
Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trails



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
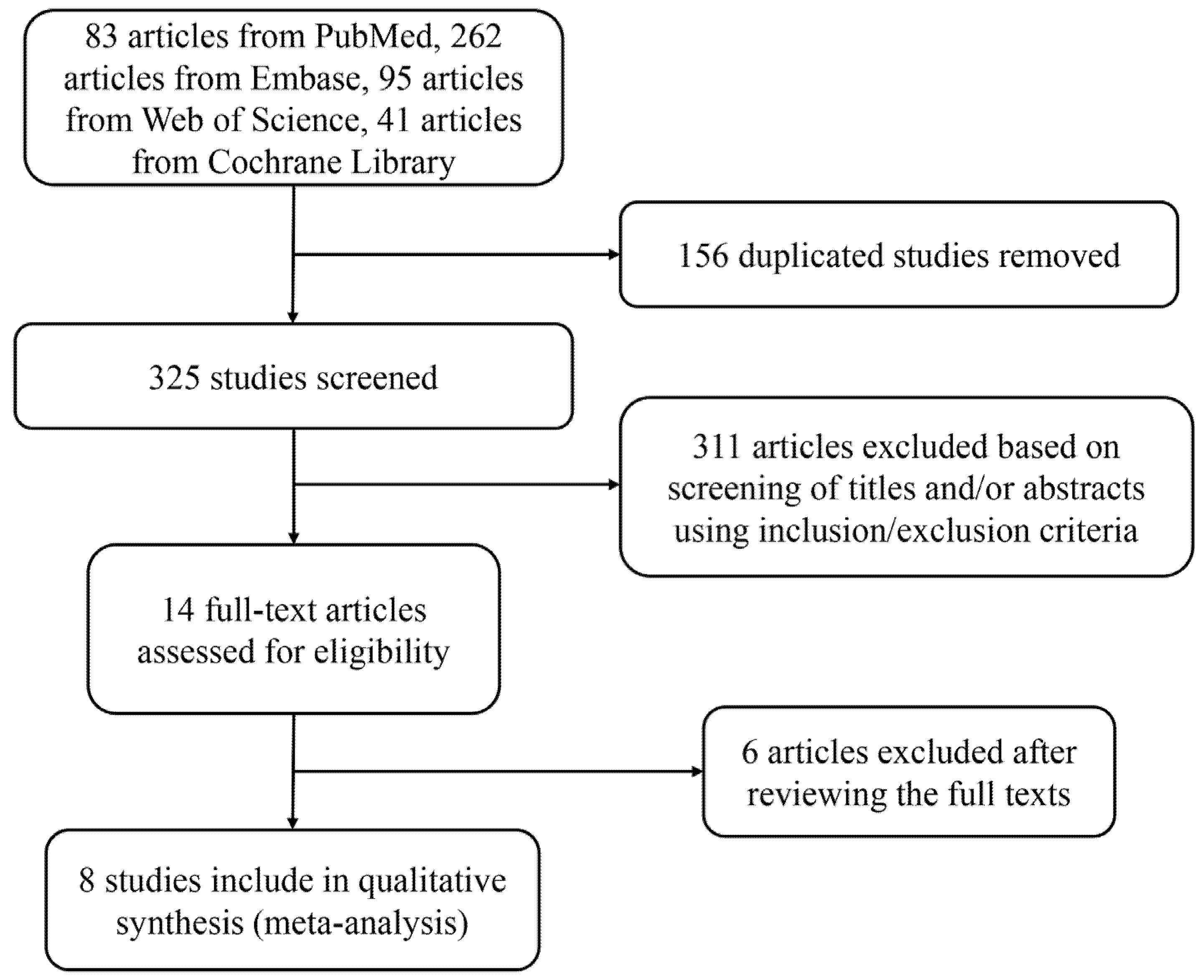
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality of the Included Trials
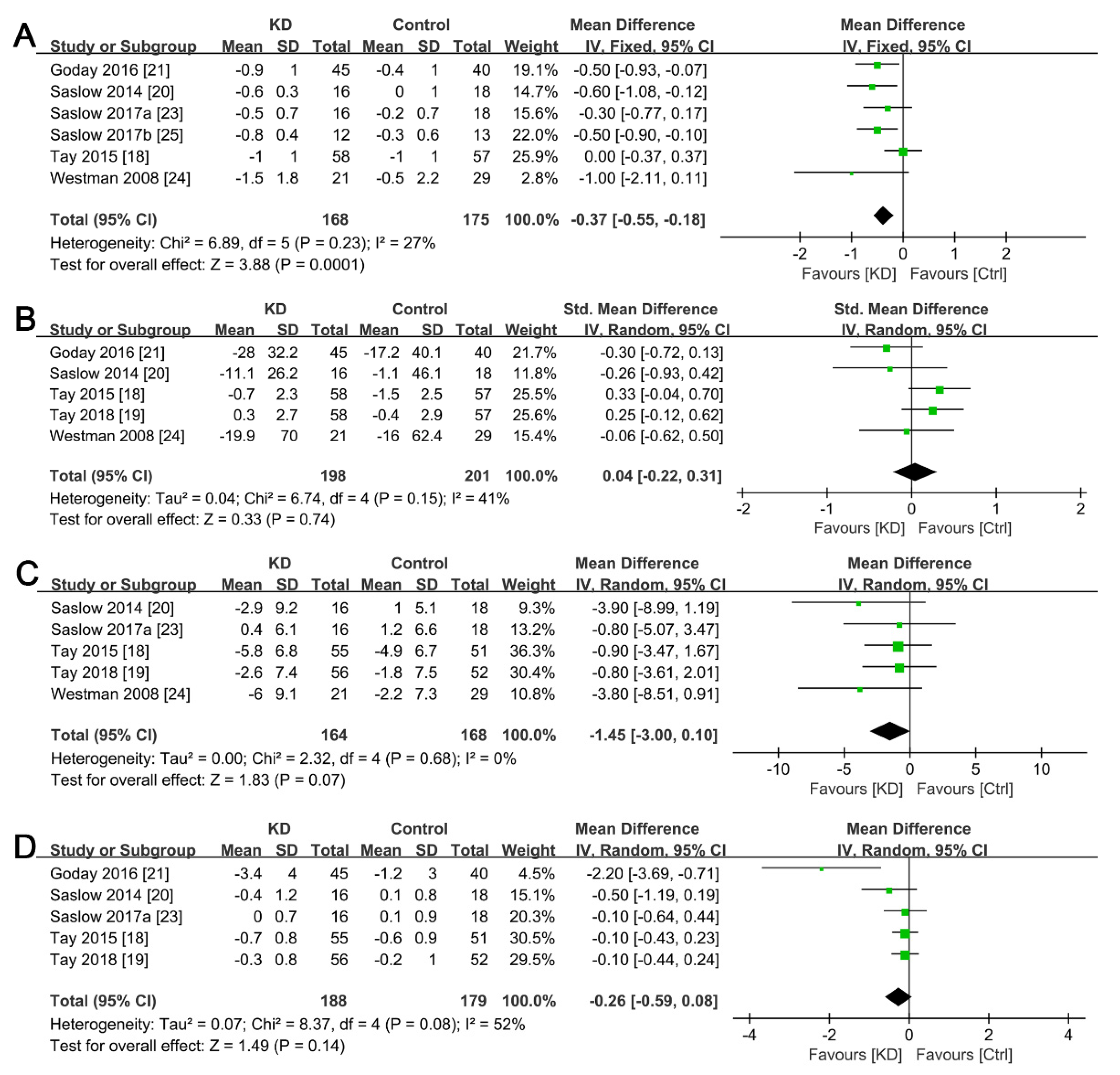
3.4. Effects of Ketogenic Diet on Body Weight Change
3.5. Effects of Ketogenic Diet on Glycemic Control
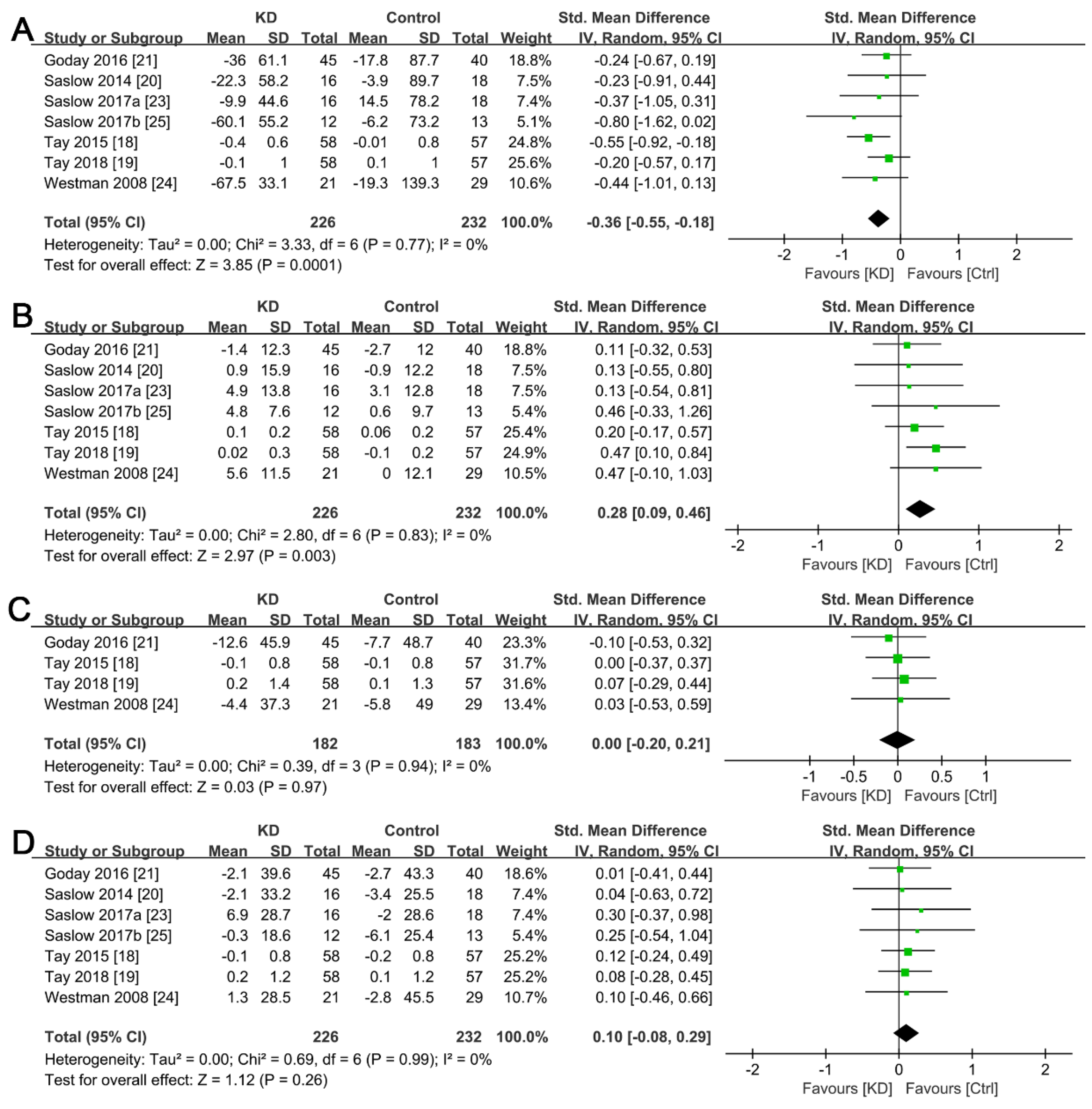
3.6. Effects of Ketogenic Diet on Lipid Profiles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, L.; Magliano, D.J.; Zimmet, P.Z. The worldwide epidemiology of type 2 diabetes mellitus—Present and future perspectives. Nat. Rev. Endocrinol. 2011, 8, 228–236. [Google Scholar] [CrossRef]
- Tripathi, B.K.; Srivastava, A.K. Diabetes mellitus: Complications and therapeutics. Med. Sci. Monit. 2006, 12, 130–147. [Google Scholar]
- Lambrinou, E.; Hansen, T.B.; Beulens, J.W. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur. J. Prev. Cardiol. 2019, 26, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampaio, L.P. Ketogenic diet for epilepsy treatment. Arq. Neuropsiquiatr. 2016, 74, 842–848. [Google Scholar] [CrossRef] [Green Version]
- Gershuni, V.M.; Yan, S.L.; Medici, V. Nutritional ketosis for weight management and reversal of metabolic syndrome. Curr. Nutr. Rep. 2018, 7, 97–106. [Google Scholar] [CrossRef]
- Shilpa, J.; Mohan, V. Ketogenic diets: Boon or bane? Indian J. Med. Res. 2018, 148, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A. Ketogenic diet for obesity: Friend or foe? Int. J. Environ. Res. Public Health 2014, 11, 2092–2107. [Google Scholar] [CrossRef] [Green Version]
- Hall, K.D.; Chen, K.Y.; Guo, J.; Lam, Y.Y.; Leibel, R.L.; Mayer, L.E.; Reitman, M.L.; Rosenbaum, M.; Smith, S.R.; Walsh, B.T.; et al. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. Am. J. Clin. Nutr. 2016, 104, 324–333. [Google Scholar] [CrossRef] [Green Version]
- Joshi, S.; Ostfeld, R.J.; McMacken, M. The ketogenic diet for obesity and diabetes-enthusiasm outpaces evidence. JAMA Intern. Med. 2019, 179, 1163–1164. [Google Scholar] [CrossRef]
- Hamdy, O.; Tasabehji, M.W.; Elseaidy, T.; Tomah, S.; Ashrafzadeh, S.; Mottalib, A. Fat versus carbohydrate-based energy-restricted diets for weight loss in patients with type 2 diabetes. Curr. Diab. Rep. 2018, 18, 128. [Google Scholar] [CrossRef] [Green Version]
