
Cross-Sectional Study of Factors Influencing Perceived Threat and Stress among the Arab Minority in Israel during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Instruments
2.2. Data Analysis
3. Results
Sample Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). WHO declares novel coronavirus (2019-nCoV) sixth Public Health Emergency of International Concern. Eurosurveillance 2020, 25, 200131e. [Google Scholar] [CrossRef]
- Fiorillo, A.; Gorwood, P.; Bodescot, M. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, 35–62. [Google Scholar] [CrossRef] [PubMed]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef]
- Tucci, V.; Moukaddam, N.; Meadows, J.; Shah, S.; Galwankar, S.C.; Kapur, G.B. The forgotten plague: Psychiatric manifestations of Ebola, zika, and emerging infectious diseases. J. Glob. Infect. Dis. 2017, 9, 151–156. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.C.; Kurosawa, M.; Benedek, D.M. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry Clin. Neurosci. 2020, 74, 281–282. [Google Scholar] [CrossRef]
- Banerjee, D.; Rai, M. Social isolation in Covid-19: The impact of loneliness. Int. J. Soc. Psychiatry 2020, 66, 525–527. [Google Scholar] [CrossRef]
- Grote, N.K.; Bledsoe, S.E.; Larkin, J.; Lemay, E.P., Jr.; Brown, C. Stress exposure and depression in disadvantaged women: The protective effects of optimism and perceived control. Soc. Work. Res. 2007, 31, 19–33. [Google Scholar] [CrossRef]
- Zhang, W.; Liu, H.; Jiang, X.; Wu, D.; Tian, Y. A longitudinal study of posttraumatic stress disorder symptoms and its relationship with coping skill and locus of control in adolescents after an earthquake in China. PLoS ONE 2014, 9, e88263. [Google Scholar] [CrossRef]
- Smith, N.B.; Sippel, L.M.; Presseau, C.; Rozek, D.; Mota, N.; Gordon, C.; Horvath, M.; Harpaz-Rotem, I. Locus of control in US combat veterans: Unique associations with posttraumatic stress disorder 5-factor model symptom clusters. Psychiatry Res. 2018, 268, 152–156. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19): How to Prepare. 2020. Available online: www.cdc.gov/coronavirus/2019-ncov/prepare/prevention.html (accessed on 20 May 2020).
- Ministry of Health. 2020. Available online: https://govextra.gov.il/ministry-of-health/corona/corona-virus/ (accessed on 20 May 2020).
- Zandifar, A.; Badrfam, R. Iranian mental health during the COVID-19 epidemic. Asian J. Psychiatry 2020, 51, 101990. [Google Scholar] [CrossRef]
- Hwang, T.J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and Social Isolation during the COVID-19 Pandemic. Int. Psychogeriatr. 2020, 32, 1217–1220. [Google Scholar] [CrossRef]
- O’Súilleabháin, P.S.; Gallagher, S.; Steptoe, A. Loneliness, living alone, and all-cause mortality: The role of emotional and social loneliness in the elderly during 19 years of follow-up. Psychosom. Med. 2019, 81, 521–526. [Google Scholar] [CrossRef]
- Stickley, A.; Koyanagi, A. Physical multimorbidity and loneliness: A population-based study. PLoS ONE 2018, 13, e0191651. [Google Scholar] [CrossRef]
- Valtorta, N.K.; Kanaan, M.; Gilbody, S.; Hanratty, B. Loneliness, social isolation and risk of cardiovascular disease in the English Longitudinal Study of Ageing. Eur. J. Prev. Cardiol. 2018, 25, 1387–1396. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Cacioppo, S. The growing problem of loneliness. Lancet 2018, 391, 426. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, S.; Gruen, R.; DeLongis, A. Appraisal, coping, health status and psychological symptoms. J. Personal. Soc. Psychol. 1986, 50, 571579. [Google Scholar] [CrossRef]
- Taha, S.; Matheson, K.; Cronin, T.; Anisman, H. Intolerance of uncertainty, appraisals, coping, and anxiety: The case of the 2009 H1N1 pandemic. Br. J. Health Psychol. 2014, 19, 592–605. [Google Scholar] [CrossRef]
- Stodolska, M. #QuarantineChallenge2k20: Leisure in the Time of the Pandemic. Leis. Sci. 2020, 43, 232–239. [Google Scholar] [CrossRef]
- Cutter, S.L.; Boruff, B.J.; Shirley, W.L. Social vulnerability to environmental hazards. Soc. Sci. Q. 2003, 84, 242–261. [Google Scholar] [CrossRef]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry Interpers. Biol. Process. 2002, 65, 207–239. [Google Scholar] [CrossRef]
- Central Bureau of Statistics. Statistical Abstract of Israel 2015—No. 66. 2015. Available online: https://www.cbs.gov.il/en/publications/Pages/2015/Statistical-Abstract-of-Israel-2015-No66.aspx (accessed on 21 May 2020).
