
Health Care Providers’ Perspectives on Promoting Physical Activity and Exercise in Health Care

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Provider Physical Activity Perception Questionnaire
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morris, J.N. Exercise in the prevention of coronary heart disease: Today’s best buy in public health. Med. Sci. Sports Exerc. 1994, 26, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Koné Pefoyo, A.J.; Bronskill, S.E.; Gruneir, A.; Calzavara, A.; Thavorn, K.; Petrosyan, Y.; Maxwell, C.J.; Bai, Y.; Wodchis, W.P. The increasing burden and complexity of multimorbidity disease epidemiology—Chronic. BMC Public Health 2015, 15, 415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. S3), 1–72. [Google Scholar] [CrossRef] [Green Version]
- Naci, H.; John, P.A. Comparative effectiveness of exercise and drug interventions on mortality outcomes: Metaepidemiological study. BMJ 2013, 347, f5577. [Google Scholar] [CrossRef] [Green Version]
- Nova Scotia Health Authority. Nova Scotia Health Profile. Introduction Health Profile. 2015. Available online: https://novascotia.ca/dhw/publichealth/documents/Population-Health-Profile-Nova-Scotia.pdf (accessed on 9 January 2022).
- Lion, A.; Vuillemin, A.; Thornton, J.S.; Theisen, D.; Stranges, S.; Ward, M. Physical activity promotion in primary care: A Utopian quest? Health Promot. Int. 2019, 34, 877–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, F.A.; Crowe, M.J.; Malau-Aduli, A.E.O.; Malau-Aduli, B.S. Physical activity promotion: A systematic review of the perceptions of healthcare professionals. Int. J. Environ. Res. Public Health 2020, 17, 4358. [Google Scholar] [CrossRef]
- Hébert, E.T.; OCaughy, M.; Shuval, K. Primary care providers’ perceptions of physical activity counselling in a clinical setting: A systematic review. Br. J. Sports Med. 2012, 46, 625–631. [Google Scholar] [CrossRef]
- Petrella, R.J.; Lattanzio, C.N.; Overend, T.J. Physical activity counseling and prescription among Canadian primary care physicians. Arch. Intern. Med. 2007, 167, 1774–1781. [Google Scholar] [CrossRef]
- Short, C.E.; Hayman, M.; Rebar, A.L.; Gunn, K.M.; De Cocker, K.; Duncan, M.J.; Turnbull, D.; Dollman, J.; Van Uffelen, J.G.; Vandelanotte, C. Physical activity recommendations from general practitioners in Australia. Results from a national survey. Aust. N. Zealand J. Public Health 2015, 40, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, M.W.; Shields, C.A.; Dunbar, M.J.; Crowell, S.J.; Fowles, J.R. Physical activity counselling and exercise prescription practices among dietitians across nova scotia. Can. J. Diet. Pract. Res. 2022, 83, 35–40. [Google Scholar] [CrossRef]
- Litchfield, I.; Andrews, R.C.; Narendran, P.; Greenfield, S. Patient and healthcare professionals perspectives on the delivery of exercise education for patients with type 1 diabetes. Front. Endocrinol. 2019, 10, 76. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.W.; Shields, C.A.; Campbell, K.L.; Crowell, S.J.; Fowles, J.R. Perceptions and practices of providing physical activity counselling and exercise prescriptions among physiotherapists in nova scotia. Physiother. Can. 2020, 72, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Freene, N.; Cools, S.; Bissett, B. Are we missing opportunities? Physiotherapy and physical activity promotion: A cross-sectional survey. BMC Sports Sci. Med. Rehabil. 2017, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.W.; Bray, N.W.; Kivell, M.J.; Fowles, J.R. A scoping review of exercise referral schemes involving qualified exercise professionals in primary health care. Appl. Physiol. Nutr. Metab. 2021, 46, 1007–1018. [Google Scholar] [CrossRef]
- Nova Scotia Health Authority. Finding a Primary Care Provider in Nova Scotia—April 2022. Available online: https://www.nshealth.ca/files/finding-provider-nova-scotia-public-report-april-2022 (accessed on 4 May 2022).