- Kachur, S.; Lavie, C.J.; de Schutter, A.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular diseases. Minerv. Med. 2017, 108, 212–228. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Nan, F.; Wang, L.Y.; Jiang, H.; Chen, W.; Jiang, Y. Effects of high-protein diet on glycemic control, insulin resistance and blood pressure in type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2020, 39, 1724–1734. [Google Scholar] [CrossRef] [PubMed]
- Castellana, M.; Conte, E.; Cignarelli, A.; Perrini, S.; Giustina, A.; Giovanella, L.; Giorgino, F.; Trimboli, P. Efficacy and safety of very low calorie ketogenic diet (VLCKD) in patients with overweight and obesity: A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2020, 21, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Partsalaki, I.; Karvela, A.; Spiliotis, B.E. Metabolic impact of a ketogenic diet compared to a hypocaloric diet in obese children and adolescents. J. Pediatr. Endocrinol. Metab. 2012, 25, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Leow, Z.Z.X.; Guelfi, K.J.; Davis, E.A.; Jones, T.W.; Fournier, P.A. The glycaemic benefits of a very-low-carbohydrate ketogenic diet in adults with type 1 diabetes mellitus may be opposed by increased hypoglycaemia risk and dyslipidaemia. Diabet. Med. 2018, 35, 1258–1263. [Google Scholar] [CrossRef]
- Krebs, J.D.; Bell, D.; Hall, R.; Parry-Strong, A.; Docherty, P.D.; Clarke, K.; Chase, J.G. Improvements in glucose metabolism and insulin sensitivity with a low-carbohydrate diet in obese patients with type 2 diabetes. J. Am. Coll. Nutr. 2013, 32, 11–17. [Google Scholar] [CrossRef]
- Alsharairi, N.A. The role of short-chain fatty acids in mediating very low-calorie ketogenic diet-infant gut microbiota relationships and its therapeutic potential in obesity. Nutrients 2021, 13, 3702. [Google Scholar] [CrossRef] [PubMed]
- Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S., Jr.; Brinkworth, G.D. Comparison of low- and high-carbohydrate diets for type 2 diabetes management: A randomized trial. Am. J. Clin. Nutr. 2015, 102, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Tay, J.; Thompson, C.H.; Luscombe-Marsh, N.D.; Wycherley, T.P.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S., Jr.; Brinkworth, G.D. Effects of an energy-restricted low-carbohydrate, high unsaturated fat/low saturated fat diet versus a high-carbohydrate, low-fat diet in type 2 diabetes: A 2-year randomized clinical trial. Diabetes Obes. Metab. 2018, 20, 858–871. [Google Scholar] [CrossRef]
- Saslow, L.R.; Kim, S.; Daubenmier, J.J.; Moskowitz, J.T.; Phinney, S.D.; Goldman, V.; Murphy, E.J.; Cox, R.M.; Moran, P.; Hecht, F.M. A randomized pilot trial of a moderate carbohydrate diet compared to a very low carbohydrate diet in overweight or obese individuals with type 2 diabetes mellitus or prediabetes. PLoS ONE 2014, 9, e91027. [Google Scholar] [CrossRef] [Green Version]
- Goday, A.; Bellido, D.; Sajoux, I.; Crujeiras, A.B.; Burguera, B.; García-Luna, P.P.; Oleaga, A.; Moreno, B.; Casanueva, F.F. Short-Term safety, tolerability and efficacy of a very low-calorie-ketogenic diet interventional weight loss program versus hypocaloric diet in patients with type 2 diabetes mellitus. Nutr. Diabetes 2016, 6, e230. [Google Scholar] [CrossRef] [PubMed]
- Hussain, T.A.; Mathew, T.C.; Dashti, A.A.; Asfar, S.; Al-Zaid, N.; Dashti, H.M. Effect of low-calorie versus low-carbohydrate ketogenic diet in type 2 diabetes. Nutrition 2012, 28, 1016–1021. [Google Scholar] [CrossRef] [PubMed]
- Saslow, L.R.; Daubenmier, J.J.; Moskowitz, J.T.; Kim, S.; Murphy, E.J.; Phinney, S.D.; Ploutz-Snyder, R.; Goldman, V.; Cox, R.M.; Mason, A.E.; et al. Twelve-month outcomes of a randomized trial of a moderate-carbohydrate versus very low-carbohydrate diet in overweight adults with type 2 diabetes mellitus or prediabetes. Nutr. Diabetes 2017, 7, 304. [Google Scholar] [CrossRef] [PubMed]
- Westman, E.C.; Yancy, W.S., Jr.; Mavropoulos, J.C.; Marquart, M.; McDuffie, J.R. The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus. Nutr. Metab. 2008, 5, 36. [Google Scholar] [CrossRef] [Green Version]
- Saslow, L.R.; Mason, A.E.; Kim, S.; Goldman, V.; Ploutz-Snyder, R.; Bayandorian, H.; Daubenmier, J.; Hecht, F.M.; Moskowitz, J.T. An online intervention comparing a very low-carbohydrate ketogenic diet and lifestyle recommendations versus a plate method diet in overweight individuals with type 2 diabetes: A randomized controlled trial. J. Med. Intern. Res. 2017, 19, e36. [Google Scholar] [CrossRef] [Green Version]
