
Collateral Impact of COVID-19 Prevention Measures on Re-Emergence of Scarlet Fever and Pertussis in Mainland China and Hong Kong China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Collection
2.2. Statistical Analysis
3. Results
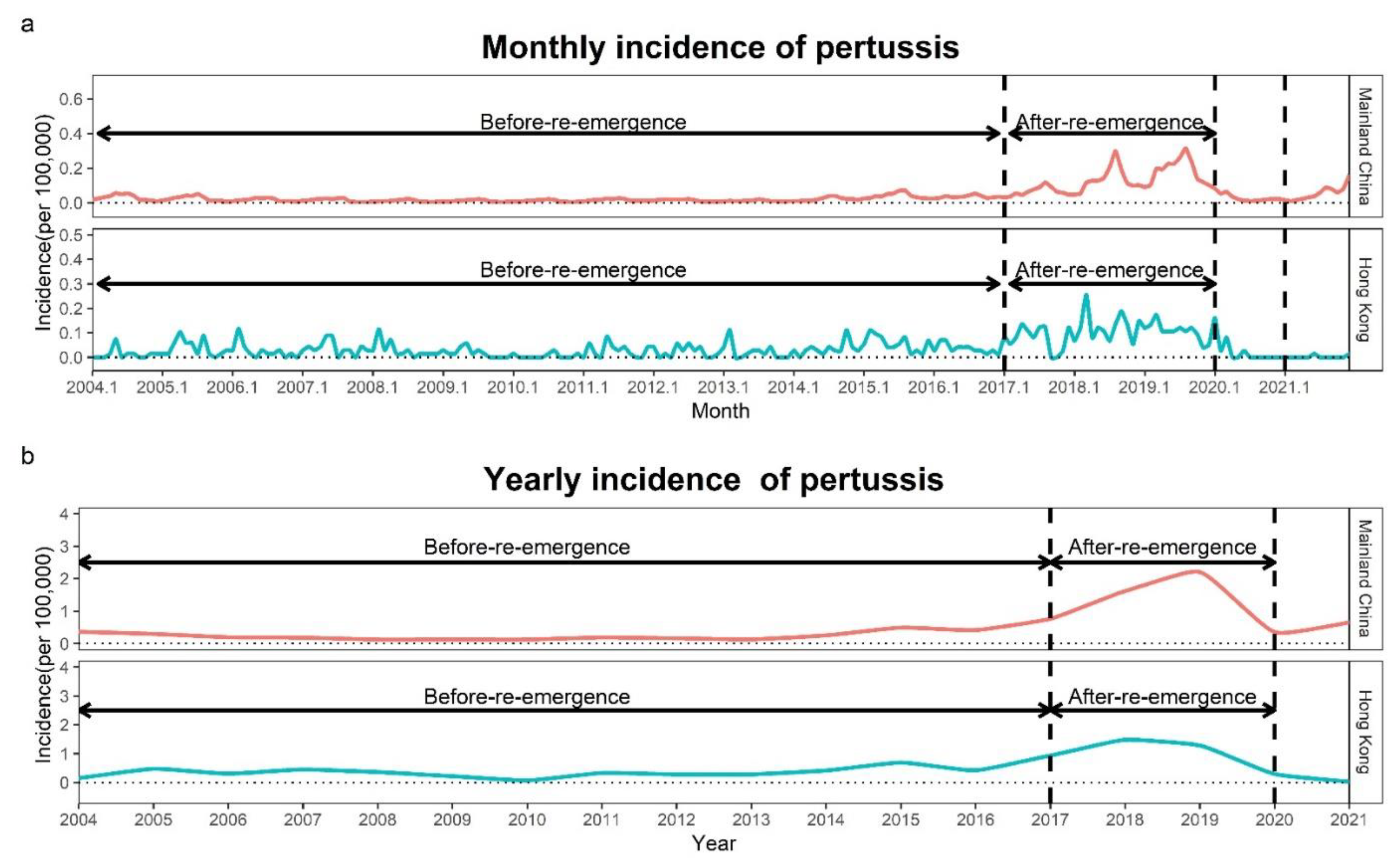
3.1. Description of the Incidence of Scarlet Fever and Pertussis in Mainland China
3.2. Description of the Incidence of Scarlet Fever and Pertussis in Hong Kong
3.3. Description of the Difference in the Incidence of Scarlet Fever and Pertussis during the Emergency and Routine Responses to COVID-19 in Mainland China in 2020
3.4. Description of the Difference in the Incidence of Scarlet Fever and Pertussis during the Emergency and Routine Responses to COVID-19 in Hong Kong in 2020
3.5. Comparison of the Observed and Predicted Incidences of Scarlet Fever and Pertussis in Mainland China
3.6. Comparison of the Observed and Predicted Incidences of Scarlet Fever and Pertussis in Hong Kong
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamagni, T.; Guy, R.; Chand, M.; Henderson, K.L.; Chalker, V.; Lewis, J.; Saliba, V.; Elliot, A.J.; Smith, G.E.; Rushton, S.; et al. Resurgence of scarlet fever in England, 2014–2016: A population-based surveillance study. Lancet Infect. Dis. 2018, 18, 180–187. [Google Scholar] [CrossRef]
- Riolo, M.; King, A.; Rohani, P. Can vaccine legacy explain the British pertussis resurgence? Vaccine 2013, 31, 5903–5908. [Google Scholar] [CrossRef] [PubMed]
- Rao, H.X.; Li, D.M.; Zhao, X.Y.; Yu, J. Spatiotemporal clustering and meteorological factors affected scarlet fever incidence in mainland China from 2004 to 2017. Sci. Total Environ. 2021, 777, 146145. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Pan, J.; Chen, M.; Zhang, T.; Li, J.; Lu, L. Seroepidemiology of pertussis in China: A population-based, cross-sectional study. Vaccine 2021, 39, 1687–1692. [Google Scholar] [CrossRef]
- Park, D.W.; Kim, S.H.; Park, J.W.; Kim, M.J.; Cho, S.J.; Park, H.J.; Jung, S.H.; Seo, M.H.; Lee, Y.S.; Kim, B.H.; et al. Incidence and characteristics of scarlet fever, South Korea, 2008–2015. Emerg. Infect. Dis. 2017, 23, 658–661. [Google Scholar] [CrossRef]
