
Proof of Concept of a 6-Month Person-Oriented Exercise Intervention ‘MultiPill-Exercise’ among Patients at Risk of or with Multiple Chronic Diseases: Results of a One-Group Pilot Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
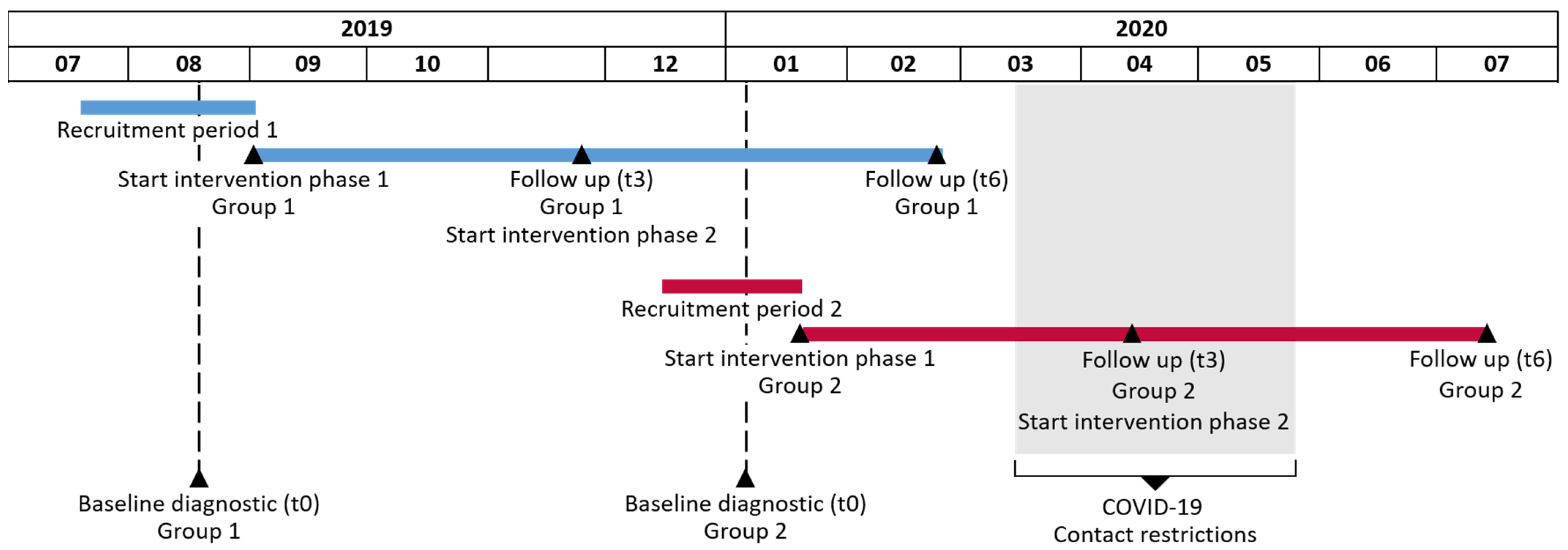
2.1. Study Design and Setting
2.2. Participants
2.3. Sample Size Calculation
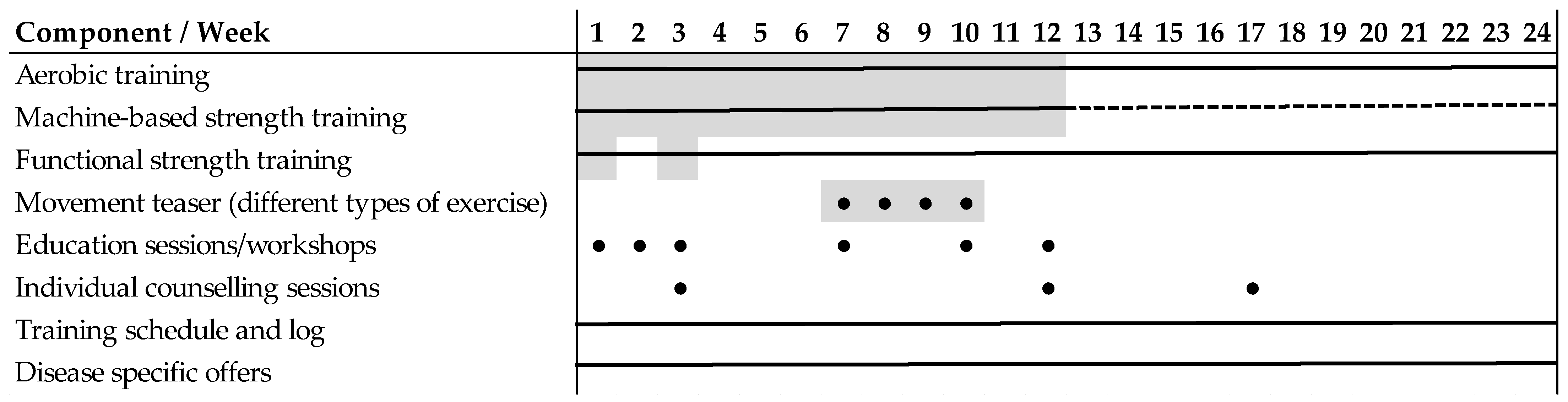
2.4. Person-Oriented Physical Exercise Intervention ‘MultiPill-Exercise’
2.5. Data Collection and Outcome Measures
2.5.1. Baseline Characteristics and Exercise Pre-Participation Screening
2.5.2. Primary Outcome Measure: Physical Exercise Participation
2.5.3. Secondary Outcome Measures
Physical Performance Measures
2.6. Statistical Methods
2.6.1. Data Analysis
2.6.2. Handling of Missing Data
3. Results
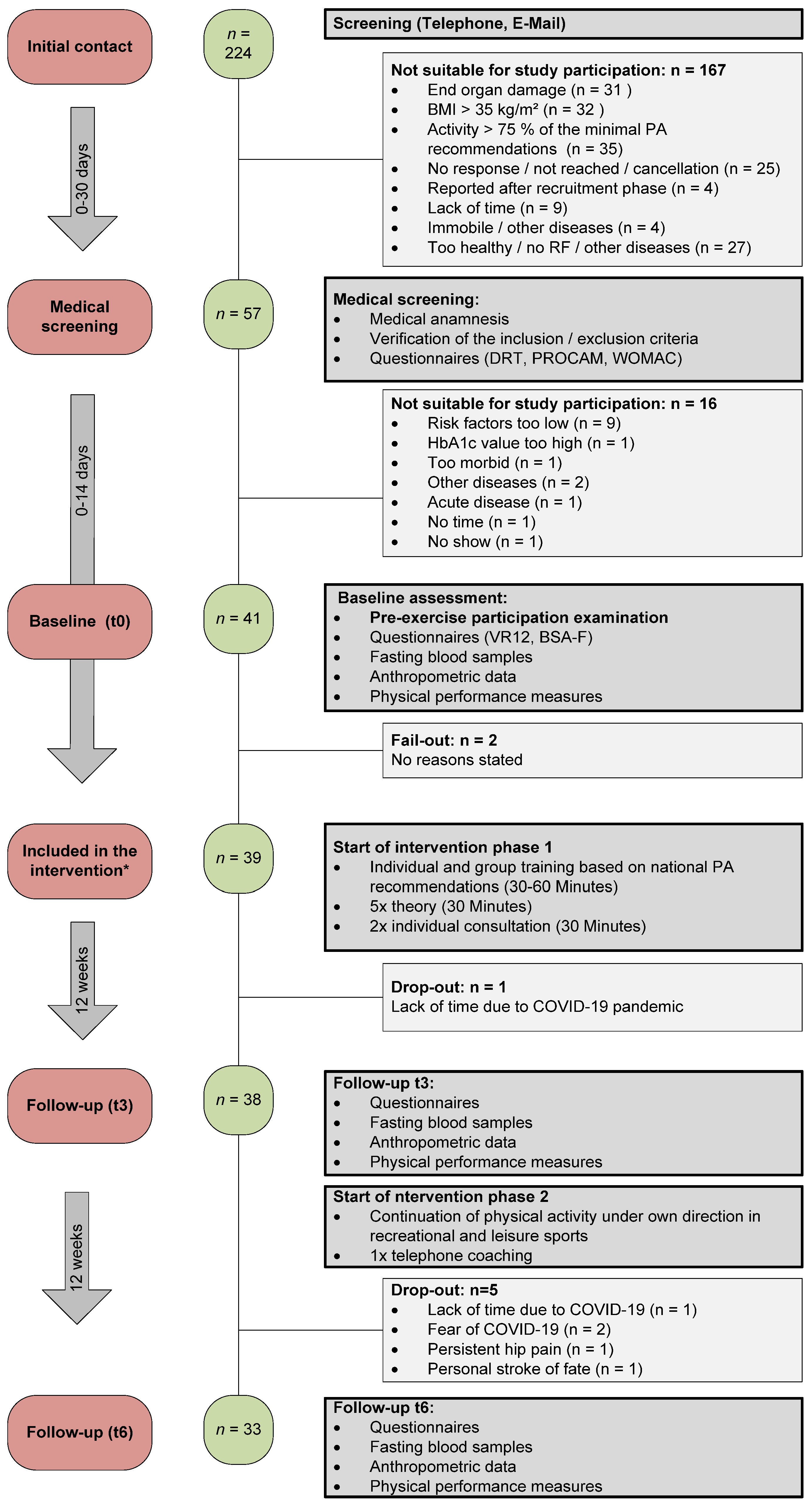
3.1. Recruitment
3.2. Baseline Characteristics of the Participants
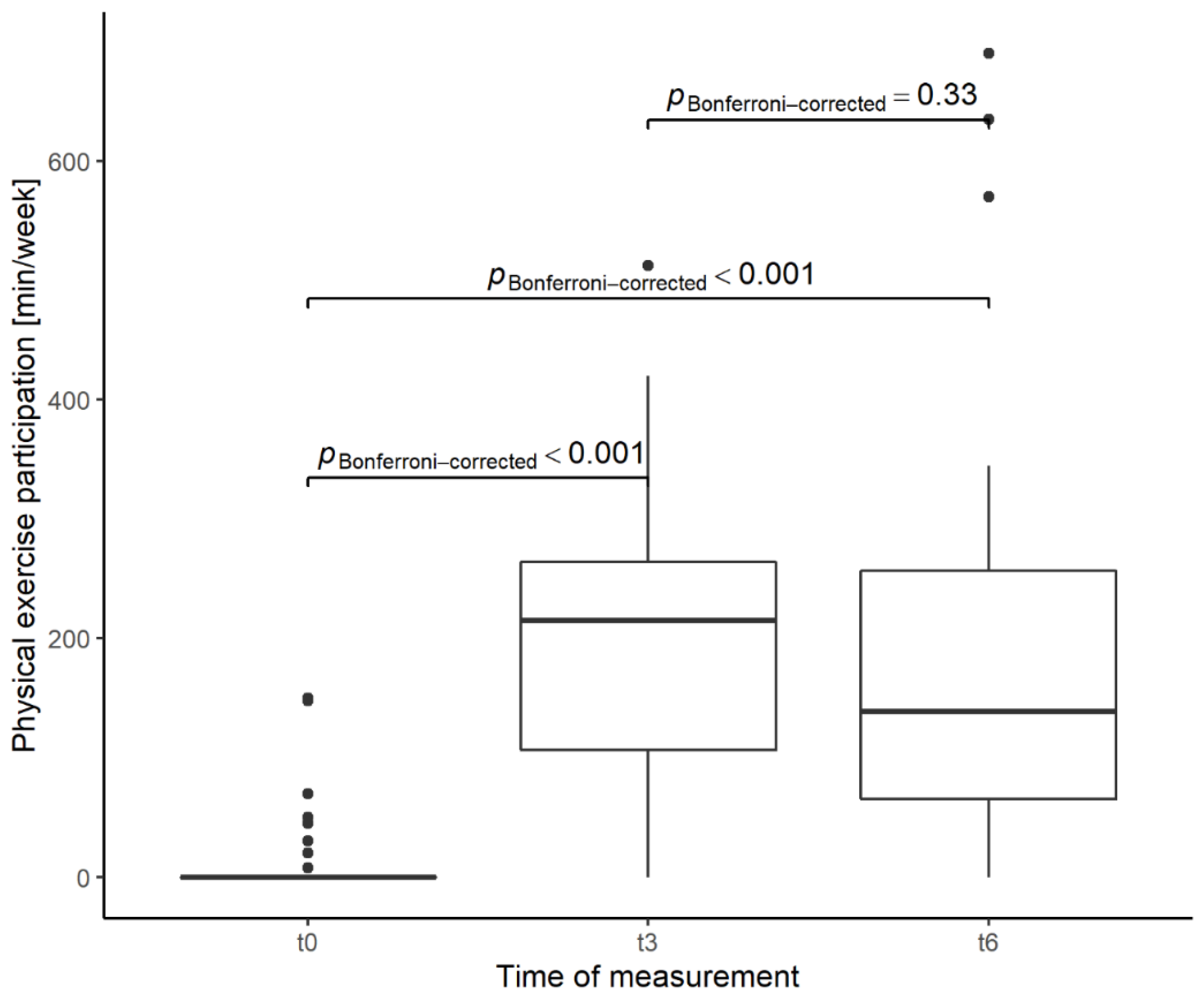
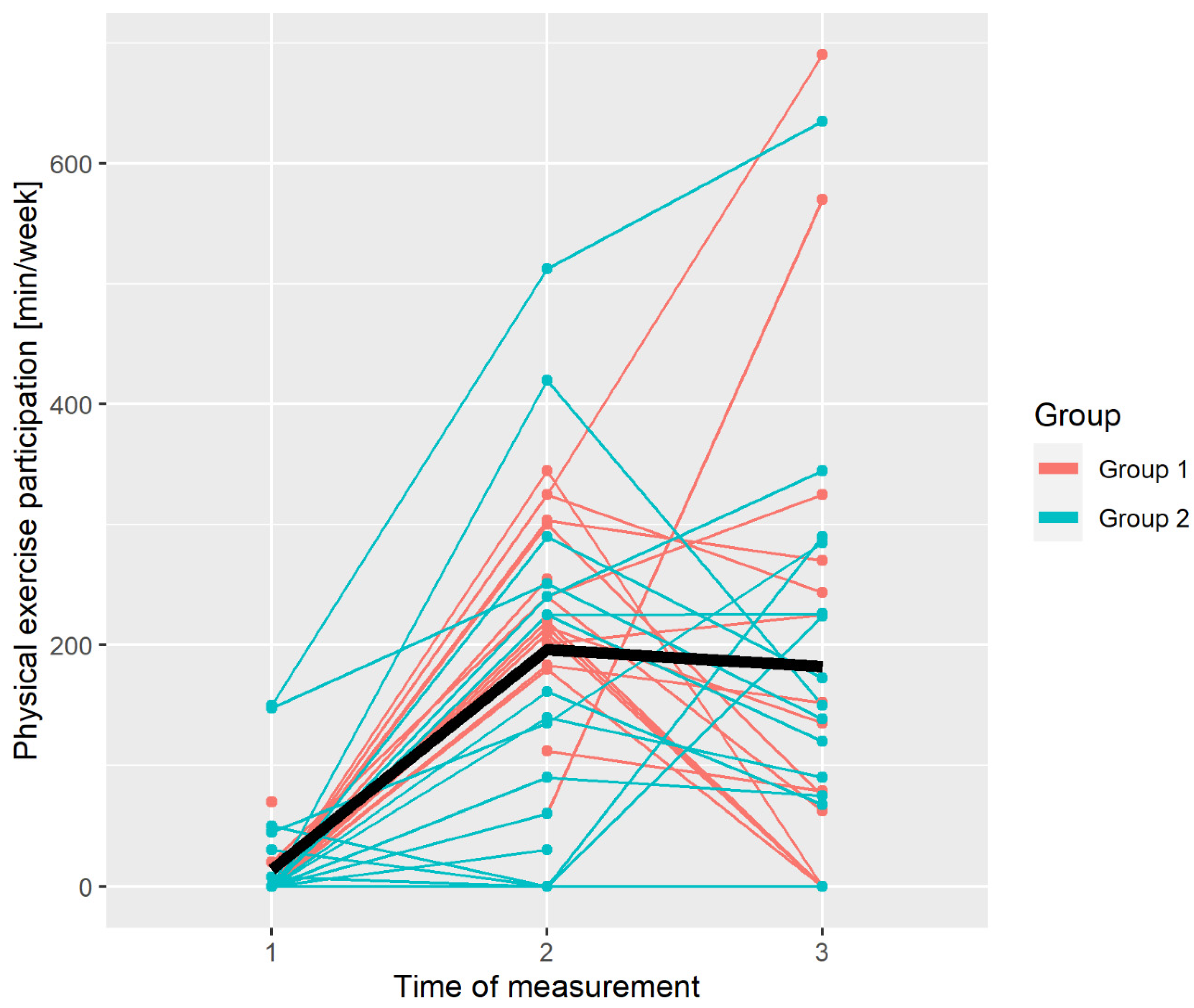
3.3. Primary Outcome Measure: Physical Exercise Participation
3.4. Secondary Outcomes
Physical Performance Measures
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Content/Technique | Rational/Determinant | Setting (How) | Dosage Phase 1 | Dosage Phase 2 | References |
|---|---|---|---|---|---|---|
| Endurance training |
| Knowledge, self-efficacy | HCC or HB, indoor or outdoor, group or individual | At least 2 x/week, total duration: 90–150 min moderate training or 45–75 min of vigorous training:
| At least 2–3 x/week, total duration 150 min moderate (moderate: 70% max. PO or 75 min of vigorous (for EIT: intense: 90% max. PO) training | [28,77,78,79] |
| Machine-based strength training | Strength training using weight-machines | Knowledge, self-efficacy | HCC, individual | At least 1 x/week, duration: approx. 90 min
| [28,77,78,79] | |
| Functional training | Whole body strengthening exercises with own body weight | Knowledge, self-efficacy | HB, leaflet/video instruction ii | At least 1 x/week, duration 30 min Strength endurance, 30–40% of maximum/BORG 6-7 W 1-12: S 3-R 25 | At least 1 x/week, duration 30 min Strength endurance training, 30–40% of maximum/BORG 6-7 W 1-12: S 3-R 25 | [28,77,78,79] |
| Movement Teaser | COMET:
| Self-efficacy, self-concordance | HCC, Indoor or Outdoor, group training | 4 units, each 60 min | COMET [80] | |
| Patient education session, delivering theoretical and practical knowledge | Competence approach (learning, reflecting, experiencing)
| Risk perception, knowledge, outcome expectation, self-efficacy, self-concordance, goal setting, coping strategies | HCC, group training | 5 units each 30 min | 1 unit, 30–45 min | MoVo [54] BMZI [81] Active everyday life [27,82,83] |