- Tomasone, J.R.; Flood, S.M.; Latimer-Cheung, A.E.; Faulkner, G.; Duggan, M.; Jones, R.; Lane, K.N.; Bevington, F.; Carrier, J.; Dolf, M.; et al. Knowledge translation of the Canadian 24-Hour movement guidelines for adults aged 18–64 years and adults aged 65 years or older: A collaborative movement guideline knowledge translation process. Appl. Physiol. Nutr. Metab. 2020, 45, 103–124. [Google Scholar] [CrossRef] [PubMed]
- Education Committee on Allied Health and Accreditation. What Does “Allied Health” Mean? Allied Health Education Directory; National Academy Press: Washington, DC, USA, 1993. [Google Scholar]
- O’Brien, M.; Shields, C.; Crowell, S.; Theou, O.; McGrath, P.; Fowles, J. The effects of previous educational training on physical activity counselling and exercise prescription practices among physicians across Nova Scotia: A cross-sectional study. Can. Med. Educ. J. 2018, 9, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Dacey, M.; Arnstein, F.; Kennedy, M.A.; Wolfe, J.; Phillips, E.M. The impact of lifestyle medicine continuing education on provider knowledge, attitudes, and counseling behaviors. Med. Teach. 2012, 35, e1149–e1156. [Google Scholar] [CrossRef]
- Shields, C.A.; Fowles, J.R.; Dunbar, P.; Barron, B.; McQuaid, S.; Dillman, C.J. Increasing diabetes educators’ confidence in physical activity and exercise counselling: The effectiveness of the “physical activity and exercise toolkit” training intervention. Can. J. Diabetes 2013, 37, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, M.W.; Shields, C.A.; Oh, P.; Fowles, J.R. Health care provider confidence and exercise prescription practices of Exercise is Medicine Canada workshop attendees. Appl. Physiol. Nutr. Metab. 2017, 42, 384–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elley, C.R.; Kerse, N.; Arroll, B.; Robinson, E. Effectiveness of counselling patients on physical activity in general practice: Cluster randomised controlled trial. BMJ 2003, 326, 793. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.M.; Skerrett, P.J. Physical activity and all-cause mortality: What is the dose-response relation? Med. Sci. Sports Exerc. 2001, 33, S459–S471. [Google Scholar] [CrossRef] [PubMed]
