
Epidemiological Analysis of Diabetes-Related Hospitalization in Poland before and during the COVID-19 Pandemic, 2014–2020


 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Statistical Analysis
3. Results
3.1. Trends in Diabetes-Related Hospitalizations in Poland between 2014 and 2020
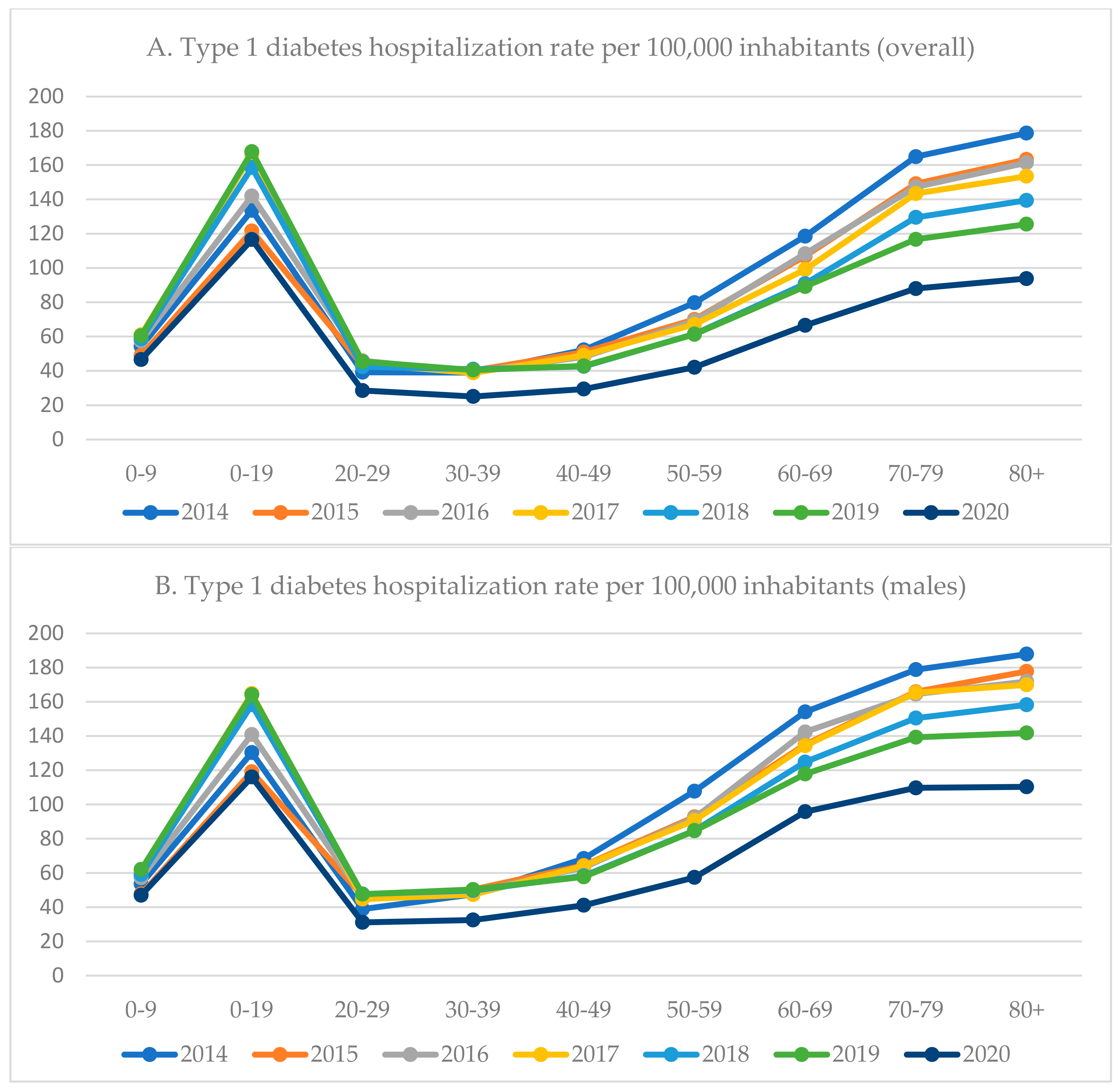
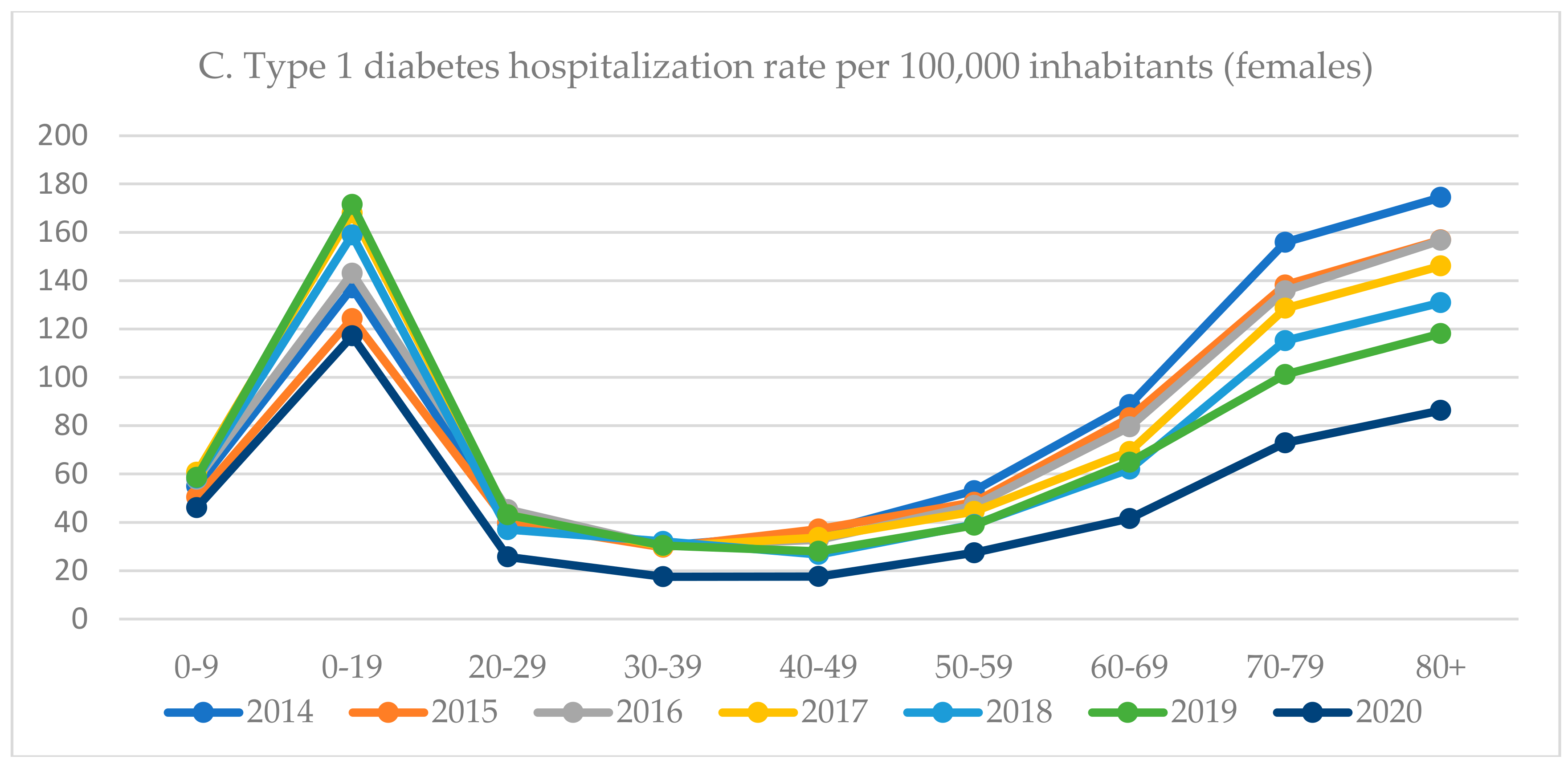
3.2. Type 1 Diabetes-Related Hospitalizations by Gender and Age
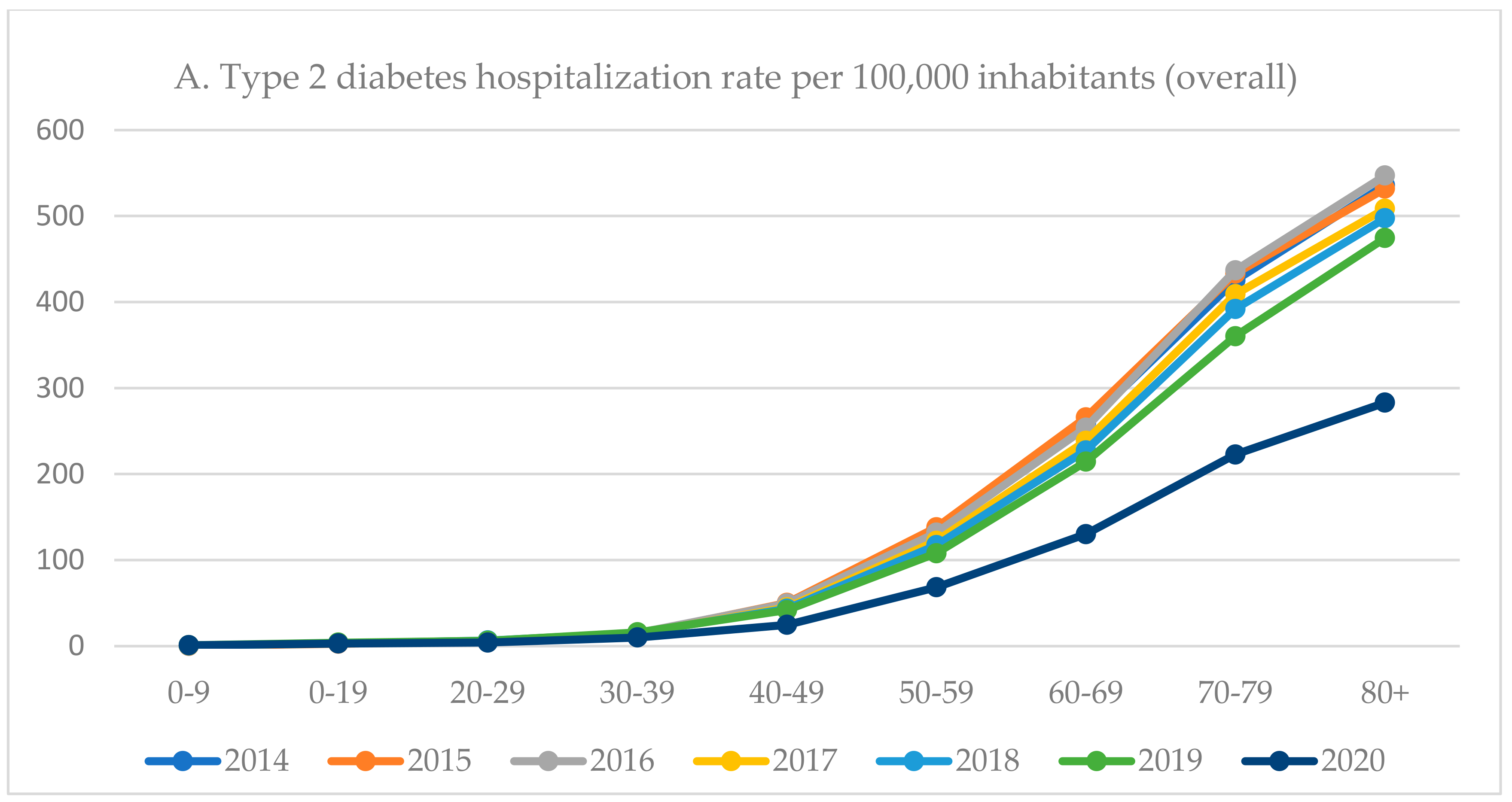
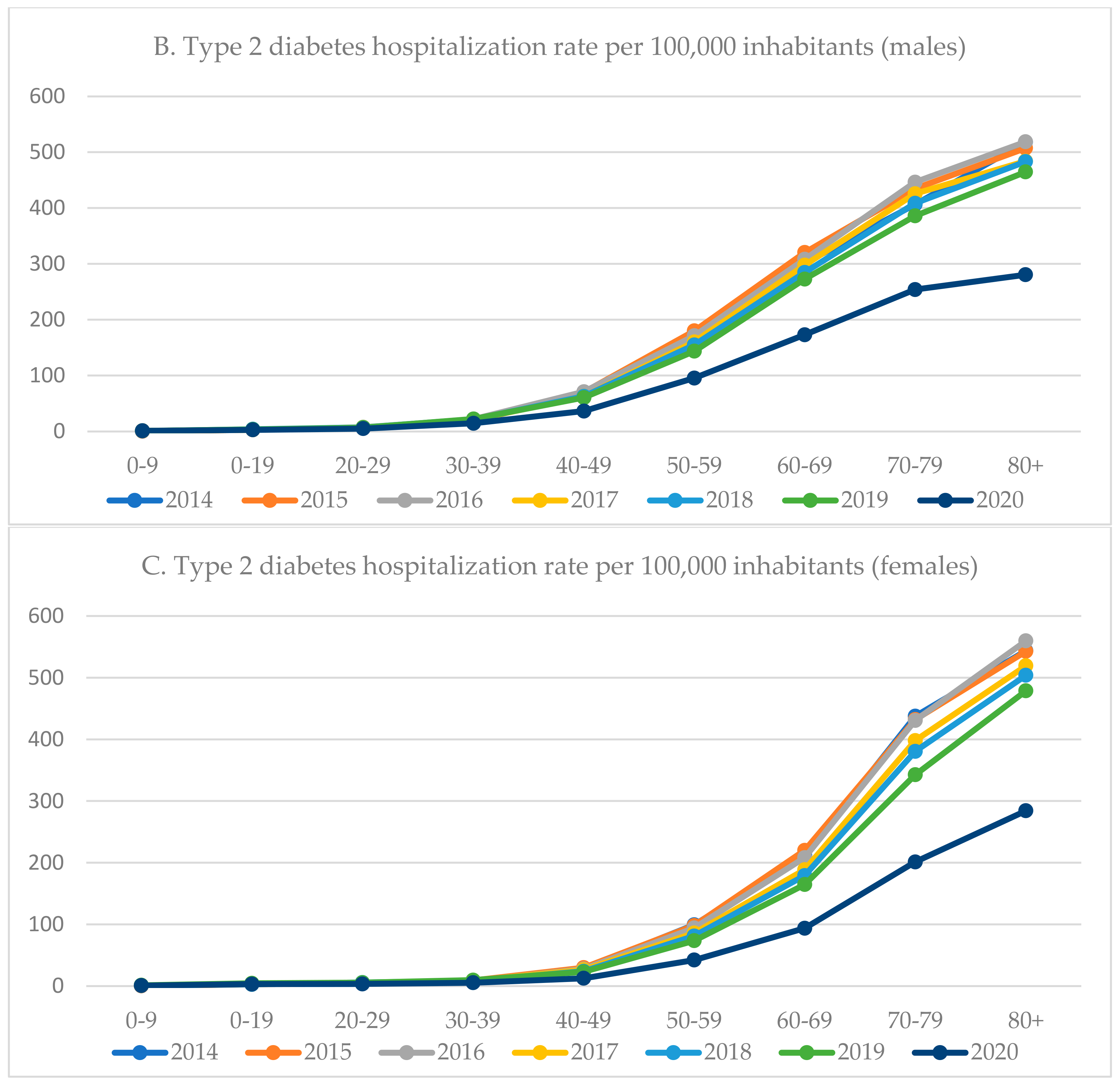
3.3. Type 2 Diabetes-Related Hospitalizations by Gender and Age
3.4. The Average Duration of Hospitalization
3.5. In-Hospital Mortality Rate
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Banday, M.Z.; Sameer, A.S.; Nissar, S. Pathophysiology of diabetes: An overview. Avicenna J. Med. 2020, 10, 174–188. [Google Scholar] [CrossRef] [PubMed]
- Petersmann, A.; Müller-Wieland, D.; Müller, U.A.; Landgraf, R.; Nauck, M.; Freckmann, G.; Heinemann, L.; Schleicher, E. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2019, 127, S1–S7. [Google Scholar] [CrossRef] [PubMed]
- Committee of the Japan Diabetes Society on the Diagnostic Criteria of Diabetes Mellitus; Seino, Y.; Nanjo, K.; Tajima, N.; Kadowaki, T.; Kashiwagi, A.; Araki, E.; Ito, C.; Inagaki, N.; Iwamoto, Y.; et al. Report of the committee on the classification and diagnostic criteria of diabetes mellitus. J. Diabetes Investig. 2010, 1, 212–228. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Liu, B.; Sun, Y.; Du, Y.; Snetselaar, L.G.; Hu, F.B.; Bao, W. Prevalence of diagnosed type 1 and type 2 diabetes among US adults in 2016 and 2017: Population based study. BMJ 2018, 362, k1497. [Google Scholar] [CrossRef]
- Tao, Z.; Shi, A.; Zhao, J. Epidemiological Perspectives of Diabetes. Cell Biochem. Biophys. 2015, 73, 181–185. [Google Scholar] [CrossRef]
- Narayan, K.M.; Gregg, E.W.; Fagot-Campagna, A.; Engelgau, M.M.; Vinicor, F. Diabetes—A common, growing, serious, costly, and potentially preventable public health problem. Diabetes Res. Clin. Pract. 2000, 50, S77–S84. [Google Scholar] [CrossRef]
- World Health Organization. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 3 July 2022).
- International Diabetes Federation. Diabetes around the World in 2021. Available online: https://diabetesatlas.org (accessed on 3 July 2022).
- Lovic, D.; Piperidou, A.; Zografou, I.; Grassos, H.; Pittaras, A.; Manolis, A. The Growing Epidemic of Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 104–109. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef]
- Kolb, H.; Martin, S. Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med. 2017, 15, 131. [Google Scholar] [CrossRef]
- Norris, J.M.; Johnson, R.K.; Stene, L.C. Type 1 diabetes-early life origins and changing epidemiology. Lancet Diabetes Endocrinol. 2020, 8, 226–238. [Google Scholar] [CrossRef]
