
Guided Endodontics as a Personalized Tool for Complicated Clinical Cases

 ,
,
Abstract
: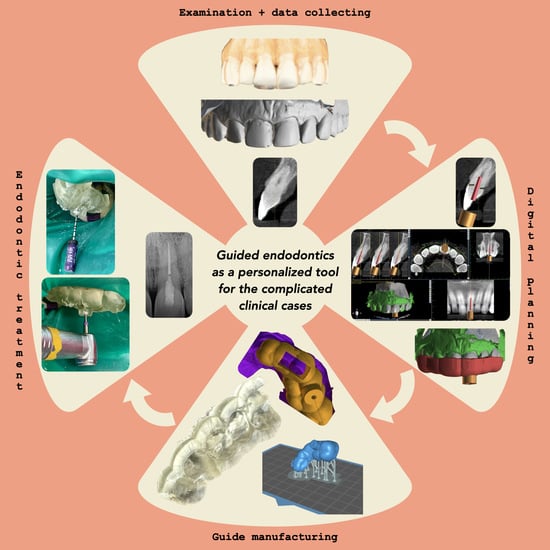
1. Introduction
2. Case Series Presentation
2.1. Post-Traumatic Pulp Canal Obliteration (PCO)
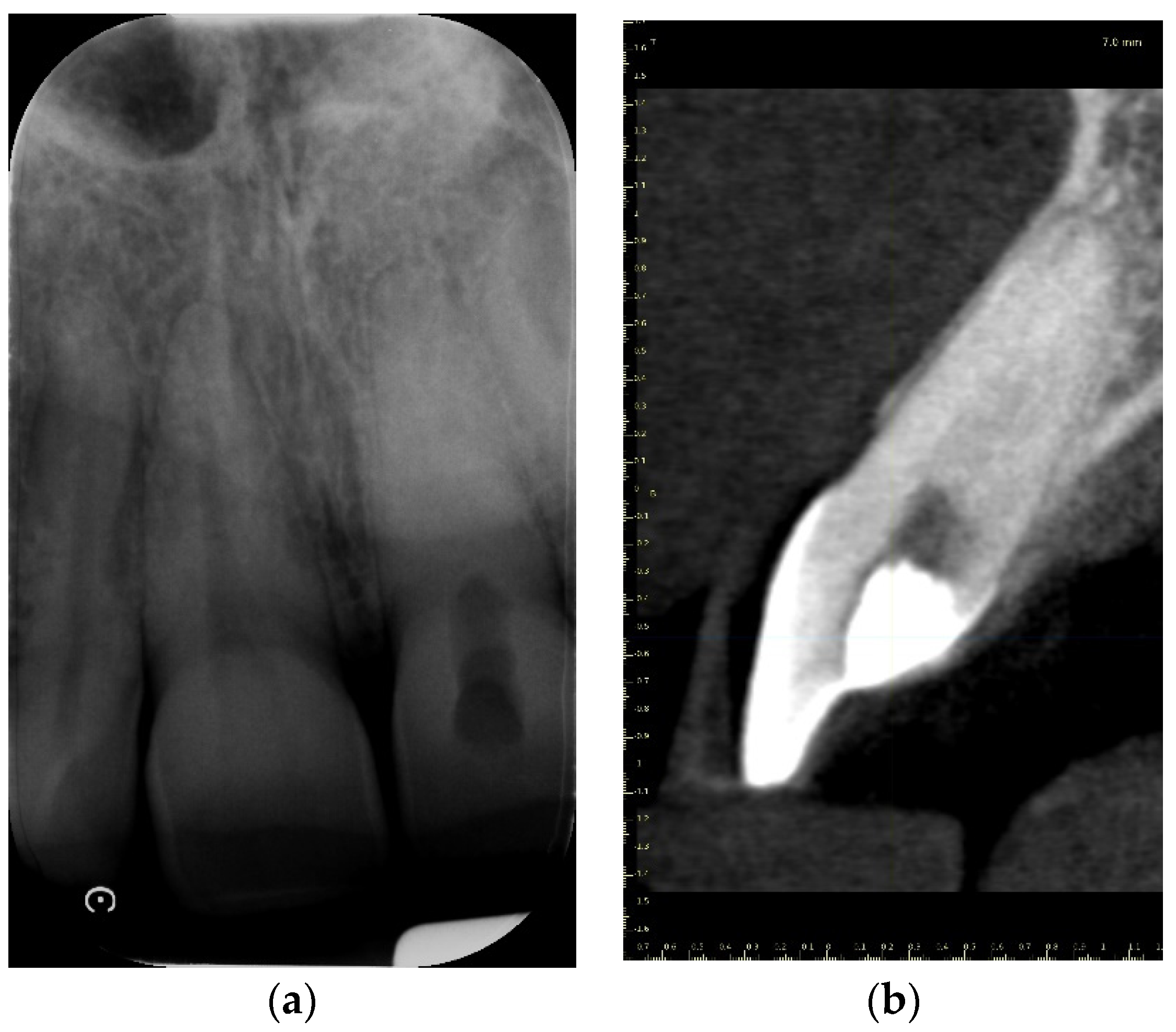
2.1.1. Case Report—Patient A: Symptomatic Pulp Necrosis after Trauma
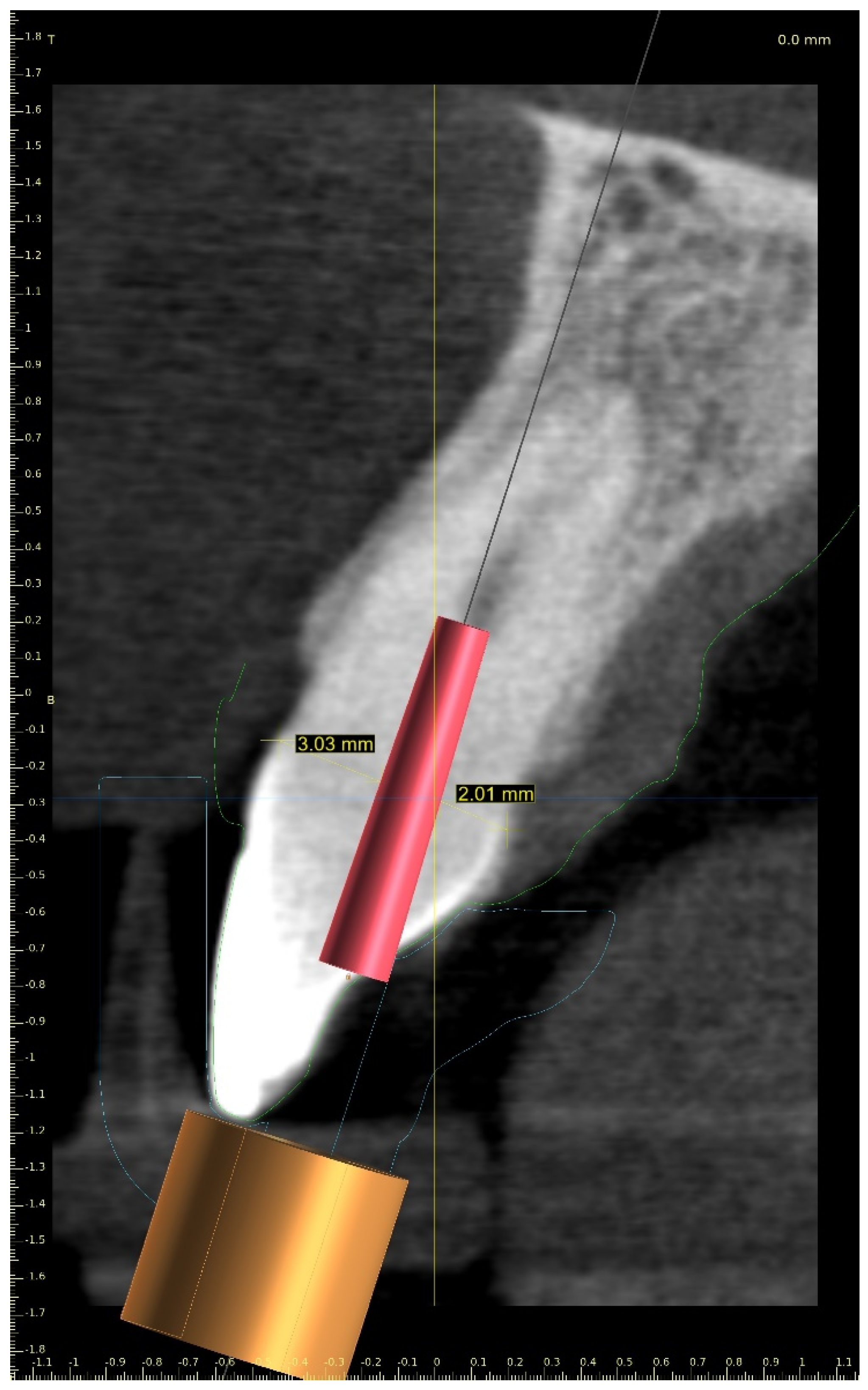
