
Bidirectional Causality between Spreading COVID-19 and Individual Mobilisation with Consumption Motives across Prefectural Borders in Japan


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Target Regions and Period
2.3. Statistical Analysis
3. Results
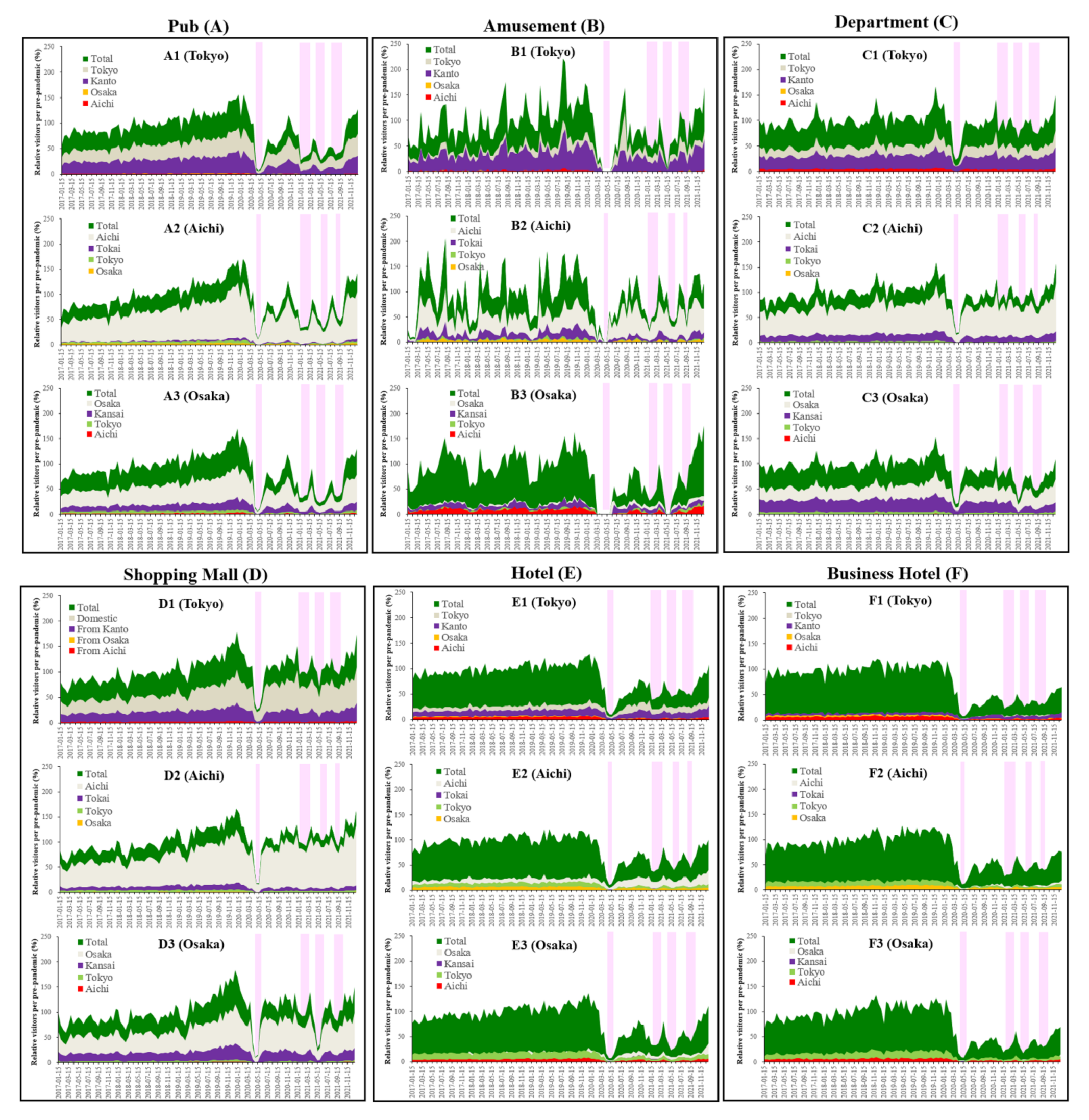
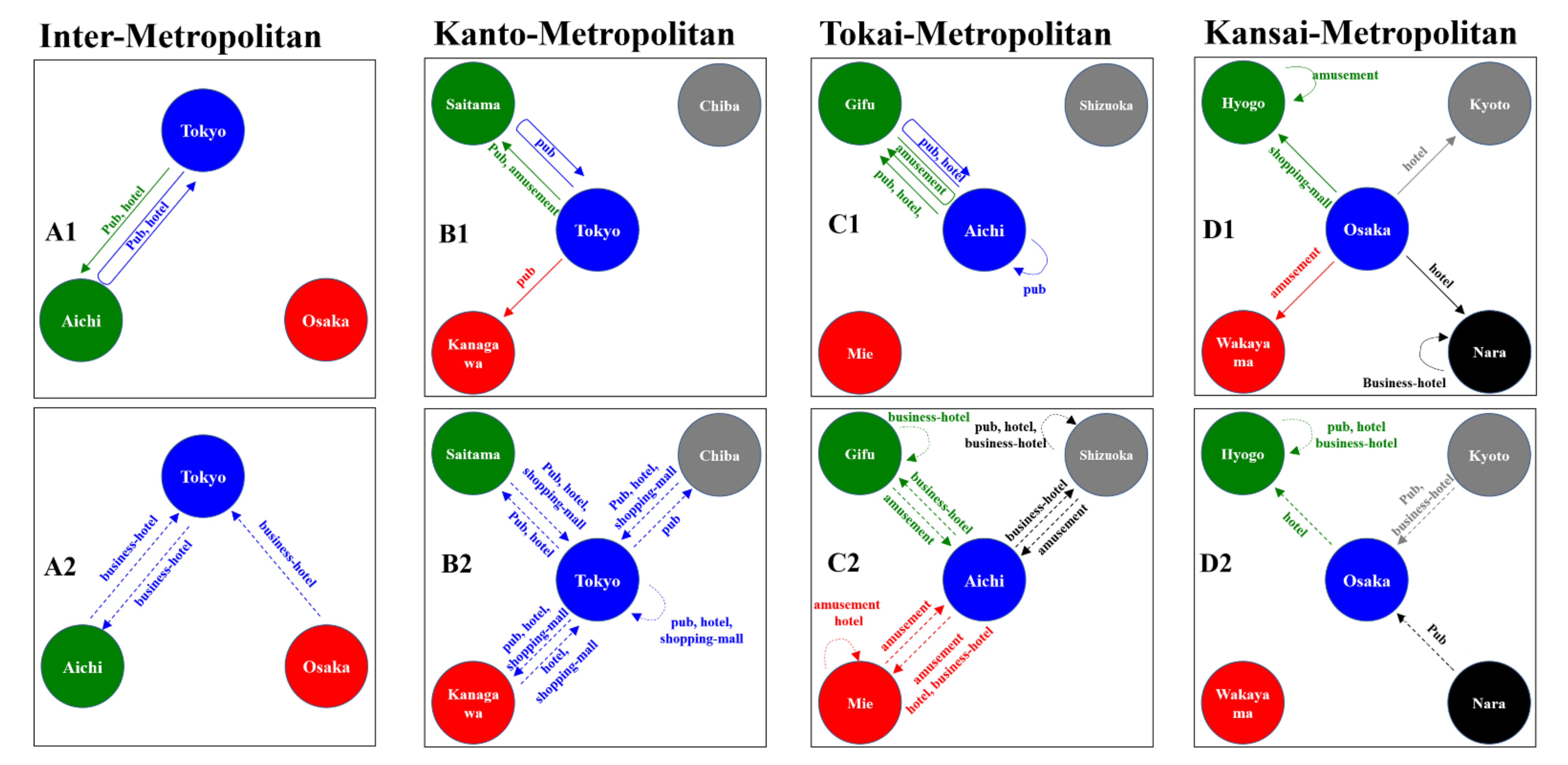
3.1. Individual Mobilisations between the Centre Prefectures in Three Metropolitan Regions
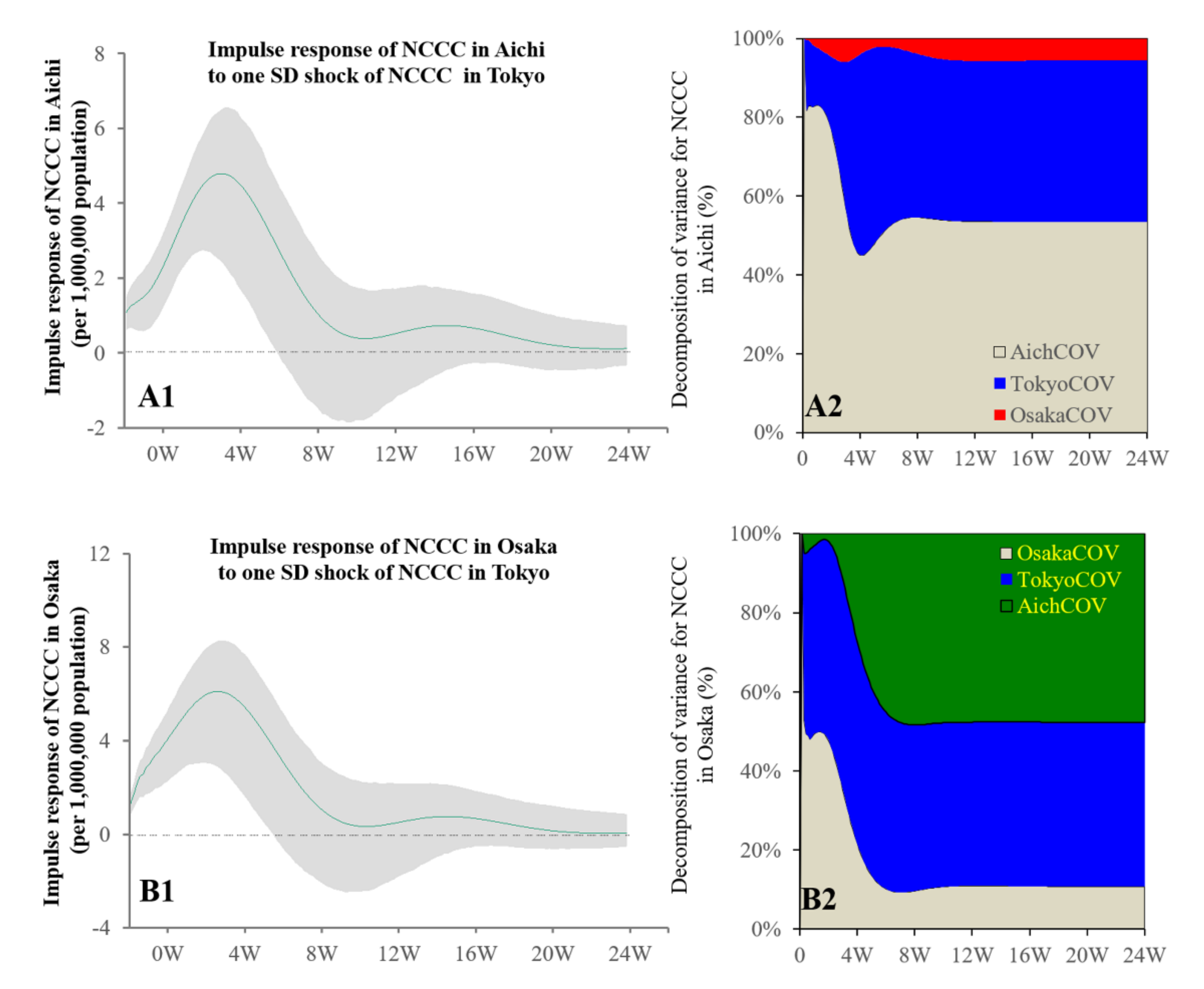
3.2. Inter-Metropolitan Regions Causalities
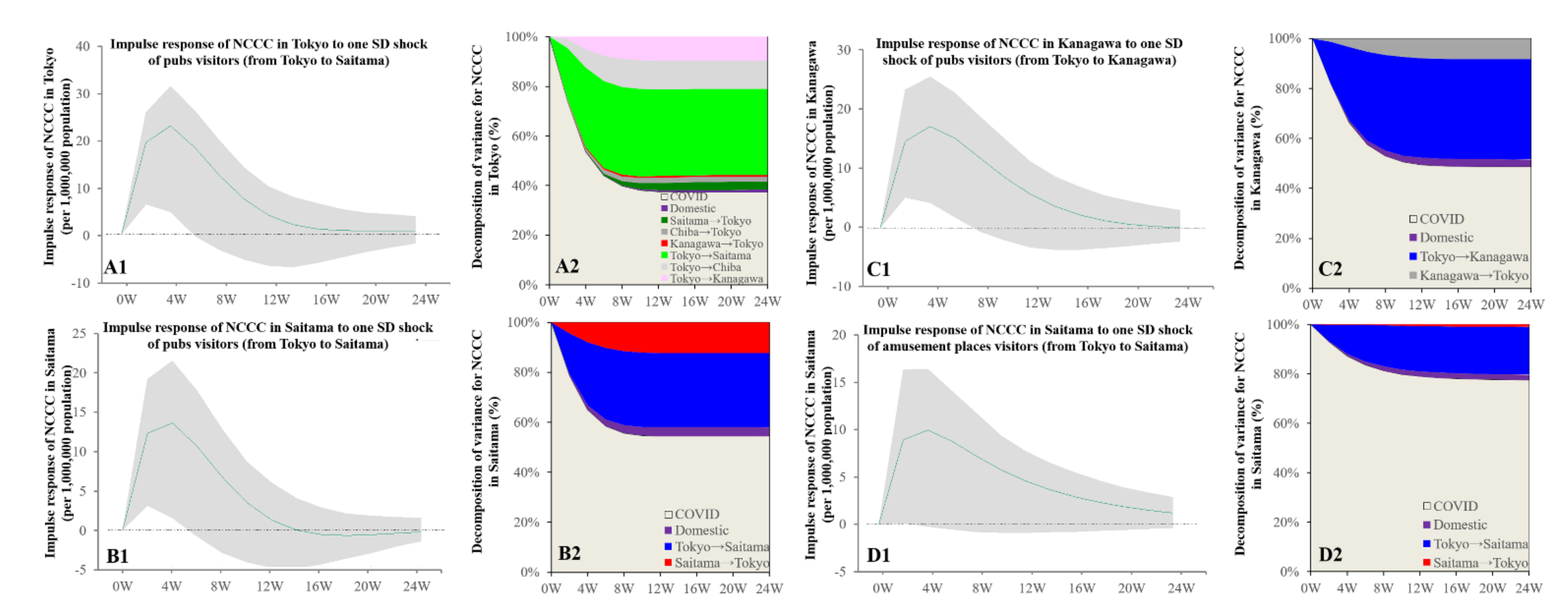
3.3. Intra-Relations in Kanto Metropolitan Region
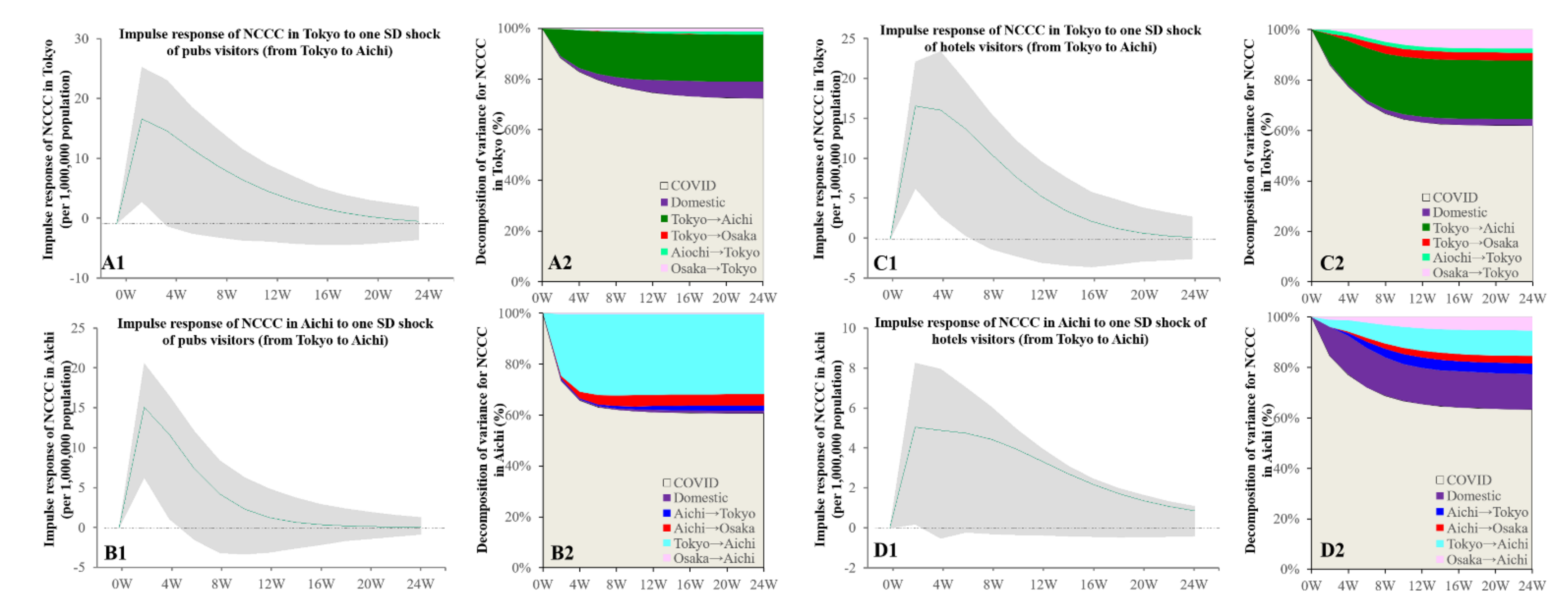
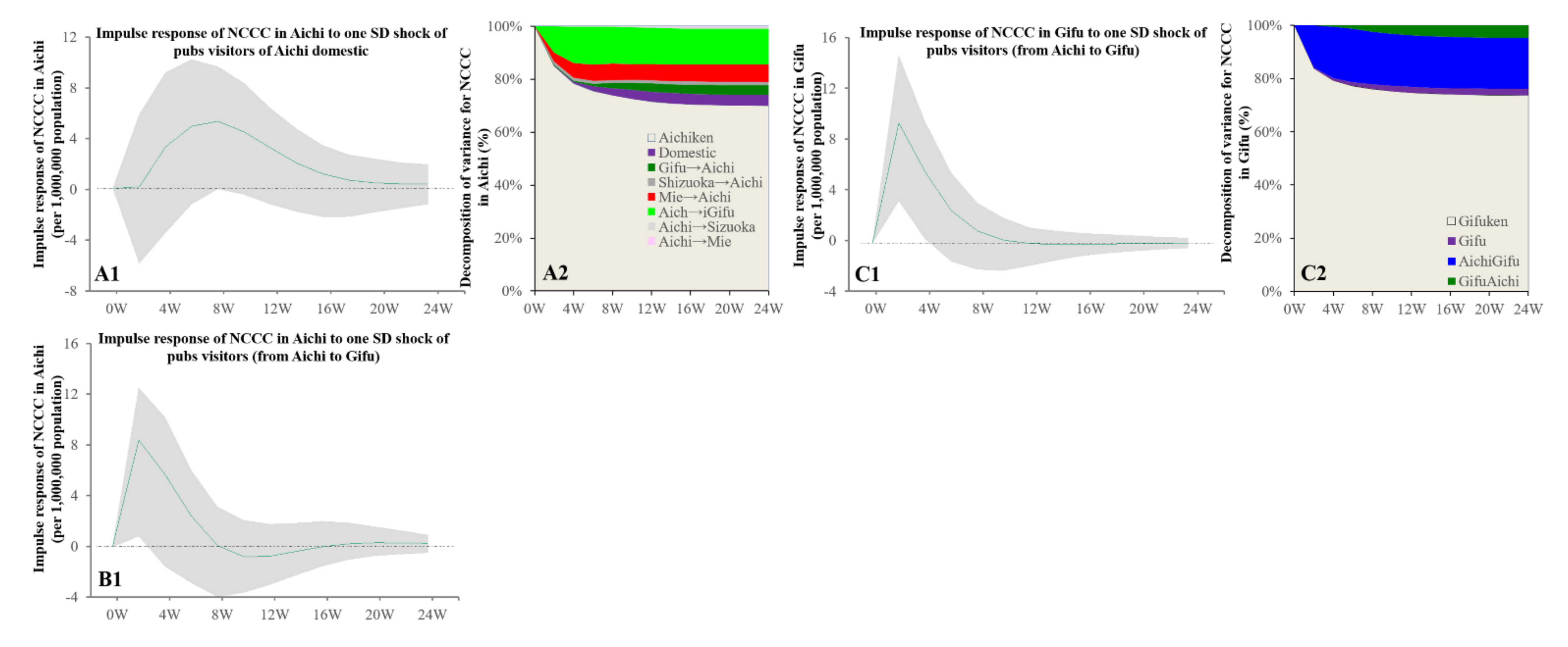
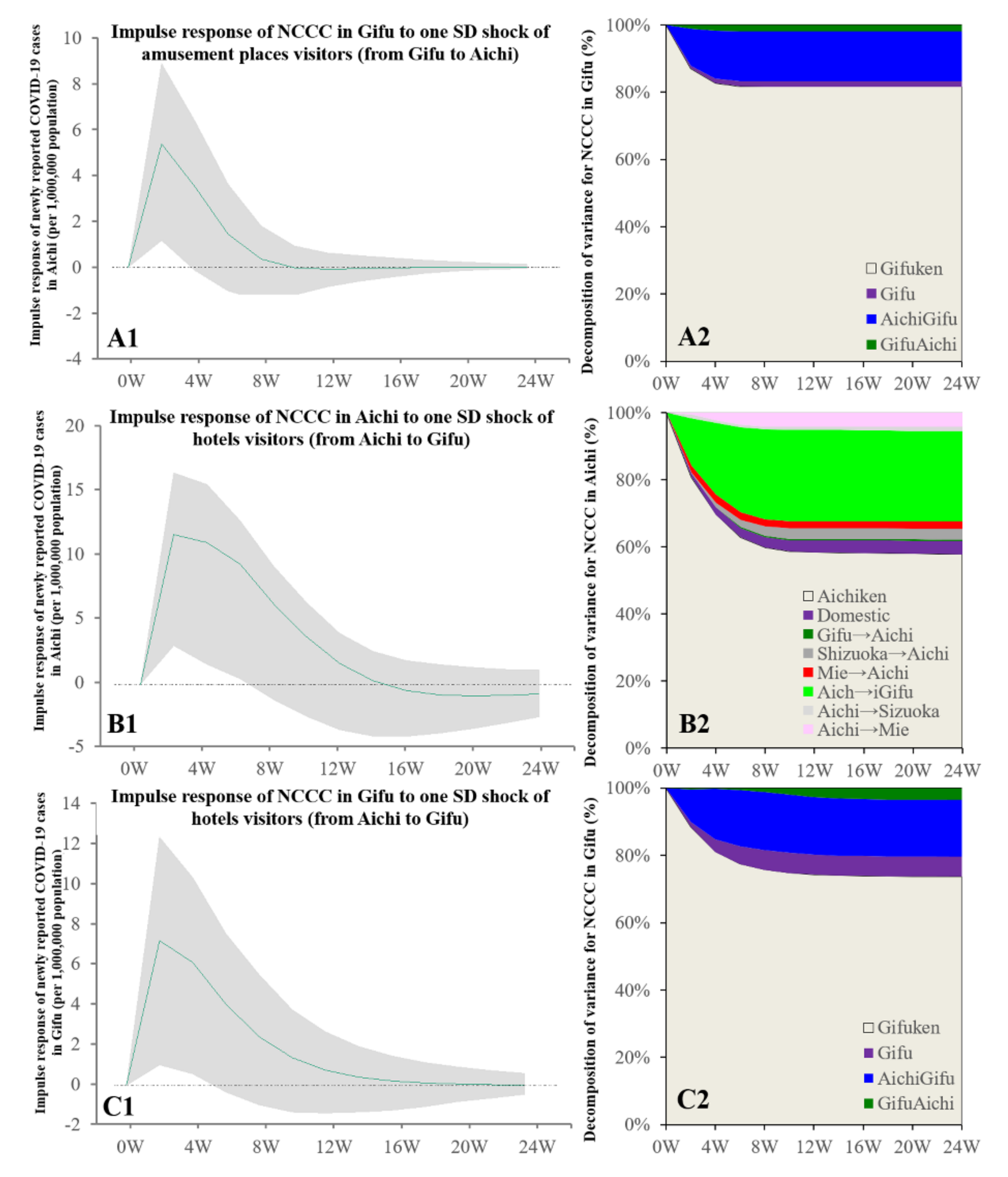
3.4. Intra-Relations in Tokai Metropolitan Region
3.5. Intra-Relations in Kansai Metropolitan Region
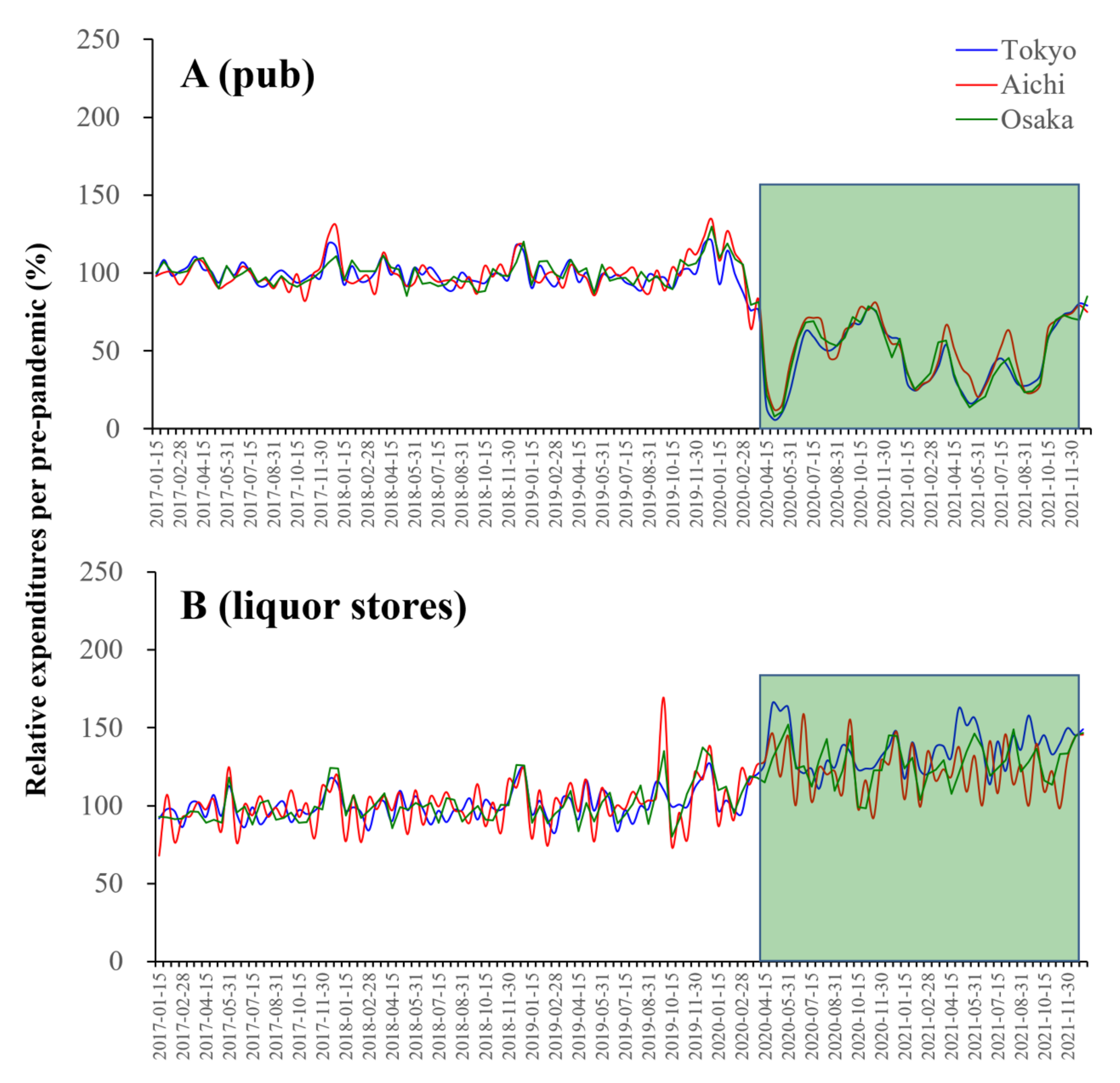
3.6. COVID-19 Spreading and Alcohol Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holmes, E.C.; Goldstein, S.A.; Rasmussen, A.L.; Robertson, D.L.; Crits-Christoph, A.; Wertheim, J.O.; Anthony, S.J.; Barclay, W.S.; Boni, M.F.; Doherty, P.C.; et al. The origins