- Weng, J.; Zhou, Z.; Guo, L.; Zhu, D.; Ji, L.; Luo, X.; Mu, Y.; Jia, W. T1D China Study Group. Incidence of type 1 diabetes in China, 2010–2013: Population based study. BMJ. 2018, 360, j5295. [Google Scholar] [CrossRef]
- Patterson, C.C.; Harjutsalo, V.; Rosenbauer, J.; Neu, A.; Cinek, O.; Skrivarhaug, T.; Rami-Merhar, B.; Soltesz, G.; Svensson, J.; Parslow, R.C.; et al. Trends and cyclical variation in the incidence of childhood type 1 diabetes in 26 European centres in the 25 year period 1989–2013: A multicentre prospective registration study. Diabetologia 2019, 62, 408–417. [Google Scholar] [CrossRef]
- Organisation for Economic Co-Operation and Development. Health at a Glance: Europe 2020. Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-europe-2020_82129230-en (accessed on 3 July 2022).
- Statista. Prevalence of Diabetes in Adult Population in Europe 2019, by Country. Available online: https://www.statista.com/statistics/1081006/prevalence-of-diabetes-in-europe/#:~:text=Germany%20had%20the%20highest%20prevalence%20of%20diabetes%20in,prevalence%20of%20diabetes%20in%20Europe%20at%204.4%20percent (accessed on 3 July 2022).
- Zatońska, K.; Basiak-Rasała, A.; Różańska, D.; Karczewski, M.; Wołyniec, M.; Szuba, A.; Połtyn-Zaradna, K. Changes in diabetes prevalence and corresponding risk factors-findings from 3- and 6-year follow-up of PURE Poland cohort study. BMC Public Health 2020, 20, 843. [Google Scholar] [CrossRef]
- Polish Ministry of Health. Diabetes in Numbers. Available online: https://pacjent.gov.pl/artykul/cukrzyca-w-liczbach (accessed on 3 July 2022).
