
Hospitalization Costs of Respiratory Diseases Attributable to Temperature in Australia and Projections for Future Costs in the 2030s and 2050s under Climate Change

 ,
,  ,
,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Data Sources
2.2.1. Hospitalisation Cost Data
2.2.2. Meteorological Data
2.3. Statistical Analyses
2.3.1. First Stage
2.3.2. Second Stage
3. Results
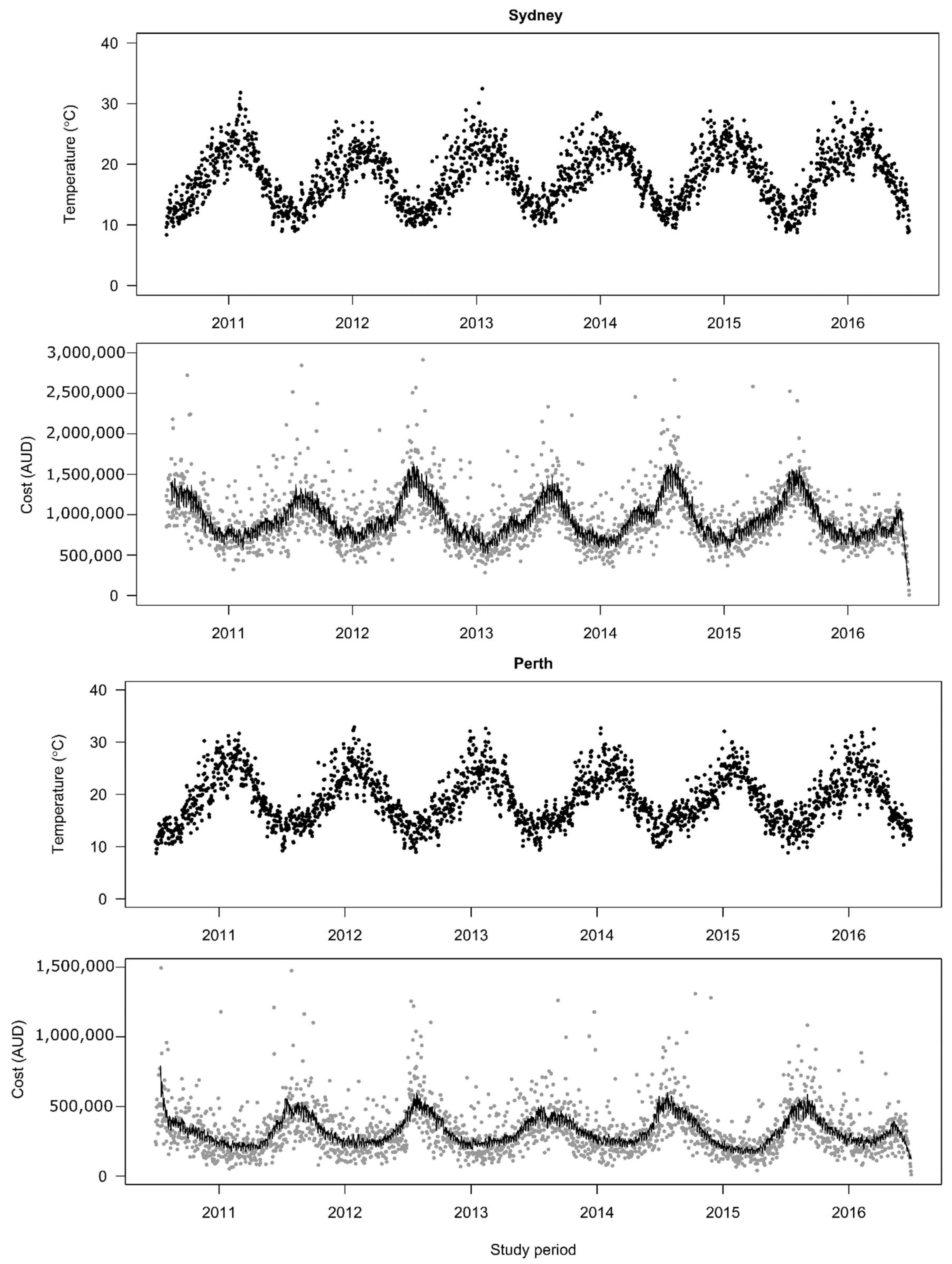
3.1. Descriptive Results of Daily Temperatures and Hospitalization Costs
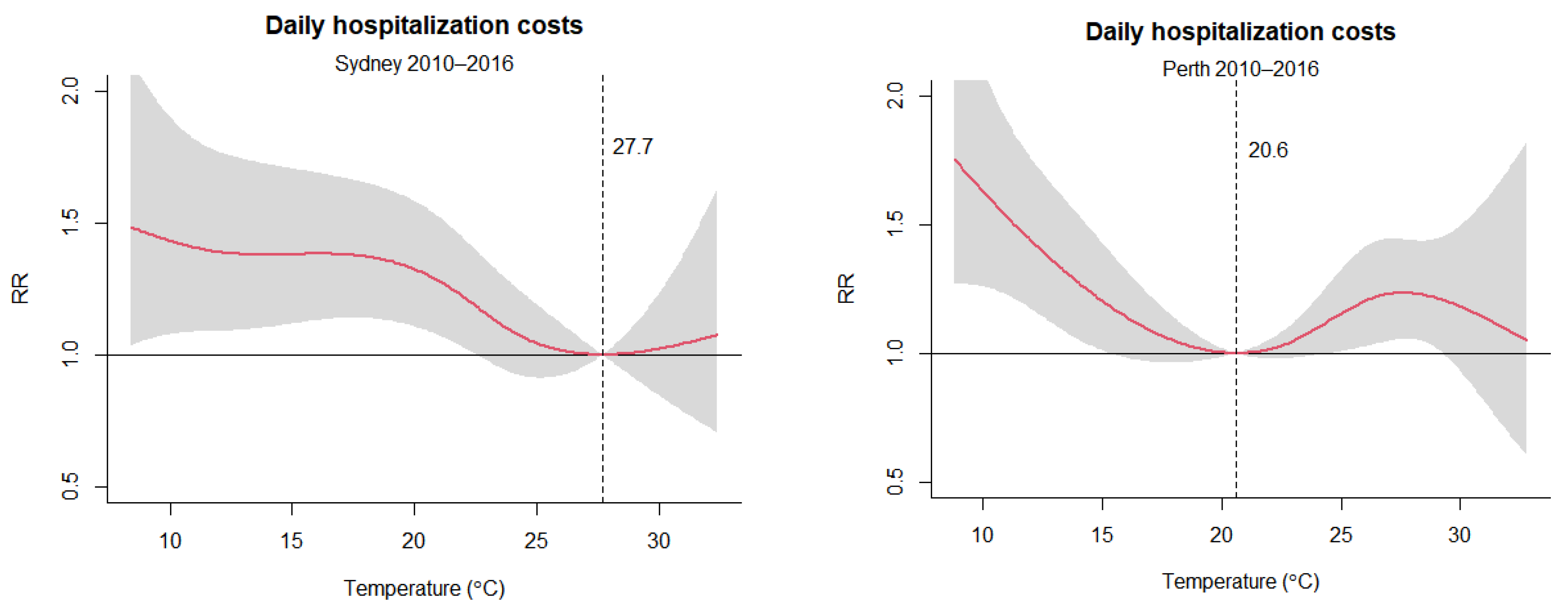
3.2. Exposure–Response Relationship between Daily Mean Temperatures and Hospitalization Costs
3.3. The Effects of Current and Future Temperature Increase on Hospitalization Costs for Respiratory Diseases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schurer, A.P.; Mann, M.E.; Hawkins, E.; Tett, S.F.B.; Hegerl, G.C. Importance of the Pre-Industrial Baseline in Determining the Likelihood of Exceeding the Paris Limits. Nat. Clim. Change 2017, 7, 563–567. [Google Scholar] [CrossRef]
- Hawkins, E.; Ortega, P.; Suckling, E.; Schurer, A.; Hegerl, G.; Jones, P.; Joshi, M.; Osborn, T.J.; Masson-Delmotte, V.; Mignot, J.; et al. Estimating Changes in Global Temperature since the Preindustrial Period. Bull. Am. Meteorol. Soc. 2017, 98, 1841–1856. [Google Scholar] [CrossRef]
- Zhang, Y.; Beggs, P.J.; Bambrick, H.; Berry, H.L.; Linnenluecke, M.K.; Trueck, S.; Alders, R.; Bi, P.; Boylan, S.M.; Green, D.; et al. The MJA–Lancet Countdown on health and climate change: Australian policy inaction threatens lives. Med. J. Aust. 2018, 209, 474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, A.; Abbas, M.; Allen, A.; Ball, S.; Bell, S.; Bellamy, R.; Friel, S.; Groce, N.; Johnson, A.; Kett, M.; et al. Managing the health effects of climate change: Lancet and University College London Institute for Global Health Commission. Lancet 2009, 373, 1693–1733. [Google Scholar] [CrossRef]