| Training log | BCT (motivational) Weekly targets and feedback | Action and coping planning, goal setting, outcome expectation | HB and HCC | 1/week | 1/week | [54,84] |
| Individual counselling sessions | MI, 5A’s, BCT
| Self-efficacy, outcome expectation, outcome experience | HCC/Written Feedback (Dietetics) | 3 | 2 | MI [85] 5A’s [86] MoVo [54] COMET [80] Anti-inflammatory diet [87] |
| Disease-specific offers |
| Additional disease-specific offers to enhance health benefits. | HCC and HB | Optional: 1–2 offers/person | [88,89] |
Appendix B
| Week | Intervention Group | Frequency Endurance (Mean in %) | Time Endurance (Mean in %) | Frequency Strength (Mean in %) | Missing Datasets (n) |
|---|---|---|---|---|---|
| 1 | Group 1 | 92.5 | 92.0 | 92.5 | 0 |
| Group 2 | 83.3 | 84.4 | 69.4 | 0 | |
| Overall | 87.9 | 88.2 | 81.0 | 0 | |
| 2 | Group 1 | 97.5 | 95.0 | 100.0 | 0 |
| Group 2 | 61.1 | 61.5 | 100.0 | 0 | |
| Overall | 79.3 | 78.2 | 100.0 | 0 | |
| 3 | Group 1 | 95.0 | 83.7 | 97.5 | 0 |
| Group 2 | 94.4 | 100.0 | 100.0 | 0 | |
| Overall | 94.7 | 91.8. | 98.8 | 0 | |
| 4 | Group 1 | 100.0 | 92.4 | 97.5 | 0 |
| Group 2 | 63.9 | 63.3 | 58.3 | 3 | |
| Overall | 81.9 | 77.8 | 77.9 | 3 | |
| 5 | Group 1 | 100.0 | 94.9 | 75.0 | 0 |
| Group 2 | 91.7 | 96.7 | 86.1 | 0 | |
| Overall | 95.8 | 95.8 | 80.6 | 0 | |
| 6 | Group 1 | 85.0 | 84.9 | 70.0 | 0 |
| Group 2 | 63.9 | 55.2 | 63.9 | 3 | |
| Overall | 74.4 | 70.0 | 66.9 | 3 | |
| 7 | Group 1 | 77.5 | 84.4 | 80.0 | 0 |
| Group 2 | 69.4 | 57.8 | 63.9 | 2 | |
| Overall | 73.5 | 71.1 | 71.9 | 2 | |
| 8 | Group 1 | 85.0 | 84.7 | 82.5 | 1 |
| Group 2 | 72.2 | 56.9 | 58.3 | 4 | |
| Overall | 78.6 | 70.8 | 70.4 | 5 | |
| 9 | Group 1 | 85.0 | 76.8 | 70.0 | 2 |
| Group 2 | 63.9 | 55.6 | 30.6 | 5 | |
| Overall | 74.4 | 66.2 | 50.3 | 7 | |
| 10 | Group 1 | 82.5 | 78.3 | 100.0 | 0 |
| Group 2 | 55.6 | 54.8 | 52.8 | 5 | |
| Overall | 69.0 | 66.6 | 76.4 | 5 | |
| 11 | Group 1 | 77.5 | 89.8 | 67.5 | 0 |
| Group 2 | 58.3 | 58.8 | 44.4 | 5 | |
| Overall | 67.9 | 74.3 | 56.0 | 5 | |
| 12 | Group 1 | 75.0 | 65.2 | 70.0 | 2 |
| Group 2 | 66.7 | 60.6 | 47.2 | 4 | |
| Overall | 70.8 | 62.9 | 58.6 | 6 |

References
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–2. [Google Scholar] [PubMed]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Hämäläinen, R.-M.; Breda, J.; da Silva Gomes, F.; Gongal, G.; Khan, W.; Mendes, R.; Nederveen, L.; Ramanandraibe, N.; Sako, B.; Whiting, S. New global physical activity guidelines for a more active and healthier world: The WHO Regional Offices perspective. Br. J. Sports Med. 2020, 54, 1449–1450. [Google Scholar] [CrossRef] [PubMed]
- Comission, E. Eurobarometer on Sport and Physical Activity. Available online: https://sport.ec.europa.eu/news/new-eurobarometer-on-sport-and-physical-activity (accessed on 23 February 2021).