- Mungall, B.; Kim, H.; Oh, K. A systematic review of the burden of pertussis in South Korea. Hum. Vaccines Immunother. 2021, 17, 1747–1756. [Google Scholar] [CrossRef]
- Lee, C.; Cowling, B.; Lau, E. Epidemiology of reemerging scarlet fever, Hong Kong, 2005–2015. Emerg. Infect. Dis. 2017, 23, 1707. [Google Scholar] [CrossRef]
- Liu, Y.; Ding, H.; Chang, S.T.; Lu, R.; Zhong, H.; Zhao, N.; Lin, T.H.; Bao, Y.; Yap, L.; Xu, W.; et al. Exposure to air pollution and scarlet fever resurgence in China: A six-year surveillance study. Nat. Commun. 2020, 11, 4229. [Google Scholar] [CrossRef]
- World Health Organization. Pertussis vaccines: WHO position paper. Wkly. Epidemiol. Rec. 2010, 85, 385–400. [Google Scholar]
- Domenech de Cellès, M.; Magpantay, F.M.; King, A.A.; Rohani, P. The pertussis enigma: Reconciling epidemiology, immunology and evolution. Proceedings. Proc. Biol. Sci. 2016, 283, 20152309. [Google Scholar] [CrossRef]
- Zhang, Y.; Huang, H.; Liu, Y.; Gao, Z.; Shi, K.; Chen, D.; Wu, S. Incidence surveillance of pertussis based on community and analysis of its transmitted features in Tianjin. Chin. J. Vaccines Immun. 2011, 17, 209–211+257. [Google Scholar]
- Zhang, Y.; Bambrick, H.; Mengersen, K.; Tong, S.; Feng, L.; Zhang, L.; Liu, G.; Xu, A.; Hu, W. Resurgence of pertussis infections in Shandong, China: Space-time cluster and trend analysis. Am. J. Trop. Med. Hyg. 2019, 100, 1342–1354. [Google Scholar] [CrossRef]
- Liu, Z.; Liu, S.; Shu, Y.; Yang, Z.; Peng, B.; Xu, H.; Li, Q.; Luo, Z.; Dai, J.; Liu, E. Severe Bordetella pertussis infection and vaccine issue in Chongqing, from 2012 to 2018. Int. J. Infect. Dis. 2019, 84, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Scientific Committee on Vaccine Preventable Diseases. Consensus Recommendations on Pertussis Vaccination for Pregnant Women in Hong Kong. 2020. Available online: https://www.chp.gov.hk/files/pdf/recommendations_on_pertussis_vaccination_for_pregnant_women_in_hk_formatted.pdf (accessed on 6 March 2022).