of SARS-CoV-2: A critical review. Cell 2021, 184, 4848–4856. [Google Scholar] [CrossRef]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Eurosurveillance Editorial Team. Note from the editors: World health organization declares novel coronavirus (2019-ncov) sixth public health emergency of international concern. Eurosurveillance 2020, 25, 200131e. [Google Scholar]
- WHO. Director-Generals Opening Remarks at the Media Briefing on COVID-19–11 March 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Mbala-Kingebeni, P.; Aziza, A.; Di Paola, N.; Wiley, M.R.; Makiala-Mandanda, S.; Caviness, K.; Pratt, C.B.; Ladner, J.T.; Kugelman, J.R.; Prieto, K.; et al. Medical countermeasures during the 2018 ebola virus disease outbreak in the North Kivu and Ituri provinces of the Democratic Republic of the Congo: A rapid genomic assessment. Lancet Infect. Dis. 2019, 19, 648–657. [Google Scholar] [CrossRef] [Green Version]
- Khan, K.; Arino, J.; Hu, W.; Raposo, P.; Sears, J.; Calderon, F.; Heidebrecht, C.; Macdonald, M.; Liauw, J.; Chan, A.; et al. Spread of a novel influenza a (h1n1) virus via global airline transportation. N. Engl. J. Med. 