- Bertuol, C.; Tozetto, W.R.; Streb, A.R.; Del Duca, G.F. Combined relationship of physical inactivity and sedentary behaviour with the prevalence of noncommunicable chronic diseases: Data from 52,675 Brazilian adults and elderly. Eur. J. Sport Sci. 2021, 22, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [Green Version]
- National Guideline Centre. National Guideline Centre. National Institute for Health and Care Excellence: Clinical Guidelines. In Multimorbidity: Assessment, Prioritisation and Management of Care for People with Commonly Occurring Multimorbidity; National Institute for Health and Care Excellence: London, UK, 2016. [Google Scholar]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef]
- Garin, N.; Koyanagi, A.; Chatterji, S.; Tyrovolas, S.; Olaya, B.; Leonardi, M.; Lara, E.; Koskinen, S.; Tobiasz-Adamczyk, B.; Ayuso-Mateos, J.L.; et al. Global Multimorbidity Patterns: A Cross-Sectional, Population-Based, Multi-Country Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 205–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzuto, D.; Melis, R.J.F.; Angleman, S.; Qiu, C.; Marengoni, A. Effect of Chronic Diseases and Multimorbidity on Survival and Functioning in Elderly Adults. J. Am. Geriatr. Soc. 2017, 65, 1056–1060. [Google Scholar] [CrossRef] [Green Version]
- Rijken, M.; Struckmann, V.; Dyakova, M.; Melchiorre, M.G.; Rissanen, S.; Van Ginneken, E. ICARE4EU: Improving care for people with multiple chronic conditions in Europe. Eurohealth Inc. Euro Obs. 2013, 19, 29–31. [Google Scholar]
- Smith, S.M.; Wallace, E.; O’Dowd, T.; Fortin, M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst. Rev. 2017, 3, Cd006560. [Google Scholar] [CrossRef]
- Rijken, P.M.; Bekkema, N. Chronic Disease Management Matrix 2010: Results of a Survey in Ten European Countries; Belgian Federal Institute for Health and Disability Insurance: Utrecht, The Netherlands, 2011; pp. 1–146. [Google Scholar]
- Rijken, M.; Hujala, A.; van Ginneken, E.; Melchiorre, M.G.; Groenewegen, P.; Schellevis, F. Managing multimorbidity: Profiles of integrated care approaches targeting people with multiple chronic conditions in Europe. Health Policy 2018, 122, 44–52. [Google Scholar] [CrossRef] [PubMed]
- de Rooij, M.; van der Leeden, M.; Cheung, J.; van der Esch, M.; Häkkinen, A.; Haverkamp, D.; Roorda, L.D.; Twisk, J.; Vollebregt, J.; Lems, W.F.; et al. Efficacy of Tailored Exercise Therapy on Physical Functioning in Patients With Knee Osteoarthritis and Comorbidity: A Randomized Controlled Trial. Arthritis. Care Res. 2017, 69, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Stoll, C.R.T.; Izadi, S.; Fowler, S.; Philpott-Streiff, S.; Green, P.; Suls, J.; Winter, A.C.; Colditz, G.A. Multimorbidity in randomized controlled trials of behavioral interventions: A systematic review. Health Psychol. J. Div. Health Psychol. Am. Psychol. Assoc. 