- Chamberlain, J.J.; Herman, W.H.; Leal, S.; Rhinehart, A.S.; Shubrook, J.H.; Skolnik, N.; Kalyani, R.R. Pharmacologic Therapy for Type 2 Diabetes: Synopsis of the 2017 American Diabetes Association Standards of Medical Care in Diabetes. Ann. Intern. Med. 2017, 166, 572–578. [Google Scholar] [CrossRef]
- Mayo Clinic. Type 2 Diabetes. Available online: https://www.mayoclinic.org/diseases-conditions/type-2-diabetes/diagnosis-treatment/drc-20351199 (accessed on 2 July 2022).
- Chamberlain, J.J.; Kalyani, R.R.; Leal, S.; Rhinehart, A.S.; Shubrook, J.H.; Skolnik, N.; Herman, W.H. Treatment of Type 1 Diabetes: Synopsis of the 2017 American Diabetes Association Standards of Medical Care in Diabetes. Ann. Intern. Med. 2017, 167, 493–498. [Google Scholar] [CrossRef]
- Mayo Clinic. Type 1 Diabetes. Available online: https://www.mayoclinic.org/diseases-conditions/type-1-diabetes/diagnosis-treatment/drc-20353017 (accessed on 2 July 2022).
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]
- Overbeek, J.A.; Heintjes, E.M.; Prieto-Alhambra, D.; Blin, P.; Lassalle, R.; Hall, G.C.; Lapi, F.; Bianchini, E.; Hammar, N.; Bezemer, I.D.; et al. Type 2 Diabetes Mellitus Treatment Patterns Across Europe: A Population-based Multi-database Study. Clin. Ther. 2017, 39, 759–770. [Google Scholar] [CrossRef]
- Polish Diabetes Society. Clinical Recommendations for the Management of Diabetes Mellitus 2020. Available online: https://ptmr.info.pl/wp-content/uploads/2021/03/Zalecenia-kliniczne-dotyczace-postepowania-u-chorych-na-cukrzyce-2020.pdf (accessed on 4 July 2022).
- Grudziąż-Sękowska, J.; Sękowski, K.; Kobuszewski, B. Healthcare Utilization and Adherence to Treatment Recommendations among Children with Type 1 Diabetes in Poland during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4798. [Google Scholar] [CrossRef]
- Pinkas, J.; Jankowski, M.; Szumowski, Ł.; Lusawa, A.; Zgliczyński, W.S.; Raciborski, F.; Wierzba, W.; Gujski, M. Public Health Interventions to Mitigate Early Spread of SARS-CoV-2 in Poland. Med. Sci Monit. 2020, 26, e924730. [Google Scholar] [CrossRef]
- Kruszyńska-Fischbach, A.; Sysko-Romańczuk, S.; Rafalik, M.; Walczak, R.; Kludacz-Alessandri, M. Organizational E-Readiness for the Digital Transformation of Primary Healthcare Providers during the COVID-19 Pandemic in Poland. J. Clin. Med. 2021, 11, 133. [Google Scholar] [CrossRef]
- Kamrath, C.; Mönkemöller, K.; Biester, T.; Rohrer, T.R.; Warncke, K.; Hammersen, J.; Holl, R.W. Ketoacidosis in Children and Adolescents with Newly Diagnosed Type 1 Diabetes During the COVID-19 Pandemic in Germany. JAMA 2020, 324, 801–804. [Google Scholar] [CrossRef] [PubMed]
- Vellanki, P.; Umpierrez, G.E. Diabetic ketoacidosis risk during the COVID-19 pandemic. Lancet Diabetes Endocrinol. 2021, 9, 643–644. [Google Scholar] [CrossRef]
- Poznańska, A.; Goryński, P.; Seroka, W.; Stokwiszewski, J.; Radomski, P.; Wojtyniak, B. Nationwide General Hospital Morbidity Study as a source of data about Polish population health. Przegl. Epidemiol. 2019, 73, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Gujski, M.; Jankowski, M.; Rabczenko, D.; Goryński, P.; Juszczyk, G. The Prevalence of Acute Respiratory Distress Syndrome (ARDS) and Outcomes in Hospitalized Patients with COVID-19—A Study Based on Data from the Polish National Hospital Register. Viruses 2022, 14, 76. [Google Scholar] [CrossRef]
- International Statistical Classification of Diseases and Related Health Problems 10th Revision. ICD-10. Available online: https://icd.who.int/browse10/2010/en (accessed on 1 July 2022).
- Statistics of Poland. Demographic Characteristics. Available online: https://demografia.stat.gov.pl/BazaDemografia/CustomSelect.aspx (accessed on 1 July 2022).
- Jin, J.; Sklar, G.E.; Min Sen Oh, V.; Chuen Li, S. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther. Clin. Risk Manag. 2008, 4, 269–286. [Google Scholar]
- Schmitt, A.; Reimer, A.; Kulzer, B.; Haak, T.; Gahr, A.; Hermanns, N. Assessment of diabetes acceptance can help identify patients with ineffective diabetes self-care and poor diabetes control. Diabet. Med. 2014, 31, 1446–1451. [Google Scholar] [CrossRef]
- Caruso, R.; Magon, A.; Baroni, I.; Dellafiore, F.; Arrigoni, C.; Pittella, F.; Ausili, D. Health literacy in type 2 diabetes patients: A systematic review of systematic reviews. Acta Diabetol. 2018, 55, 1–12. [Google Scholar] [CrossRef]
- Espelt, A.; Borrell, C.; Palència, L.; Goday, A.; Spadea, T.; Gnavi, R.; Font-Ribera, L.; Kunst, A.E. Socioeconomic inequalities in the incidence and prevalence of type 2 diabetes mellitus in Europe. Gac. Sanit. 2013, 27, 494–501. [Google Scholar] [CrossRef]
- Ang, G.Y. Age of onset of diabetes and all-cause mortality. World J. Diabetes 2020, 11, 95–99. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Just Diagnosed with Type 1 Diabetes. Available online: https://www.cdc.gov/diabetes/basics/diabetes-type-1-diagnosis.html (accessed on 4 July 2022).
- Chew, B.H.; Ghazali, S.S.; Ismail, M.; Haniff, J.; Bujang, M.A. Age ≥ 60 years was an independent risk factor for diabetes-related complications despite good control of cardiovascular risk factors in patients with type 2 diabetes mellitus. Exp. Gerontol. 2013, 48, 485–491. [Google Scholar] [CrossRef]
- Aras, M.; Tchang, B.G.; Pape, J. Obesity and Diabetes. Nurs. Clin. N. Am. 2021, 56, 527–541. [Google Scholar] [CrossRef]
- Cooper, A.J.; Gupta, S.R.; Moustafa, A.F.; Chao, A.M. Sex/Gender Differences in Obesity Prevalence, Comorbidities, and Treatment. Curr. Obes. Rep. 2021, 10, 458–466. [Google Scholar] [CrossRef]
- Stoś, K.; Rychlik, E.; Woźniak, A.; Ołtarzewski, M.; Jankowski, M.; Gujski, M.; Juszczyk, G. Prevalence and Sociodemographic Factors Associated with Overweight and Obesity among Adults in Poland: A 2019/2020 Nationwide Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2022, 19, 1502. [Google Scholar] [CrossRef]
- Statistics Poland. Health Status of Population in Poland in 2019. Available online: https://stat.gov.pl/en/topics/health/health/health-status-of-population-in-poland-in-2019,4,2.html (accessed on 4 July 2022).