- Solmundson, K.; Koehle, M.; McKenzie, D. Exercise medicine in residency training. Med. Sci. Sports Exerc. 2016, 48, 131. [Google Scholar] [CrossRef]
- CSEP. CSEP Physical Activity Training for Health® (CSEP-PATH®) Resource Manual, 3rd ed.; CSEP: Ottawa, ON, Canada, 2021. [Google Scholar]
- Fien, S.; Linton, C.; Mitchell, J.S.; Wadsworth, D.P.; Szabo, H.; Askew, C.D.; Schaumberg, M.A. Characteristics of community-based exercise programs for community-dwelling older adults in rural/regional areas: A scoping review. Aging 2022, 34, 1511–1528. [Google Scholar] [CrossRef] [PubMed]
- Yun, L.; Vanderloo, L.; Berry, T.R.; Latimer-Cheung, A.E.; O’Reilly, N.; Rhodes, R.E.; Spence, J.C.; Tremblay, M.S.; Faulkner, G. Assessing the social climate of physical (in)activity in Canada. BMC Public Health 2018, 18, 1301. [Google Scholar] [CrossRef] [Green Version]
- Orrow, G.; Kinmonth, A.-L.; Sanderson, S.; Sutton, S. Effectiveness of physical activity promotion based in primary care: Systematic review and meta-analysis of randomised controlled trials. BMJ 2012, 344, e1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, J.R. A quantitative estimate of the clinical significance of treating tobacco dependence. Am. J. Prev. Med. 2010, 39, 285–286. [Google Scholar] [CrossRef] [Green Version]
- Queralt, A.; Queralt, V.; Molina-García, J. Physical exercise prescription by primary care nurses. J. Sci. Med. Sport 2012, 15, 350–351. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Physicians (n = 114) | Nurses (n = 48) | Dietitians (n = 65) | Exercise Professionals (n = 114) | |
|---|---|---|---|---|
| Age (years) | 52 ± 12 | 50 ± 10 | 41 ± 11 | 43 ± 11 |
| Years of Practice | 23 ± 13 | 27 ± 9 | 15 ± 10 | 18 ± 11 |
| Gender (% women) | 54.9 | 97.9 | 96.9 | 75.2 |
| Race (% Caucasian) | 86.7 | 97.9 | 100.0 | 94.6 |
| Include PAE in sessions (% of patients/clients) | 43 ± 30 | 55 ± 36 | 57 ± 30 | 85 ± 22 |
| Assess PAE Participations (% of patients/clients) | 47 ± 34 | 66 ± 37 | 60 ± 37 | 82 ± 26 |
| Assess PAE Readiness (% of patients/clients) | 35 ± 32 | 58 ± 38 | 57 ± 35 | 69 ± 35 |
| Recommend PAE (% of patients/clients) | 63 ± 30 | 73 ± 31 | 70 ± 28 | 93 ± 13 |
| Prescribe Exercise (% of patients/clients) | 13 ± 21 | 19 ± 30 | 20 ± 29 | 83 ± 24 |