2019, 38, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Sudeck, G.; Geidl, W.; Abu-Omar, K.; Finger, J.; Krauß, I.; Pfeifer, K. Do adults with non-communicable diseases meet the German physical activity recommendations—A cross-sectional analysis of the GEDA-2014/2015 survey. Ger. J. Exerc. Sport Res. 2021, 51, 183–193. [Google Scholar] [CrossRef]
- Chudasama, Y.V.; Khunti, K.; Gillies, C.L.; Dhalwani, N.N.; Davies, M.J.; Yates, T.; Zaccardi, F. Healthy lifestyle and life expectancy in people with multimorbidity in the UK Biobank: A longitudinal cohort study. PLoS Med. 2020, 17, 1003332. [Google Scholar] [CrossRef]
- Brawner, C.A.; Churilla, J.R.; Keteyian, S.J. Prevalence of Physical Activity Is Lower among Individuals with Chronic Disease. Med. Sci. Sports Exerc. 2016, 48, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Dobson, F.; Bennell, K.L.; French, S.D.; Nicolson, P.J.; Klaasman, R.N.; Holden, M.A.; Atkins, L.; Hinman, R.S. Barriers and Facilitators to Exercise Participation in People with Hip and/or Knee Osteoarthritis: Synthesis of the Literature Using Behavior Change Theory. Am. J. Phys. Med. Rehabil. 2016, 95, 372–389. [Google Scholar] [CrossRef]
- Jansons, P.S.; Robins, L.; Haines, T.P.; O’Brien, L. Barriers and enablers to ongoing exercise for people with chronic health conditions: Participants’ perspectives following a randomized controlled trial of two interventions. Arch. Gerontol. Geriatr. 2018, 76, 92–99. [Google Scholar] [CrossRef]
- Brawley, L.R.; Rejeski, W.J.; King, A.C. Promoting physical activity for older adults—The challenges for changing behavior. Am. J. Prev. Med. 2003, 25, 172–183. [Google Scholar] [CrossRef]
- Geidl, W.; Semrau, J.; Pfeifer, K. Health behaviour change theories: Contributions to an ICF-based behavioural exercise therapy for individuals with chronic diseases. Disabil. Rehabil. 2014, 36, 2091–2100. [Google Scholar] [CrossRef] [PubMed]
- Sudeck, G.; Pfeifer, K. Physical activity-related health competence as an integrative objective in exercise therapy and health sports—conception and validation of a short questionnaire. Sportwissenschaft 2016, 46, 74–87. [Google Scholar] [CrossRef]
- Carl, J.; Sudeck, G.; Pfeifer, K. Competencies for a Healthy Physically Active Lifestyle—Reflections on the Model of Physical Activity-Related Health Competence. J. Phys. Act. Health 2020, 17, 688. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Erlbaum: Hillsdals, NJ, USA, 1988; Volume 2. [Google Scholar]