- Butler, C.D. Climate Change, Health and Existential Risks to Civilization: A Comprehensive Review (1989–2013). Int. J. Environ. Res. Public Health 2018, 15, 2266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, X.; Wolff, R.; Yu, W.; Vaneckova, P.; Pan, X.; Tong, S. Ambient Temperature and Morbidity: A Review of Epidemiological Evidence. Environ. Health Perspect. 2012, 120, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, R.; Samet, J.M. Relation between Elevated Ambient Temperature and Mortality: A Review of the Epidemiologic Evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Nitschke, M.; Weinstein, P.; Pisaniello, D.L.; Parton, K.A.; Bi, P. The impact of summer temperatures and heatwaves on mortality and morbidity in Perth, Australia 1994–2008. Environ. Int. 2012, 40, 33–38. [Google Scholar] [CrossRef]
- Borg, M.; Bi, P.; Nitschke, M.; Williams, S.; McDonald, S. The impact of daily temperature on renal disease incidence: An ecological study. Environ. Health 2017, 16, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Xiang, J.; Hansen, A.; Liu, Q.; Liu, X.; Tong, M.X.; Sun, Y.; Cameron, S.; Hanson-Easey, S.; Han, G.-S.; Williams, C.; et al. Association between dengue fever incidence and meteorological factors in Guangzhou, China, 2005–2014. Environ. Res. 2017, 153, 17–26. [Google Scholar] [CrossRef]
- Xiang, J.; Hansen, A.; Liu, Q.; Tong, M.X.; Liu, X.; Sun, Y.; Cameron, S.; Hanson-Easey, S.; Han, G.S.; Williams, C.; et al. Association between malaria incidence and meteorological factors: A multi-location study in China, 2005–2012. Epidemiology Infect. 2017, 146, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Xiang, J.; Hansen, A.; Liu, Q.; Tong, M.X.; Liu, X.; Sun, Y.; Cameron, S.; Hanson-Easey, S.; Han, G.-S.; Williams, C.; et al. Impact of meteorological factors on hemorrhagic fever with renal syndrome in 19 cities in China, 2005–2014. Sci. Total Environ. 2018, 636, 1249–1256. [Google Scholar] [CrossRef]
- Bi, P.; Tong, S.L.; Donald, K.; Parton, K.; Hobbs, J. Climate variability and the transmission of Ross River virus infection in the coastal region of Queensland, Australia. Epidemiology 2000, 11, S64. [Google Scholar]
- Watts, N.; Amann, M.; Ayeb-Karlsson, S.; Belesova, K.; Bouley, T.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Chambers, J.; et al. The Lancet Countdown on health and climate change: From 25 years of inaction to a global transformation for public health. Lancet 2017, 391, 581–630. [Google Scholar] [CrossRef]