- Commission WMH. Notification for the Unknown Cause of Viral Pneumonia in Wuhan by Wuhan Municipal Health Commission. 2020. Available online: http://wjw.hubei.gov.cn/bmdt/dtyw/202001/t20200105_1903301.shtml (accessed on 8 December 2021).
- Choi, E.; Hui, B.; Wan, E. Depression and anxiety in Hong Kong during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 20 March 2021).
- Ren, R.; Zhang, Y.; Li, Q.; McGoogan, J.M.; Feng, Z.; Gao, G.F.; Wu, Z. Asymptomatic SARS-CoV-2 infections among persons entering China from 16 April to 12 October 2020. JAMA 2021, 325, 489–492. [Google Scholar] [CrossRef]
- Government of the Hong Kong Special Administrative Region. The Chief Executive Has Raised the Response Level for Novel Coronavirus Infections to Emergency. 2020. Available online: https://sc.isd.gov.hk/TuniS/www.info.gov.hk/gia/general/202001/26/P2020012600013.htm (accessed on 6 March 2022).
- News.gov.hk. Public Services Will Resume Gradually Next Monday. 2020. Available online: https://sc.news.gov.hk/TuniS/www.news.gov.hk/chi/2020/04/20200429/20200429_114534_469.html?type=category&name=covid19&tl=t (accessed on 6 March 2022).
- Liu, Q.; Lu, P.; Shen, Y.; Li, C.; Wang, J.; Zhu, L.; Lu, W.; Martinez, L. Collateral impact of the Coronavirus Disease 2019 (COVID-19) pandemic on tuberculosis control in Jiangsu Province, China. Clin. Infect. Dis. 2021, 73, 542–544. [Google Scholar] [CrossRef]
- Hu, C.Y.; Tang, Y.W.; Su, Q.M.; Lei, Y.; Cui, W.S.; Zhang, Y.Y.; Zhou, Y.; Li, X.Y.; Wang, Z.F.; Zhao, Z.X. Public health measures during the COVID-19 pandemic reduce the spread of other respiratory infectious diseases. Front. Public Health 2021, 9, 771638. [Google Scholar] [CrossRef]
- Rana, M.S.; Usman, M.; Alam, M.M.; Ikram, A.; Salman, M.; Zaidi, S.; Umair, M.; Qadir, M. Impact of COVID-19 preventive measures on other infectious and non-infectious respiratory diseases in Pakistan. J. Infect. 2021, 82, e31–e32. [Google Scholar] [CrossRef]
- Feng, L.; Zhang, T.; Wang, Q.; Xie, Y.; Peng, Z.; Zheng, J.; Qin, Y.; Zhang, M.; Lai, S.; Wang, D.; et al. Impact of COVID-19 outbreaks and interventions on influenza in China and the United States. Nat. Commun. 2021, 12, 3249. [Google Scholar] [CrossRef]
- Huang, Q.S.; Wood, T.; Jelley, L.; Jennings, T.; Jefferies, S.; Daniells, K.; Nesdale, A.; Dowell, T.; Turner, N.; Campbell-Stokes, P.; et al. Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat. Commun. 2021, 12, 1001. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ueda, P. Seasonal influenza activity during the SARS-CoV-2 outbreak in Japan. JAMA 2020, 323, 1969–1971. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, H.; Song, K.H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H.B. Impact of public health interventions on seasonal influenza activity during the COVID-19 outbreak in Korea. Clin. Infect. Dis. 2021, 73, e132–e140. [Google Scholar] [CrossRef] [PubMed]