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.P.; Bentham, J. The epidemiological burden of obesity in childhood: A worldwide epidemic requiring urgent action. BMC Med. 2019, 17, 212. [Google Scholar] [CrossRef]
- Clements, M.A.; Lind, M.; Raman, S.; Patton, S.R.; Lipska, K.J.; Fridlington, A.G.; Tang, F.; Jones, P.G.; Wu, Y.; Spertus, J.A.; et al. Age at diagnosis predicts deterioration in glycaemic control among children and adolescents with type 1 diabetes. BMJ Open Diabetes Res. Care 2014, 2, e000039. [Google Scholar] [CrossRef]
- Grudziąż-Sękowska, J.; Zamarlik, M.; Sękowski, K. Assessment of Selected Aspects of the Quality of Life of Children with Type 1 Diabetes Mellitus in Poland. Int. J. Environ. Res. Public Health 2021, 18, 2107. [Google Scholar] [CrossRef]
- Niccoli, T.; Partridge, L. Ageing as a risk factor for disease. Curr. Biol. 2012, 22, R741–R7452. [Google Scholar] [CrossRef]
- Jeleff, M.; Traugott, M.; Jirovsky-Platter, E.; Jordakieva, G.; Kutalek, R. Occupational challenges of healthcare workers during the COVID-19 pandemic: A qualitative study. BMJ Open 2022, 12, e054516. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICD-10 | 2014 n = 75,476 | 2015 n = 74,826 | 2016 n = 76,220 | 2017 n = 74,670 | 2018 n = 72,188 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | |
| Hospitalization Rate (Number of Diabetes-Related Hospitalizations) per 100,000 Inhabitants | |||||||||||||||
| Overall | 196.2 | 205.5 | 187.3 | 194.7 | 206.4 | 183.7 | 198.3 | 211.4 | 186.0 | 194.3 | 209.9 | 179.7 | 187.9 | 205.2 | 171.7 |
| E10 | 80.4 | 89.2 | 72.1 | 75.2 | 83.7 | 67.2 | 78.1 | 87.5 | 69.3 | 79.0 | 89.4 | 69.2 | 74.4 | 85.9 | 63.6 |
| E11 | 107.3 | 106.0 | 108.4 | 110.8 | 112.1 | 109.6 | 111.4 | 113.0 | 110.0 | 106.0 | 108.7 | 103.3 | 103.9 | 107.4 | 100.6 |
| E13 | 4.5 | 5.5 | 3.5 | 4.7 | 5.9 | 3.6 | 4.6 | 5.8 | 3.4 | 4.5 | 5.8 | 3.3 | 4.3 | 5.6 | 3.1 |
| E14 | 4.0 | 4.8 | 3.3 | 4.0 | 4.8 | 3.2 | 4.2 | 5.1 | 3.4 | 4.9 | 5.9 | 3.8 | 5.3 | 6.2 | 4.4 |
| ICD-10 | 2019 n = 68,906 | 2020 n = 45,159 | Percentage Difference 2019–2020 | ||||||||||||
| T | M | F | T | M | F | Overall | Males | Females | p | ||||||
| Overall | 179.5 | 196.4 | 163.7 | 118.0 | 134.3 | 102.7 | −34.2 | −31.6 | −37.2 | <0.001 | |||||
| E10 | 74.6 | 85.4 | 64.4 | 53.0 | 62.5 | 44.1 | −28.9 | −26.7 | −31.6 | <0.001 | |||||
| E11 | 99.4 | 104.1 | 95.0 | 61.6 | 67.5 | 56.1 | −38.0 | −35.2 | −40.9 | <0.001 | |||||
| E13 | 0.5 | 0.6 | 0.3 | 0.3 | 0.4 | 0.2 | −38.0 | −38.4 | −37.1 | 0.9 | |||||
| E14 | 5.2 | 6.3 | 4.0 | 3.1 | 3.9 | 2.4 | −39.0 | −37.7 | −41.0 | 0.5 | |||||
| Age Group | 2014 n = 30,931 | 2015 n = 28,890 | 2016 n = 30,027 | 2017 n = 30,351 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | Males | Females | Overall | Males | Females | Overall | Males | Females | Overall | Males | Females | |||||||||||||
| X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | |
| Total | 7.6 | 9.7 | 7.7 | 8.5 | 7.4 | 10.9 | 7.6 | 8.1 | 7.8 | 8.8 | 7.4 | 7.3 | 7.4 | 8.5 | 7.7 | 9.2 | 7.0 | 7.4 | 7.4 | 9.5 | 7.7 | 9.2 | 7.0 | 9.9 |
| 0–9 | 5.2 | 5.0 | 5.1 | 4.8 | 5.2 | 5.2 | 5.3 | 5.2 | 5.2 | 5.0 | 5.5 | 5.3 | 5.2 | 6.3 | 5.3 | 7.3 | 5.1 | 5.0 | 4.9 | 4.8 | 5.0 | 4.8 | 4.8 | 4.7 |
| 10–19 | 4.4 | 3.9 | 4.5 | 4.1 | 4.4 | 3.8 | 4.5 | 3.9 | 4.5 | 3.9 | 4.5 | 3.7 | 4.4 | 3.8 | 4.3 | 3.8 | 4.4 | 3.8 | 4.0 | 3.7 | 3.9 | 3.7 | 4.0 | 3.7 |
| 20–29 | 5.6 | 3.7 | 5.6 | 3.5 | 5.6 | 4.0 | 5.6 | 6.8 | 5.8 | 4.3 | 5.4 | 3.4 | 5.2 | 3.3 | 5.3 | 3.5 | 5.1 | 3.1 | 5.5 | 4.5 | 5.5 | 4.1 | 5.4 | 4.9 |