- Kim, K.-H.; Kabir, E.; Jahan, S.A. A Review of the Consequences of Global Climate Change on Human Health. J. Environ. Sci. Health Part C 2014, 32, 299–318. [Google Scholar] [CrossRef]
- Eccles, R.; Wilkinson, J.E. Exposure to cold and acute upper respiratory tract infection. Rhinology 2015, 53, 99–106. [Google Scholar] [CrossRef]
- Mäkinen, T.M.; Juvonen, R.; Jokelainen, J.; Harju, T.H.; Peitso, A.; Bloigu, A.; Silvennoinen-Kassinen, S.; Leinonen, M.; Hassi, J. Cold temperature and low humidity are associated with increased occurrence of respiratory tract infections. Respir. Med. 2009, 103, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Ma, W.; Xu, X.; Peng, L.; Kan, H. Impact of extreme temperature on hospital admission in Shanghai, China. Sci. Total Environ. 2011, 409, 3634–3637. [Google Scholar] [CrossRef]
- Xu, Z.; Hu, W.; Su, H.; Turner, L.; Ye, X.; Wang, J.; Tong, S. Extreme temperatures and paediatric emergency department admissions. J. Epidemiol. Community Health 2014, 68, 304–311. [Google Scholar] [CrossRef] [Green Version]
- Tong, M.; Wondmagegn, B.Y.; Xiang, J.; Williams, S.; Hansen, A.; Dear, K.; Pisaniello, D.; Varghese, B.M.; Xiao, J.; Jian, L.; et al. Heat-attributable hospitalisation costs in Sydney: Current estimations and future projections in the context of climate change. Urban Clim. 2021, 40, 101028. [Google Scholar] [CrossRef]
- Tong, M.X.; Wondmagegn, B.Y.; Williams, S.; Hansen, A.; Dear, K.; Pisaniello, D.; Xiang, J.; Xiao, J.; Jian, L.; Scalley, B.; et al. Hospital healthcare costs attributable to heat and future estimations in the context of climate change in Perth, Western Australia. Adv. Clim. Chang. Res. 2021, 12, 638–648. [Google Scholar] [CrossRef]
- Wondmagegn, B.Y.; Xiang, J.; Dear, K.; Williams, S.; Hansen, A.; Pisaniello, D.; Nitschke, M.; Nairn, J.; Scalley, B.; Xiao, A.; et al. Increasing impacts of temperature on hospital admissions, length of stay, and related healthcare costs in the context of climate change in Adelaide, South Australia. Sci. Total Environ. 2021, 773, 145656. [Google Scholar] [CrossRef] [PubMed]
