that extraversion might moderate the relationship between measure stringency and depressive symptoms [
71], as the constraints of an inpatient alcohol rehabilitation treatment may in many ways resemble those imposed during the COVID-19 pandemic. In turn, we found greater agreeableness to constitute a protective factor against depressive symptoms at discharge from alcohol treatment, indicating that individuals who are known to be more considerate, friendly, generous, helpful, and to value cooperation and social harmony tended to be less prone to reporting negative affectivity. Such an inverse relationship between self-reported depressed mood and agreeable personality disposition remains in line with previous findings across different cohorts [
72,
73,
74,
75,
76] and suggests a potentially greater capacity to cope with the restrictions of an inpatient treatment while preserving a state of subjective well-being due to more proficient social skills.
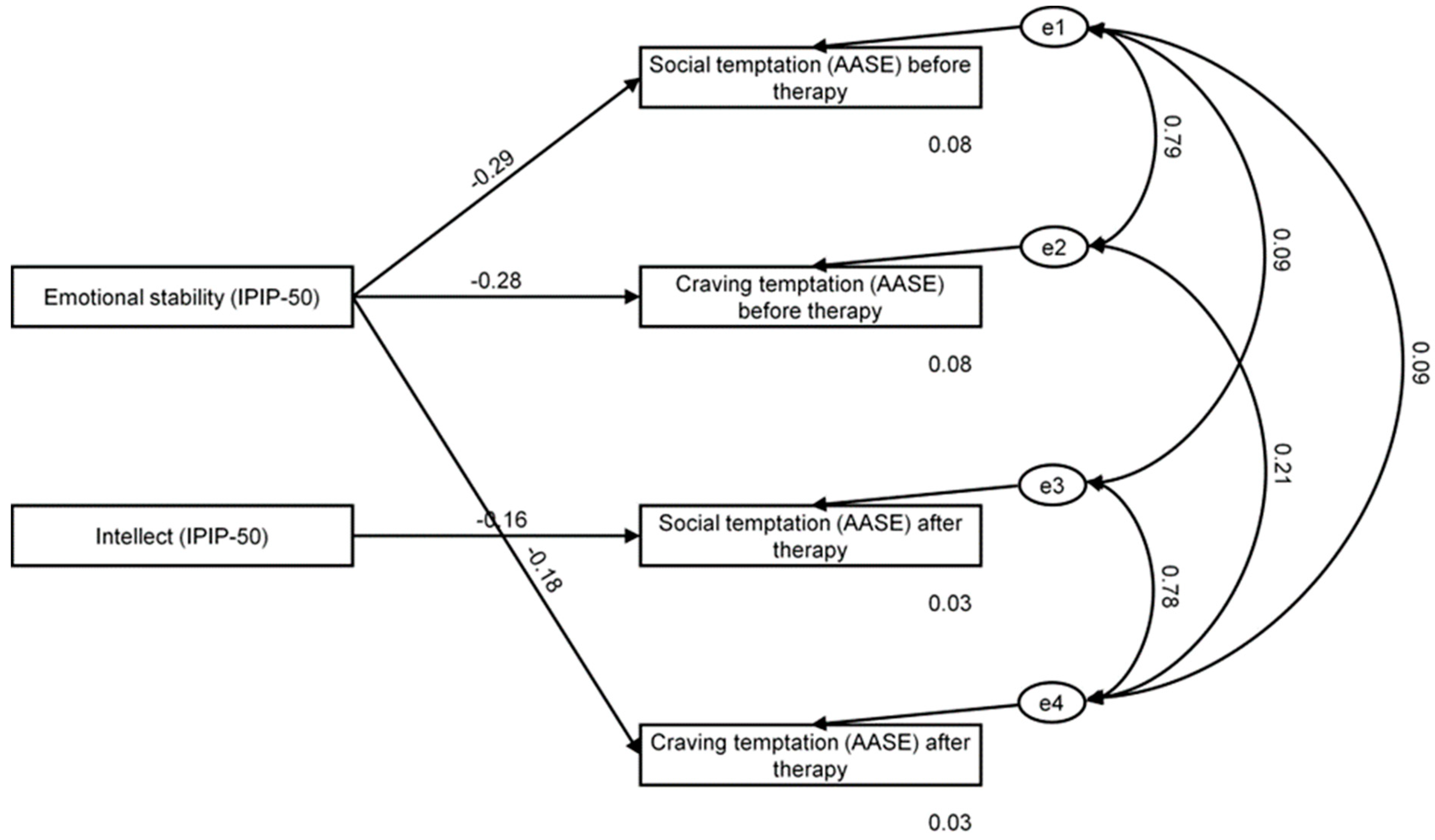
Interestingly, we further revealed significant negative correlations between emotional stability and (i) social/positive factor of AASE temptation at baseline, (ii) craving and urges of AASE temptation at baseline and endpoint, and intellect and endpoint measurement of social/positive factor of AASE temptation, with further analyses suggesting that intellect may in fact constitute a significant predictor thereof, while emotional stability may significantly predict AASE craving and urges at discharge. Such results suggest that higher emotional stability correlates with a lesser-reported tendency to feel tempted to reach for alcohol during social engagements or to boost the subjective state of well-being (i.e., seeing others drinking at a bar or at a party; excited or celebrating with others; when on vacation and wanting to relax; when people they used to drink with encourage them to drink; when offered a drink in a social situation). Of note, however, such an association was only observed at baseline and lost towards discharge. This may mean that an individual disposition to cope with stressful situations in a calm and composed fashion could mitigate the anticipated external pressure to drink or the internal desire to use alcohol as a means to alleviate negative affective states during admission, i.e., at the time when AUD patients are motivated and full of hope that prospective therapy will result in favorable outcomes, and when their actual ability to reach for alcohol (due to imposed restrictions) seems remote. Towards discharge, however, their appraisal of the situation as well as their own feelings may change to become more realistic, especially when the opportunity to use becomes so much more tangible. In turn, and as may have been expected, the negative correlation between emotional stability and craving and urges persists throughout therapy, suggesting that the disposition not to feel tempted even in the case of suffering from withdrawal, craving, or tested willpower (i.e., being in agony because of stopping or withdrawing from alcohol use; having the urge to try just one drink to see what happens; feeling a physical need or craving for alcohol; wanting to test willpower over drinking or experiencing an urge or impulse to take a drink when caught unprepared) may be more stable in individuals who are also more stable emotionally. The links we found between individual differences