
Characterization of Communes with Quality Accredited Primary Healthcare Centers in Chile

 ,
,  ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
- Classify accredited CESFAMs according to socioeconomic, demographic, and municipal management variables;
- Identify interdependence between the communes that have accredited CESFAMs, according to the variables under study;
- Analyze the groups of communes that have accredited CESFAMs by applying hierarchical methods.
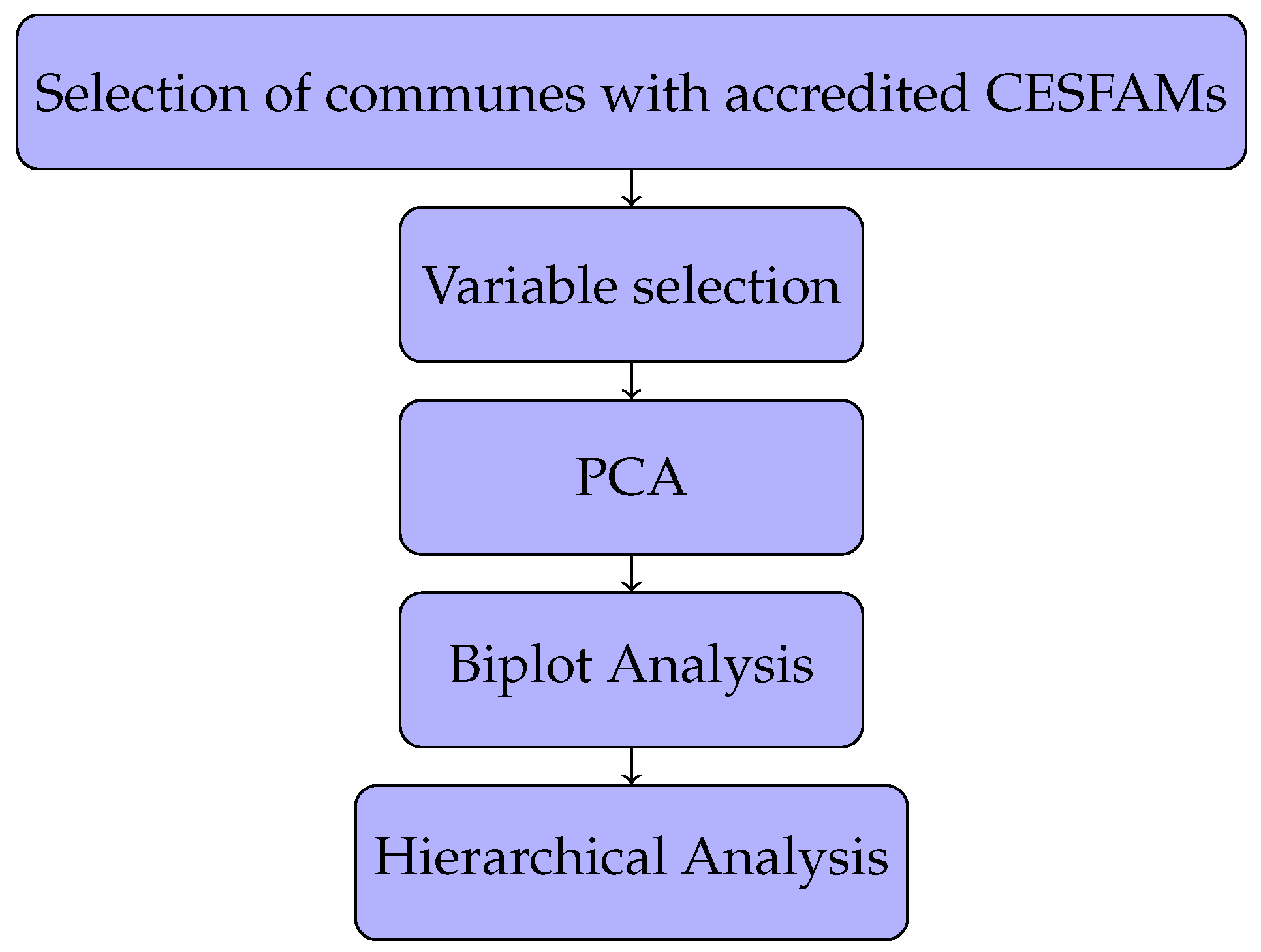
2. Materials and Methods
3. Results
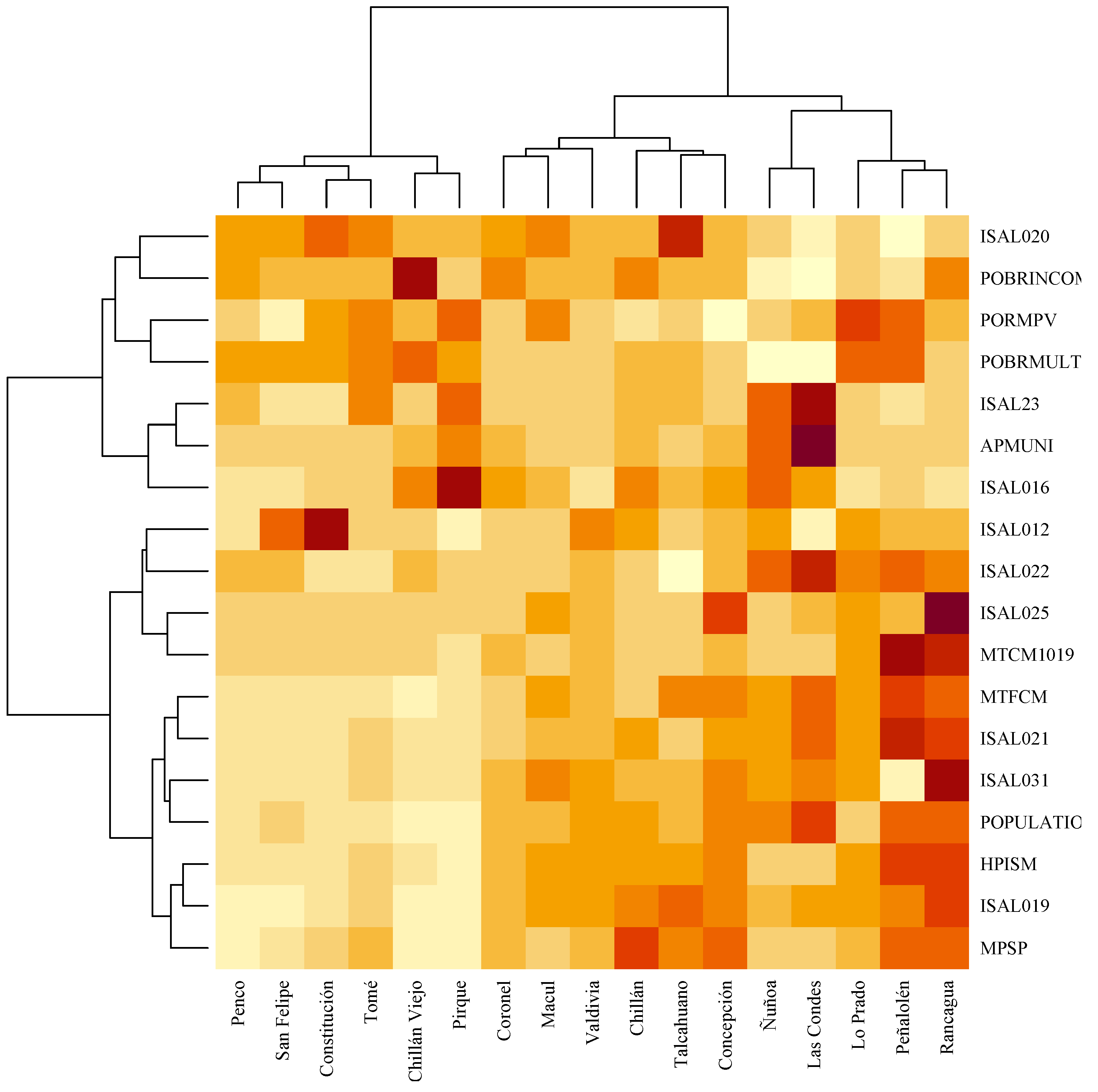
- 1.