- Tong, M.X.; Wondmagegn, B.Y.; Xiang, J.; Williams, S.; Hansen, A.; Dear, K.; Pisaniello, D.; Xiao, J.; Jian, L.; Scalley, B.; et al. Emergency department visits and associated healthcare costs attributable to increasing temperature in the context of climate change in Perth, Western Australia, 2012–2019. Environ. Res. Lett. 2021, 16, 065011. [Google Scholar] [CrossRef]
- Toloo, G.S.; Hu, W.; FitzGerald, G.; Aitken, P.; Tong, S. Projecting excess emergency department visits and associated costs in Brisbane, Australia, under population growth and climate change scenarios. Sci. Rep. 2015, 5, 12860. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.; Luo, M.; Walker, R.J.; Liu, X.; Hwang, S.-A.; Chinery, R. Extreme high temperatures and hospital admissions for respiratory and cardiovascular diseases. Epidemiology 2009, 20, 738–746. [Google Scholar] [CrossRef]
- Michelozzi, P.; Accetta, G.; De Sario, M.; D’Ippoliti, D.; Marino, C.; Baccini, M.; Biggeri, A.; Anderson, H.R.; Katsouyanni, K.; Ballester, F.; et al. High Temperature and Hospitalizations for Cardiovascular and Respiratory Causes in 12 European Cities. Am. J. Respir. Crit. Care Med. 2009, 179, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Guo, Y.; Wang, C.; Li, W.; Lu, J.; Shen, S.; Xia, H.; He, J.; Qiu, X. Association between temperature change and outpatient visits for respiratory tract infections among children in Guangzhou, China. Int. J. Environ. Res. Public. Health 2015, 12, 439–454. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.-K.; Chang, C.-K.; Chang, S.-C.; Chen, P.-S.; Lin, C.; Wang, Y.-C. Temperature, nitrogen dioxide, circulating respiratory viruses and acute upper respiratory infections among children in Taipei, Taiwan: A population-based study. Environ. Res. 2013, 120, 109–118. [Google Scholar] [CrossRef]
- Wondmagegn, B.Y.; Xiang, J.; Williams, S.; Pisaniello, D.; Bi, P. What do we know about the healthcare costs of extreme heat exposure? A comprehensive literature review. Sci. Total Environ. 2019, 657, 608–618. [Google Scholar] [CrossRef]
- Australian Government Department of Health. The Australian Health System. Available online: https://www.health.gov.au/about-us/the-australian-health-system (accessed on 6 May 2019).