- Tomiyama, A.J. Stress and obesity. Annu. Rev. Psychol. 2019, 70, 703–718. [Google Scholar] [CrossRef] [Green Version]
- Ye, J. Mechanisms of insulin resistance in obesity. Front. Med. 2013, 7, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Vidal, J. Updated review on the benefits of weight loss. Int. J. Obes. Relat. Metab. Disord. 2002, 26 (Suppl. 4), S25–S28. [Google Scholar] [CrossRef] [Green Version]
- Bueno, N.B.; de Melo, I.S.; de Oliveira, S.L.; da Rocha Ataide, T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2013, 110, 1178–1187. [Google Scholar] [CrossRef] [Green Version]
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Muscogiuri, G.; Barrea, L.; Laudisio, D.; Pugliese, G.; Salzano, C.; Savastano, S.; Colao, A. The management of very low-calorie ketogenic diet in obesity outpatient clinic: A practical guide. J. Transl. Med. 2019, 17, 356. [Google Scholar] [CrossRef] [PubMed]
- Huxley, R.; Mendis, S.; Zheleznyakov, E.; Reddy, S.; Chan, J. Body mass index, waist circumference and waist: Hip ratio as predictors of cardiovascular risk--a review of the literature. Eur. J. Clin. Nutr. 2010, 64, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbeling, C.B.; Swain, J.F.; Feldman, H.A.; Wong, W.W.; Hachey, D.L.; Garcia-Lago, E.; Ludwig, D.S. Effects of dietary composition on energy expenditure during weight-loss maintenance. JAMA 2012, 307, 2627–2634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnstone, A.M.; Horgan, G.W.; Murison, S.D.; Bremner, D.M.; Lobley, G.E. Effects of a high-protein ketogenic diet on hunger, appetite, and weight loss in obese men feeding ad libitum. Am. J. Clin. Nutr. 2008, 87, 44–55. [Google Scholar] [CrossRef] [Green Version]
- Sumithran, P.; Prendergast, L.A.; Delbridge, E.; Purcell, K.; Shulkes, A.; Kriketos, A.; Proietto, J. Ketosis and appetite-mediating nutrients and hormones after weight loss. Eur. J. Clin. Nutr. 2013, 67, 759–764. [Google Scholar] [CrossRef] [Green Version]