| 30–39 | 6.3 | 5.9 | 6.6 | 6.3 | 6.0 | 5.4 | 6.4 | 8.1 | 6.5 | 5.9 | 6.3 | 8.2 | 6.2 | 5.4 | 6.5 | 5.8 | 5.7 | 4.5 | 6.4 | 6.7 | 6.5 | 6.3 | 6.1 | 7.3 |
| 40–49 | 7.3 | 6.6 | 7.5 | 7.2 | 7.0 | 5.1 | 7.8 | 9.2 | 8.0 | 8.4 | 7.4 | 7.3 | 7.4 | 8.0 | 7.6 | 7.1 | 7.1 | 9.6 | 7.7 | 7.7 | 7.8 | 7.4 | 7.6 | 8.3 |
| 50–59 | 8.5 | 8.9 | 8.8 | 9.6 | 8.0 | 7.5 | 8.9 | 9.8 | 9.3 | 9.9 | 8.3 | 7.7 | 8.8 | 10.5 | 9.5 | 11.3 | 7.7 | 8.6 | 9.3 | 10.5 | 9.8 | 11.4 | 8.2 | 8.2 |
| 60–69 | 9.6 | 11.1 | 9.8 | 11.0 | 9.4 | 11.3 | 9.7 | 9.2 | 9.9 | 10.5 | 9.3 | 8.7 | 9.6 | 10.2 | 10.2 | 11.4 | 8.7 | 8.2 | 9.8 | 10.7 | 10.5 | 11.7 | 8.8 | 8.8 |
| 70–79 | 9.9 | 15.5 | 10.3 | 10.6 | 9.7 | 18.3 | 9.4 | 9.8 | 10.0 | 10.5 | 8.9 | 8.1 | 9.4 | 9.8 | 9.8 | 10.1 | 9.0 | 9.4 | 9.6 | 10.3 | 10.3 | 11.4 | 9.1 | 9.3 |
| 80+ | 9.2 | 12.7 | 9.0 | 8.0 | 9.3 | 14.4 | 9.3 | 8.1 | 9.8 | 12.8 | 9.1 | 8.0 | 9.2 | 10.7 | 9.6 | 14.5 | 9.0 | 8.2 | 10.0 | 17.8 | 10.0 | 11.5 | 10.0 | 20.3 |
| Age Group | 2018 n = 28,584 | 2019 n = 28,617 | 2020 n = 20,282 | |||||||||||||||||||||
| Overall | Males | Females | Overall | Males | Females | Overall | Males | Females | ||||||||||||||||
| X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | |||||||
| Total | 7.6 | 8.8 | 7.8 | 9.6 | 6.9 | 7.6 | 7.2 | 8.7 | 7.5 | 9.4 | 6.8 | 7.8 | 7.7 | 11.3 | 8.0 | 11.3 | 7.2 | 11.2 | ||||||
| 0–9 | 5.1 | 5.1 | 5.3 | 5.2 | 4.9 | 5.0 | 5.0 | 5.0 | 4.9 | 5.1 | 5.0 | 4.9 | 6.0 | 7.1 | 6.1 | 8.5 | 5.9 | 5.3 | ||||||
| 10–19 | 4.1 | 3.7 | 4.1 | 3.7 | 4.1 | 3.7 | 3.9 | 3.8 | 3.8 | 3.6 | 4.0 | 4.0 | 4.3 | 4.5 | 4.2 | 4.1 | 4.3 | 4.9 | ||||||
| 20–29 | 5.3 | 4.0 | 5.3 | 3.6 | 5.3 | 4.5 | 5.3 | 3.8 | 5.4 | 3.5 | 5.2 | 4.1 | 5.4 | 3.9 | 5.5 | 4.2 | 5.4 | 3.4 | ||||||
| 30–39 | 6.3 | 6.4 | 6.7 | 7.3 | 5.8 | 4.4 | 6.2 | 5.5 | 6.4 | 5.7 | 5.8 | 5.0 | 6.6 | 7.3 | 6.7 | 7.2 | 6.4 | 7.5 | ||||||
| 40–49 | 7.7 | 7.8 | 8.0 | 8.3 | 6.8 | 6.5 | 7.4 | 7.3 | 7.6 | 7.6 | 7.0 | 6.6 | 7.8 | 8.0 | 7.8 | 7.7 | 7.6 | 8.6 | ||||||
| 50–59 | 8.9 | 9.2 | 9.4 | 9.8 | 8.0 | 7.6 | 9.2 | 12.1 | 9.6 | 13.4 | 8.3 | 8.7 | 9.6 | 11.7 | 10.1 | 12.4 | 8.4 | 10.0 | ||||||
| 60–69 | 10.0 | 11.8 | 10.8 | 12.9 | 8.7 | 9.4 | 9.9 | 11.1 | 10.4 | 12.0 | 9.0 | 9.7 | 10.4 | 15.5 | 11.0 | 17.4 | 9.1 | 10.9 | ||||||
| 70–79 | 10.3 | 11.5 | 11.2 | 12.3 | 9.4 | 10.7 | 9.7 | 10.7 | 10.2 | 11.1 | 9.3 | 10.3 | 10.4 | 17.6 | 10.3 | 12.3 | 10.4 | 21.8 | ||||||
| 80+ | 9.6 | 10.6 | 9.8 | 13.1 | 9.4 | 9.0 | 9.5 | 10.6 | 10.1 | 11.6 | 9.2 | 9.9 | 9.5 | 10.3 | 9.9 | 11.9 | 9.2 | 9.2 | ||||||
| Age Group | 2014 n = 41,275 | 2015 n = 42,599 | 2016 n = 42,821 | 2017 n = 40,722 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | Males | Females | Overall | Males | Females | Overall | Males | Females | Overall | Males | Females | |||||||||||||
| X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | |
| Total | 7.6 | 7.1 | 7.6 | 6.9 | 7.7 | 7.3 | 7.7 | 7.7 | 7.7 | 7.5 | 7.7 | 7.9 | 7.7 | 7.7 | 7.7 | 8.6 | 7.6 | 6.7 | 7.8 | 7.9 | 7.7 | 7.7 | 7.8 | 8.1 |
| 0–9 | 3.4 | 6.1 | 5.3 | 8.2 | 1.6 | 2.3 | 4.1 | 5.2 | 3.4 | 5.3 | 4.6 | 5.5 | 7.4 | 11.8 | 9.0 | 14.3 | 5.0 | 5.8 | 5.1 | 7.7 | 6.4 | 10.1 | 3.6 | 3.9 |
| 10–19 | 4.4 | 3.5 | 4.4 | 3.9 | 4.5 | 3.2 | 4.2 | 4.0 | 4.4 | 3.4 | 4.0 | 3.7 | 4.3 | 4.1 | 4.1 | 4.5 | 4.5 | 3.6 | 3.6 | 3.5 | 3.0 | 2.9 | 4.0 | 3.8 |
| 20–29 | 5.1 | 3.5 | 5.2 | 3.5 | 5.1 | 3.5 | 5.3 | 3.4 | 5.6 | 5.5 | 4.9 | 3.3 | 5.3 | 3.3 | 5.3 | 3.4 | 5.3 | 3.2 | 5.3 | 3.3 | 5.3 | 3.5 | 5.2 | 3.0 |
| 30–39 | 5.6 | 3.7 | 5.7 | 3.8 | 5.5 | 3.5 | 6.1 | 5.8 | 6.2 | 6.2 | 5.7 | 4.8 | 6.1 | 5.4 | 6.2 | 5.4 | 5.8 | 5.5 | 6.0 | 5.0 | 6.0 | 5.2 | 5.9 | 4.3 |
