
Childbirth Satisfaction during the COVID-19 Pandemic in a Hospital in Southwestern Spain

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Sample
2.3. Measurement
- Sociodemographic variables: age, education level (no studies/primary; secondary studies; university/postgraduate studies), stable partner (yes/no) and employment status (student, unemployed, work for others, own-account work);
- Variables related to care or expectations of childbirth: accompaniment during childbirth and early postpartum(partner/other relative/no), the companion was the same chosen before birth (yes/no), number of professionals who provide care, number of professionals who perform vaginal exams, prenatal education (yes/no), type of feeding desired for the newborn (exclusive breastfeeding, partial breastfeeding, formula feeding), prepartum desire to use epidural analgesia (yes/no), perceived efficacy of the analgesia employed during childbirth (relieved/did not/partial relieved);
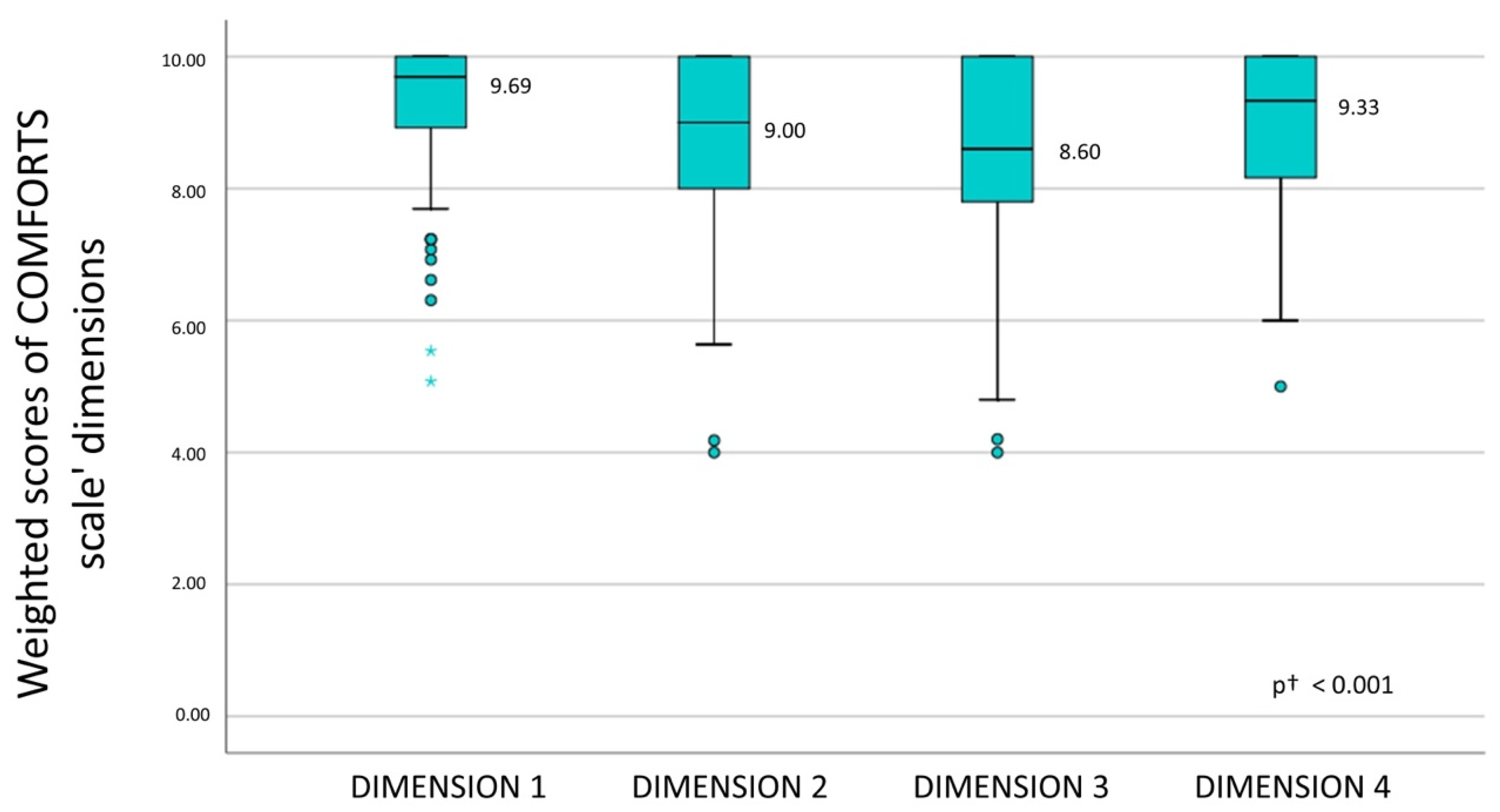
- Satisfaction with the care received during childbirth was measured by the COMFORTS scale [22], translated and validated into Spanish [23]. This scale consists of 40 items grouped into 4 dimensions: (1) Care during the childbirth period. This dimension includes 13 items. All the items included in this area provided information on the care provided to the puerperal woman and her partner or support person during the labour. (2) Postpartum care in the ward. This dimension includes 11 items that explore the care received during the postpartum period, the information and education received by nurses in relation to the care and feeding of the newborn. (3) New-born care. This area includes 10 items and explores woman’s confidence that nurses can meet the needs of her newborn. (4) Logistical aspects and respect for privacy. This dimension includes 6 items and explores satisfaction in relation to the environment (suitability, space, lighting), respect for privacy or quality of the food received; the scale is scored using a Likert scale with a maximum score of 200 points. This scale has good reliability (Cronbach’s alpha = 0.952). This scale categorizes the total degree of satisfaction during the birth process from calculating the total scale score and grouping this within the following ranges: very unsatisfied (40–71 points); unsatisfied (72–103 points); indifferent (104–135 points); satisfied (136–167 points); and very satisfied (168–200 points); and