and alcohol abstinence self-efficacy also suggested that higher intellect scores may predict a lesser inclination to feel tempted to drink in social situations or those where alcohol is used to enhance positive emotionality. Intellect, equivalent to openness to experience, reflects an inherent tendency to enjoy novelty, variety, and change, and is frequently found in curious, imaginative, and creative individuals. Such greater mental capacity for reflection may therefore constitute a prerequisite for better cognitive (rather than impulsive affect-dominated) processing of cravings resulting in a greater ability to control/inhibit automatic approach tendencies aimed at indulging emergent urges. Nevertheless, given that both scores (i.e., intellect and the social/positive aspect of AASE) represent self-reported beliefs our participants hold about themselves, they may not necessarily reflect their real disposition towards the good cognitive control of the temptation to drink in social engagements, but may instead indicate how they desire to see themselves. Alternatively, such results could be construed to indicate that other factors (beyond the experienced temptation to drink) might moderate their behavior, as indeed, the reported greater capacity to cope with urges apparent in social context did not translate to either greater confidence they would refrain from drinking or higher abstinence results at follow-up predicted by either of the two measures.
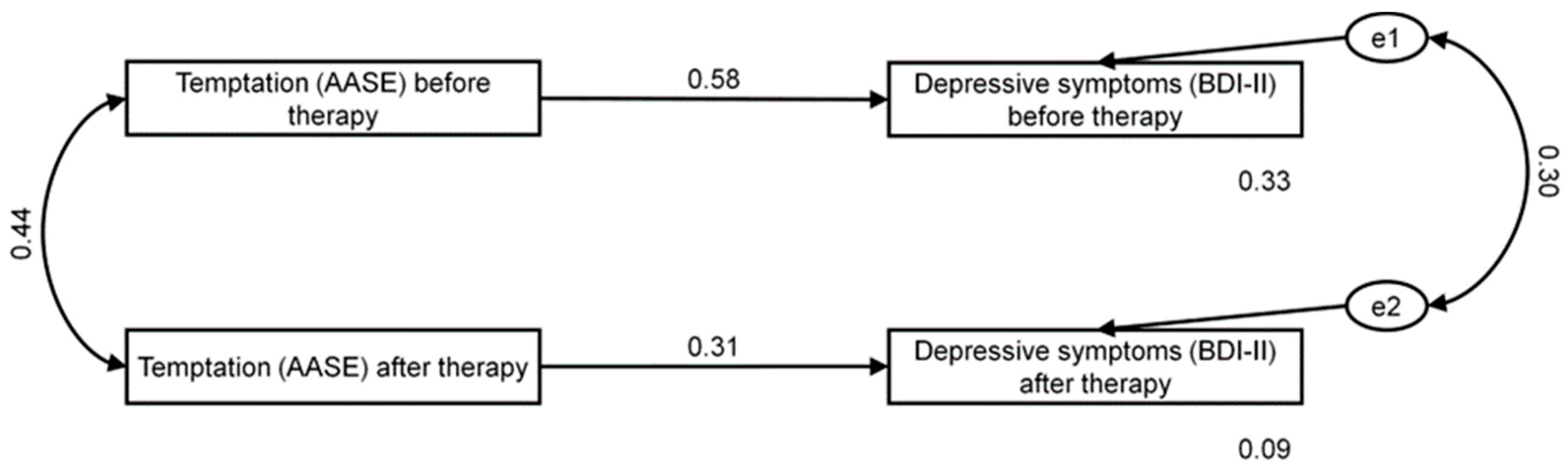
Of note, significant links emerged between alcohol abstinence self-efficacy and depression. Given the temporal stability of alcohol abstinence self-efficacy in time as suggested by our results (cf. no significant changes in AASE scores vs changes within BDI scores pre- vs post-treatment, as presented in
Table 2), we no longer considered alcohol abstinence self-efficacy and depressive symptomatology as interdependent variables, but rather assumed the former to predict the level of the latter both before and after therapy, and therefore estimated alcohol abstinence self-efficacy’s effect on depression level using the SEM framework. Such an approach resulted in demonstrating positive correlations between AASE temptation and depressive symptomatology at both investigated time points (pre- and post-therapy). More specifically, the observed associations included those between all the facets of the former (i.e., negative affect, social/positive, physical and other concerns and craving and other urges) and depressive symptom severity at baseline and endpoint, with initial correlation with social/positive no longer significant at discharge. Self-efficacy is known to play a positive role in alleviating depressive symptoms, as efforts to build and maintain a sense of control over one’s life and environment might serve to dynamically reappraise stressful circumstances and establish a certain resistance to depressive symptoms [
77,
78]. A strong sense thereof is further known to enhance personal achievements, reduce stress, and lower vulnerability to depression. In turn, alongside greater vulnerability to stress and depression [
77,
79,
80], low self-efficacy might contribute to doubting one’s own capacities, formulating low aspirations, and generally manifesting poor commitment to established goals [