- WHO. International Classification of Functioning, Disability and Health (ICF). Available online: https://www.who.int/classifications/icf/en/ (accessed on 30 July 2020).
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: champaign, IL, USA, 1998. [Google Scholar]
- Schweda, S.; Sudeck, G.; Schmid, J.; Janßen, P.; Krauß, I. MultiPill-Exercise: Conception of an individualized exercise program for people with multiple chronic diseases at the interfaces of health care as well as recreational and health sports. BG 2021, 37, 30–36. [Google Scholar]
- Schweda, S.; Müller, G.; Munz, B.; Sudeck, G.; Martus, P.; Dierkes, K.; Krauss, I. Implementation and evaluation of an individualized physical exercise promotion program in people with manifested risk factors for multimorbidity (MultiPill-Exercise): A study protocol for a pragmatic randomized controlled trial. BMC Public Health 2022, 22, 1174. [Google Scholar] [CrossRef]
- Assmann, G.; Schulte, H.; Cullen, P.; Seedorf, U. Assessing risk of myocardial infarction and stroke: New data from the Prospective Cardiovascular Münster (PROCAM) study. Eur. J. Clin. Investig. 2007, 37, 925–932. [Google Scholar] [CrossRef]
- Mühlenbruch, K.; Ludwig, T.; Jeppesen, C.; Joost, H.-G.; Rathmann, W.; Meisinger, C.; Peters, A.; Boeing, H.; Thorand, B.; Schulze, M.B. Update of the German Diabetes Risk Score and external validation in the German MONICA/KORA study. Diabetes Res. Clin. Pract. 2014, 104, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Fuchs, R.; Klaperski, S.; Gerber, M.; Seelig, H. Messung der Bewegungs- und Sportaktivität mit dem BSA-Fragebogen. Z. Gesundh. 2015, 23, 60–76. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N. Physical Activity & Behavioral Medicine; SAGE Publications, Inc.: London, UK, 1999. [Google Scholar] [CrossRef]
- Kazis, L.E.; Selim, A.; Rogers, W.; Ren, X.S.; Lee, A.; Miller, D.R. Dissemination of methods and results from the Veterans Health Study: Final comments and implications for future monitoring strategies within and outside the veterans healthcare system. J. Ambul. Care Manag. 2006, 29, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A. Just one question: If one question works, why ask several? J. Epidemiol. Community Health 2005, 59, 342–345. [Google Scholar] [CrossRef] [Green Version]
- Hays, R.D.; Spritzer, K.L.; Thompson, W.W.; Cella, D.U.S. general population estimate for “excellent” to “poor” self-rated health item. J. Gen. Intern. Med. 2015, 30, 1511–1516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. nparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. J. Stat. Softw. 2012, 50, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Glossary of Common Site Terms. Available online: https://clinicaltrials.gov/ct2/about-studies/glossary (accessed on 30 December 2021).