| Provide PAE Referral (% of patients/clients) | 10 ± 18 | 17 ± 27 | 16 ± 22 | 25 ± 26 |
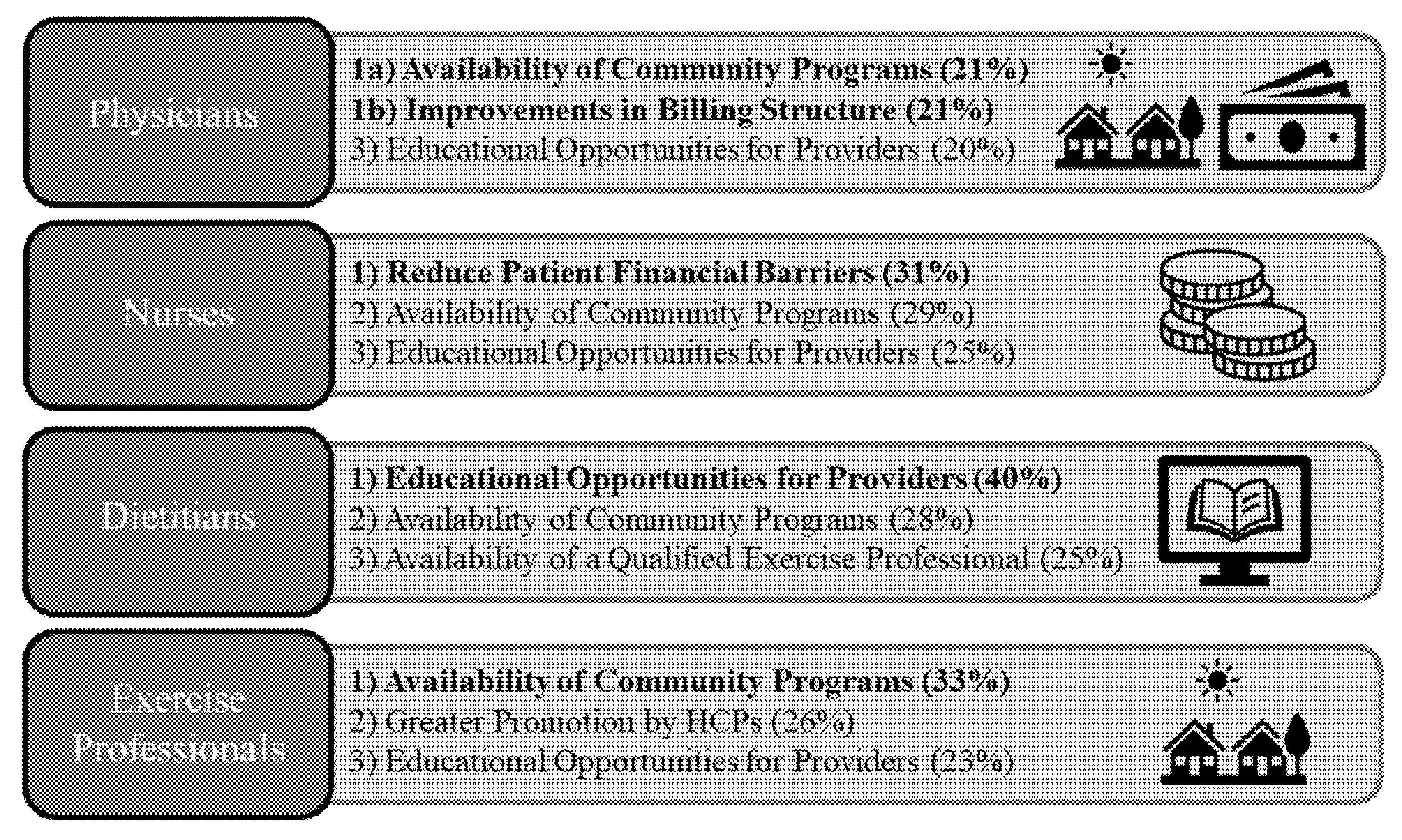
| Theme | Physicians (n = 114) | Nurses (n = 48) | Dietitians (n = 65) | Exercise Professionals (n = 114) |
|---|---|---|---|---|
| Community Program Availability (%) | 21 | 29 | 28 | 33 |
| Educational Opportunities for HCPs (%) | 20 | 25 | 40 | 23 |
| More Frequent Promotion by HCP (%) | 12 | 22 | 17 | 26 |
| Qualified Exercise Professional Availability (%) | 11 | 12 | 25 | 20 |
| Reduce Patient Financial Barriers (%) | 19 | 31 | 11 | 16 |
| Tools/Resources for HCPs to use (%) | 12 | 12 | 17 | 9 |
| Greater Public Promotion (%) | 18 | 12 | 3 | 12 |
| Improvements in Billing Structure (%) | 21 | 4 | 2 | 8 |
| Intervene in Childhood (%) | 11 | 10 | 3 | 14 |
| Tools/Resources for Patients (%) | 10 | 10 | 5 | 8 |
| Other (%) | 9 | 10 | 9 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellerine, L.P.; O’Brien, M.W.; Shields, C.A.; Crowell, S.J.; Strang, R.; Fowles, J.R. Health Care Providers’ Perspectives on Promoting Physical Activity and Exercise in Health Care. Int. J. Environ. Res. Public Health 2022, 19, 9466. https://doi.org/10.3390/ijerph19159466
Pellerine LP, O’Brien MW, Shields CA, Crowell SJ, Strang R, Fowles JR. Health Care Providers’ Perspectives on Promoting Physical Activity and Exercise in Health Care. International Journal of Environmental Research and Public Health. 2022; 19(15):9466. https://doi.org/10.3390/ijerph19159466
Chicago/Turabian StylePellerine, Liam P., Myles W. O’Brien, Chris A. Shields, Sandra J. Crowell, Robert Strang, and Jonathon R. Fowles. 2022. "Health Care Providers’ Perspectives on Promoting Physical Activity and Exercise in Health Care" International Journal of Environmental Research and Public Health 19, no. 15: 9466. https://doi.org/10.3390/ijerph19159466
APA StylePellerine, L. P., O’Brien, M. W., Shields, C. A., Crowell, S. J., Strang, R., & Fowles, J. R. (2022). Health Care Providers’ Perspectives on Promoting Physical Activity and Exercise in Health Care. International Journal of Environmental Research and Public Health, 19(15), 9466. https://doi.org/10.3390/ijerph19159466