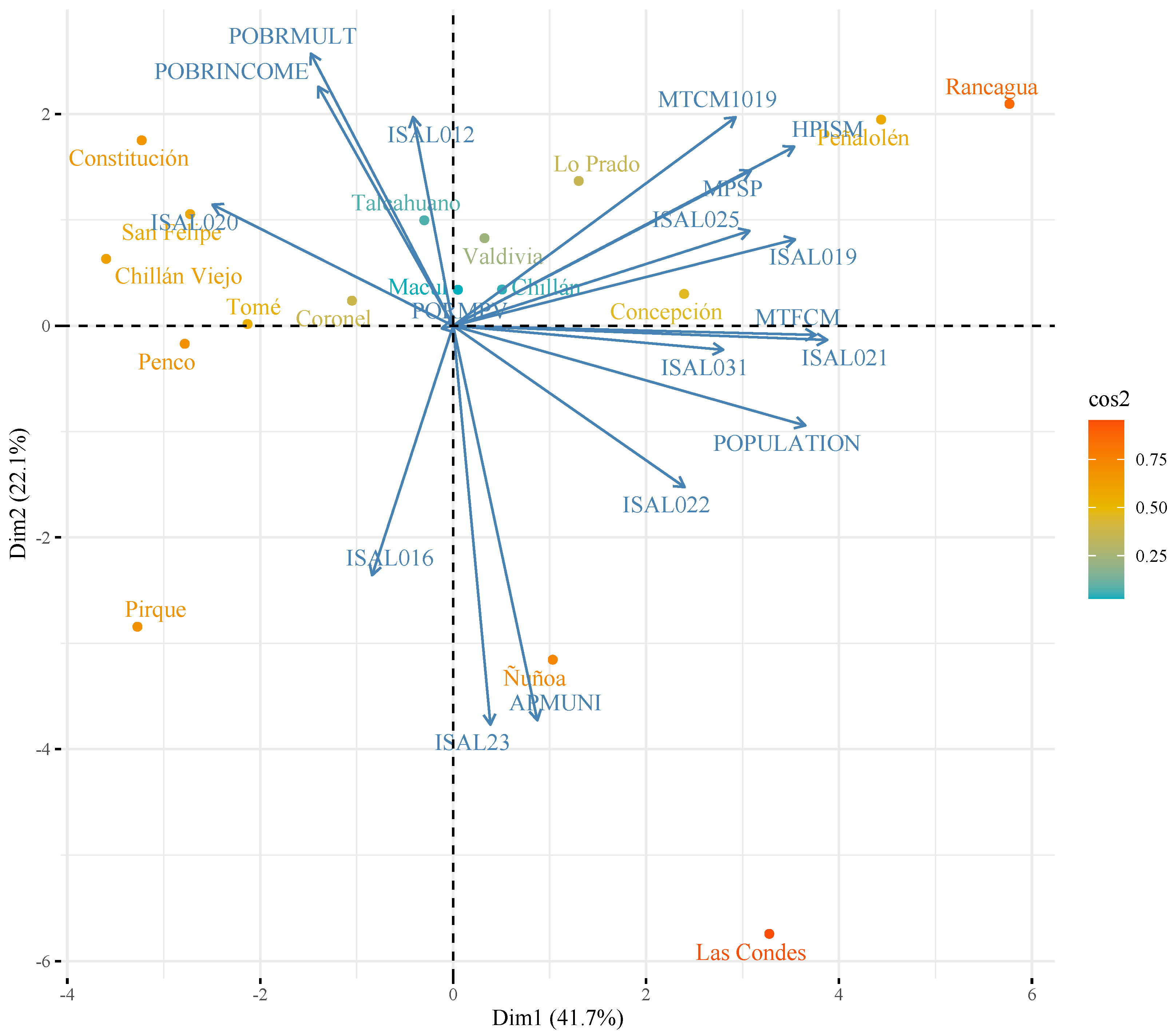
- Penco, San Felipe, Constitución, Tomé, Chillan Viejo and Pirque: this agrees with previous analysis as the communes with the lowest population concentration;
- 2.
- Coronel, Macul, Valdivia, Chillan, Talcahuano and Concepción: these are communes with values close to the average of the variables;
- 3.
- Ñuñoa, Las Condes, Lo Prado, Peñalolen y Rancagua: these are grouped together because they are communes with high concentration of population, while Las Condes and Ñuñoa differ as communes with low levels of poverty, a low proportion of registered population validated in municipal health systems, and high levels of financing of health systems.