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and how should multiple imputation be used for handling missing data in randomised clinical trials—A practical guide with flowcharts. BMC Med. Res. Methodol 2017, 17, 162. [Google Scholar] [CrossRef] [Green Version]
- Honaker, J.; King, G.; Blackwell, M. Amelia: A Program for Missing Data. J. Stat. Softw. 1998, 45, 1–47. [Google Scholar] [CrossRef]
- Lee, Y.-S.; Laffrey, S.C. Predictors of Physical Activity in Older Adults With Borderline Hypertension. Nurs. Res. 2006, 55, 110–120. [Google Scholar] [CrossRef]
- Finger, J.D.; Banzer, W.; Baumeister, S.E.; Brandes, M.; Bös, K.; Gabrys, L.; Gößwald, A.; Härtel, S.; Kluttig, A.; Kuhnert, R.; et al. Reference Values for Cardiorespiratory Fitness of the General.Population: The German National Health Interview and.Examination Survey for Adults (DEGS1) 2008–2011. Gesundheitswesen 2019, 83, 114–121. [Google Scholar]
- Selim, A.J.; Rogers, W.; Fleishman, J.A.; Qian, S.X.; Fincke, B.G.; Rothendler, J.A.; Kazis, L.E. Updated U.S. population standard for the Veterans RAND 12-item Health Survey (VR-12). Qual. Life Res. 2008, 18, 43–52. [Google Scholar] [CrossRef]
- Morfeld, M.; Bullinger, M.; Nantke, J.; Brahler, E. The version 2.0 of the SF-36 Health Survey: Results of a population-representative study. Soz. Prav. 2005, 50, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Ekblom-Bak, E.; Börjesson, M.; Bergman, F.; Bergström, G.; Dahlin-Almevall, A.; Drake, I.; Engström, G.; Engvall, J.E.; Gummesson, A.; Hagström, E.; et al. Accelerometer derived physical activity patterns in 27.890 middle-aged adults—the SCAPIS cohort study. Scand. J. Med. Sci. Sports 2022, 32, 866–880. [Google Scholar] [CrossRef] [PubMed]
- Turrisi, T.B.; Bittel, K.M.; West, A.B.; Hojjatinia, S.; Hojjatinia, S.; Mama, S.K.; Lagoa, C.M.; Conroy, D.E. Seasons, weather, and device-measured movement behaviors: A scoping review from 2006 to 2020. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 24. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.P.; Chiang, S.L.; Lin, C.H.; Liu, H.C.; Chiang, L.C. Effects of Individualized Aerobic Exercise Training on Physical Activity and Health-Related Physical Fitness among Middle-Aged and Older Adults with Multimorbidity: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 18, 101. [Google Scholar] [CrossRef]
- Weinstein, A.A.; Chin, L.M.; Keyser, R.E.; Kennedy, M.; Nathan, S.D.; Woolstenhulme, J.G.; Connors, G.; Chan, L. Effect of aerobic exercise training on fatigue and physical activity in patients with pulmonary arterial hypertension. Respir. Med. 2013, 107, 778–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, R.; Goehner, W.; Seelig, H. Long-term effects of a psychological group intervention on physical exercise and health: The MoVo concept. J. Phys. Act. Health 2011, 8, 794–803. [Google Scholar] [CrossRef] [PubMed]
- Bennie, J.A.; De Cocker, K.; Tittlbach, S. The epidemiology of muscle-strengthening and aerobic physical activity guideline adherence among 24,016 German adults. Scand. J. Med. Sci. Sports 2021, 31, 1096–1104. [Google Scholar] [CrossRef] [PubMed]
- Finger, J.D.; Tafforeau, J.; Gisle, L.; Oja, L.; Ziese, T.; Thelen, J.; Mensink, G.B.; Lange, C. Development of the European Health Interview Survey—Physical Activity Questionnaire (EHIS-PAQ) to monitor physical activity in the European Union. Arch. Public Health 2015, 73, 59. [Google Scholar] [CrossRef] [Green Version]
- Simoes, M.d.S.; Wehrmeister, F.; Romiti, M.; Gagliardi, A.d.T.; Arantes, R.; Dourado, V.Z. Effect modification of cardiorespiratory fitness, obesity, and physical activity in adults. Int. J. Sports Med. 2022, 43, 561–566. [Google Scholar] [CrossRef]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement from the American Heart Association. Circulation 2016, 134, 653–699. [Google Scholar] [CrossRef] [PubMed]
- O’Donoghue, G.; Blake, C.; Cunningham, C.; Lennon, O.; Perrotta, C. What exercise prescription is optimal to improve body composition and cardiorespiratory fitness in adults living with obesity? A network meta-analysis. Obes. Rev. 2020, 22, e13137. [Google Scholar] [CrossRef] [PubMed]
- Uusitupa, M.; Khan, T.A.; Viguiliouk, E.; Kahleova, H.; Rivellese, A.A.; Hermansen, K.; Pfeiffer, A.; Thanopoulou, A.; Salas-Salvadó, J.; Schwab, U.; et al. Prevention of Type 2 Diabetes by Lifestyle Changes: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 2611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keating, S.E.; Coombes, J.S.; Stowasser, M.; Bailey, T.G. The Role of Exercise in Patients with Obesity and Hypertension. Curr. Hypertens. Rep. 2020, 22, 21. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, J.R.; Janus, C.; Jensen, S.B.K.; Juhl, C.R.; Olsen, L.M.; Christensen, R.M.; Svane, M.S.; Bandholm, T.; Bojsen-Møller, K.N.; Blond, M.B.; et al. Healthy Weight Loss Maintenance with Exercise, Liraglutide, or Both Combined. N. Engl. J. Med. 2021, 384, 1719–1730. [Google Scholar] [CrossRef]
- Codella, R.; Ialacqua, M.; Terruzzi, I.; Luzi, L. May the force be with you: Why resistance training is essential for subjects with type 2 diabetes mellitus without complications. Endocrine 2018, 62, 14–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blond, M.B.; Rosenkilde, M.; Gram, A.S.; Tindborg, M.; Christensen, A.N.; Quist, J.S.; Stallknecht, B.M. How does 6 months of active bike commuting or leisure-time exercise affect insulin sensitivity, cardiorespiratory fitness and intra-abdominal fat? A randomised controlled trial in individuals with overweight and obesity. Br. J. Sports Med. 2019, 53, 1183–1192. [Google Scholar] [CrossRef]
- Christiansen, T.; Paulsen, S.K.; Bruun, J.M.; Pedersen, S.B.; Richelsen, B. Exercise training versus diet-induced weight-loss on metabolic risk factors and inflammatory markers in obese subjects: A 12-week randomized intervention study. Am. J. Physiol. Endocrinol. Metab. 2010, 298, E824–E831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennell, K.L.; Nelligan, R.K.; Kimp, A.J.; Schwartz, S.; Kasza, J.; Wrigley, T.V.; Metcalf, B.; Hodges, P.W.; Hinman, R.S. What type of exercise is most effective for people with knee osteoarthritis and co-morbid obesity?: The TARGET randomized controlled trial. Osteoarthr. Cartil. 2020, 28, 755–765. [Google Scholar] [CrossRef]