81]. Separate, yet closely related to efficacy, temptation may be construed as a measure of cue strength and its capacity to precipitate alcohol use. Hence, the temptation to reach for alcohol in a particular context can be low and the efficacy to abstain quite high. This, however, may not always be the case, especially during recovery when, in spite of high temptation, an individual’s levels of efficacy to abstain could still remain high due to acquired skills, motivation and commitment [
82]. In our sample, temptation proved to correlate with the symptoms of depression throughout the study, meaning that a higher-experienced desire to drink was linked with a higher depression level. This could be interpreted in two different ways. AUD patients could construe the high-experienced temptation to use alcohol as surpassing their ability to resist and thus consider it a significant predictor of post-therapy relapse and/or poor prognostic of therapeutic success. Such an appraisal, in line with the theoretical approach proposed by DiClemente et al. [
39], suggesting an inverse relationship between temptation and self-efficacy, could result in a more pessimistic outlook on their actual ability to abstain from drinking and consequently a more depressive mood. Conversely, a more depressive mood could entail a more negative evaluation of one’s own tendencies to consider various cues and situations in terms of a temptation or a cognitive inclination towards making such types of appraisals.
As previously indicated, another interesting finding was a significant drop in depressive symptoms recorded at discharge. Managing depression symptoms and regulating emotional distress are not often prioritized in normal substance misuse treatment [
83,
84]. Rather, the conventional treatment focus is on measures to promote abstinence and decrease substance use. The available research shows that therapies aimed at reducing the negative consequences of depression symptoms and subjective distress (e.g., susceptibility to stress-induced and cue-induced craving) could help improve treatment success. Our results, indicating a significant drop in depressive symptomatology, could mean that the administered interventions or other treatment-related variables had an overall positive effect on the self-reported psychological well-being of the participants and could thus lead to improved treatment outcomes. This shows that pharmaceutical and behavioral methods aimed at regulating negative emotionality or alleviating depressive symptoms require particular consideration in conventional substance use treatment. Furthermore, a continuity of care approach for depression and depressive symptoms following the cessation of addiction treatment may be required for many AUD individuals in order to maintain attained alcohol-free status [
85]. Perhaps it could therefore be the varied post-discharge management of mental health across our sample that might potentially explain the unexpected lack of associations between the recorded levels of depression and abstinence status. In addition, in regards to our patients’ self-efficacy, the reduction in depressive symptomatology post-therapy could have a boosting effect on cognitive performance and potentially underlie a more favorable approach to self-efficacy (and temptation) appraisals, thus deeming the initially observed link between depression and social/positive facets of AASE temptation ultimately insignificant.


 ,
, 



{kind=link}
{kind=link}
{kind=link}