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CECOSF | Community Family Healthcare Center |
| CENABAST | National Supply Center |
| CESFAM | Family Healthcare Center |
| DEIS | Department of Health Information Statistics |
| FONASA | National Health Fund |
| HR | Human Resources |
| ISAPRE | Social Security Institutions |
| ISP | Public Health Institute |
| MAIS | Comprehensive Family and Community Health Model |
| MINSAL | Ministry of Health |
| OECD | Organization for Economic Cooperation and Development |
| PCA | Principal Components Analysis |
| PHC | Primary Healthcare Centers |
| SNSS | National Services System Health |
| WHO | World Health Organization |
References
- World Health Organization. Quality in Primary Health Care; On Primary Health Care, World Health Organization: Geneva, Switzerland, 2018; p. 28. [Google Scholar]
- Vergara-Iturriaga, M.; Martínez-Gutiérrez, M.S. Financiamiento del sistema de salud chileno. Salud Pública Méx. 2006, 48, 512–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soto, L.; Soto, J.; Riquelme, F. Hacia un modelo de atención en salud para el siglo XXI: Breve historia del modelo de atención integrada en Chile. Rev. Médica Clín. Condes 2021, 32, 373–378. [Google Scholar] [CrossRef]
- DEIS Ministerio de Salud. Departamento de Estadisticas e Información de Salud. 2022. Available online: http://www.deis.cl/ (accessed on 31 May 2022).
- Donabedian, A. The Lichfield lectura. Garantía de Calidad en la Atención de Salud: El papel del consumidor. Rev. Calid. Asist. 2001, 16, S102–S106. [Google Scholar]
- Donabedian, A. Evaluating the Quality of Medical Care. Milbank Q. 2005, 83, 691–729. [Google Scholar] [CrossRef] [Green Version]
- Soranz, D.; Coelho Pisco, L.A. Reforma dos Cuidados Primários em Saúde na cidade de Lisboa e Rio de Janeiro: Contexto, estratégias, resultados, aprendizagem, desafios. Cienc. E Saude Coletiva 2017, 22, 679–686. [Google Scholar] [CrossRef] [Green Version]
- Tabrizi, J.S.; Gharibi, F. Primary healthcare accreditation standards: A systematic review. Int. J. Health Care Qual. Assur. 2019, 32, 310–320. [Google Scholar] [CrossRef]
- Díaz Herrera, C.; Galán Torres, G. Modernization of family health centers in Chile. Tension between management, quality and structural conditions. Aten. Primaria 2019, 51, 390–391. [Google Scholar] [CrossRef]
- Ghareeb, A.; Said, H.; El Zoghbi, M. Examining the impact of accreditation on a primary healthcare organization in Qatar. BMC Med. Educ. 2018, 18, 216. [Google Scholar] [CrossRef]
- Due, T.D.; Thorsen, T.; Kousgaard, M.B. Understanding accreditation standards in general practice—A qualitative study. BMC Fam. Pract. 2019, 20, 23. [Google Scholar] [CrossRef] [Green Version]
- Mahmoud, A.S.; Alkhenizan, A.; Shafiq, M.; Alsoghayer, S. The impact of the implementation of a clinical decision support system on the quality of healthcare services in a primary care setting. J. Fam. Med. Prim. Care 2020, 9, 6078–6084. [Google Scholar] [CrossRef]
- Syengo, M.; Suchman, L. Private Providers’ Experiences Implementing a Package of Interventions to Improve Quality of Care in Kenya: Findings From a Qualitative Evaluation. Glob. Health Sci. Pract. 2020, 8, 478–487. [Google Scholar] [CrossRef]
- Dominguez-Cancino, K.A.; Palmieri, P.A.; Martinez-Gutierrez, M.S. National Health Policy Reform for Primary Care in Chile: A Qualitative Analysis of the Health Program Documents. J. Prim. Care Community Health 2020, 11, 2150132720924884. [Google Scholar] [CrossRef]
- Ministerio de Salud. Ley 19937: Modifica el D.L. Nº 2.763, de 1979, con la finalidad de establecer una nueva concepción de la autoridad sanitaria, distintas modalidades de gestión y fortalecer la participación ciudadana. Biblioteca del Congreso Nacional de Chile/BCN. 2004, p. 64. Available online: http://bcn.cl/2b1q1 (accessed on 31 May 2022).
- Ministerio de Salud. Decreto 3; Aprueba garantías explícitas en salud del régimen general de garantías en salud. Biblioteca del Congreso Nacional de Chile/BCN. 2016, p. 110. Available online: http://bcn.cl/2ewta (accessed on 31 May 2022).