- Steinhilber, B.; Haupt, G.; Miller, R.; Janssen, P.; Krauss, I. Exercise therapy in patients with hip osteoarthritis: Effect on hip muscle strength and safety aspects of exercise—results of a randomized controlled trial. Mod. Rheumatol. 2017, 27, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Bullard, T.; Ji, M.; An, R.; Trinh, L.; Mackenzie, M.; Mullen, S.P. A systematic review and meta-analysis of adherence to physical activity interventions among three chronic conditions: Cancer, cardiovascular disease, and diabetes. BMC Public Health 2019, 19, 636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dwyer, M.J.; Pasini, M.; De Dominicis, S.; Righi, E. Physical activity: Benefits and challenges during the COVID-19 pandemic. J. Med. Sci. Sports 2020, 30, 1291–1294. [Google Scholar] [CrossRef] [PubMed]
- Jacob, L.; Tully, M.A.; Barnett, Y.; Lopez-Sanchez, G.F.; Butler, L.; Schuch, F.; López-Bueno, R.; McDermott, D.; Firth, J.; Grabovac, I.; et al. The relationship between physical activity and mental health in a sample of the UK public: A cross-sectional study during the implementation of COVID-19 social distancing measures. Ment. Health Phys. Act. 2020, 19, 100345. [Google Scholar] [CrossRef]
- Schweda, S.; Krauss, I. The influence of the COVID-19 lockdown on regular physical exercise habits in multiple chronic diseases. Dtsch. Z. Sportmed. 2021, 72, 365–372. [Google Scholar] [CrossRef]
- Loellgen, H.; Borjesson, M.; Cummiskey, J.; Bachl, N.; Debruyne, A. The Pre-Participation Examination in Sports: EFSMA Statement on ECG for Pre-Participation Examination. Dtsch. Z. Sportmed. 2015, 66, 151–155. [Google Scholar] [CrossRef]
- Dekker, J.; Buurman, B.M.; van der Leeden, M. Exercise in people with comorbidity or multimorbidity. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2019, 38, 822–830. [Google Scholar] [CrossRef]
- Reid, H.; Ridout, A.J.; Tomaz, S.A.; Kelly, P.; Jones, N. Benefits outweigh the risks: A consensus statement on the risks of physical activity for people living with long-term conditions. Br. J. Sports Med. 2021, 56, 427–438. [Google Scholar] [CrossRef]
- Sember, V.; Meh, K.; Sorić, M.; Starc, G.; Rocha, P.; Jurak, G. Validity and Reliability of International Physical Activity Questionnaires for Adults across EU Countries: Systematic Review and Meta Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7161. [Google Scholar] [CrossRef]
- The ARIC Investigators. The Atherosclerosis Risk in Communities (ARIC) Study: Design and objectives. Am. J. Epidemiol. 1989, 129, 687–702. [Google Scholar] [CrossRef]
- Rütten, A.; Pfeifer, K. National Recommendations for Physical Activity and Physical Activity Promotion; FAU University Press: Erlangen, Germany, 2016. [Google Scholar]
- Nieß, A.M.; Thiel, A. Körperliche Aktivität und Sport bei Typ-2-Diabetes [Physical Activity and Sports in Patients with Type 2 Diabetes]. Diabetologie 2017, 12, 112–126. [Google Scholar]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, 147–167. [Google Scholar] [CrossRef] [Green Version]
- Schmid, J.; Schorno, N.; Gut, V.; Sudeck, G.; Conzelmann, A. “What type of activity suits me?” Development and implementation of the Exercise and Sport Counselling Approach COMET. Zeitschr. Sportpsychol. 2020, 27, 127–138. [Google Scholar] [CrossRef]
- Schmid, J.; Gut, V.; Conzelmann, A.; Sudeck, G. Bernese motive and goal inventory in exercise and sport: Validation of an updated version of the questionnaire. PLoS ONE 2018, 13, e0193214. [Google Scholar] [CrossRef] [PubMed]
- Sudeck, G.; Höner, O.; Edel, K. Integration theoriegeleiteter edukativer Maßnahmen in die kardiologische Sport und Bewegungstherapie. Beweg. Gesundh. 2007, 22, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Pfeifer, K.; Sudeck, G.; Geidl, W.; Tallner, A. Bewegungsförderung und Sport in der Neurologie–Kompetenzorientierung und Nachhaltigkeit. Neurol. Rehabil. 2013, 19, 7–19. [Google Scholar]
- Geidl, W.; Hofmann, J.; Gohner, W.; Sudeck, G.; Pfeifer, K. Behaviour-orientated exercise therapy-initiating and maintaining a physically active lifestyle. Rehabilitation 2012, 51, 259–268. [Google Scholar] [CrossRef]
- Miller, W.R.; Rose, G.S. Toward a theory of motivational interviewing. Am. Psychol. 2009, 64, 527–537. [Google Scholar] [CrossRef]
- Carroll, J.K.; Fiscella, K.; Epstein, R.M.; Sanders, M.R.; Williams, G.C. A 5A’s communication intervention to promote physical activity in underserved populations. BMC Health Serv. Res. 2012, 12, 374. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Pontillo, A.; Di Palo, C.; Giugliano, G.; Masella, M.; Marfella, R.; Giugliano, D. Effect of weight loss and lifestyle changes on vascular inflammatory markers in obese women: A randomized trial. JAMA 2003, 289, 1799–1804. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K.L.; Dobson, F.; Hinman, R.S. Exercise in osteoarthritis: Moving from prescription to adherence. Best Pract. Res. Clin. Rheumatol. 2014, 28, 93–117. [Google Scholar] [CrossRef]
- Liu, D.; Yi, L.; Sheng, M.; Wang, G.; Zou, Y. The Efficacy of Tai Chi and Qigong Exercises on Blood Pressure and Blood Levels of Nitric Oxide and Endothelin-1 in Patients with Essential Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid. Based Complement. Altern. Med. 2020, 2020, 3267971. [Google Scholar] [CrossRef] [PubMed]




| Inclusion Criteria (Two or More of the Following Diagnoses and/or Risk Profiles) | ||
|---|---|---|
| Diagnosis | Risk profile | |
| Osteoarthrosis of hip and/or knee | According to the ACR criteria i | WOMAC > 15 (pain and function) |
| Diabetes mellitus Type 2 | HbA1c < 6.5% Fasting blood glucose < 126 mg/dL | German diabetes risk score ≥ 57 points |