| 40–49 | 6.5 | 5.1 | 6.5 | 5.1 | 6.5 | 4.9 | 6.6 | 5.8 | 6.6 | 6.9 | 6.4 | 4.6 | 6.6 | 6.3 | 6.8 | 6.9 | 6.0 | 4.0 | 6.7 | 7.0 | 6.8 | 7.2 | 6.3 | 6.6 |
| 50–59 | 7.2 | 6.3 | 7.3 | 6.6 | 7.1 | 6.0 | 7.2 | 6.8 | 7.3 | 8.6 | 7.1 | 6.7 | 7.1 | 7.0 | 7.4 | 7.5 | 6.7 | 6.0 | 7.3 | 6.9 | 7.4 | 6.8 | 7.0 | 7.2 |
| 60–69 | 7.5 | 7.0 | 7.7 | 7.8 | 7.2 | 6.1 | 7.8 | 7.9 | 7.9 | 7.2 | 7.6 | 6.8 | 7.6 | 9.1 | 7.8 | 10.3 | 7.4 | 7.1 | 7.7 | 7.8 | 7.8 | 8.4 | 7.5 | 6.8 |
| 70–79 | 8.1 | 7.3 | 8.2 | 7.3 | 8.0 | 7.4 | 8.0 | 6.6 | 8.2 | 7.3 | 7.9 | 6.3 | 8.0 | 7.5 | 8.4 | 8.6 | 7.8 | 6.6 | 8.0 | 8.9 | 8.3 | 8.3 | 7.9 | 9.3 |
| 80+ | 8.3 | 8.3 | 8.3 | 6.5 | 8.4 | 8.9 | 8.3 | 9.9 | 8.4 | 7.5 | 8.3 | 10.8 | 8.4 | 7.0 | 8.4 | 7.4 | 8.4 | 6.8 | 8.5 | 8.0 | 8.4 | 7.0 | 8.6 | 8.4 |
| Age Group | 2018 n = 39,904 | 2019 n = 38,138 | 2020 n = 23,568 | |||||||||||||||||||||
| Overall | Males | Females | Overall | Males | Females | Overall | Males | Females | ||||||||||||||||
| X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | X | SD | |||||||
| Total | 7.9 | 8.8 | 8.0 | 8.5 | 7.8 | 9.0 | 7.7 | 7.5 | 7.8 | 7.8 | 7.6 | 7.2 | 8.1 | 9.9 | 8.2 | 9.2 | 8.0 | 10.6 | ||||||
| 0–9 | 5.4 | 5.3 | 5.6 | 5.7 | 5.2 | 5.2 | 5.0 | 5.4 | 4.5 | 6.1 | 5.3 | 4.9 | 3.7 | 4.8 | 4.1 | 4.8 | 3.2 | 4.9 | ||||||
| 10–19 | 3.9 | 3.3 | 4.2 | 3.6 | 3.4 | 2.9 | 4.2 | 3.7 | 4.8 | 4.2 | 3.8 | 3.2 | 4.4 | 4.1 | 4.3 | 4.5 | 4.5 | 3.8 | ||||||
| 20–29 | 5.2 | 4.5 | 5.8 | 5.3 | 4.5 | 3.1 | 5.1 | 3.4 | 5.2 | 3.8 | 4.8 | 2.8 | 5.4 | 5.1 | 5.8 | 5.8 | 4.9 | 3.8 | ||||||
| 30–39 | 6.4 | 6.6 | 6.3 | 6.2 | 6.5 | 7.6 | 5.8 | 5.8 | 5.7 | 4.2 | 6.2 | 8.3 | 6.0 | 5.6 | 6.1 | 5.0 | 5.9 | 7.2 | ||||||
| 40–49 | 6.5 | 5.8 | 6.6 | 5.9 | 6.3 | 5.6 | 6.5 | 6.2 | 6.6 | 6.6 | 6.1 | 5.0 | 7.1 | 7.7 | 7.3 | 7.6 | 6.7 | 8.1 | ||||||
| 50–59 | 7.5 | 7.5 | 7.8 | 8.3 | 6.9 | 5.6 | 7.5 | 8.4 | 7.9 | 9.2 | 6.9 | 6.5 | 7.9 | 8.9 | 8.2 | 9.7 | 7.0 | 6.8 | ||||||
| 60–69 | 7.9 | 8.3 | 8.1 | 8.8 | 7.5 | 7.4 | 7.7 | 7.6 | 7.9 | 8.0 | 7.4 | 7.0 | 8.1 | 8.6 | 8.3 | 9.1 | 7.7 | 7.6 | ||||||
| 70–79 | 8.1 | 8.6 | 8.4 | 8.6 | 7.9 | 8.6 | 8.0 | 8.1 | 8.3 | 8.0 | 7.8 | 8.1 | 8.4 | 9.2 | 8.7 | 9.9 | 8.2 | 8.4 | ||||||
| 80+ | 8.7 | 11.1 | 8.8 | 9.7 | 8.6 | 11.7 | 8.2 | 6.8 | 8.2 | 6.7 | 8.3 | 6.9 | 8.8 | 13.6 | 8.7 | 9.0 | 8.8 | 15.1 | ||||||
| Age Group | 2014 n = 30,931 | 2015 n = 28,890 | 2016 n = 30,027 | 2017 n = 30,351 | 2018 n = 28,584 | 2019 n = 28,617 | 2020 n = 20,282 | Percentage Difference 2019–2020 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | p | |
| Overall | 1.9 | 1.7 | 2.1 | 2.1 | 1.9 | 2.4 | 2.2 | 2.0 | 2.5 | 2.2 | 2.0 | 2.4 | 2.4 | 2.2 | 2.6 | 2.1 | 2.0 | 2.3 | 3.5 | 3.2 | 3.8 | 66.7 | 60.0 | 65.2 | <0.001 |
| 0–9 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | N/A | N/A | N/A | N/A |
| 10–19 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | N/A | N/A | N/A | N/A |
| 20–29 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.0 | 0.2 | 0.2 | 0.3 | 0.2 | 0.2 | 0.1 | 0.2 | 0.1 | 0.2 | 0.1 | 0.2 | 0.3 | 0.0 | N/A | N/A | N/A | N/A |
| 30–39 | 0.6 | 0.7 | 0.3 | 0.4 | 0.5 | 0.1 | 0.5 | 0.6 | 0.2 | 0.4 | 0.6 | 0.1 | 0.8 | 1.0 | 0.4 | 0.6 | 0.8 | 0.3 | 1.1 | 1.6 | 0.2 | N/A | N/A | N/A | N/A |
| 40–49 | 0.6 | 0.5 | 0.8 | 1.3 | 1.6 | 0.9 | 0.7 | 0.8 | 0.5 | 1.0 | 1.5 | 0.1 | 0.9 | 1.1 | 0.6 | 1.0 | 1.3 | 0.4 | 1.8 | 2.1 | 1.0 | 80.0 | 61.5 | 150.0 | 0.03 |
| 50–59 | 1.2 | 1.4 | 0.7 | 1.6 | 1.7 | 1.5 | 1.9 | 1.8 | 2.0 | 1.5 | 1.2 | 2.0 | 1.7 | 1.7 | 1.7 | 1.9 | 2.2 | 1.3 | 2.7 | 3.1 | 2.0 | 42.1 | 40.9 | 53.8 | 0.052 |
