
Risk Factors Analysis of Surgical Infection Using Artificial Intelligence: A Single Center Study




Abstract
:1. Introduction
2. Materials and Methods
- Gender (male/female);
- Age;
- Length of stay (days);
- Hospital regime;
- Surgery department;
- Number of antibiotics;
- SSI (yes/no).
2.1. Statistical Analysis
2.2. Predictive Analysis
3. Results
3.1. Statistical Analysis
3.2. Predictive Analysis
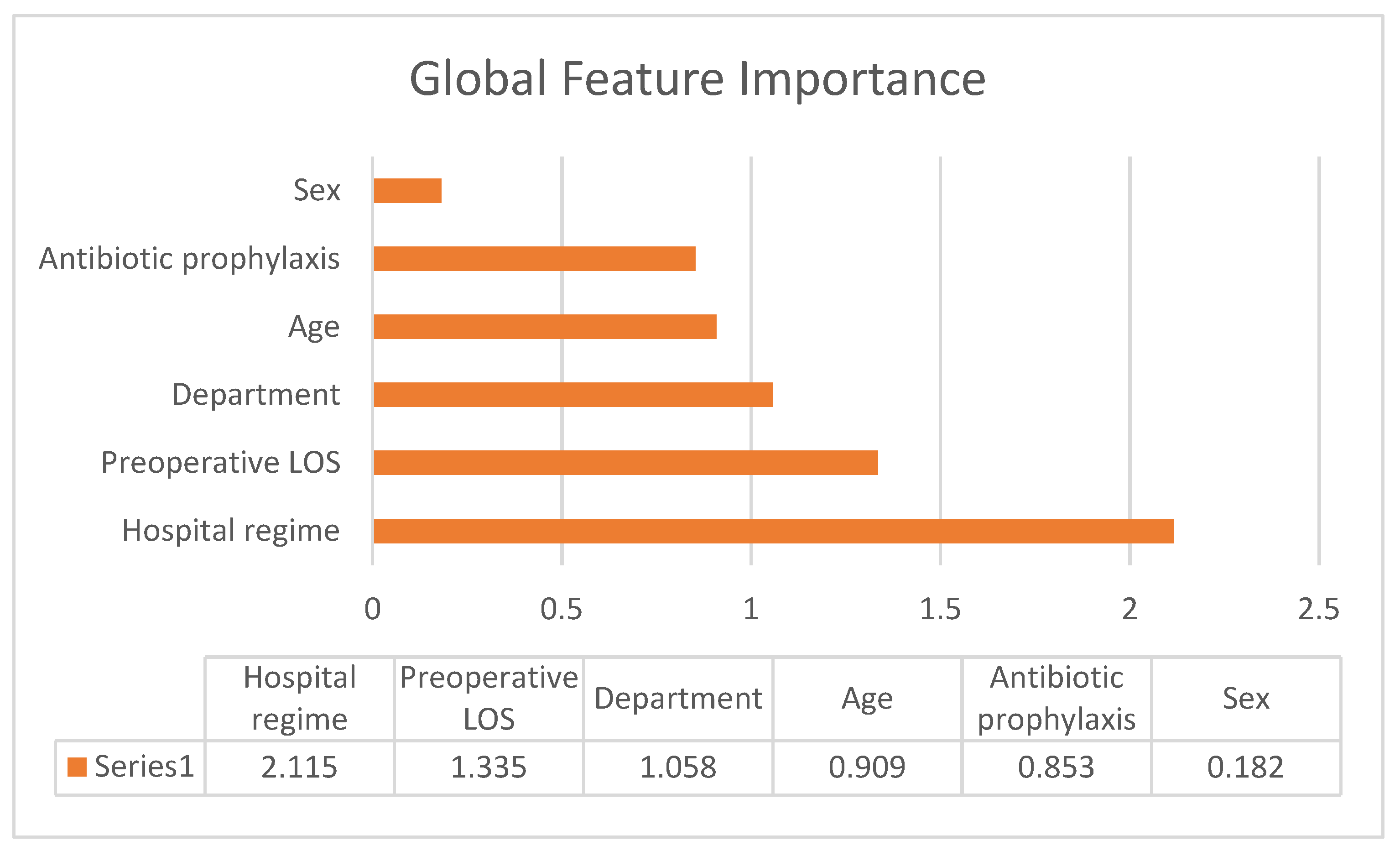
3.3. Global Feature Importance
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Tawfiq, J.A.; Tambyah, P.A. Healthcare associated infections (HAI) perspectives. J. Infect. Public Health 2014, 7, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Berríos-Torres, S.I.; Umscheid, C.A.; Bratzler, D.W.; Leas, B.; Stone, E.C.; Kelz, R.R.; Reinke, C.E.; Morgan, S.; Solomkin, J.S.; Mazuski, J.E.; et al. Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surg. 2017, 152, 784. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Healthcare-Associated Infections: Surgical Site Infections; Annual Epidemiological Report for 2017; ECDC: Stockholm, Sweden, 2019.