- Tagliabue, A.; Bertoli, S.; Trentani, C.; Borrelli, P.; Veggiotti, P. Effects of the ketogenic diet on nutritional status, resting energy expenditure, and substrate oxidation in patients with medically refractory epilepsy: A 6-month prospective observational study. Clin. Nutr. 2012, 31, 246–249. [Google Scholar] [CrossRef]
- Feinman, R.D.; Fine, E.J. Nonequilibrium thermodynamics and energy efficiency in weight loss diets. Biol. Med. Model. 2007, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Yancy, W.S.; Vernon, M.C.; Westman, E.C. A pilot trial of a low-carbohydrate, ketogenic diet in patients with type 2 diabetes. Metab. Syndr. Relat. Disord. 2003, 1, 239–243. [Google Scholar] [CrossRef]
- Bolla, A.M.; Caretto, A.; Laurenzi, A.; Scavini, M.; Piemonti, L. Low-carb and ketogenic diets in type 1 and type 2 diabetes. Nutrients 2019, 11, 962. [Google Scholar] [CrossRef] [Green Version]
- Weykamp, C. HbA1c: A review of analytical and clinical aspects. Ann. Lab. Med. 2013, 33, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Yuan, X.; Wang, J.; Yang, S.; Gao, M.; Cao, L.; Li, X.; Hong, D.; Tian, S.; Sun, C. Effect of the ketogenic diet on glycemic control, insulin resistance, and lipid metabolism in patients with T2DM: A systematic review and meta-analysis. Nutr. Diabetes 2020, 10, 38. [Google Scholar] [CrossRef] [PubMed]
- Veech, R.L. The therapeutic implications of ketone bodies: The effects of ketone bodies in pathological conditions: Ketosis, ketogenic diet, redox states, insulin resistance, and mitochondrial metabolism. Prostaglandins Leukot Essent Fat. Acids 2004, 70, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Brietzke, E.; Mansur, R.B.; Subramaniapillai, M.; Balanzá-Martínez, V.; Vinberg, M.; González-Pinto, A.; Rosenblat, J.D.; Ho, R.; McIntyre, R.S. Ketogenic diet as a metabolic therapy for mood disorders: Evidence and developments. Neurosci. Biobehav. Rev. 2018, 94, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Gupta, L.; Khandelwal, D.; Kalra, S.; Gupta, P.; Dutta, D.; Aggarwal, S. Ketogenic diet in endocrine disorders: Current perspectives. J. Postgrad. Med. 2017, 63, 242–251. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; O’Keefe, J.H. Effects of dietary fats on blood lipids: A review of direct comparison trials. Open Heart 2018, 5, e000871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dashti, H.M.; Mathew, T.C.; Khadada, M.; Al-Mousawi, M.; Talib, H.; Asfar, S.K.; Behbahani, A.I.; Al-Zaid, N.S. Beneficial effects of ketogenic diet in obese diabetic subjects. Mol. Cell Biochem. 2007, 302, 249–256. [Google Scholar] [CrossRef]