- Chernichovsky, D.; Bisharat, B.; Bowers, L.; Brill, A.; Sharony, C. The Health of the Arab Israeli Population. In State of the Nation Report, Taub Center for Social Policy Studies in Israel, Jerusalem. 2017, pp. 325–365. Available online: http://taubcenter.org.il/wp-content/files_mf/healthofthearabisraelipopulation.pdf (accessed on 26 May 2020).
- Habib, J.; King, J.; Shoham, A.B.; Wolde-Tsadick, A.; Lasky, K. Labour market and socio-economic outcomes of the Arab-Israeli population. In OECD Social, Employment and Migration Working Papers; No. 102; OECD Publishing: Paris, France, 2010. [Google Scholar]
- National Insurance Institute. Poverty and Social Gaps, Annual Report. 2016. Available online: https://www.btl.gov.il/English%20Homepage/Publications/Poverty_Report/Documents/oni2016-e.pdf (accessed on 28 May 2020).
- Baron-Epel, O.; Kaplan, G.; Haviv-Messika, A.; Tarabeia, J.; Green, M.S.; Kaluski, D.N. Self-reported health as a cultural health determinant in Arab and Jewish Israelis MABAT—National Health and Nutrition Survey 1999–2001. Soc. Sci. Med. 2005, 61, 1256–1266. [Google Scholar] [CrossRef]
- Kimhi, S.; Eshel, Y.; Marciano, H.; Adini, B. Distress and resilience in the days of COVID-19: Comparing two ethnicities. Int. J. Environ. Res. Public Health 2020, 17, 3956. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.O.M.; Mermelstein, R.O.B.I.N. Perceived stress scale. In Measuring Stress: A Guide for Health and Social Scientists; Oxford University Press: Oxford, UK, 1994; Volume 10, pp. 1–2. [Google Scholar]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Personal. Soc. Psychol. 1989, 56, 267. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Lima, B.R.; Chavez, H.; Samaniego, N.; Pompei, M.S.; Pai, S.; Santacruz, H.; Lozano, J. Disaster severity and emotional disturbance: Implications for primary mental health care in developing countries. Acta Psychiatr. Scand. 1989, 79, 74–82. [Google Scholar] [CrossRef]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Ben-Zur, H.; Gilbar, O.; Lev, S. Coping with breast cancer: Patient, spouse and dyadic models. Psychosom. Med. 2001, 63, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Ben-Zur, H. Monitoring/blunting and social support: Associations with coping and affect. Int. J. Stress Manag. 2002, 9, 357–373. [Google Scholar] [CrossRef]
- Krampe, H.; Danbolt, L.J.; Haver, A.; Stålsett, G.; Schnell, T. Locus of control moderates the association of COVID-19 stress and general mental distress: Results of a Norwegian and a German-speaking cross-sectional survey. BMC Psychiatry 2021, 21, 437. [Google Scholar] [CrossRef] [PubMed]
- O’Hea, E.L.; Moon, S.; Grothe, K.B.; Boudreaux, E.; Bodenlos, J.S.; Wallston, K.; Brantley, P.J. The interaction of locus of control, self-efficacy, and outcome expectancy in relation to HbA1c in medically underserved individuals with type 2 diabetes. J. Behav. Med. 2009, 32, 106–117. [Google Scholar] [CrossRef]
- Norenzayan, A.; Lee, A. It was meant to happen: Explaining cultural variations in fate attributions. J. Personal. Soc. Psychol. 2010, 98, 702–720. [Google Scholar] [CrossRef]
- Threlfall, J.M.; Seay, K.D.; Kohl, P.L. The parenting role of African American fathers in the context of urban poverty. J. Child. Poverty 2013, 19, 45–61. [Google Scholar] [CrossRef]
- Ahmed, A.S. Post-traumatic stress disorder, resilience, and vulnerability. Adv. Psychiatr. Treat. 2007, 13, 369–375. [Google Scholar] [CrossRef]
- Mayor, E. Gender roles and traits in stress and health. Front. Psychol. 2015, 6, 779. [Google Scholar] [CrossRef]
- Yarcheski, A.; Mahon, N.E.; Yarcheski, T.J. Stress, hope, and loneliness in young adolescents. Psychol. Rep. 2011, 108, 919–922. [Google Scholar] [CrossRef]
- Brown, E.G.; Gallagher, S.; Creaven, A.M. Loneliness and acute stress reactivity: A systematic review of psychophysiological studies. Psychophysiology 2018, 55, e13031. [Google Scholar] [CrossRef]
- Baqutayan, S. Stress and social support. Indian J. Psychol. Med. 2011, 33, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Kumanova, M.; Karastoyanov, G.S. Perceived Stress and Coping Strategies. 2019. Available online: https://www.researchgate.net/publication/332466379 (accessed on 9 November 2020).