- Dipartimento Scienze della Salute Pubblica e Pediatriche, Università di Torino. Studio di Prevalenza Italiano Sulle Infezioni Correlate All’assistenza e Sull’uso di Antibiotici Negli Ospedali per Acuti—Protocollo ECDC; Università di Torino: Torino, Italy, 2018. [Google Scholar]
- Leaper, D.J. Surgical-site infection. Br. J. Surg. 2010, 97, 1601–1602. [Google Scholar] [CrossRef] [PubMed]
- Urban, J.A. Cost Analysis of Surgical Site Infections. Surg. Infect. 2006, 7, s19–s22. [Google Scholar] [CrossRef]
- Gastmeier, P.; Schwab, F.; Sohr, D.; Behnke, M.; Geffers, C. Reproducibility of the Surveillance Effect to Decrease Nosocomial Infection Rates. Infect. Control Hosp. Epidemiol. 2009, 30, 993–999. [Google Scholar] [CrossRef]
- Haley, R.W.; Culver, D.H.; White, J.W.; Morgan, W.M.; Emori, T.G.; Munn, V.P.; Hooton, T.M. The efficacy of infection surveillance and control programs in preventing nosocomial infections in us hospitals. Am. J. Epidemiol. 1985, 121, 182–205. [Google Scholar] [CrossRef]
- Mahmoud, N.N.; Turpin, R.S.; Yang, G.; Saunders, W.B. Impact of Surgical Site Infections on Length of Stay and Costs in Selected Colorectal Procedures. Surg. Infect. 2009, 10, 539–544. [Google Scholar] [CrossRef]
- Poggio, J. Perioperative Strategies to Prevent Surgical-Site Infection. Clin. Colon Rectal Surg. 2013, 26, 168–173. [Google Scholar] [CrossRef]
- Kocbek, P.; Fijacko, N.; Soguero-Ruiz, C.; Mikalsen, K.Ø.; Maver, U.; Povalej Brzan, P.; Stozer, A.; Jenssen, R.; Skrøvseth, S.O.; Stiglic, G. Maximizing Interpretability and Cost-Effectiveness of Surgical Site Infection (SSI) Predictive Models Using Feature-Specific Regularized Logistic Regression on Preoperative Temporal Data. Comput. Math. Methods Med. 2019, 2019, 2059851. [Google Scholar] [CrossRef]
- Mujagic, E.; Marti, W.R.; Coslovsky, M.; Soysal, S.D.; Mechera, R.; von Strauss, M.; Zeindler, J.; Saxer, F.; Mueller, A.; Fux, C.A.; et al. Associations of Hospital Length of Stay with Surgical Site Infections. World J. Surg. 2018, 42, 3888–3896. [Google Scholar] [CrossRef]
- Bisgaard, S.; Does, R.J.M.M. Quality Quandaries*: Health CareQuality—Reducing the Lengthof Stay at a Hospital. Qual. Eng. 2008, 21, 117–131. [Google Scholar] [CrossRef]
- Trunfio, T.A.; Scala, A.; Giglio, C.; Rossi, G.; Borrelli, A.; Romano, M.; Improta, G. Multiple regression model to analyze the total LOS for patients undergoing laparoscopic appendectomy. BMC Med. Inform. Decis. Mak. 2022, 22, 141. [Google Scholar] [CrossRef] [PubMed]
- Scala, A.; Trunfio, T.A.; De Coppi, L.; Rossi, G.; Borrelli, A.; Triassi, M.; Improta, G. Regression Models to Study the Total LOS Related to Valvuloplasty. Int. J. Environ. Res. Public Health 2022, 19, 3117. [Google Scholar] [CrossRef] [PubMed]
- Colella, Y.; Scala, A.; De Lauri, C.; Bruno, F.; Cesarelli, G.; Ferrucci, G.; Borrelli, A. Studying variables affecting the length of stay in patients with lower limb fractures by means of Machine Learning. In Proceedings of the 2021 5th International Conference on Medical and Health Informatics, Kyoto, Japan, 14–16 May 2021; pp. 39–43. [Google Scholar]