- Data related to the process of childbirth and the early postpartum period: number of pregnancies, onset of labor (induced/spontaneous), duration of pregnancy (preterm/term/post term), parity (primiparous/multiparous), type of childbirth (eutocic, instrumental, caesarean section), use of epidural analgesia (yes/no), use of nonpharmacological analgesia (yes/no), perineal injury (intact, 1st degree tear, 2nd degree tear, 3rd degree tear, 4th degree tear, episiotomy), time of childbirth (day/night) and feeding of the newborn 48 h after birth (exclusive breastfeeding, partial breastfeeding, formula feeding).
2.4. Data Collection
2.5. Data Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valls Martínez, M.C.; Abad Segura, E. Patient satisfaction in the Spanish National Health System. An. Sist. Sanit. Navar. 2018, 41, 309–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caminal, J. Satisfaction measurement: A people participation instrument in the improvement of quality healthcare services. Rev. Calid. Asist. 2001, 16, 276–279. [Google Scholar] [CrossRef]
- Mas-Pons, R.; Barona-Vilar, C.; Carregui-Vila, S.; Ibañez-Gil, N.; Margaix-Fontestad, L.; Escribà-Agüi, V. Satisfacción de las mujeres con la experiencia del parto: Validación de la Mackey Satisfaction Childbirth Rating Scale. Gac. Sanit. 2012, 26, 236–242. [Google Scholar] [CrossRef] [Green Version]
- Aguilar Cordero, M.J.; Sáez Martín, I.; Menor Rodríguez, M.J.; Mur Villar, N.; Expósito Ruiz, M.; Hervás Pérez, A.; González Mendoza, J.L. Valoración del nivel de satisfacción en un grupo de mujeres de Granada sobre atención al parto, acompañamiento y duración de la lactancia. Nutr. Hosp. 2013, 28, 920–926. [Google Scholar] [CrossRef]
- Linder-Pelz, S. Toward a theory of patient satisfaction. Soc. Sci. Med. 1982, 16, 577–582. [Google Scholar] [CrossRef]
- Williams, B. Patient satisfaction: A valid concept? Soc. Sci. Med. 1994, 38, 509–516. [Google Scholar] [CrossRef]
- López-Mirones, M.; Alonso-Salcines, A.; Terán-Muñoz, O.; García-González, C.; Laurrieta-Saiz, I.; González-Maestro, M. Satisfacción materna en el área de partos según la Escala Mackey. Nubero Científica 2017, 3, 36–43. [Google Scholar]
- Ponce Capitán, M.Á. Conocimientos de las puerperas sobre autocuidados y cuidados del recien nacido en el momento del alta hospitalaria. Matronas Prof. 2005, 6, 14–19. [Google Scholar]