- Brockwell, P.; Davis, R. Introduction to Time Series and Forecasting; Springer: New York, NY, USA, 1996. [Google Scholar]
- Liu, J.; Zhang, L.; Yan, Y.; Zhou, Y.; Yin, P.; Qi, J.; Wang, L.; Pan, J.; You, J.; Yang, J.; et al. Excess mortality in Wuhan city and other parts of China during the three months of the COVID-19 outbreak: Findings from nationwide mortality registries. BMJ 2021, 372, n415. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Wu, H.; Wu, C.; Lu, Q.; Lin, J. Surveillance for notifiable communicable diseases in the context of emergency response to COVID-19 in Zhejiang. Dis. Surveill. 2020, 35, 746–752. [Google Scholar] [CrossRef]
- Huang, S.; Zhang, P.; Hong, X.; Zhong, C. Characteristics of public health emergencies at schools in Hubei Province, 2004–2013. Chin. J. Sch. Health 2015, 36, 113–115+118. [Google Scholar] [CrossRef]
- Zhuang, Z.; Cao, P.; Zhao, S.; Han, L.; He, D.; Yang, L. The shortage of hospital beds for COVID-19 and non-COVID-19 patients during the lockdown of Wuhan, China. Ann. Transl. Med. 2021, 9, 200. [Google Scholar] [CrossRef]
- Duan, Y.; Yang, L.J.; Zhang, Y.J.; Huang, X.L.; Pan, G.X.; Wang, J. Effects of meteorological factors on incidence of scarlet fever during different periods in different districts of China. Sci. Total Environ. 2017, 581–582, 19–24. [Google Scholar] [CrossRef]
- Güriş, D.; Strebel, P.M.; Bardenheier, B.; Brennan, M.; Tachdjian, R.; Finch, E.; Wharton, M.; Livengood, J.R. Changing epidemiology of pertussis in the United States: Increasing reported incidence among adolescents and adults, 1990–1996. Clin. Infect. Dis. 1999, 28, 1230–1237. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diseases | 2021 vs. 2020 | 2021 vs. before-COVID-19 Stage | 2020 vs. before-COVID-19 Stage | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2021 | 2020 | Changes (%) | p Value | 2021 | Before-Re-Emergence | Changes (%) | p Value | 2020 | Before-Re-Emergence | Changes (%) | p Value | |
| Scarlet Fever | 2.10 | 1.23 | 70.60 | <0.001 | 2.10 | 1.92 | 9.68 | <0.001 | 1.23 | 1.92 | −35.71 | <0.001 |
| Pertussis | 0.65 | 0.36 | 82.51 | <0.001 | 0.65 | 0.23 | 179.12 | <0.001 | 0.36 | 0.23 | 52.94 | <0.001 |
| 2021 | 2020 | Changes (%) | p Value | 2021 | After-Re-Emergence | Changes (%) | p Value | 2020 | After-Re-Emergence | Changes (%) | p Value | |
| Scarlet Fever | 2.10 | 1.23 | 70.60 | <0.001 | 2.10 | 4.58 | −54.15 | <0.001 | 1.23 | 4.58 | −73.13 | <0.001 |
| Pertussis | 0.65 | 0.36 | 82.51 | <0.001 | 0.65 | 1.53 | −57.35 | <0.001 | 0.36 | 1.53 | −76.63 | <0.001 |
| Diseases | 2021 vs. 2020 | 2021 vs. before-COVID-19 stage | 2020 vs. before-COVID-19 stage | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2021 | 2020 | Changes (%) | p Value | 2021 | Before-Re-Emergence | Changes (%) | p Value | 2020 | Before-Re-Emergence | Changes (%) | p Value | |