| 60–69 | 2.2 | 2.6 | 1.6 | 2.6 | 2.3 | 2.9 | 2.8 | 2.9 | 2.6 | 3.0 | 3.2 | 2.6 | 3.2 | 3.0 | 3.6 | 3.0 | 2.7 | 3.5 | 4.5 | 4.7 | 4.1 | 50.0 | 74.1 | 17.1 | <0.001 |
| 70–79 | 4.4 | 4.6 | 4.2 | 4.7 | 4.7 | 4.8 | 4.9 | 4.7 | 5.2 | 4.5 | 5.2 | 3.9 | 5.0 | 5.8 | 4.3 | 5.1 | 5.2 | 4.9 | 8.8 | 8.0 | 9.6 | 72.5 | 53.8 | 95.9 | <0.001 |
| 80+ | 7.7 | 6.9 | 8.1 | 8.3 | 8.8 | 8.0 | 9.3 | 10.1 | 8.9 | 10.0 | 9.5 | 10.3 | 11.3 | 12.5 | 10.6 | 9.7 | 9.8 | 9.7 | 14.1 | 13.2 | 14.7 | 45.4 | 34.7 | 51.5 | <0.001 |
| Age Group | 2014 n = 41,275 | 2015 n = 42,599 | 2016 n = 42,821 | 2017 n = 40,722 | 2018 n = 39,904 | 2019 n = 38,138 | 2020 n = 23,568 | Percentage Difference 2019–2020 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | T | M | F | p | |
| Overall | 2.9 | 2.4 | 3.3 | 2.9 | 2.4 | 3.3 | 3.2 | 2.8 | 3.5 | 2.9 | 2.4 | 3.4 | 3.3 | 2.8 | 3.8 | 3.3 | 2.9 | 3.8 | 4.9 | 4.5 | 5.4 | 48.5 | 55.2 | 42.1 | <0.001 |
| 0–9 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | N/A | N/A | N/A | N/A |
| 10–19 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | N/A | N/A | N/A | N/A |
| 20–29 | 0.7 | 0.6 | 1.0 | 0.0 | 0.0 | 0.0 | 0.4 | 0.6 | 0.0 | 0.3 | 0.0 | 0.8 | 0.3 | 0.6 | 0.0 | 0.0 | 0.0 | 0.0 | 0.5 | 0.0 | 1.4 | N/A | N/A | N/A | N/A |
| 30–39 | 0.4 | 0.5 | 0.0 | 0.4 | 0.3 | 0.7 | 0.3 | 0.4 | 0.0 | 0.1 | 0.2 | 0.0 | 0.6 | 0.6 | 0.8 | 0.7 | 0.6 | 1.0 | 1.8 | 1.8 | 1.9 | N/A | N/A | N/A | N/A |
| 40–49 | 0.2 | 0.3 | 0.1 | 0.8 | 0.8 | 0.8 | 0.9 | 1.1 | 0.4 | 0.8 | 0.8 | 0.8 | 1.0 | 1.0 | 1.2 | 1.0 | 1.0 | 0.9 | 1.1 | 1.2 | 0.5 | 10.0 | 20.0 | −44.4 | 0.9 |
| 50–59 | 1.1 | 1.2 | 1.1 | 1.1 | 1.1 | 1.2 | 1.1 | 1.1 | 1.2 | 0.9 | 0.8 | 0.9 | 1.3 | 1.3 | 1.2 | 1.1 | 1.2 | 0.9 | 2.0 | 1.8 | 2.3 | 81.8 | 50.0 | 155.6 | 0.001 |
| 60–69 | 1.6 | 1.7 | 1.6 | 1.5 | 1.4 | 1.6 | 2.0 | 2.1 | 1.8 | 1.7 | 1.6 | 1.8 | 2.1 | 2.1 | 2.0 | 2.0 | 2.2 | 1.9 | 3.5 | 3.5 | 3.3 | 75.0 | 59.1 | 73.7 | <0.001 |
| 70–79 | 3.3 | 3.6 | 3.1 | 3.2 | 3.6 | 3.0 | 3.4 | 3.9 | 3.1 | 2.9 | 3.2 | 2.6 | 3.2 | 3.7 | 2.8 | 3.5 | 3.7 | 3.4 | 5.3 | 5.9 | 4.7 | 51.4 | 59.5 | 38.2 | <0.001 |
| 80+ | 6.8 | 6.9 | 6.8 | 7.1 | 7.7 | 6.8 | 7.2 | 7.8 | 6.9 | 7.1 | 7.3 | 7.0 | 7.5 | 6.9 | 7.8 | 7.6 | 7.8 | 7.5 | 10.2 | 11.8 | 9.4 | 34.2 | 51.3 | 25.3 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sękowski, K.; Grudziąż-Sękowska, J.; Goryński, P.; Pinkas, J.; Jankowski, M. Epidemiological Analysis of Diabetes-Related Hospitalization in Poland before and during the COVID-19 Pandemic, 2014–2020. Int. J. Environ. Res. Public Health 2022, 19, 10030. https://doi.org/10.3390/ijerph191610030
Sękowski K, Grudziąż-Sękowska J, Goryński P, Pinkas J, Jankowski M. Epidemiological Analysis of Diabetes-Related Hospitalization in Poland before and during the COVID-19 Pandemic, 2014–2020. International Journal of Environmental Research and Public Health. 2022; 19(16):10030. https://doi.org/10.3390/ijerph191610030
Chicago/Turabian StyleSękowski, Kuba, Justyna Grudziąż-Sękowska, Paweł Goryński, Jarosław Pinkas, and Mateusz Jankowski. 2022. "Epidemiological Analysis of Diabetes-Related Hospitalization in Poland before and during the COVID-19 Pandemic, 2014–2020" International Journal of Environmental Research and Public Health 19, no. 16: 10030. https://doi.org/10.3390/ijerph191610030
APA StyleSękowski, K., Grudziąż-Sękowska, J., Goryński, P., Pinkas, J., & Jankowski, M. (2022). Epidemiological Analysis of Diabetes-Related Hospitalization in Poland before and during the COVID-19 Pandemic, 2014–2020. International Journal of Environmental Research and Public Health, 19(16), 10030. https://doi.org/10.3390/ijerph191610030