- CSIRO and Bureau of Meteorology. Climate Change in Australia. Projections for Australia′s NRM Regions. Available online: https://www.climatechangeinaustralia.gov.au/media/ccia/2.2/cms_page_media/168/CCIA_2015_NRM_TechnicalReport_WEB.pdf (accessed on 5 August 2015).
- Chen, D.; Chen, H.W. Using the Köppen classification to quantify climate variation and change: An example for 1901–2010. Environ. Dev. 2013, 6, 69–79. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Population Projections, Australia. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3222.02017%20(base)%20-%202066?OpenDocument (accessed on 10 June 2018).
- Australian Bureau of Statistics. Regional Population. Available online: https://www.abs.gov.au/statistics/people/population/regional-population/latest-release (accessed on 25 April 2021).
- Commonwealth Scientific and Industrial Research Organisation. Climate Futures Exploration Tool. Available online: https://www.climatechangeinaustralia.gov.au/en/projections-tools/climate-futures-tool/detailed-projections/ (accessed on 11 June 2018).
- Newbury, J. Linear Interpolation. In Basic Numeracy Skills and Practice; Macmillan Education UK: London, UK, 1981; pp. 67–72. [Google Scholar]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A. Statistical Methods in Studies on Temperature-Health Associations. Ph.D. Thesis, London School of Hygiene and Tropical Medicine (University of London), London, UK, 2011. [Google Scholar]
- Gasparrini, A.; Leone, M. Attributable risk from distributed lag models. BMC Med. Res. Methodol. 2014, 14, 55. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Gasparrini, A. Modeling exposure–lag–response associations with distributed lag non-linear models. Stat. Med. 2014, 33, 881–899. [Google Scholar] [CrossRef] [Green Version]
- Bai, L.; Woodward, A.; Chen, B.; Liu, Q. Temperature, hospital admissions and emergency room visits in Lhasa, Tibet: A time-series analysis. Sci. Total Environ. 2014, 490, 838–848. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. Consumer Price Index, Australia. Available online: https://www.abs.gov.au/statistics/economy/price-indexes-and-inflation/consumer-price-index-australia/latest-release (accessed on 30 September 2020).
- Vicedo-Cabrera, A.M.; Sera, F.; Gasparrini, A. Hands-on tutorial on a modeling framework for projections of climate change impacts on health. Epidemiology 2019, 30, 321–329. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Australian Bureau of Statistics. Migration, Australia. Available online: https://www.abs.gov.au/statistics/people/population/migration-australia/latest-release (accessed on 5 May 2021).
- Department of Industry Science Energy and Resources. Status of Air Conditioners in Australia. Available online: https://www.energyrating.gov.au/sites/default/files/documents/200509-ac-aust_0.pdf (accessed on 5 May 2006).
- Nicholls, L.; McCann, H.; Strengers, Y.; Bosomworth, K. Homes & Health Why Household Vulnerability to Extreme Heat is an Electricity Policy Issue. Available online: https://cur.org.au/cms/wp-content/uploads/2017/11/heatwaves-homes-and-health-rmit_full-report.pdf (accessed on 5 May 2017).