- Improta, G.; Borrelli, A.; Triassi, M. Machine Learning and Lean Six Sigma to Assess How COVID-19 Has Changed the Patient Management of the Complex Operative Unit of Neurology and Stroke Unit: A Single Center Study. Int. J. Environ. Res. Public Health 2022, 19, 5215. [Google Scholar] [CrossRef] [PubMed]
- Trunfio, T.A.; Borrelli, A.; Improta, G. Is It Possible to Predict the Length of Stay of Patients Undergoing Hip-Replacement Surgery? Int. J. Environ. Res. Public Health 2022, 19, 6219. [Google Scholar] [CrossRef] [PubMed]
- Maria Ponsiglione, A.; Profeta, M.; Giglio, C.; Lombardi, A.; Borrelli, A.; Scala, A. Modeling the variation in length of stay for appendectomy and cholecystectomy interventions in the emergency general surgery. In Proceedings of the 2021 International Symposium on Biomedical Engineering and Computational Biology, Nanchang, China, 13–15 August 2021; pp. 1–4. [Google Scholar]
- Lei, P.-R.; Liao, J.-W.; Ruan, Y.; Yang, X.-F.; Hu, K.-P.; Liu, J.-P.; Chen, T.-F. Risk factors analysis for surgical site infection following elective colorectal resection: A retrospective regression analysis. Chin. Med. J. 2020, 133, 571–576. [Google Scholar] [CrossRef]
- Improta, G.; Triassi, M.; Guizzi, G.; Santillo, L.C.; Revetria, R.; Catania, A.; Cassettari, L. An Innovative Contribution to Health Technology Assessment. In Modern Advances in Intelligent Systems and Tools; Studies in Computational Intelligence; Ding, W., Jiang, H., Ali, M., Li, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 431, pp. 127–131. ISBN 978-3-642-30731-7. [Google Scholar]
- Improta, G.; Perrone, A.; Russo, M.A.; Triassi, M. Health technology assessment (HTA) of optoelectronic biosensors for oncology by analytic hierarchy process (AHP) and Likert scale. BMC Med. Res. Methodol. 2019, 19, 140. [Google Scholar] [CrossRef]
- Improta, G.; Russo, M.A.; Triassi, M.; Converso, G.; Murino, T.; Santillo, L.C. Use of the AHP methodology in system dynamics: Modelling and simulation for health technology assessments to determine the correct prosthesis choice for hernia diseases. Math. Biosci. 2018, 299, 19–27. [Google Scholar] [CrossRef]
- Improta, G.; Converso, G.; Murino, T.; Gallo, M.; Perrone, A.; Romano, M. Analytic Hierarchy Process (AHP) in Dynamic Configuration as a Tool for Health Technology Assessment (HTA): The Case of Biosensing Optoelectronics in Oncology. Int. J. Inf. Technol. Decis. Mak. 2019, 18, 1533–1550. [Google Scholar] [CrossRef]
- Improta, G.; Ponsiglione, A.M.; Parente, G.; Romano, M.; Cesarelli, G.; Rea, T.; Triassi, M. Evaluation of Medical Training Courses Satisfaction: Qualitative Analysis and Analytic Hierarchy Process. In Proceedings of the European Medical and Biological Engineering Conference, Portorož, Slovenia, 29 November–3 December 2020; Springer International Publishing: Cham, Switzerland, 2020; pp. 518–526. [Google Scholar]
- Centro Nazionale per la Prevenzione e il Controllo Delle Malattie (CCM). Sistema Nazionale Sorveglianza Delle Infezioni Del Sito Chirurgico (SNICh)—Protocollo; CCM: Bologna, Italy, 2011.