2009, 361, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Pierson, E.; Koh, P.W.; Gerardin, J.; Redbird, B.; Grusky, D.; Leskovec, J.J.N. Mobility network models of COVID-19 explain inequities and inform reopening. Nature 2021, 589, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-ncov) outbreak. J. Travel Med. 2020, 27, taaa020. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; Garcia-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in asia pacific and europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- Gwee, S.X.W.; Chua, P.E.Y.; Wang, M.X.; Pang, J. Impact of travel ban implementation on COVID-19 spread in singapore, taiwan, hong kong and south korea during the early phase of the pandemic: A comparative study. BMC Infect. Dis. 2021, 21, 799. [Google Scholar] [CrossRef] [PubMed]
- Ng, O.T.; Marimuthu, K.; Koh, V.; Pang, J.; Linn, K.Z.; Sun, J.; De Wang, L.; Chia, W.N.; Tiu, C.; Chan, M.; et al. SARS-CoV-2 seroprevalence and transmission risk factors among high-risk close contacts: A retrospective cohort study. Lancet Infect. Dis. 2021, 21, 333–343. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Pierri, F.; Cinelli, M.; Flori, A.; Galeazzi, A.; Porcelli, F.; Schmidt, A.L.; Valensise, C.M.; Scala, A.; Quattrociocchi, W.; et al. Economic and social consequences of human mobility restrictions under COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 15530–15535. [Google Scholar] [CrossRef]
- Campion, J.; Javed, A.; Lund, C.; Sartorius, N.; Saxena, S.; Marmot, M.; Allan, J.; Udomratn, P. Public mental health: Required actions to address implementation failure in the context of COVID-19. Lancet Psychiatry 2022, 9, 169–182. [Google Scholar] [CrossRef]
- Lu, J.; Lin, A.; Jiang, C.; Zhang, A.; Yang, Z. Influence of transportation network on transmission heterogeneity of COVID-19 in China. Transp. Res. Part C Emerg. Technol. 2021, 129, 103231. [Google Scholar] [CrossRef]
- Lin, C.-H.; Wen, T.-H. Using geographically weighted regression (gwr) to explore spatial varying relationships of immature mosquitoes and human densities with the incidence of dengue. Int. J. Environ. Res. Public Health 2011, 8, 2798–2815. [Google Scholar] [CrossRef] [Green Version]