- Buckley, J.P.; Richardson, D.B. Seasonal modification of the association between temperature and adult emergency department visits for asthma: A case-crossover study. Environ. Health 2012, 11, 55. [Google Scholar] [CrossRef] [Green Version]
- Turner, L.R.; Connell, D.; Tong, S. Exposure to hot and cold temperatures and ambulance attendances in Brisbane, Australia: A time-series study. BMJ Open 2012, 2, e001074. [Google Scholar] [CrossRef] [Green Version]
- Analitis, A.; Katsouyanni, K.; Biggeri, A.; Baccini, M.; Forsberg, B.; Bisanti, L.; Kirchmayer, U.; Ballester, F.; Cadum, E.; Goodman, P.; et al. Effects of Cold Weather on Mortality: Results from 15 European Cities Within the PHEWE Project. Am. J. Epidemiol. 2008, 168, 1397–1408. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.; Zhao, Y.; Li, S.; Zhang, Y.; Wang, Q.; Zhang, H.; Qiao, H.; Li, W.; Huxley, R.; Williams, G.; et al. Impact of ambient temperature on clinical visits for cardio-respiratory diseases in rural villages in northwest China. Sci. Total Environ. 2018, 612, 379–385. [Google Scholar] [CrossRef]
- Australian Bureau of Meteorology. Climate Statistics for Australian Locations Sydney. Available online: http://www.bom.gov.au/climate/averages/tables/cw_066062.shtml (accessed on 1 May 2022).
- Australian Bureau of Meteorology. Climate Statistics for Australian Locations Perth. Available online: http://www.bom.gov.au/climate/averages/tables/cw_009225.shtml (accessed on 1 May 2022).
- Patz, J.A.; Campbell-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef]
- Mourtzoukou, E.G.; Falagas, M.E. Exposure to cold and respiratory tract infections. Int. J. Tuberc. Lung Dis. 2007, 11, 938–943. [Google Scholar]
- Eccles, R. An explanation for the seasonality of acute upper respiratory tract viral infections. Acta Otolaryngol. 2002, 122, 183–191. [Google Scholar] [CrossRef]
- Johnson, C.; Eccles, R. Acute cooling of the feet and the onset of common cold symptoms. Fam. Pract. 2005, 22, 608–613. [Google Scholar] [CrossRef] [Green Version]
- Lowen, A.C.; Mubareka, S.; Steel, J.; Palese, P. Influenza virus transmission is dependent on relative humidity and temperature. PLoS Pathog. 2007, 3, 1470–1476. [Google Scholar] [CrossRef]
- Barregard, L.; Sallsten, G.; Andersson, L.; Almstrand, A.-C.; Gustafson, P.; Olin, A.-C. Experimental exposure to wood smoke: Effects on airway inflammation and oxidative stress. Occup. Environ. Med. 2008, 65, 319–324. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Older Australia at a Glance. Available online: https://www.aihw.gov.au/reports/older-people/older-australia-at-a-glance/contents/demographics-of-older-australians/australia-s-changing-age-and-gender-profile (accessed on 15 August 2021).
- Anderson, G.B.; Dominici, F.; Wang, Y.; McCormack, M.C.; Bell, M.L.; Peng, R.D. Heat-related emergency hospitalizations for respiratory diseases in the Medicare population. Am. J. Respir. Crit. Care Med. 2013, 187, 1098–1103. [Google Scholar] [CrossRef] [Green Version]
- Nairn, J.; Beaty, M.; Varghese, B.M. Australia′s black summer heatwave impacts. Aust. J. Emerg. Manag. 2021, 36, 17–20. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Sydney | Perth |
|---|---|---|
| Daily mean temperature °C (SD) | 18.1 (4.7) | 18.9 (5.0) |
| Hospitalization costs | AUD 2080.3 million | AUD 709.3 million |