- Ministerio de Salud; Subsecretaría de Redes Asistenciales. Decreto 15: Reglamento del sistema de acreditación para los prestadores institucionales de salud. Biblioteca del Congreso Nacional de Chile/BCN. 2007, p. 18. Available online: https://www.bcn.cl/leychile/navegar?idNorma=262240 (accessed on 31 May 2022).
- Ministerio de Salud. Reglamento Sistema de Acreditación Para los Prestadores Institucionales de Salud: Decreto Supremo N° 15, de 2007; del Ministerio de Salud: Buenos Aires, Argentina, 2007. [Google Scholar]
- Superintendencia de Salud. Gobierno de Chile. Manual del Estándar General de Acreditación para Prestadores Institucionales de Atención Abierta; Technical Report; Superintendencia de Salud, Intendencia de Prestadores: Santiago, Chile, 2009. [Google Scholar]
- Superintendencia de Salud, G.d.C. Trámites y Servicios: Registro de Prestadores Acreditados. 2022. Available online: http://www.supersalud.gob.cl/servicios/669/w3-article-6193.html (accessed on 20 May 2022).
- Subsecretaría de Desarrollo Regional y Administrativo. Sistema Nacional de Información Municipal: Datos Municipales. 2022. Available online: http://datos.sinim.gov.cl/datos_municipales.php (accessed on 20 May 2022).
- Superintendencia de Salud. Registro de Prestadores Acreditados Por N° de Registro. 2022. Available online: https://www.supersalud.gob.cl/acreditacion/673/w3-propertyvalue-4710.html (accessed on 6 June 2022).
- Ministerio de Desarrollo Social y Familia. CASEN 2017: Estimaciones de la Tasa de Pobreza por Ingresos y Multidimensional a Nivel Comunal, año 2017: Aplicación de Metodología de Estimación para áreas Pequeñas (SAE); Technical Report; Ministerio de Desarrollo Social y Familia: Santiago, Chile, 2017. [Google Scholar]
- INE. Síntesis de Resultados Censo 2017; Technical Report; Instituto Nacional de Estadísticas: Santiago, Chile, 2018. [Google Scholar]
- Bruni, V.; Cardinali, M.L.; Vitulano, D. A Short Review on Minimum Description Length: An Application to Dimension Reduction in PCA. Entropy 2022, 24, 269. [Google Scholar] [CrossRef]
- Güngör, H.; Çıkılı, Y.; Dumlupınar, Z. Screening of oat varieties and landraces at early vegetative stage under salt stress conditions: Morpho-physiological and PCA biplot analysis. Cereal Res. Commun. 2021, 49, 587–597. [Google Scholar] [CrossRef]
- Zhang, H.; Srinivasan, R. A Biplot-Based PCA Approach to Study the Relations between Indoor and Outdoor Air Pollutants Using Case Study Buildings. Buildings 2021, 11, 218. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Kassambara, A.; Mundt, F. Factoextra: Extract and Visualize the Results of Multivariate Data Analyses; Version 1.0.7; Alboukadel Kassambara and Fabian Mundt: Los Ángeles, CA, USA, 2020. [Google Scholar]
- Organización Mundial de la Salud. Atención Primaria de Salud: Proyecto de Marco Operacional Atención Primaria de Salud: 470 Transformar la Visión en Acción; Organización Mundial de la Salud: Geneva, Switzerland, 2019. [Google Scholar]
- Troncoso, J.; González, C.; Mena, F.; Valencia, A.; Cuevas, P.; Rubio, J.P. «Falta tiempo»: Experiencias de médicos gestores de la demanda en la atención primaria de salud chilena. Atención Primaria 2021, 53, 102159. [Google Scholar] [CrossRef]
- Almeida, G.; Artaza, O.; Donoso, N.; Fábrega, R. La atención primaria de salud en la Región de las Américas a 40 años de la Declaración de Alma-Ata. Rev. Panam. Salud Publica 2018, 42, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Centro de Políticas Públicas UC. Fortalecimiento de la atención primaria de salud: Propuestas para mejorar el sistema sanitario chileno. Pontif. Univ. Catol. Chile 2014, 9, 1–19. [Google Scholar]
- Parada-Lezcano, M.; Moraga-Cortés, F. Crise do seguro saúde no chile: Doença crônica socialmente transmissível. Tempus Actas Saúde Coletiva 2019, 13, 177–203. [Google Scholar] [CrossRef]
- Banks, J.; Marmot, M.; Oldfield, Z.; Smith, J.P. Disease and Disadvantage in the United States and in England. JAMA 2006, 295, 2037–2045. [Google Scholar] [CrossRef]