| Scarlet Fever | 1.20 | 3.50 | −65.63 | <0.001 | 1.20 | 2.70 | −55.47 | <0.001 | 3.50 | 2.70 | 29.58 | 0.006 |
| Pertussis | 0.03 | 0.29 | −90.80 | <0.001 | 0.03 | 0.34 | −92.09 | <0.001 | 0.29 | 0.34 | −13.96 | 0.611 |
| 2021 | 2020 | Changes (%) | p Value | 2021 | After-Re-Emergence | Changes (%) | p Value | 2020 | After-Re-Emergence | Changes (%) | p Value | |
| Scarlet Fever | 1.20 | 3.50 | −65.63 | <0.001 | 1.20 | 21.48 | −94.40 | <0.001 | 3.50 | 21.48 | −83.70 | <0.001 |
| Pertussis | 0.03 | 0.29 | −90.80 | <0.001 | 0.03 | 1.23 | −97.80 | <0.001 | 0.29 | 1.23 | −76.10 | <0.001 |
| Diseases | Emergency Stage (January to April 2020) | Routine Stage (May to December 2020) | 2021 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mainland China | ||||||||||||
| Observed | Predicted | Changes (%) | p Value | Observed | Predicted | Changes (%) | p Value | Observed | Predicted | Changes (%) | p Value | |
| Scarlet Fever | 0.14 | 0.51 | −72.40 | <0.001 | 0.08 | 0.67 | −87.45 | <0.001 | 0.18 | 0.68 | −74.17 | <0.001 |
| Pertussis | 0.06 | 0.18 | −67.61 | <0.001 | 0.02 | 0.27 | −94.10 | <0.001 | 0.05 | 0.31 | −82.59 | <0.001 |
| Hong Kong | ||||||||||||
| Observed | Predicted | Changes (%) | p Value | Observed | Predicted | Changes (%) | p Value | Observed | Predicted | Changes (%) | p Value | |
| Scarlet Fever | 0.63 | 2.27 | −72.17 | <0.001 | 0.12 | 2.05 | −94.05 | <0.001 | 0.10 | 2.17 | −95.38 | <0.001 |
| Pertussis | 0.07 | 0.12 | −41.95 | 0.327 | 0.00 | 0.11 | −96.89 | 0.007 | 0.00 | 0.12 | −98.16 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, Y.; Ma, C.; Guo, X.; Pan, J.; Xu, W.; Liu, S. Collateral Impact of COVID-19 Prevention Measures on Re-Emergence of Scarlet Fever and Pertussis in Mainland China and Hong Kong China. Int. J. Environ. Res. Public Health 2022, 19, 9909. https://doi.org/10.3390/ijerph19169909
He Y, Ma C, Guo X, Pan J, Xu W, Liu S. Collateral Impact of COVID-19 Prevention Measures on Re-Emergence of Scarlet Fever and Pertussis in Mainland China and Hong Kong China. International Journal of Environmental Research and Public Health. 2022; 19(16):9909. https://doi.org/10.3390/ijerph19169909
Chicago/Turabian StyleHe, Yiran, Chenjin Ma, Xiangyu Guo, Jinren Pan, Wangli Xu, and Shelan Liu. 2022. "Collateral Impact of COVID-19 Prevention Measures on Re-Emergence of Scarlet Fever and Pertussis in Mainland China and Hong Kong China" International Journal of Environmental Research and Public Health 19, no. 16: 9909. https://doi.org/10.3390/ijerph19169909
APA StyleHe, Y., Ma, C., Guo, X., Pan, J., Xu, W., & Liu, S. (2022). Collateral Impact of COVID-19 Prevention Measures on Re-Emergence of Scarlet Fever and Pertussis in Mainland China and Hong Kong China. International Journal of Environmental Research and Public Health, 19(16), 9909. https://doi.org/10.3390/ijerph19169909