- Athyros, V.G.; Doumas, M.; Imprialos, K.P.; Stavropoulos, K.; Georgianou, E.; Katsimardou, A.; Karagiannis, A. Diabetes and lipid metabolism. Hormones 2018, 17, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, R.A.K. Dysfunctional HDL in diabetes mellitus and its role in the pathogenesis of cardiovascular disease. Mol. Cell. Biochem. 2018, 440, 167–187. [Google Scholar] [CrossRef]
- Ponce, A.J.; Galván-Salas, T.; Lerma-Alvarado, R.M.; Ruiz-Herrera, X.; Hernández-Cortés, T.; Valencia-Jiménez, R.; Cárdenas-Rodríguez, L.E.; Martínez de la Escalera, G.; Clapp, C.; Macotela, Y. Low prolactin levels are associated with visceral adipocyte hypertrophy and insulin resistance in humans. Endocrine 2020, 67, 331–343. [Google Scholar] [CrossRef]
- Karásek, D.; Vaverková, H. Diabetic dyslipidemia and microvascular complications of diabetes. Vnitr. Lek. 2018, 64, 17–24. [Google Scholar] [CrossRef]
- Lacombe, J.; Armstrong, M.E.G.; Wright, F.L.; Foster, C. The impact of physical activity and an additional behavioral risk factor on cardiovascular disease, cancer and all-cause mortality: A systematic review. BMC Public Health 2019, 19, 900. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Inclusion Criteria |
|---|---|
| Population | Population>Overweight T2DM patients |
| Intervention | Ketogenic diet; very low-carbohydrate diet |
| Comparison | Any comparisons |
| Outcomes | Body weight change, glycemic control, lipid profile |
| Study design | Randomized controlled trials |
| First Author/Year | Country | Study Design | Intervention Duration | Inclusion Criteria | Exclusion Criteria | Interventions | N | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Goday (2016) [21] | Spain | RCT | 4 months | Age: 30–65 years old; BMI: 30–35 kg/m2; T2DM | T2DM duration longer than 10 years; insulin therapy; HbA1c ≥ 9%; fasting C-peptide < 1 ng/mL. In addition: impaired renal or liver function, alcohol intake ≥ 40 g/d for men and ≥ 24 g/d for women, pregnancy, lactation, sever eating or psychiatric disorder. | VLCKD: <50 g/d carbohydrates | 45 | body weight, BMI, waist circumference, fasting plasma glucose, HbA1c, fasting insulin, HOMA-IR, total cholesterol, TG, LDL, HDL |