| Observation days | 2192 | 2192 |
| Population | 5.5 million | 2.1 million |
| Population median age | 36.3 years | 37.1 years |
| Climate | Temperate climate | Mediterranean climate |
| Sydney | Perth | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Period | Costs (Million AUD) | Overall (95% CI) | Cold (95% CI) | Heat (95% CI) | Costs (Million AUD) | Overall (95% CI) | Cold (95% CI) | Heat (95% CI) | |
| 2010s | |||||||||
| Baseline | 493.2 | 23.71 (8.39; 34.96) | 23.69 (8.28; 34.99) | 0.02 (−0.08; 0.11) | 98.0 | 13.82 (5.95; 20.90) | 11.20 (2.93; 18.67) | 2.64 (0.65; 4.72) | |
| 2030s | |||||||||
| RCP2.6 | 623.8 | 20.26 (6.02; 30.73) | 20.24 (5.84; 30.97) | 0.03 (−0.24; 0.28) | 118.6 | 11.34 (5.79; 16.69) | 6.75 (1.22; 11.80) | 4.61 (1.10; 8.25) | |
| RCP4.5 | 617.7 | 20.07 (5.92; 30.53) | 20.04 (5.73; 30.79) | 0.03 (−0.25; 0.29) | 118.1 | 11.29 (5.79; 16.62) | 6.64 (1.16; 11.64) | 4.67 (1.10; 8.35) | |
| RCP8.5 | 605.4 | 19.67 (5.73; 30.12) | 19.64 (5.49; 30.32) | 0.03 (−0.29; 0.34) | 117.2 | 11.20 (5.73; 16.40) | 6.46 (1.05; 11.38) | 4.76 (1.14; 8.50) | |
| 2050s | |||||||||
| RCP2.6 | 784.5 | 20.11 (5.96; 30.54) | 20.08 (5.77; 30.81) | 0.03 (−0.25; 0.30) | 155.9 | 11.24 (5.76; 16.54) | 6.63 (1.16; 11.62) | 4.63 (1.09; 8.30) | |
| RCP4.5 | 753.2 | 19.30 (5.58; 29.67) | 19.28 (5.20; 29.94) | 0.04 (−0.33; 0.39) | 151.2 | 10.90 (5.54; 15.93) | 5.91 (0.80; 10.62) | 5.01 (1.25; 8.93) | |
| RCP8.5 | 705.8 | 18.09 (5.06; 28.04) | 18.04 (4.62; 28.40) | 0.06 (−0.49; 0.57) | 146.1 | 10.54 (5.40; 15.69) | 5.07 (0.37; 9.41) | 5.48 (1.39; 9.78) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tong, M.; Wondmagegn, B.; Xiang, J.; Hansen, A.; Dear, K.; Pisaniello, D.; Varghese, B.; Xiao, J.; Jian, L.; Scalley, B.; et al. Hospitalization Costs of Respiratory Diseases Attributable to Temperature in Australia and Projections for Future Costs in the 2030s and 2050s under Climate Change. Int. J. Environ. Res. Public Health 2022, 19, 9706. https://doi.org/10.3390/ijerph19159706
Tong M, Wondmagegn B, Xiang J, Hansen A, Dear K, Pisaniello D, Varghese B, Xiao J, Jian L, Scalley B, et al. Hospitalization Costs of Respiratory Diseases Attributable to Temperature in Australia and Projections for Future Costs in the 2030s and 2050s under Climate Change. International Journal of Environmental Research and Public Health. 2022; 19(15):9706. https://doi.org/10.3390/ijerph19159706
Chicago/Turabian StyleTong, Michael, Berhanu Wondmagegn, Jianjun Xiang, Alana Hansen, Keith Dear, Dino Pisaniello, Blesson Varghese, Jianguo Xiao, Le Jian, Benjamin Scalley, and et al. 2022. "Hospitalization Costs of Respiratory Diseases Attributable to Temperature in Australia and Projections for Future Costs in the 2030s and 2050s under Climate Change" International Journal of Environmental Research and Public Health 19, no. 15: 9706. https://doi.org/10.3390/ijerph19159706
APA StyleTong, M., Wondmagegn, B., Xiang, J., Hansen, A., Dear, K., Pisaniello, D., Varghese, B., Xiao, J., Jian, L., Scalley, B., Nitschke, M., Nairn, J., Bambrick, H., Karnon, J., & Bi, P. (2022). Hospitalization Costs of Respiratory Diseases Attributable to Temperature in Australia and Projections for Future Costs in the 2030s and 2050s under Climate Change. International Journal of Environmental Research and Public Health, 19(15), 9706. https://doi.org/10.3390/ijerph19159706