- Sarnelli, B.; D’Agostino, F.; Signoriello, G.; Guida, A. Sorveglianza delle Infezioni del Sito Chirurgico in Campania; Direzione Generale per la Tutela della Salute ed il Coordinamento del SSR: Regione Campania, Italy, 2019; ISBN 978-88-31204-06-4. [Google Scholar]
- Regione Campania—Giunta Regionale Deliberazione N. 1715—Area Generale di Coordinamento N. 20—Assistenza Sanitaria—del Piano Regionale di Prevenzione e Controllo delle Infezioni Associate All’assistenza Sanitaria. Bollettino Ufficiale Della Regione Campania, 22 October 2007. [Google Scholar]
- UK Health Security Agency. Protocol for the Surveillance of Surgical Site Infection Surgical Site Infection Surveillance Service; UKHSA: London, UK, 2013.
- Guarino, F.; Improta, G.; Triassi, M.; Castiglione, S.; Cicatelli, A. Air quality biomonitoring through Olea europaea L.: The study case of “Land of pyres”. Chemosphere 2021, 282, 131052. [Google Scholar] [CrossRef]
- Guarino, F.; Improta, G.; Triassi, M.; Cicatelli, A.; Castiglione, S. Effects of Zinc Pollution and Compost Amendment on the Root Microbiome of a Metal Tolerant Poplar Clone. Front. Microbiol. 2020, 11, 1677. [Google Scholar] [CrossRef] [PubMed]
- Guarino, F.; Conte, B.; Improta, G.; Sciarrillo, R.; Castiglione, S.; Cicatelli, A.; Guarino, C. Genetic characterization, micropropagation, and potential use for arsenic phytoremediation of Dittrichia viscosa (L.) Greuter. Ecotoxicol. Environ. Saf. 2018, 148, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Guarino, F.; Cicatelli, A.; Brundu, G.; Improta, G.; Triassi, M.; Castiglione, S. The use of MSAP reveals epigenetic diversity of the invasive clonal populations of Arundo donax L. PLoS ONE 2019, 14, e0215096. [Google Scholar] [CrossRef] [PubMed]
- De Agostini, A.; Caltagirone, C.; Caredda, A.; Cicatelli, A.; Cogoni, A.; Farci, D.; Guarino, F.; Garau, A.; Labra, M.; Lussu, M.; et al. Heavy metal tolerance of orchid populations growing on abandoned mine tailings: A case study in Sardinia Island (Italy). Ecotoxicol. Environ. Saf. 2020, 189, 110018. [Google Scholar] [CrossRef] [PubMed]
- Moccia, E.; Intiso, A.; Cicatelli, A.; Proto, A.; Guarino, F.; Iannece, P.; Castiglione, S.; Rossi, F. Use of Zea mays L. in phytoremediation of trichloroethylene. Environ. Sci. Pollut. Res. 2017, 24, 11053–11060. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Cunha, T.F.S.; Soares Melancia, T.A.; Zagalo Fernandes Ribeiro, C.M.; Almeida de Brito, J.A.; Abreu Miguel, S.S.; André Abreu Esteves Bogalhão do Casal, D. Risk factors for surgical site infection in cervico-facial oncological surgery. J. Cranio-Maxillofac. Surg. 2012, 40, 443–448. [Google Scholar] [CrossRef]
- Cousin, A.-S.; Bouletreau, P.; Giai, J.; Ibrahim, B.; Louvrier, A.; Sigaux, N. Severity and long-term complications of surgical site infections after orthognathic surgery: A retrospective study. Sci. Rep. 2020, 10, 12015. [Google Scholar] [CrossRef]
- Manoukian, S.; Stewart, S.; Dancer, S.; Graves, N.; Mason, H.; McFarland, A.; Robertson, C.; Reilly, J. Estimating excess length of stay due to healthcare-associated infections: A systematic review and meta-analysis of statistical methodology. J. Hosp. Infect. 2018, 100, 222–235. [Google Scholar] [CrossRef]