- Crowther, S.; Smythe, L.; Spence, D. Mood and birth experience. Women Birth 2014, 27, 21–25. [Google Scholar] [CrossRef]
- Lundgren, I. Swedish women’s experience of childbirth 2 years after birth. Midwifery 2005, 21, 346–354. [Google Scholar] [CrossRef]
- Bell, A.F.; Andersson, E. The birth experience and women’s postnatal depression: A systematic review. Midwifery 2016, 39, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Fortis, A.S.; Fortis, C.S.; Cano, M.D.P. Satisfacción de las mujeres con la atención al parto. Matronas Hoy 2018, 06, 6. [Google Scholar]
- Mattison, C.A.; Dion, M.L.; Lavis, J.N.; Hutton, E.K.; Wilson, M.G. Midwifery and obstetrics: Factors influencing mothers’ satisfaction with the birth experience. Birth 2018, 45, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Donate-Manzanares, M.; Rodríguez-Cano, T.; Gómez-Salgado, J.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Barrilero-Fernández, E.; Beato-Fernández, L. Quality of Childbirth Care in Women Undergoing Labour: Satisfaction with Care Received and How It Changes over Time. J. Clin. Med. 2019, 8, 434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-de la Torre, H.; Miñarro-Jiménez, S.; Palma-Arjona, I.; Jeppesen-Gutierrez, J.; Berenguer-Pérez, M.; Verdú-Soriano, J. Perceived satisfaction of women during labour at the Hospital Universitario Materno-Infantil of the Canary Islands through the Childbirth Experience Questionnaire (CEQ-E). Enferm. Clin. 2021, 31, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Zeyneloğlu, S.; Kısa, S.; Özberk, H.; Badem, A. Predictors and measurement of satisfaction with postpartum care in a government hospital. Nurs. Health Sci. 2017, 19, 198–203. [Google Scholar] [CrossRef] [Green Version]
- Overgaard, C.; Fenger-Grøn, M.; Sandall, J. The impact of birthplace on women’s birth experiences and perceptions of care. Soc. Sci. Med. 2012, 74, 973–981. [Google Scholar] [CrossRef]
- Arnau Sánchez, J.; Martínez Roche, M.E.; Nicolás Vigueras, M.D.; Bas Peña, E.; Morales López, R.; Álvarez Muñarriz, L. Los conceptos de parto normal, natural y humanizado. El caso del área 1 de salud de la región de Murcia. Rev. Antropol. Iberoam. 2012, 7, 225–247. [Google Scholar]
- Ministerio de Sanidad Ministerio de Sanidad—Profesionales—Enfermedad por nuevo Coronavirus, COVID-19. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/ (accessed on 8 June 2022).