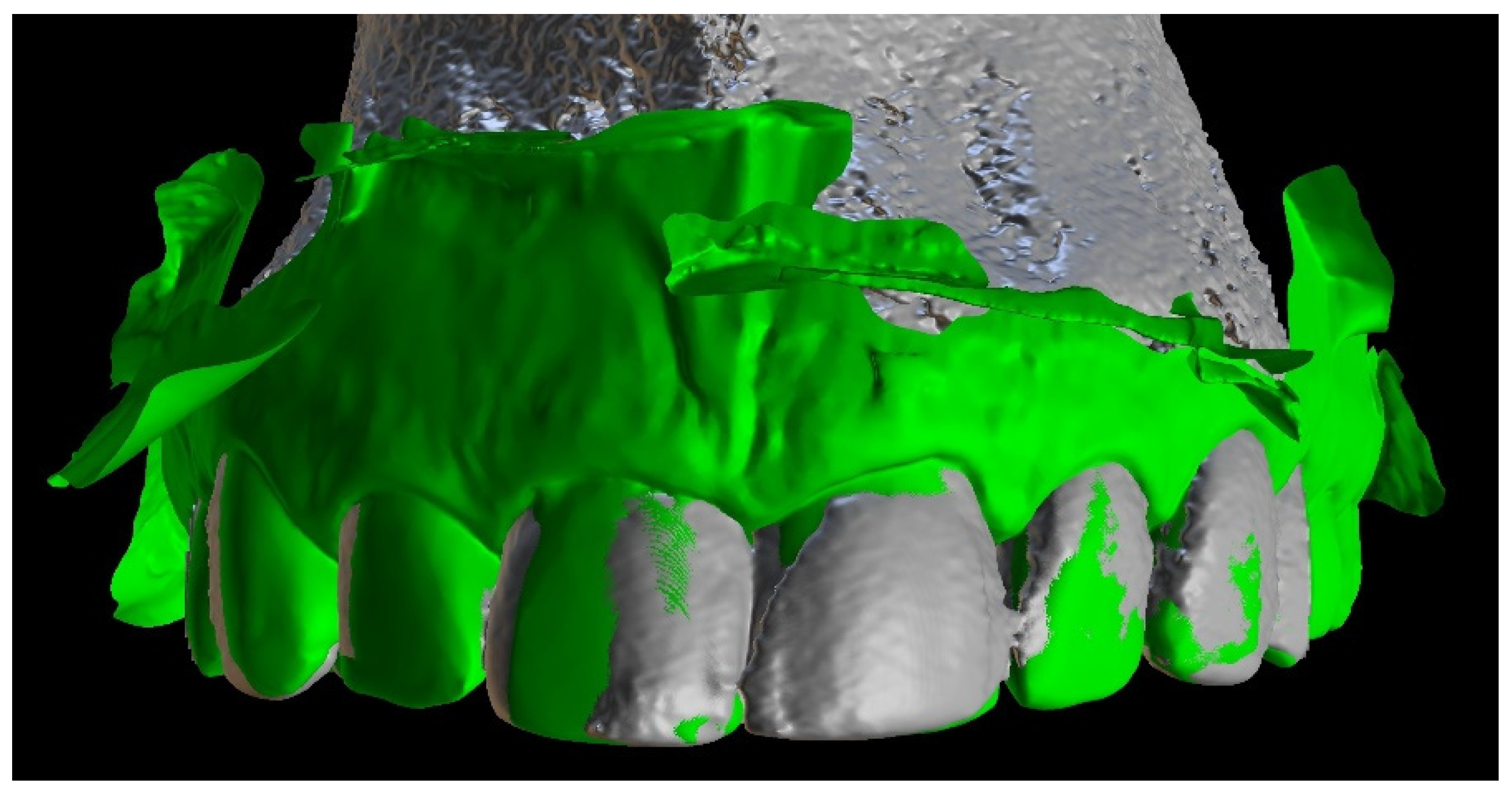
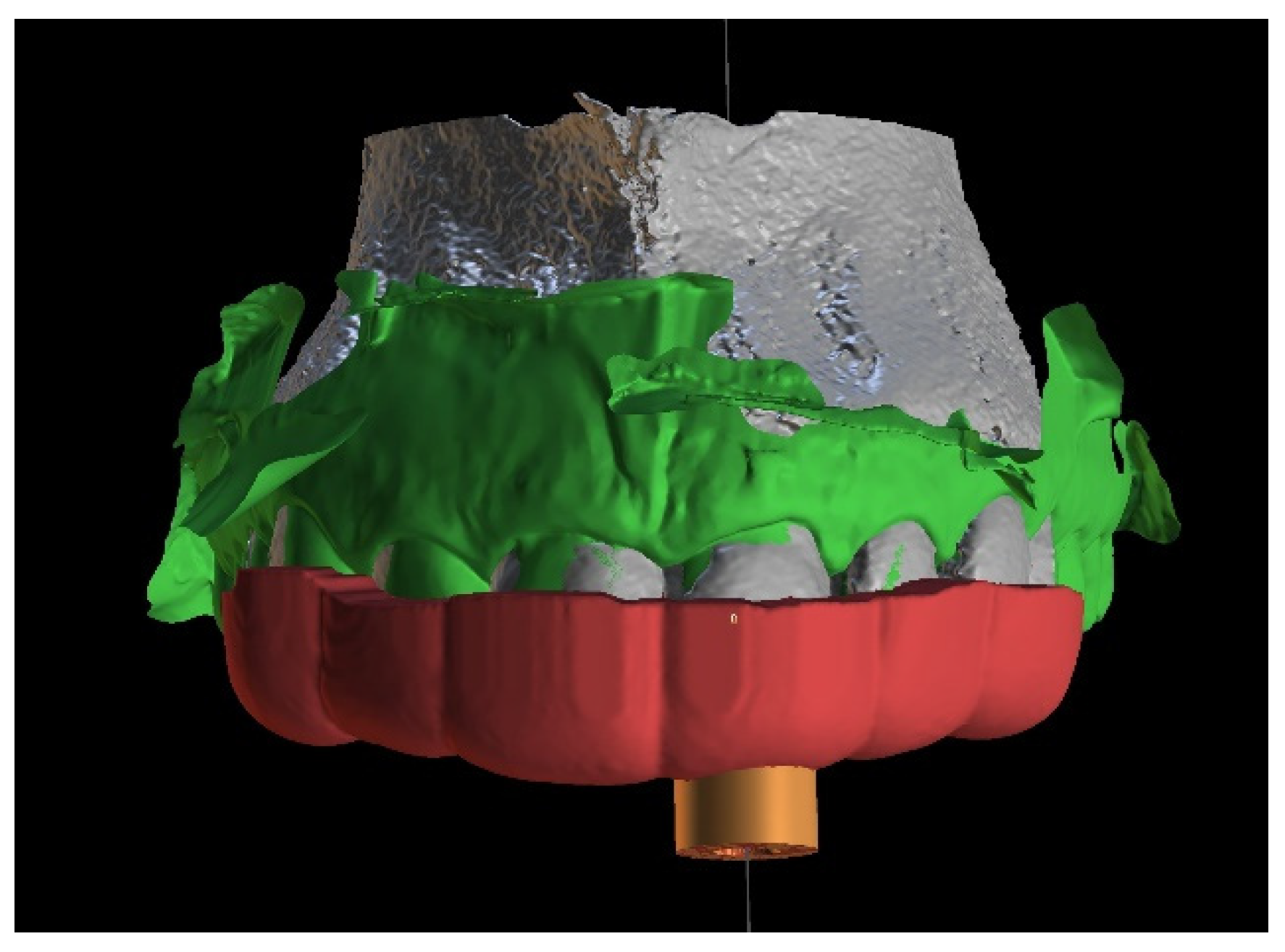
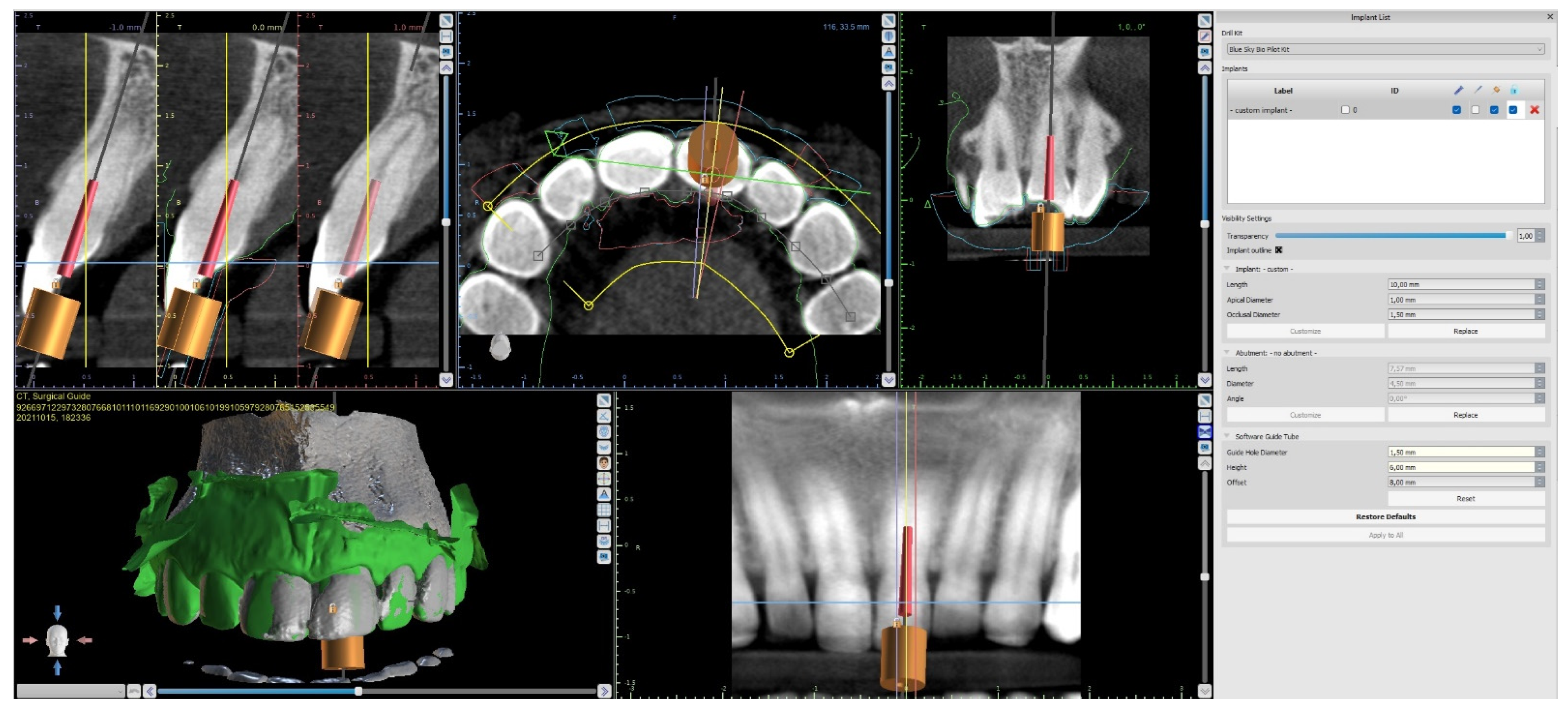
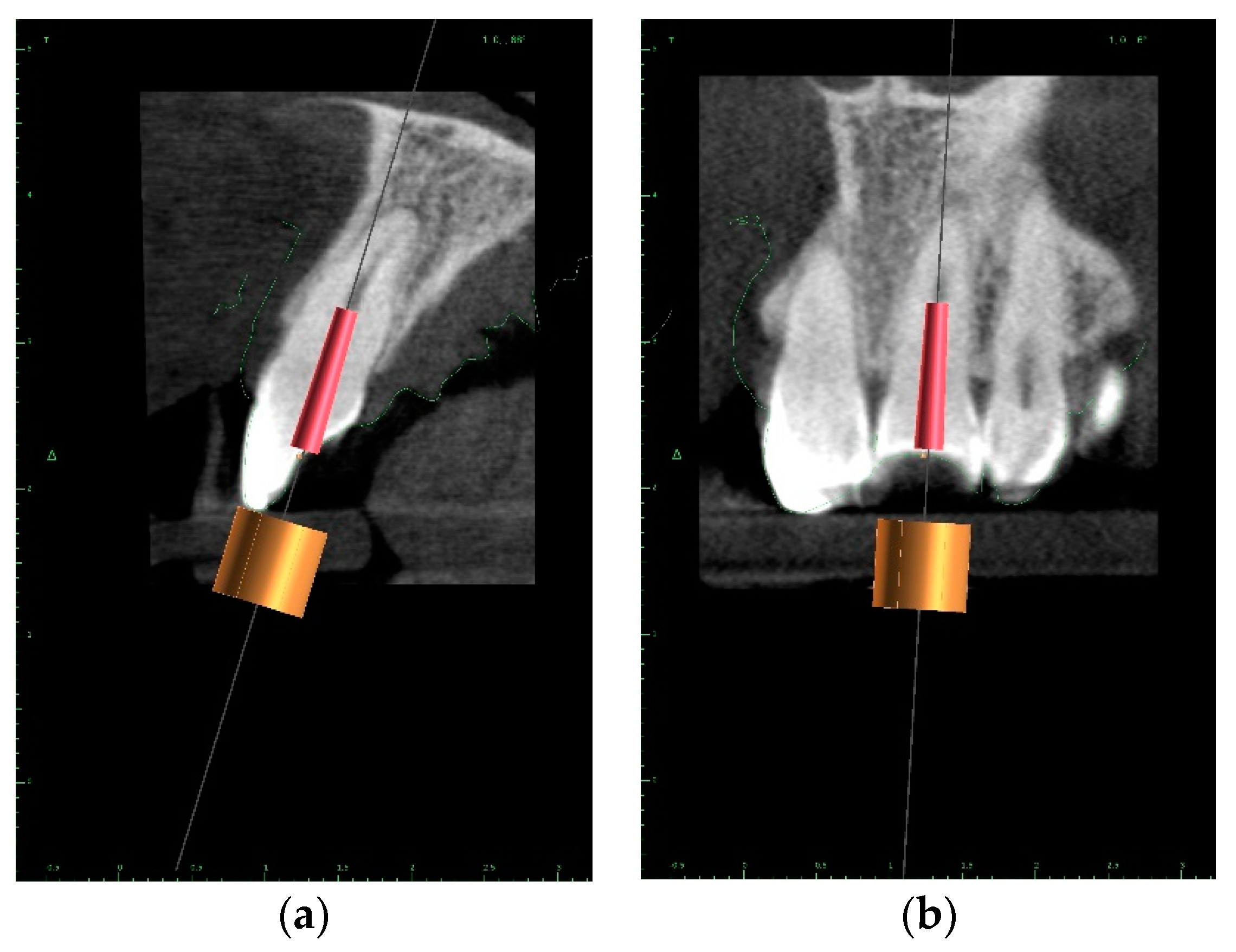
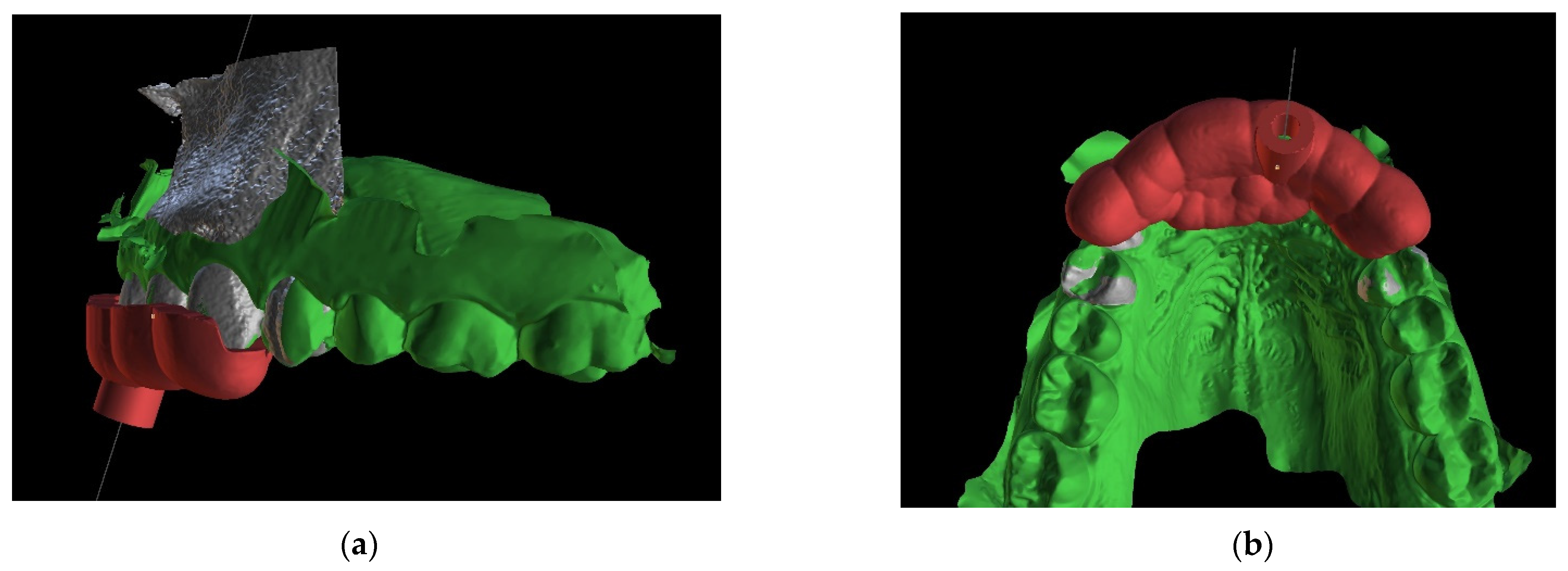
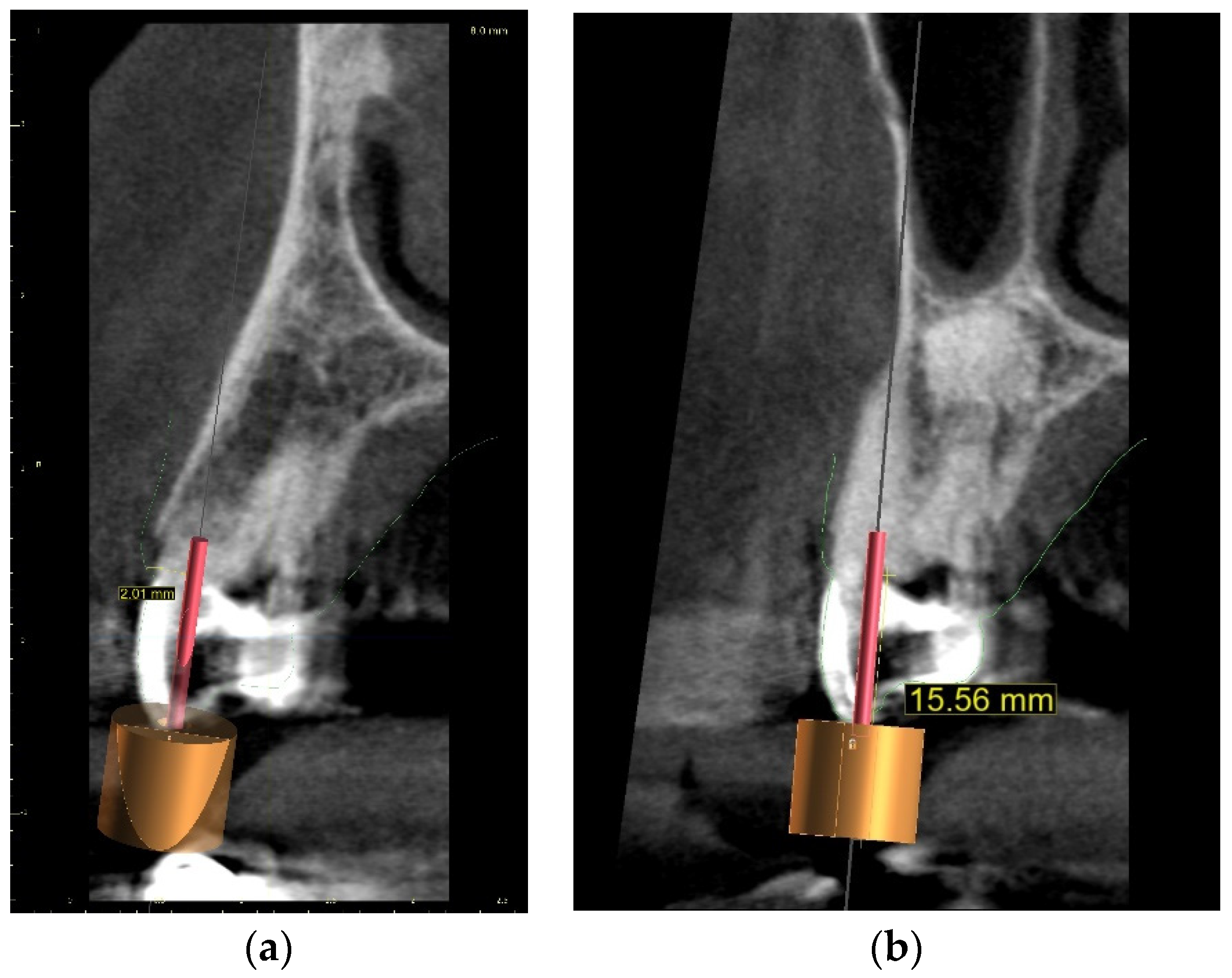
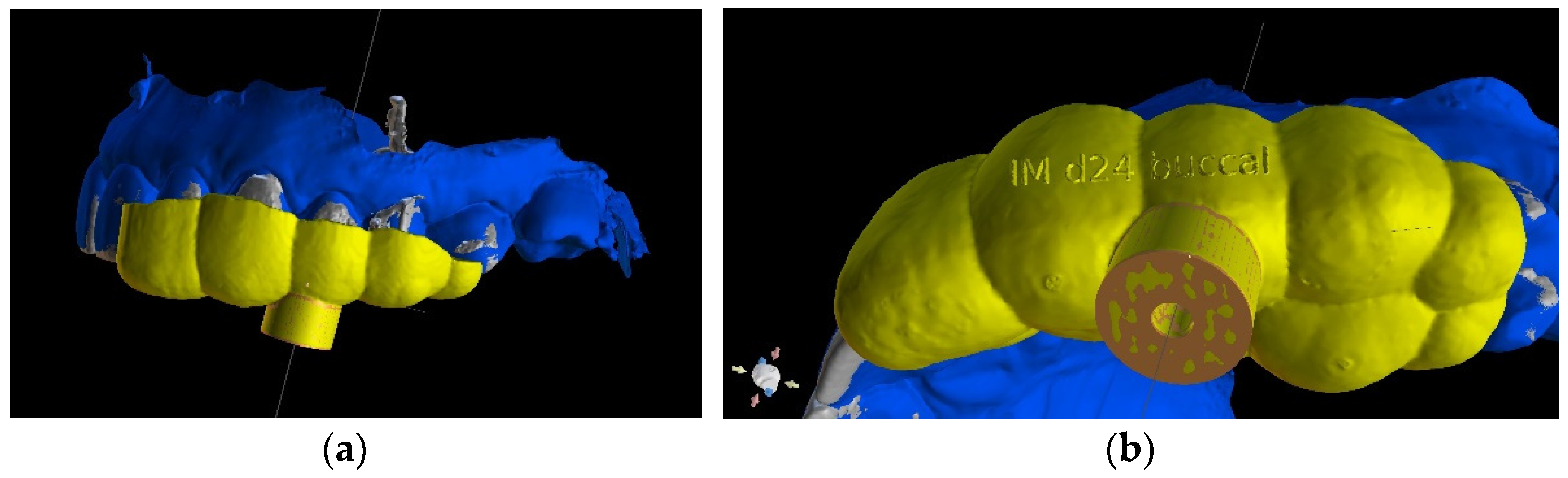
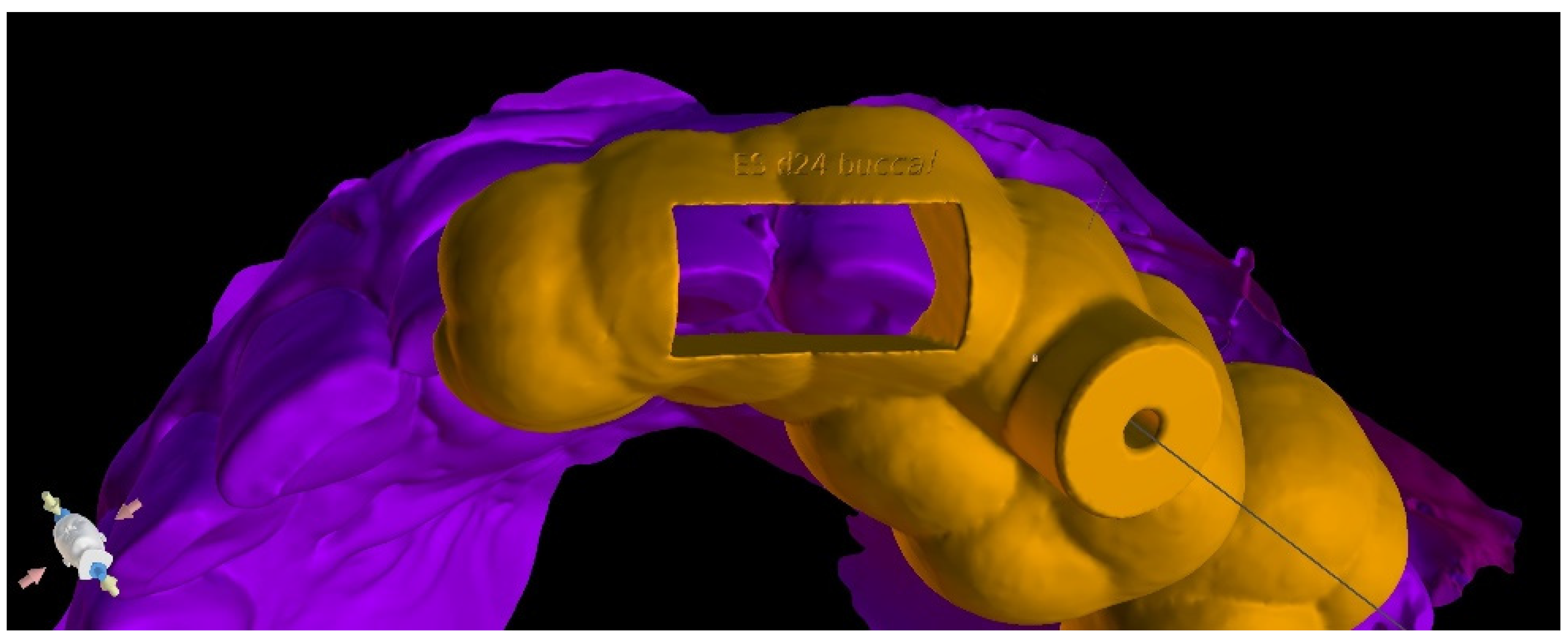
Three-Dimensional Treatment Plan
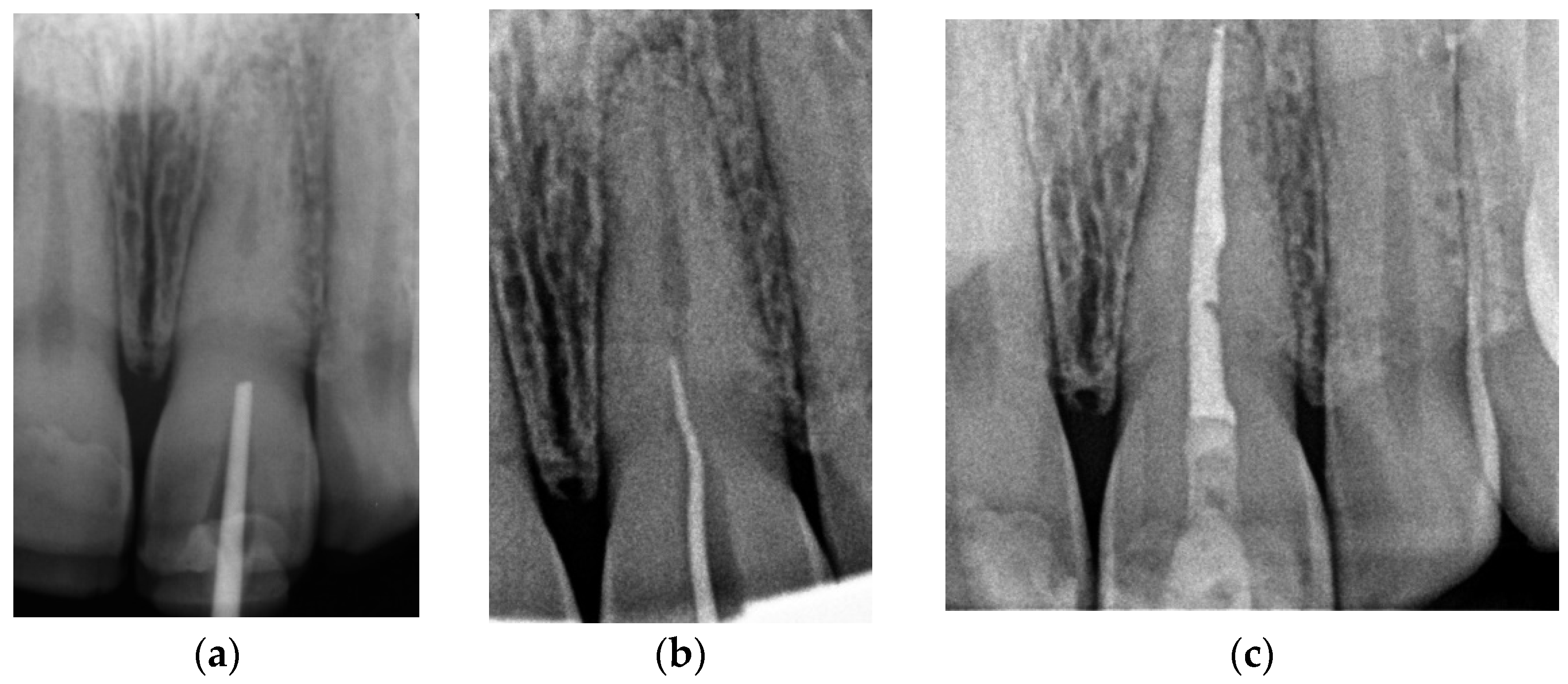