- Putermana, E.; DeLongisa, A.; Lee-Baggleya, D.; Greenglass, E. Coping and health behaviors in times of global health crises: Lessons from SARS and West Nile. Glob. Public Health 2009, 4, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Goldzweiga, G.; Hasson-Ohayonb, I.; Alonc, S.; Shalita, E. Perceived threat and depression among patients with cancer: The moderating role of health locus of control. Psychol. Health Med. 2016, 21, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Moorey, S.; Greer, S. Cognitive Behavior Therapy for People with Cancer; Oxford University Press: Oxford, UK, 2002. [Google Scholar]


{kind=link}
| Variable | ||
|---|---|---|
| Gender | Male (%) | 102 (21.0) |
| Female (%) | 384 (79.0) | |
| Age | 18–25 (%) | 56 (11.5) |
| 26–45 (%) | 281 (57.8) | |
| 46–65 (%) | 149 (30.7) | |
| Ethnicity | Muslim (%) | 426 (87.7) |
| Christian (%) | 47 (9.7) | |
| Other (%) | 13 (2.6) | |
| Place of living | Rural (%) | 363 (74.7) |
| Urban (%) | 123 (25.3) | |
| Religiosity | Secular (%) | 61 (12.6) |
| Partly religious (%) | 220 (45.5) | |
| Religious (%) | 203 (41.9) | |
| Marital status | Married/in a steady relationship (%) | 397 (81.7) |
| Single (%) | 71 (14.6) | |
| Divorced/Widowed (%) | 18 (3.7) | |
| Children | Yes (%) | 383 (78.8) |
| Number of children | Mean number of children (SD), range | 3.07 (1.06), 1–7 |
| Education | Elementary (%) | 4 (0.8) |
| High school (%) | 77 (15.8) | |
| Professional (%) | 76 (15.6) | |
| Academic (%) | 329 (67.7) | |
| Health | Good (%) | 437 (89.9) |
| Not good (%) | 49 (10.1) | |
| Employment | Employed (%) | 412 (84.8) |
| Unemployed (%) | 74 (15.2) | |
| Usual place of work (n = 412) | Outside the home (%) | 322 (78.2) |
| At home (%) | 90 (21.8) | |
| Leave of absence during COVID (n = 412) | Yes (%) | 124 (30.1) |
| No (%) | 288 (69.9) |
| M (SD) | 2. | 3. | 4. | 5. | 6. | 7. | |
|---|---|---|---|---|---|---|---|
| 1. Stress (1–4) | 2.18 (0.47) | 0.37 *** | −0.38 *** | −0.22 *** | 0.54 *** | 0.14 ** | 0.47 *** |
| 2. Perceived threat (1–4) | 3.15 (0.62) | −0.14 ** | 0.12 ** | 0.25 *** | 0.15 *** | 0.06 | |