| LCD: a daily energy restriction of 500–1000 kcal, <30% fat, 10–20% protein, 45–60% carbohydrates. | 44 | |||||||
| Saslow (2014) [20] | USA | RCT | 3 months | Age: >18 years old; BMI: ≥25 kg/m2; T2DM (HbAc1 ≥ 6.5) or prediabetes (HbAc1 ≥ 6.0) | insulin or more than 3 glucose-lowering agents; oral glucocorticoids or weight loss medications; pregnancy; breastfeeding; weight loss surgery; vegan | LCKD: 20–50 g/d carbohydrates | 16 | HbA1c, LDL, HDL, TG, fasting glucose and insulin, HOMA-IR, body weight, BMI, waist circumference |
| MCCRD: 45–50% carbohydrates. | 18 | |||||||
| Saslow (2017a) [23] | USA | RCT | 12 months | Age: >18 years old; BMI: ≥ 25 kg/m2; T2DM (HbAc1 ≥ 6.5) or prediabetes (HbAc1 ≥ 6.0) | insulin or more than 3 glucose-lowering agents | LCKD: 20–50 g/d carbohydrates | 16 | HbA1c, LDL, HDL, TG, fasting glucose and insulin, HOMA-IR, body weight, BMI, waist circumference |
| MCCRD: 45–50% carbohydrates. | 18 | |||||||
| Saslow (2017b) [25] | USA | RCT | 32 weeks | Age ≥ 18 years old; BMI ≥ 25 kg/m2; T2DM (HbA1c 6.5–9.0) | any diabetes medication other than metformin | LCKD: 20–50 g/d carbohydrates | 12 | HbA1c, LDL, HDL, TG; body weight, BMI, waist circumference |
| American Diabetes Associations’ “Create Your Plate” diet | 13 | |||||||
| Tay (2015) [18] | Australia | RCT | 52 weeks | Age: 35–68 years old; BMI: 26–45 kg/m2; T2DM (HbA1c ≥ 7.0 and/or antidiabetic treatment) | T1DM; impaired renal or liver function; overt endocrinopathy; history of malignancy; respiratory disease, gastrointestinal disease, or CVD; pregnancy or lactation; history of or current eating disorder or smoking. | LCD: 14% carbohydrates (<50 g/d), 28% protein, 58% fat (35% monounsaturated fat and 13% polyunsaturated fat) | 58 | HbA1c, LDL, HDL, total cholesterol, TG, fasting glucose and insulin, HOMA-IR, body weight, BMI, waist circumference |
| HCD: 53% carbohydrates, 17% protein, 30% fat (15% monounsaturated fat and 9% polyunsaturated fat) | 57 | |||||||