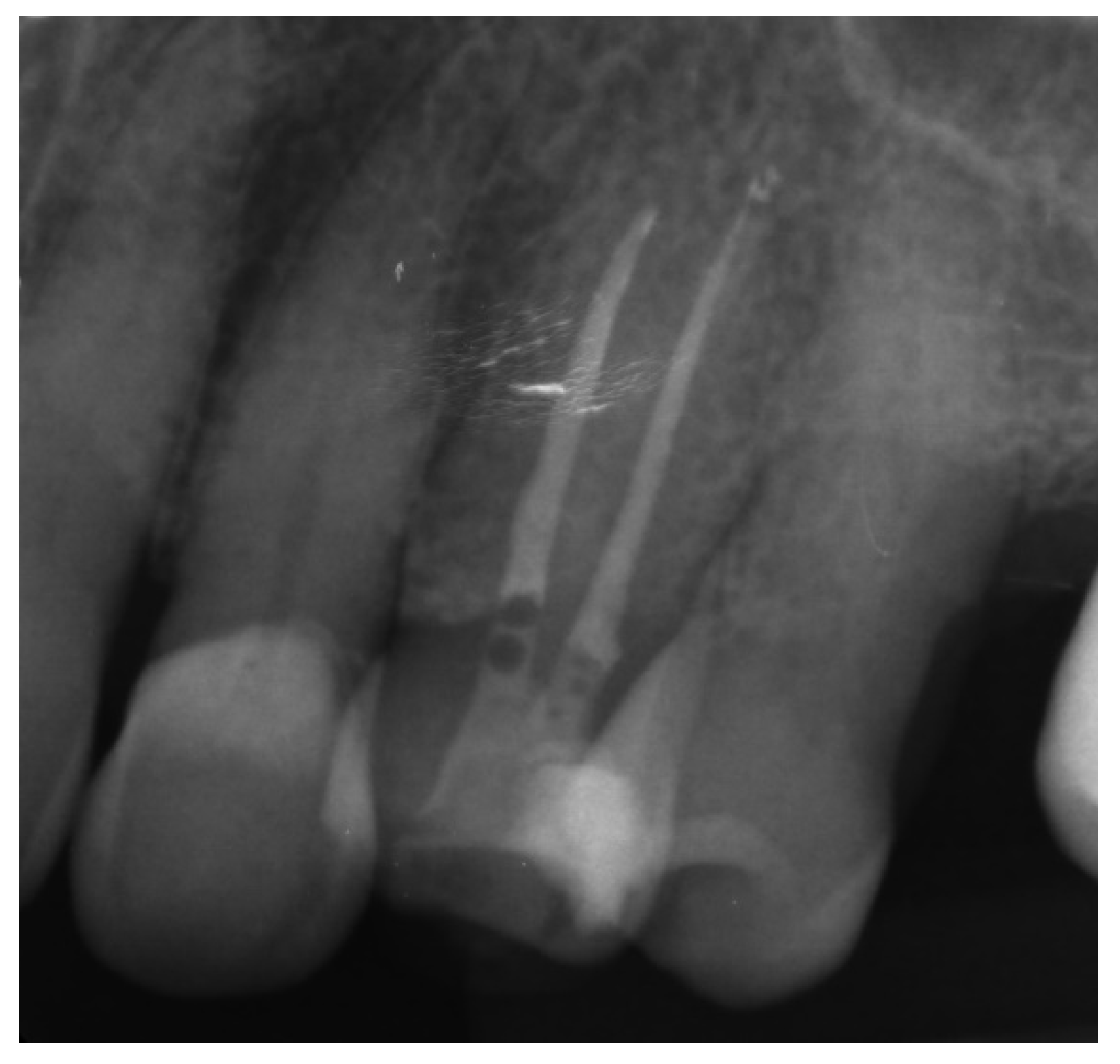
Canal Treatment
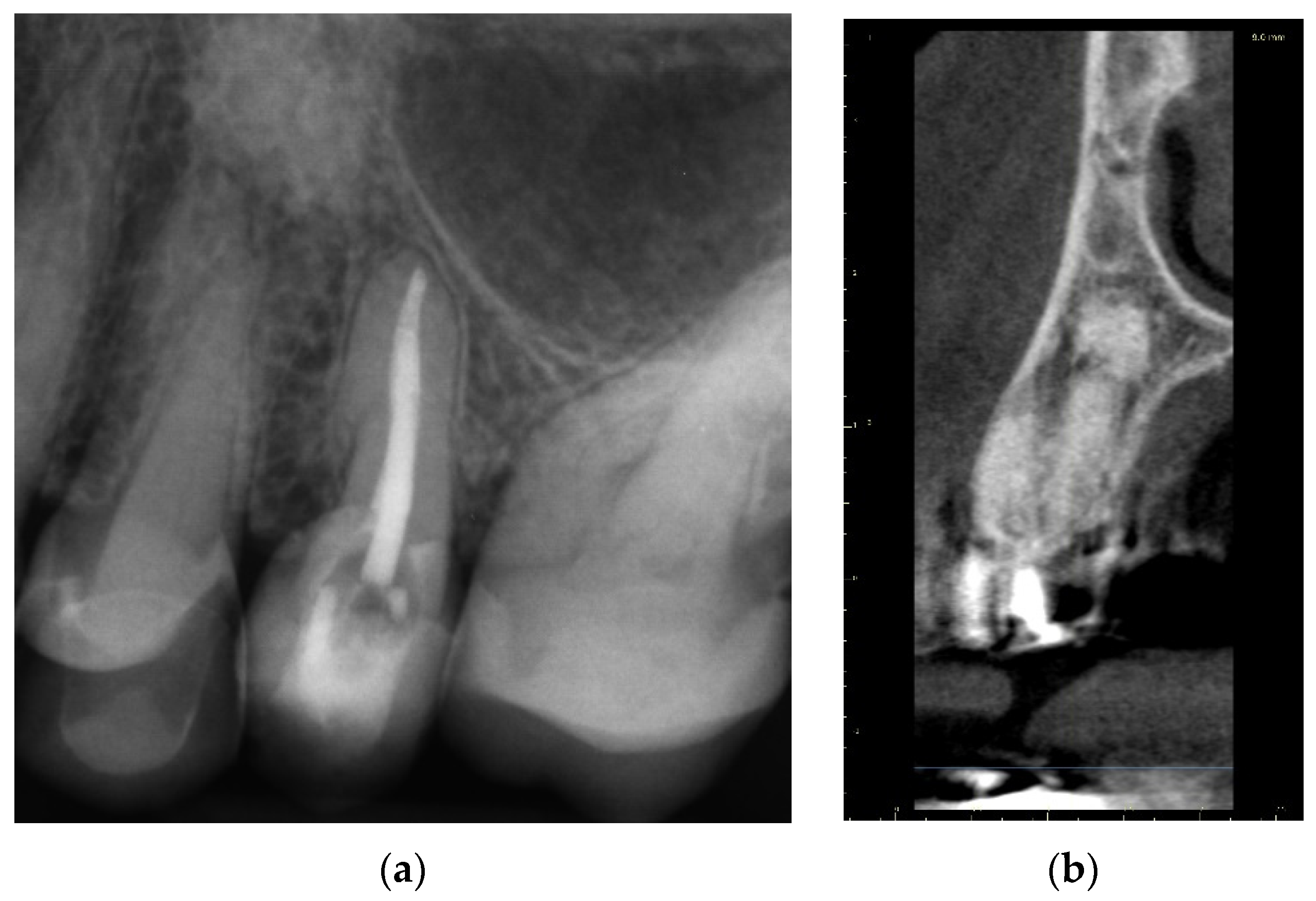
2.1.2. Case Report—Patient B: Asymptomatic Pulp Canal Obliteration after Trauma in Tooth Requiring Prosthetic Treatment (Aesthetic Dental Crown)
Three-Dimensional Treatment Plan
Canal Treatment
2.2. Canal Calcification in Elderly Patients