- Gong, P.; Liang, S.; Carlton, E.J.; Jiang, Q.; Wu, J.; Wang, L.; Remais, J.V. Urbanisation and health in China. Lancet 2012, 379, 843–852. [Google Scholar] [CrossRef]
- Kenneson, A.; Beltran-Ayala, E.; Borbor-Cordova, M.J.; Polhemus, M.E.; Ryan, S.J.; Endy, T.P.; Stewart-Ibarra, A.M. Social-ecological factors and preventive actions decrease the risk of dengue infection at the household-level: Results from a prospective dengue surveillance study in Machala, Ecuador. PLoS Negl. Trop. Dis. 2017, 11, e0006150. [Google Scholar] [CrossRef]
- Nakanishi, M.; Shibasaki, R.; Yamasaki, S.; Miyazawa, S.; Usami, S.; Nishiura, H.; Nishida, A. On-site dining in Tokyo during the COVID-19 pandemic: Time series analysis using mobile phone location data. JMIR Mhealth Uhealth 2021, 9, e27342. [Google Scholar] [CrossRef]
- Yamauchi, T.; Takeuchi, S.; Uchida, M.; Saito, M.; Kokaze, A. The association between the dynamics of COVID-19, related measures, and daytime population in Tokyo. Sci. Rep. 2022, 12, 3063. [Google Scholar] [CrossRef]
- Yabe, T.; Tsubouchi, K.; Fujiwara, N.; Wada, T.; Sekimoto, Y.; Ukkusuri, S.V. Non-compulsory measures sufficiently reduced human mobility in Tokyo during the COVID-19 epidemic. Sci. Rep. 2020, 10, 18053. [Google Scholar] [CrossRef]