- Lamagni, T.; Elgohari, S.; Harrington, P. Trends in surgical site infections following orthopaedic surgery. Curr. Opin. Infect. Dis. 2015, 28, 125–132. [Google Scholar] [CrossRef]
- Nasution, A.; Syed Sulaiman, S.A.; Shafie, A.A. PHP33 Drug-Related Problems and Length of Stay in the Management of Infection in Patients with Chronic Kidney Disease. Value Health 2012, 15, A615. [Google Scholar] [CrossRef]
- Hawn, M.T.; Richman, J.S.; Vick, C.C.; Deierhoi, R.J.; Graham, L.A.; Henderson, W.G.; Itani, K.M.F. Timing of Surgical Antibiotic Prophylaxis and the Risk of Surgical Site Infection. JAMA Surg. 2013, 148, 649. [Google Scholar] [CrossRef] [PubMed]
- Fisichella, L.; Fenga, D.; Rosa, M.A. Surgical Site Infection In Orthopaedic Surgery: Correlation Between Age, Diabetes, Smoke And Surgical Risk. Folia Med. 2014, 56, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Latham, R.; Lancaster, A.D.; Covington, J.F.; Pirolo, J.S.; Thomas, C.S. The Association of Diabetes and Glucose Control with Surgical-Site Infections among Cardiothoracic Surgery Patients. Infect. Control Hosp. Epidemiol. 2001, 22, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Montella, E.; Ferraro, A.; Sperlì, G.; Triassi, M.; Santini, S.; Improta, G. Predictive Analysis of Healthcare-Associated Blood Stream Infections in the Neonatal Intensive Care Unit Using Artificial Intelligence: A Single Center Study. Int. J. Environ. Res. Public. Health 2022, 19, 2498. [Google Scholar] [CrossRef]
- Tunthanathip, T.; Sae-heng, S.; Oearsakul, T.; Sakarunchai, I.; Kaewborisutsakul, A.; Taweesomboonyat, C. Machine learning applications for the prediction of surgical site infection in neurological operations. Neurosurg. Focus 2019, 47, E7. [Google Scholar] [CrossRef]
- Hopkins, B.S.; Mazmudar, A.; Driscoll, C.; Svet, M.; Goergen, J.; Kelsten, M.; Shlobin, N.A.; Kesavabhotla, K.; Smith, Z.A.; Dahdaleh, N.S. Using artificial intelligence (AI) to predict postoperative surgical site infection: A retrospective cohort of 4046 posterior spinal fusions. Clin. Neurol. Neurosurg. 2020, 192, 105718. [Google Scholar] [CrossRef]
- Ferraro, A.; Centobelli, P.; Cerchione, R.; Cicco, M.V.D.; Montella, E.; Raiola, E.; Triassi, M.; Improta, G. Implementation of lean practices to reduce healthcare associated infections. Int. J. Healthc. Technol. Manag. 2020, 18, 51. [Google Scholar] [CrossRef]
- Cesarelli, G.; Montella, E.; Scala, A.; Raiola, E.; Triassi, M.; Improta, G. DMAIC Approach for the Reduction of Healthcare-Associated Infections in the Neonatal Intensive Care Unit of the University Hospital of Naples ‘Federico II’. In Proceedings of the 8th European Medical and Biological Engineering Conference, Portorož, Slovenia, 29 November–3 December 2020; Jarm, T., Cvetkoska, A., Mahnič-Kalamiza, S., Miklavcic, D., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 414–423. [Google Scholar]
- Colella, Y.; Valente, A.S.; Rossano, L.; Trunfio, T.A.; Fiorillo, A.; Improta, G. A Fuzzy Inference System for the Assessment of Indoor Air Quality in an Operating Room to Prevent Surgical Site Infection. Int. J. Environ. Res. Public. Health 2022, 19, 3533. [Google Scholar] [CrossRef]


{kind=link}
| SSIs | Non-SSIs | p-Value | |
|---|---|---|---|
| Sex, boys | 29 (1.23%) | 2331 (98.77%) | 0.791 |
| Sex, girls | 19 (1.14%) | 1652 (98.86%) | |
| Hospital Regime | |||
| Ordinary hospitalization | 48 (1.33%) | 35,558 (98.67%) | 0.017 |