| Cardiovascular disease | Including hypertension, coronary artery disease, arteriosclerosis, etc. | PROCAM-Score > 1.2 at risk (compared to gender and age group) |
| Overweight/Obesity | BMI ≥ 27–≤ 35 kg/m2 | |
| Exclusion criteria | ||
| Overall |
| |
| Osteoarthrosis | Appointment for elective joint replacement | |
| Baseline Data | |
|---|---|
| N (thereof female) | 39 (27) |
| Age (years) | |
| Mean ± SD | 55.2 ± 10.3 |
| Minimum (years) | 27 |
| Maximum (years) | 69 |
| Employed | 30 (77) |
| Retired | 8 (20) |
| In education | 1 (3) |
| Physician | 4 (10) |
| Medical assistant | 9 (23) |
| Craftsperson | 1 (3) |
| Freelancer | 3 (8) |
| Civil cervices employee | 9 (23) |
| Office employee | 10 (26) |
| Others | 3 (8) |
| BMI (Mean ± SD) | 31.1 ± 3.0 |
| Overweight/Obesity, n (%) | 38 (97) |
| thereof > 27 kg/m2 < 30 kg/m2 | 11 |
| thereof ≥ 30 kg/m2 | 24 |
| Cardiovascular disease (yes, n (%)/risk factor, n (%)) | 28 (72)/2 (5) |
| thereof arterial hypertension | 28/2 |
| thereof pharmacological treatment | 23 |
| Diabetes mellitus type 2 (yes, n (%)/risk factor, n (%)) | 4 (10)/27 (69) |
| Osteoarthritis (yes, n (%)/risk factor, n (%)) | 17 (43)/11 (28) |
| thereof hip osteoarthritis | 2/3 |
| thereof knee osteoarthritis | 15/8 |
| Physical exercise participation (minutes/week) | |
| Mean ± SD | 27.7 ± 94.3 |
| Median ± IQR | 0.0 ± 0.0 |
| Minimum/Maximum | 0.0/559.0 * |
| Study Visit | Rank Means i | RTE ii | p-Value |
|---|---|---|---|
| Baseline | 29.3 | 0.25 | |
| t3 (12-weeks post baseline) | 77.1 | 0.66 | <0.001 |
| t6 (24-weeks post baseline) | 70.6 | 0.60 | <0.001 |
| Study Visit | Mean (SE) | Mean Difference (95% CI) | p-Value | ES i | ||||
|---|---|---|---|---|---|---|---|---|
| Norm Values ii | Baseline | t3 | t6 | Time Points | ||||
| Physical Performance Measures | ||||||||
| Cardio-respiratory Outcomes | ||||||||
| Relative VO2peak (mL/kg/min) | ♀: 26.2 ♂: 32.8 | 20.0 (0.8) | 22.7 (0.9) | 22.0 (0.8) | t3-t0 | 2.6 (1.4 to 3.6) | <0.001 | 0.53 |
| t6-t0 | 2.0 (0.7 to 3.2) | 0.001 | 0.41 | |||||
| VO2peak (l/min) | n.a. | 1.8 (0.1) | 2.0 (0.1) | 2.0 (0.1) | t3-t0 | 0.2 (0.1 to 0.3) | 0.001 | 0.32 |
| t6-t0 | 0.1 (0.01 to 0.3) | 0.03 | 0.16 | |||||
| Muscular Strength Measures | ||||||||
| Maximum force: Extension (Nm) | n.a. | 114.5 (8.7) | 126.2 (9.1) | 132.6 (8.9) | t3-t0 | 11.7 (2.7 to 20.7) | 0.007 | 0.22 |
| t6-t0 | 18.1 (7.7 to 28.4) | <0.001 | 0.33 | |||||
| Maximum force: Flexion (Nm) | n.a. | 88.4 (6.5) | 91.5 (6.7) | 96.1 (6.6) | t3-t0 | 3.2 (−4.4 to 10.7) | 0.90 | |
| t6-t0 | 7.8 (−1.1 to 16.6) | 0.10 | ||||||
| Metabolic Measures (blood variables and anthropometrics) | ||||||||
| Total Cholesterol (mg/dL) | 130–190 | 217.6 (6.7) | 215.0 (7.7) | 210.5 (7.1) | t3-t0 | −2.7 (−17.7 to 12.3) | 1.00 | |
| t6-t0 | −7.1 (−22.4 to 8.2) | 0.75 | ||||||
| HDL-cholesterol (mg/dL) | ≥35 | 58.7 (2.1) | 59.9 (2.3) | 61.5 (2.2) | t3-t0 | 1.1 (−2.3 to 4.6) | 1.00 | |
| t6-t0 | 2.8 (−1.1 to 6.7) | 0.23 | ||||||
| LDL-cholesterol (mg/dL) | ≤160 | 148.2 (6.8) | 146.6 (7.5) | 141.4 (7.1) | t3-t0 | −1.6 (−14.6 to 11.5) | 1.00 | |
| t6-t0 | −6.8 (−20.5 to 7.0) | 0.68 | ||||||
| Triglycerides (mg/dL) | ≤200 | 125.8 (10.8) | 124.1 (11.7) | 120.5 (11.1) | t3-t0 | −1.7 (−19.8 to 16.4) | 1.00 | |
| t6-t0 | −5.2 (−23.0 to 12.5) | 1.00 | ||||||
| Fasting glucose (mg/dL) | 70–99 | 92.3 (1.8) | 91.3 (2.2) | 91.8 (1.9) | t3-t0 | −1.0 (−6.4 to 4.4) | 1.00 | |
| t6-t0 | −0.5 (−4.8 to 3.9) | 1.00 | ||||||
| HbA1c (%) | 4.5–6.2 | 5.7 (0.1) | 5.6 (0.1) | 5.7 (0.1) | t3-t0 | −0.1 (−0.2 to 0.1) | 0.80 | |
| t6-t0 | 0.04 (−0.02 to 0.1) | 0.32 | ||||||
| Body weight (kg) | n.a. | 90.8 (2.0) | 89.2 (2.0) | 89.3 (2.0) | t3-t0 | −1.6 (−3.3 to 0.02) | 0.05 | |
| t6-t0 | −1.6 (−3.6 to 0.5) | 0.18 | ||||||
| Health-related Quality of Life iii | ||||||||
| Physical Component Scale | 40.7 | 42.7 (1.9) | 44.3 (1.9) | 44.2 (1.9) | t3-t0 | 1.6 (−1.3 to 4.4) | 0.54 | |
| t6-t0 | 1.5 (−4.8 to 1.8) | 0.80 | ||||||
| Mental Component Scale | 53.1 | 47.0 (1.3) | 50.1 (1.3) | 46.3 (1.4) | t3-t0 | 3.1 (−0.4 to 6.6) | 0.10 | |
| t6-t0 | −0.7 (−4.6 to 3.2) | 1.00 | ||||||
| General Health | 64.4 | 44.6 (3.4) | 60.8 (3.5) | 58.0 (3.7) | t3-t0 | 16.2 (4.7 to 27.7) | 0.003 | 0.76 |
| t6-t0 | 13.4 (3.0 to 23.8) | 0.008 | 0.63 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schweda, S.; Munz, B.; Burgstahler, C.; Niess, A.M.; Roesel, I.; Sudeck, G.; Krauss, I. Proof of Concept of a 6-Month Person-Oriented Exercise Intervention ‘MultiPill-Exercise’ among Patients at Risk of or with Multiple Chronic Diseases: Results of a One-Group Pilot Trial. Int. J. Environ. Res. Public Health 2022, 19, 9469. https://doi.org/10.3390/ijerph19159469
Schweda S, Munz B, Burgstahler C, Niess AM, Roesel I, Sudeck G, Krauss I. Proof of Concept of a 6-Month Person-Oriented Exercise Intervention ‘MultiPill-Exercise’ among Patients at Risk of or with Multiple Chronic Diseases: Results of a One-Group Pilot Trial. International Journal of Environmental Research and Public Health. 2022; 19(15):9469. https://doi.org/10.3390/ijerph19159469
Chicago/Turabian StyleSchweda, Simone, Barbara Munz, Christof Burgstahler, Andreas Michael Niess, Inka Roesel, Gorden Sudeck, and Inga Krauss. 2022. "Proof of Concept of a 6-Month Person-Oriented Exercise Intervention ‘MultiPill-Exercise’ among Patients at Risk of or with Multiple Chronic Diseases: Results of a One-Group Pilot Trial" International Journal of Environmental Research and Public Health 19, no. 15: 9469. https://doi.org/10.3390/ijerph19159469
APA StyleSchweda, S., Munz, B., Burgstahler, C., Niess, A. M., Roesel, I., Sudeck, G., & Krauss, I. (2022). Proof of Concept of a 6-Month Person-Oriented Exercise Intervention ‘MultiPill-Exercise’ among Patients at Risk of or with Multiple Chronic Diseases: Results of a One-Group Pilot Trial. International Journal of Environmental Research and Public Health, 19(15), 9469. https://doi.org/10.3390/ijerph19159469