| 3. Locus of control (1–5) | 3.68 (0.64) | 0.14 ** | −0.32 *** | −0.09 * | −0.24 *** | ||
| 4. Problem-focused coping (0–3) | 1.96 (0.44) | −0.01 | 0.30 *** | −0.21 *** | |||
| 5. Emotion-focused coping (0–3) | 0.87 (0.38) | 0.30 *** | 0.40 *** | ||||
| 6. Support-seeking (0–3) | 1.16 (0.56) | −0.12 ** | |||||
| 7. Loneliness (1–4) | 2.01 (0.44) |
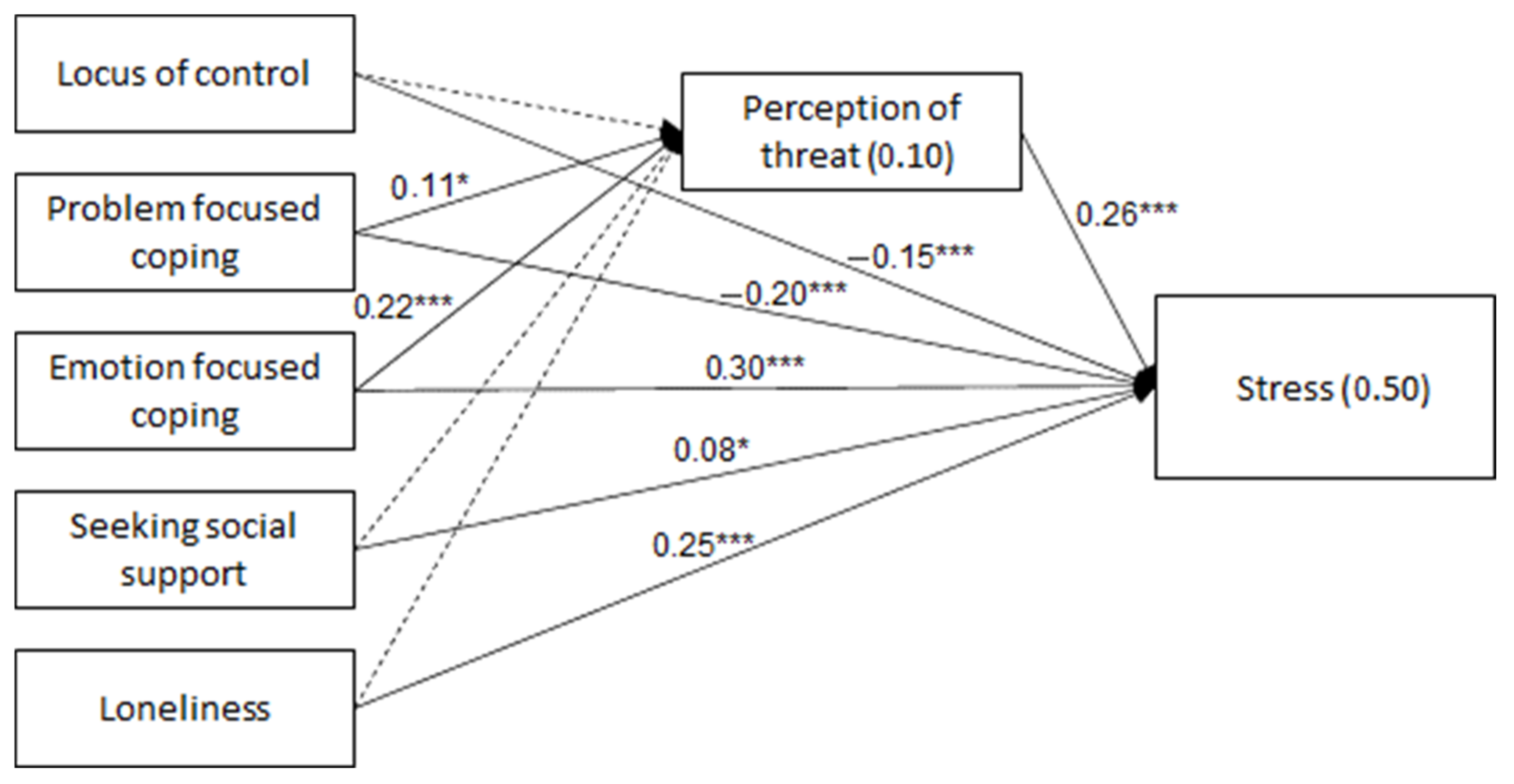
| DV (R2) | IV | β | SE | p |
|---|---|---|---|---|
| Perceived threat (0.10) | Locus of control | −0.08 | 0.05 | 0.079 |
| Problem-focused coping | 0.11 | 0.05 | 0.018 | |
| Emotion-focused coping | 0.22 | 0.05 | <0.001 | |
| Seeking social support | 0.03 | 0.05 | 0.595 | |
| Loneliness | −0.04 | 0.05 | 0.459 | |
| Experienced stress (0.50) | Locus of control | −0.15 | 0.03 | <0.001 |
| Problem-focused coping | −0.20 | 0.03 | <0.001 | |
| Emotion-focused coping | 0.30 | 0.04 | <0.001 | |
| Seeking social support | 0.08 | 0.04 | 0.040 | |
| Loneliness | 0.25 | 0.04 | <0.001 | |
| Perceived threat | 0.26 | 0.03 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali-Saleh, O.; Halperin, O. Cross-Sectional Study of Factors Influencing Perceived Threat and Stress among the Arab Minority in Israel during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 10326. https://doi.org/10.3390/ijerph191610326
Ali-Saleh O, Halperin O. Cross-Sectional Study of Factors Influencing Perceived Threat and Stress among the Arab Minority in Israel during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(16):10326. https://doi.org/10.3390/ijerph191610326
Chicago/Turabian StyleAli-Saleh, Ola, and Ofra Halperin. 2022. "Cross-Sectional Study of Factors Influencing Perceived Threat and Stress among the Arab Minority in Israel during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 16: 10326. https://doi.org/10.3390/ijerph191610326
APA StyleAli-Saleh, O., & Halperin, O. (2022). Cross-Sectional Study of Factors Influencing Perceived Threat and Stress among the Arab Minority in Israel during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(16), 10326. https://doi.org/10.3390/ijerph191610326