- Janevic, T.; Maru, S.; Nowlin, S.; McCarthy, K.; Bergink, V.; Stone, J.; Dias, J.; Wu, S.; Howell, E.A. Pandemic Birthing: Childbirth Satisfaction, Perceived Health Care Bias, and Postpartum Health During the COVID-19 Pandemic. Matern. Child Health J. 2021, 25, 860–869. [Google Scholar] [CrossRef]
- World Medical Association World Medical Association Declaration of HelsinkiEthical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [Green Version]
- Janssen, P.A.; Dennis, C.-L.; Reime, B. Development and psychometric testing of the care in obstetrics: Measure for testing satisfaction (COMFORTS) scale. Res. Nurs. Health 2006, 29, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Vivanco Montes, M.; Solís Muñoz, M.; Magdaleno del Rey, G.; Rodríguez Ferrer, R.; Álvarez Plaza, C.; Millán Santos, I.; Alonso Durán, M.; Feijoo Iglesias, M. Adaptación cultural y validación al español de la escala COMFORTS de satisfacción de las mujeres con los cuidados en el parto y puerperio. Metas Enferm. 2012, 15, 18–26. [Google Scholar]
- Coxon, K.; Turienzo, C.F.; Kweekel, L.; Goodarzi, B.; Brigante, L.; Simon, A.; Lanau, M.M. The impact of the coronavirus (COVID-19) pandemic on maternity care in Europe. Midwifery 2020, 88, 102779. [Google Scholar] [CrossRef] [PubMed]
- Vila-Candel, R.; González-Chordá, V.M.; Soriano-Vidal, F.J.; Castro-Sánchez, E.; Rodríguez-Blanco, N.; Gómez-Seguí, A.; Andreu-Pejó, L.; Martínez-Porcar, C.; Gonzálvez, C.R.; Torrent-Ramos, P.; et al. Obstetric–Neonatal Care during Birth and Postpartum in Symptomatic and Asymptomatic Women Infected with SARS-CoV-2: A Retrospective Multicenter Study. Int. J. Environ. Res. Public Health 2022, 19, 5482. [Google Scholar] [CrossRef] [PubMed]
- Instituto San Carlos III COVID-19. Informes Previos. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Paginas/-COVID-19.-Informes-previos.aspx (accessed on 8 June 2022).
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. The impacts of the COVID-19 pandemic on birth satisfaction in a prospective cohort of 2,341 U.S. women. Women Birth 2021. [CrossRef]
- Mariño-Narvaez, C.; Puertas-Gonzalez, J.A.; Romero-Gonzalez, B.; Peralta-Ramirez, M.I. Giving birth during the COVID-19 pandemic: The impact on birth satisfaction and postpartum depression. Int. J. Gynaecol. Obstet. 2021, 153, 83–88. [Google Scholar] [CrossRef]
- Arrebola, R.N.; Mahía, L.P.; López, S.B.; Castiñeira, N.L.; Pillado, T.S.; Díaz, S.P. Women’s satisfaction with childbirth and postpartum care and associated variables. Rev. Esc. Enferm. USP 2021, 55, 1–7. [Google Scholar] [CrossRef]
- Soriano-Vidal, F.J.; Oliver-Roig, A.; Cabrero-García, J.; Congost-Maestre, N.; Dencker, A.; Richart-Martínez, M. The Spanish version of the Childbirth Experience Questionnaire (CEQ-E): Reliability and validity assessment. BMC Pregnancy Childbirth 2016, 16, 372. [Google Scholar] [CrossRef] [Green Version]
- Kempe, P.; Vikström-Bolin, M. Women’s satisfaction with the birthing experience in relation to duration of labour, obstetric interventions and mode of birth. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 156–159. [Google Scholar] [CrossRef]
- Ziabakhsh, S.; Fernandez, R.; Black, B.; Brito, G. Voices of Postpartum Women: Exploring Canadian Women’s Experiences of Inpatient Postpartum Care. J. Obstet. Gynaecol. Can. 2018, 40, 1424–1436. [Google Scholar] [CrossRef]