- Tomura, H. Associations between components of household expenditures and the rate of change in the number of new confirmed cases of COVID-19 in Japan: Time-series analysis. PLoS ONE 2022, 17, e0266963. [Google Scholar] [CrossRef] [PubMed]
- Shiroyama, T.; Fukuyama, K.; Okada, M. Effects of financial expenditure of prefectures/municipalities on regional suicide mortality in Japan. Int. J. Environ. Res. Public Health 2021, 18, 8639. [Google Scholar] [CrossRef]
- Hasegawa, T.; Fukuyama, K.; Okada, M. Relationships between expenditure of regional governments and suicide mortalities caused by six major motives in Japan. Int. J. Environ. Res. Public Health 2022, 19, 84. [Google Scholar] [CrossRef]
- Kashimoto, K.; Okada, M. Analysing the impacts of financial expenditure of prefectures on methods of suicide completion in Japan. Psychiatry Int. 2022, 3, 1–16. [Google Scholar] [CrossRef]
- NIID (National Institute of Infectious Diseases). Report Week Correspondence Table. Available online: https://www.niid.go.jp/niid/ja/calendar.html (accessed on 1 July 2022).
- Idogawa, M.; Tange, S.; Nakase, H.; Tokino, T. Interactive web-based graphs of coronavirus disease 2019 cases and deaths per population by country. Clin. Infect. Dis. 2020, 71, 902–903. [Google Scholar] [CrossRef]
- SBMIAC (Statistics Bureau of the Ministry of Internal Affairs and Communications). Surveys of Population, Population Change and the Number of Households Based on the Basic Resident Registration. Available online: https://www.e-stat.go.jp/en/statistics/00200241 (accessed on 1 July 2022).
- Nowcast, Inc. JCB Consumption Now. Available online: https://www.jcbconsumptionnow.com/en (accessed on 1 February 2022).
- JCB Ltd. About JCB. Available online: https://www.global.jcb/en/ (accessed on 1 February 2022).
- SBMIAC (Statistics Bureau of the Ministry of Internal Affairs and Communications). Family Income and Expenditure Survey. Available online: https://www.e-stat.go.jp/en/statistics/00200561 (accessed on 1 February 2022).
- Cabinet Office. Vital Signs of Economy Regional Economy and Society Analyzing System (V-Resas). Available online: https://v-resas.go.jp/about (accessed on 1 February 2022).