| Tay (2018) [19] | Australia | RCT | 2 years | Age: 35–68 years old; BMI: 26–45 kg/m2; T2DM (HbA1c ≥ 7.0 and/or antidiabetic treatment) | T1DM; renal, hepatic, respiratory, gastrointestinal, or cardiovascular disease; history of malignancy; any significant endocrinopathy; pregnancy/lactation; history of or current eating disorder or smoking. | LCD: 14% carbohydrates (<50 g/d), 28% protein, 58% fat | 58 | HbA1c, LDL, HDL, total cholesterol, TG, fasting glucose and insulin, HOMA-IR, body weight, BMI, waist circumference |
| HCD: 53% carbohydrates, 17% protein, 30% fat | 57 | |||||||
| Westman (2008) [24] | USA | RCT | 24 weeks | Age: 18–65 years old; BMI: 27–50 kg/m2; T2DM > 1 year (HbA1c > 6.0); | unstable or serious medical condition; significant co-morbid illnesses such as liver disease, kidney disease, cancer; pregnancy; or nursing mothers. | LCKD: <20 g/d carbohydrates | 48 | HbA1c, fasting glucose, fasting insulin, body weight, BMI, waist circumference |
| Hussain (2012) [22] | Kuwait | RCT | 24 weeks | Age ≥ 18 years; BMI > 25 kg/m2; fasting serum glucose > 6.9 mM. | renal insufficiency, liver disease, or unstable cardiovascular disease. | LCKD: <20 g/d carbohydrates | 78 | body weight, BMI, waist circumference, HbA1c, fasting glucose, TG, total cholesterol, LDL, HDL. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, C.; Wang, M.; Liang, J.; He, G.; Chen, N. Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trails. Int. J. Environ. Res. Public Health 2022, 19, 10429. https://doi.org/10.3390/ijerph191610429
Zhou C, Wang M, Liang J, He G, Chen N. Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trails. International Journal of Environmental Research and Public Health. 2022; 19(16):10429. https://doi.org/10.3390/ijerph191610429
Chicago/Turabian StyleZhou, Chong, Meng Wang, Jiling Liang, Guomin He, and Ning Chen. 2022. "Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trails" International Journal of Environmental Research and Public Health 19, no. 16: 10429. https://doi.org/10.3390/ijerph191610429
APA StyleZhou, C., Wang, M., Liang, J., He, G., & Chen, N. (2022). Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trails. International Journal of Environmental Research and Public Health, 19(16), 10429. https://doi.org/10.3390/ijerph191610429