{kind=link}
| Variables | N = 116 |
|---|---|
| Age(SD) | 32.08 (4.68) |
| Country of origin n (%) | |
| Spain | 109 (94.0) |
| Other | 7 (6.0) |
| Education n (%) | |
| No studies/primary | 40 (34.5) |
| Secondary | 53 (45.7) |
| University/postgraduate | 23 (19.8) |
| Employment situation n (%) | |
| Student | 2 (1.7) |
| Unemployed | 41 (35.3) |
| Work for others | 65 (56.0) |
| Own-account work | 8 (6.9) |
| Stable partner n (%) | 116 (100.0) |
| Variables | N = 116 |
|---|---|
| Gravidity n (%) | |
| Primigravida | 43 (37.1) |
| Multigravida | 73 (62.9) |
| Parity (n%) | |
| Primiparous | 52 (44.8) |
| Multiparous | 64 (55.2) |
| Planned epidural analgesia before childbirth | 85 (73.3) |
| Maternal Education n (%) | |
| Yes | 46 (39.7) |
| No | 70 (60.3) |
| Onset of labor n (%) | |
| Induced | 44 (37.9) |
| Spontaneous | 72 (62.1) |
| Duration of pregnancy, n (%) | |
| Preterm | 5 (4.3) |
| Term | 67 (57. 8) |
| Post term | 44 (37.9) |
| Duration of dilation, (minutes) Median (IQR) | 170 (67.50–266.25) |
| Duration of expulsive efforts, (minutes) Median (IQR) | 52.50 (20–110) |
| Type of childbirth, n (%) | |
| Eutocic | 78 (67.2) |
| Instrumental | 14 (12.1) |
| Caesarean section | 24 (20.7) |
| Number of professionals who provided care, n (%) | |
| 1–2 | 37 (31.9) |
| 3–5 | 67 (57.8) |
| >5 | 26 (10.4) |
| Number of professionals who performed vaginal examination, n (%) | |
| 0–2 | 63 (54.3) |
| 3–5 | 52 (44.8) |
| >5 | 1 (0.9) |
| Perineal injury, n (%) | |
| No perineal trauma | 41 (35.3) |
| First degree tear | 24 (20.7) |
| Second degree tear | 33 (28.4) |
| Episiotomy | 18 (15.5) |
| Time of birth, n (%) | |
| Day | 50 (43.1) |
| Night | 66 (56.9) |
| Labor Companion, n (%) | |
| Partner | 103 (88.8) |
| Other relative | 4 (3.4) |
| Nobody | 9 (7.8) |
| The companion was chosen prior to childbirth, n (%) | 104 (89.7) |
| Use of epidural analgesia during childbirth, n (%) | 87 (75) |
| Epidural effectiveness (n = 87), n (%) | |
| Relieved | 61 (70.1) |
| Did not relieve | 2 (2.3) |
| Partial relief, use of bolus | 24 (27.6) |
| Epidural used as planned, n (%) | |
| Used as planned | 69 (59.5) |
| Did not use as planned | 13 (11.2) |
| Used without initial plan | 18 (15.5) |
| Did not use, planned do it | 16 (13.8) |
| Use of nonpharmacological pain relief methods, n (%) | 17 (14.7) |
| Variable | Median (IQR) | p |
|---|---|---|
| Education level | ||
| No education/primary (n = 40) | 184 (174–198) | 0.163 1 |
| Secondary education (n = 53) | 193 (157.5–199) | |
| Higher education (n = 23) | 179 (162–187) | |
| Gravidity | ||
| Primigravida (n = 43) | 179 (195–157) | 0.158 2 |
| Multigravida (n = 73) | 185 (199–167) | |
| Parity | ||
| Primiparous (n = 52) | 174 (193–155.5) | 0.003 2 |
| Multiparous (n = 64) | 187 (199–173) | |
| Maternal education | ||
| Yes (n = 46) | 185 (196–158.5) | 0.861 2 |
| No (n = 70) | 180.5 (199–166.8) | |
| Onset of labor | ||
| Induced (n = 44) | 179.5 (160–196.8) | 0.648 2 |
| Spontaneous (n = 72) | 183.5 (165.8–196) | |
| Duration of pregnancy | ||
| Preterm (n = 5) | 187 (164–198) | 0.556 1 |
| Term (n = 67) | 179 (172–190) | |
| Post term (n = 44) | 179.5 (160.5–195.5) | |
| Type of chilbirth | ||
| Eutocic (n = 78) | 182.5 (168.8–196.5) | 0.090 1 |