- Butler, D.C.; Petterson, S.; Phillips, R.L.; Bazemore, A.W. Measures of Social Deprivation That Predict Health Care Access and Need within a Rational Area of Primary Care Service Delivery. Health Serv. Res. 2013, 48, 539–559. [Google Scholar] [CrossRef] [Green Version]
- Quiñones, B.; de Orúe-Ríos, P.; Contreras, J. Visiones de los actores claves sobre el proceso de acreditación de los Centros de Salud Familiar de la comuna de Concepción 2016. Rev. Chil. Salud Pública 2022, 25, 153–162. [Google Scholar] [CrossRef]
- González, E. Informe: Cumplimiento de Normas de Seguridad del Paciente y Calidad de la Atención, Respecto de Resultados de sus Indicadores, en Red de Prestadores Públicos de Atención Cerrada: Análisis años 2018-2019-2020; Technical Report; Departamento Calidad y Seguridad de la Atención División de Gestión de la Red Asistencial (DIGERA), Subsecretaría de Redes Asistenciales, Ministerio de Salud: Santiago, Chile, 2021. [Google Scholar]
- Nair, S.; Chen, J. Improving Quality of Care in Federally Qualified Health Centers Through Ambulatory Care Accreditation. J. Healthc. Qual. 2018, 40, 301–309. [Google Scholar] [CrossRef]
- Tudor Hart, J. The inverse care law. Lancet 1971, 297, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Schoen, C.; Osborn, R.; Doty, M.M.; Squires, D.; Peugh, J.; Applebaum, S. A Survey Of Primary Care Physicians In Eleven Countries, 2009: Perspectives On Care, Costs, And Experiences. Health Aff. 2009, 28, 1171–1183. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Huidobro, D.; Barros, X.; Quiroz, A.; Barria, M.; Soto, G.; Vargas, I. Modelo de atencion integral en salud familiar y comunitaria en la atencion primaria chilena. Rev. Panam. Salud Publica 2018, 42, e160. [Google Scholar] [CrossRef] [Green Version]
- Castro, R.E.; Palacios, A.; Arenas, A.; Martorell, B. Modelo cuantitativo para mejorar el financiamiento de la atención primaria en Chile. Rev. Panam. Salud Publica 2017, 41, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Riquelme Briceño, C.; Haase Delgado, J.; Lavanderos Bunout, S.; Morales Martínez, A. Desigualdad en recursos financieros de la Atención Primaria de Salud Municipal en Chile, 2001–2013. Rev. Médica Chile 2017, 145, 723–733. [Google Scholar] [CrossRef] [Green Version]
- Subsecretaría de Redes Asistenciales División Atención Primaria. Eje Gestión de Recursos Financieros en Atención Primaria; Technical Report; Ministerio de Salud: Santiago, Chile, 2015. [Google Scholar]
- Limato, R.; Tumbelaka, P.; Ahmed, R.; Nasir, S.; Syafruddin, D.; Ormel, H.; Kumar, M.B.; Taegtmeyer, M.; Kok, M. What factors do make quality improvement work in primary health care? Experiences of maternal health quality improvement teams in three Puskesmas in Indonesia. PLoS ONE 2019, 14, e0226804. [Google Scholar] [CrossRef]
- Rodríguez García, L.A.; Lozano Medina, S.R. Estudio de la satisfacción de los usuarios luego de la adopción del Sistema Único de Acreditación en Salud, en el Centro Policlínico del Olaya. SIGNOS Investig. Sist. Gestión 2012, 4, 61–83. [Google Scholar] [CrossRef]
- Alvial, X.; Rojas, A.; Carrasco, R.; Duran, C.; Fernandez-Campusano, C. Overuse of Health Care in the Emergency Services in Chile. Int. J. Environ. Res. Public Health 2021, 18, 3082. [Google Scholar] [CrossRef] [PubMed]
- Pesse-Sorensen, K.; Fuentes-García, A.; Ilabaca, J. Estructura y funciones de la Atención Primaria de Salud según el Primary Care Assessment Tool para prestadores en la comuna de Conchalí—Santiago de Chile. Rev. Médica Chile 2019, 147, 305–313. [Google Scholar]
- Piña, N.M.; Chiang-Vega, M.M.; Lama, S. Variación en el nivel de compromiso y estrés laboral de los funcionarios del Hospital de Yungay Chile tras implementar un plan de intervención que los involucre en el proceso de acreditación. Rev. Fac. Cienc. Salud UDES 2018, 5, 24–35. [Google Scholar] [CrossRef]