- Cabinet Office. Regional Economy and Society Analyzing System (Resas). Available online: https://resas.go.jp/#/13/13101 (accessed on 1 February 2022).
- Matsumoto, R.; Motomura, E.; Fukuyama, K.; Shiroyama, T.; Okada, M. Determining what changed japanese suicide mortality in 2020 using governmental database. J. Clin. Med. 2021, 10, 5199. [Google Scholar] [CrossRef]
- Okada, M.; Matsumoto, R.; Motomura, E.; Shiroyama, T.; Murata, M. Exploring characteristics of increased suicide during the COVID-19 pandemic in Japan using provisional governmental data. Lancet Reg. Health West. Pac. 2022, 24, 100481. [Google Scholar] [CrossRef]
- Nishiura, H.; Linton, N.M.; Akhmetzhanov, A.R. Serial interval of novel coronavirus (COVID-19) infections. Int. J. Infect. Dis. 2020, 93, 284–286. [Google Scholar] [CrossRef]
- Du, Z.; Liu, C.; Wang, L.; Bai, Y.; Lau, E.H.Y.; Wu, P.; Cowling, B.J. Shorter serial intervals and incubation periods in SARS-CoV-2 variants than the SARS-CoV-2 ancestral strain. J. Travel Med. 2022, taac052. [Google Scholar] [CrossRef]
- Clay, J.M.; Parker, M.O. Alcohol use and misuse during the COVID-19 pandemic: A potential public health crisis? Lancet Public Health 2020, 5, e259. [Google Scholar] [CrossRef]
- Einberger, C.; Graupensperger, S.; Lee, C.M. Young adults’ physical distancing behaviors during the initial months of the COVID-19 pandemic: Adherence to guidelines and associations with alcohol use behavior. Emerg. Adulthood 2021, 9, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Solopov, P.A.; Luciano Colunga Biancatelli, R.M.; Catravas, J.D. Alcohol increases lung ace2 expression and exacerbates SARS-CoV-2 spike protein subunit 1-induced acute lung injury in k18-hace2 transgenic mice. Am. J. Pathol. 2022, 192, 990–1000. [Google Scholar] [CrossRef]
- Kilian, C.; O’Donnell, A.; Potapova, N.; Lopez-Pelayo, H.; Schulte, B.; Miquel, L.; Paniello Castillo, B.; Schmidt, C.S.; Gual, A.; Rehm, J.; et al. Changes in alcohol use during the COVID-19 pandemic in Europe: A meta-analysis of observational studies. Drug Alcohol Rev. 2022, 41, 918–931. [Google Scholar] [CrossRef] [PubMed]
- Acuff, S.F.; Strickland, J.C.; Tucker, J.A.; Murphy, J.G. Changes in alcohol use during COVID-19 and associations with contextual and individual difference variables: A systematic review and meta-analysis. Psychol. Addict. Behav. 2022, 36, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Rolland, B.; Haesebaert, F.; Zante, E.; Benyamina, A.; Haesebaert, J.; Franck, N. Global changes and factors of increase in caloric/salty food intake, screen use, and substance use during the early COVID-19 containment phase in the general population in France: Survey study. JMIR Public Health Surveill. 2020, 6, e19630. [Google Scholar] [CrossRef] [PubMed]
- Szajnoga, D.; Klimek-Tulwin, M.; Piekut, A. COVID-19 lockdown leads to changes in alcohol consumption patterns. Results from the polish national survey. J. Addict. Dis. 2021, 39, 215–225. [Google Scholar] [CrossRef]
- NIID (National Institute of Infectious Diseases). Infectious Agents Surveillance Report (IASR). Available online: https://www.niid.go.jp/niid/ja/2019-ncov/2502-idsc/iasr-in/10524–497c01.html (accessed on 1 February 2022).










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawano, Y.; Matsumoto, R.; Motomura, E.; Shiroyama, T.; Okada, M. Bidirectional Causality between Spreading COVID-19 and Individual Mobilisation with Consumption Motives across Prefectural Borders in Japan. Int. J. Environ. Res. Public Health 2022, 19, 9070. https://doi.org/10.3390/ijerph19159070
Kawano Y, Matsumoto R, Motomura E, Shiroyama T, Okada M. Bidirectional Causality between Spreading COVID-19 and Individual Mobilisation with Consumption Motives across Prefectural Borders in Japan. International Journal of Environmental Research and Public Health. 2022; 19(15):9070. https://doi.org/10.3390/ijerph19159070
Chicago/Turabian StyleKawano, Yasuhiro, Ryusuke Matsumoto, Eishi Motomura, Takashi Shiroyama, and Motohiro Okada. 2022. "Bidirectional Causality between Spreading COVID-19 and Individual Mobilisation with Consumption Motives across Prefectural Borders in Japan" International Journal of Environmental Research and Public Health 19, no. 15: 9070. https://doi.org/10.3390/ijerph19159070
APA StyleKawano, Y., Matsumoto, R., Motomura, E., Shiroyama, T., & Okada, M. (2022). Bidirectional Causality between Spreading COVID-19 and Individual Mobilisation with Consumption Motives across Prefectural Borders in Japan. International Journal of Environmental Research and Public Health, 19(15), 9070. https://doi.org/10.3390/ijerph19159070