| Instrumental (n = 14) | 191.5 (176.8–200) | |
| Caesarian section (n = 24) | 171.5 (157–193.5) | |
| Number of professionals providing care | ||
| 1–2 (n = 37) | 182 (169.5–199) | 0.703 1 |
| 3–5 (n = 67) | 180 (159–196) | |
| >5 (n = 26) | 184.50 (174–196) | |
| Number of professionals who performed a vaginal examination | ||
| 0–2 (n = 63) | 182 (162–199) | 0.338 1 |
| 3–5 (n = 52) | 181.5 (167.3–196) | |
| >5 (n = 1) | 200 (200–200) | |
| Perineal injury | ||
| No perineal trauma (n = 41) | 179 (160–196) | 0.337 1 |
| First degree tear (n = 24) | 191 (179.5–199.8) | |
| Second degree tear (n = 33) | 183 (160.5–198) | |
| Episiotomy (n = 18) | 176.5 (151–190) | |
| Labor companion | ||
| Partner (n = 103) | 183 (162–196) | 0.269 1 |
| Other relative (n = 4) | 172.5 (168.5–178) | |
| Nobody (n = 9) | 196 (168.5–199.5) | |
| The companion was chosen prior to childbirth | ||
| Yes (n = 104) | 182.50 (162.5–196) | 0.293 2 |
| No (n = 12) | 170 (168–170) | |
| Time of birth | ||
| Day (n = 50) | 185.50 (165.8–198.3) | 0.254 2 |
| Night (n = 66) | 179.50 (161.5–196) | |
| Use of epidural analgesia | ||
| Yes (n = 87) | 183 (164–196) | 0.830 2 |
| No (n = 29) | 182 (165–197) | |
| Epidural effectiveness | ||
| Relieved (n = 61) | 183 (163–196) | 0.619 1 |
| Did not relieve (n = 2) | 169 (153–169) | |
| Partial relief, use of bolus (n = 24) | 179.5 (166.5–199.8) | |
| Epidural use as planned | ||
| Used as planned (n = 69) | 186 (169.5–198) | 0.020 1 |
| Did not use as planned (n = 13) | 172 (157–185) | |
| Used without initial plan (n = 18) | 173.5 (187.50–146.3) | |
| Did not use, planned do it (n = 16) | 188 (172.5–199.8) | |
| Use of nonpharmacological analgesic methods | ||
| Yes (n = 17) | 179 (162–195.5) | 0.769 2 |
| No (n = 99) | 183 (165–196) | |
| Companion on the hospital ward during the postpartum period | ||
| Partner (n = 111) | 182 (162–196) | 0.035 1 |
| Other relative (n = 2) | 177 (175–177) | |
| Nobody (n = 3) | 200 (200–200) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Morcillo, M.; Tiburcio-Palos, E.; Cordovilla-Guardia, S.; Santano-Mogena, E.; Franco-Antonio, C. Childbirth Satisfaction during the COVID-19 Pandemic in a Hospital in Southwestern Spain. Int. J. Environ. Res. Public Health 2022, 19, 9636. https://doi.org/10.3390/ijerph19159636
González-Morcillo M, Tiburcio-Palos E, Cordovilla-Guardia S, Santano-Mogena E, Franco-Antonio C. Childbirth Satisfaction during the COVID-19 Pandemic in a Hospital in Southwestern Spain. International Journal of Environmental Research and Public Health. 2022; 19(15):9636. https://doi.org/10.3390/ijerph19159636
Chicago/Turabian StyleGonzález-Morcillo, María, Esther Tiburcio-Palos, Sergio Cordovilla-Guardia, Esperanza Santano-Mogena, and Cristina Franco-Antonio. 2022. "Childbirth Satisfaction during the COVID-19 Pandemic in a Hospital in Southwestern Spain" International Journal of Environmental Research and Public Health 19, no. 15: 9636. https://doi.org/10.3390/ijerph19159636
APA StyleGonzález-Morcillo, M., Tiburcio-Palos, E., Cordovilla-Guardia, S., Santano-Mogena, E., & Franco-Antonio, C. (2022). Childbirth Satisfaction during the COVID-19 Pandemic in a Hospital in Southwestern Spain. International Journal of Environmental Research and Public Health, 19(15), 9636. https://doi.org/10.3390/ijerph19159636