- Khoury, J.; Krejany, C.J.; Versteeg, R.W.; Lodewyckx, M.A.; Pike, S.R.; Civil, M.S.; Jiwa, M. A process for developing standards to promote quality in general practice. Fam. Pract. 2019, 36, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Superintendencia de Salud. Gobierno de Chile. Guía Práctica para el Proceso de Acreditación de Prestadores Institucionales de Salud; Technical Report; Superintendencia de Salud, Gobierno de Chile: Santiago, Chile, 2020. [Google Scholar]
- Hernández Palma, H.G. Factores críticos para promover la calidad en el sector salud del Departamento del Atlántico. Investig. Innovación Ing. 2017, 4, 94–103. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Accreditation | No | Yes | Total | % No | % Yes |
|---|---|---|---|---|---|
| CESFAM 1 | 560 | 33 | 593 | 9444 | 556 |
| Communes 2,3 | 255 | 17 | 272 | 9375 | 625 |
| Regions | 9 | 7 | 16 | 5625 | 4375 |
| Variable | Description | Unit | Class | |
|---|---|---|---|---|
| 1 | ISAL012 | Contribution of the MINSAL (per capita) with respect to the total income of the health sector | % | Financial management |
| APMUNI | Municipal contribution to the health sector per registered person validated | M$ | Financial management | |
| ISAL016 | Municipal transfers to health on municipal own income | % | Financial management | |
| ISAL019 | Expenditure on personnel in the health sector | M$ | HR management | |
| ISAL020 | Percentage of expenditure on health personnel over total expenditure | % | HR management | |
| ISAL021 | Operating expenses of the health sector | M$ | Financial management | |
| ISAL022 | Percentage of operating expenses over total health expenditure | % | Financial management | |
| ISAL025 | Expenditure on personal training health area | M$ | HR management | |
| ISAL031 | Expenditure on personnel to health sector by contract | M$ | HR management | |
| ISAL23 | Annual expenditure of the health area per registered inhabitant validated | M$ | HR management | |
| PORMPV | Percentage of women between 25 and 64 years with current PAP | % | Clinical management | |
| MPSP | Number of staff in health sector | No. | HR management | |
| MTCM1019 | Morbidity consultations made to adolescents between 10–19 | No. | Clinical management | |
| MTFCM | Total number of contracted physicians as of December 31 | No. | HR management | |
| HPISM | Registered population validated in municipal health services (FONASA) | No. | Demographic | |
| 2 | POBRINCOME | Percentage of people in a situation of income poverty | % | Socio-economic |
| POBRMULT | Percentage of people in a situation of multidimensional poverty | % | Socio-economic | |
| 3 | POPULATION | Population census 2017 | No. | Demographic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coss-Mandiola, J.; Vanegas-López, J.; Rojas, A.; Carrasco, R.; Dubo, P.; Campillay-Campillay, M. Characterization of Communes with Quality Accredited Primary Healthcare Centers in Chile. Int. J. Environ. Res. Public Health 2022, 19, 9189. https://doi.org/10.3390/ijerph19159189
Coss-Mandiola J, Vanegas-López J, Rojas A, Carrasco R, Dubo P, Campillay-Campillay M. Characterization of Communes with Quality Accredited Primary Healthcare Centers in Chile. International Journal of Environmental Research and Public Health. 2022; 19(15):9189. https://doi.org/10.3390/ijerph19159189
Chicago/Turabian StyleCoss-Mandiola, Juan, Jairo Vanegas-López, Alejandra Rojas, Raúl Carrasco, Pablo Dubo, and Maggie Campillay-Campillay. 2022. "Characterization of Communes with Quality Accredited Primary Healthcare Centers in Chile" International Journal of Environmental Research and Public Health 19, no. 15: 9189. https://doi.org/10.3390/ijerph19159189
APA StyleCoss-Mandiola, J., Vanegas-López, J., Rojas, A., Carrasco, R., Dubo, P., & Campillay-Campillay, M. (2022). Characterization of Communes with Quality Accredited Primary Healthcare Centers in Chile. International Journal of Environmental Research and Public Health, 19(15), 9189. https://doi.org/10.3390/ijerph19159189