| Day Surgery | 0 (0.00%) | 425 (100.00%) | |
| Surgery Department | |||
| General surgery | 2 (0.25%) | 796 (99.75%) | <0.000 |
| Maxillo-facial surgery | 36 (3.17%) | 1098 (96.83%) | |
| Pediatric surgery | 1 (0.12%) | 813 (99.88%) | |
| Neurosurgery | 4 (0.42%) | 958 (99.58%) | |
| Orthopedics | 5 (1.55%) | 318 (98.45%) | |
| Antibiotic prophylaxis | |||
| no | 6 (0.57%) | 1.038 (99.43%) | |
| 1 antibiotic | 19 (0.70%) | 2697 (99.30%) | <0.000 |
| 2 or more antibiotics | 23 (8.49%) | 248 (91.51%) |
| OR | 95% CI | p-Value | |
|---|---|---|---|
| Sex, girls | 0.750 | −0.705–6.228 | 0.349 |
| Age | 1.010 | −0.006–0.026 | 0.221 |
| Hospital regime | |||
| Ordinary hospitalization | 3.908 | −0.705–6.228 | 0.248 |
| Surgery Department | |||
| Maxillo-facial surgery | 7.321 | 0.867–3.595 | <0.001 |
| Pediatric surgery | 0.660 | −3.002–1.883 | 0.722 |
| Neurosurgery | 1.422 | −1.177–2.119 | 0.656 |
| Orthopedics | 4.781 | 0.015–3.370 | 0.047 |
| Length of preoperative hospital stay | 1.021 | −0.002–0.046 | 0.071 |
| Antibiotic prophylaxis, No | |||
| 1 antibiotics | 0.447 | −1.797–0.318 | 0.151 |
| 2 or more antibiotics | 4.294 | 0.438–2.627 | 0.004 |
| Performance Metrics | Class | RF | LR | DT | KNN | GBT | XGB | NB |
|---|---|---|---|---|---|---|---|---|
| Accuracy (%) | Overall | 92.5 | 78.5 | 93.9 | 94.9 | 90 | 69.5 | 72.4 |
| Error (%) | Overall | 7.5 | 21.5 | 6.1 | 5.1 | 10 | 30.5 | 27.6 |
| Precision (%) | 0 | 99.4 | 99.2 | 99.5 | 99 | 99.2 | 99.7 | 99.4 |
| 1 | 7.9 | 2.8 | 11.1 | 4.7 | 5.1 | 3.2 | 2.8 | |
| Sensitivity (%) | 0 | 93 | 78.8 | 58.3 | 95.9 | 90.6 | 69.4 | 72.5 |
| 1 | 50 | 50 | 94.4 | 16.7 | 41.7 | 83.3 | 66.7 | |
| Specificity (%) | 0 | 50 | 50 | 58.3 | 16.7 | 41.7 | 83.3 | 66.7 |
| 1 | 93 | 78.8 | 94.4 | 95.9 | 90.6 | 69.4 | 72.5 | |
| F-measure (%) | 0 | 96.1 | 87.9 | 96.9 | 97.4 | 94.7 | 81.8 | 83.9 |
| 1 | 13.6 | 5.2 | 18.7 | 7.3 | 9 | 6.1 | 5.4 |
| Real/Predicted | 0 | 1 |
|---|---|---|
| 0 | 940 | 56 |
| 1 | 5 | 7 |
| Real/Predicted | 0 | 1 |
|---|---|---|
| 0 | 926 | 70 |
| 1 | 6 | 6 |
| Real/Predicted | 0 | 1 |
|---|---|---|
| 0 | 955 | 41 |
| 1 | 10 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scala, A.; Loperto, I.; Triassi, M.; Improta, G. Risk Factors Analysis of Surgical Infection Using Artificial Intelligence: A Single Center Study. Int. J. Environ. Res. Public Health 2022, 19, 10021. https://doi.org/10.3390/ijerph191610021
Scala A, Loperto I, Triassi M, Improta G. Risk Factors Analysis of Surgical Infection Using Artificial Intelligence: A Single Center Study. International Journal of Environmental Research and Public Health. 2022; 19(16):10021. https://doi.org/10.3390/ijerph191610021
Chicago/Turabian StyleScala, Arianna, Ilaria Loperto, Maria Triassi, and Giovanni Improta. 2022. "Risk Factors Analysis of Surgical Infection Using Artificial Intelligence: A Single Center Study" International Journal of Environmental Research and Public Health 19, no. 16: 10021. https://doi.org/10.3390/ijerph191610021
APA StyleScala, A., Loperto, I., Triassi, M., & Improta, G. (2022). Risk Factors Analysis of Surgical Infection Using Artificial Intelligence: A Single Center Study. International Journal of Environmental Research and Public Health, 19(16), 10021. https://doi.org/10.3390/ijerph191610021