2.2.1. Case Report—Patient C: Asymptomatic Pulp Canal Obliteration—Endodontic Treatment before Surgical Procedure
Three-Dimensional Treatment Plan and RCT
2.2.2. Case Report—Patient D: Symptomatic Pulp Necrosis with Pulp Canal Obliteration
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mezger, U.; Jendrewski, C.; Bartels, M. Navigation in surgery. Langenbeck’s Arch. Surg. 2013, 398, 501–514. [Google Scholar] [CrossRef]
- Basten, C.H. The use of radiopaque templates for predictable implant placement. Quintessence Int. 1995, 26, 609–612. [Google Scholar] [PubMed]
- Al Yafi, F.; Camenisch, B.; Al-Sabbagh, M. Is Digital Guided Implant Surgery Accurate and Reliable? Dent. Clin. North Am. 2019, 63, 381–397. [Google Scholar] [CrossRef] [PubMed]
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Vehkalahti, M.M.; Swanljung, O. Accidental perforations during root canal treatment: An 8-year nationwide perspective on healthcare malpractice claims. Clin. Oral Investig. 2020, 24, 3683–3690. [Google Scholar] [CrossRef]
- Clark, D.; Khademi, J. Modern molar endodontic access and directed dentin conservation. Dent. Clin. North Am. 2010, 54, 249–273. [Google Scholar] [CrossRef] [PubMed]
- Maia, L.M.; Toubes, K.M.; Moreira Júnior, G.; Tonelli, S.Q.; Machado, V.d.C.; Silveira, F.F.; Nunes, E. Guided Endodontics in Nonsurgical Retreatment of a Mandibular First Molar: A New Approach and Case Report. Iran. Endod. J. 2020, 15, 111–116. [Google Scholar] [CrossRef]
- Torres, A.; Shaheen, E.; Lambrechts, P.; Politis, C.; Jacobs, R. Microguided Endodontics: A case report of a maxillary lateral incisor with pulp canal obliteration and apical periodontitis. Int. Endododontics J. 2019, 52, 540–549. [Google Scholar] [CrossRef]
- Abd-Elmeguid, A.; ElSalhy, M.; Yu, D.C. Pulp canal obliteration after replantation of avulsed immature teeth: A systematic review. Dent. Traumatol. 2015, 31, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Hegde, S.G.; Tawani, G.; Warhadpande, M.; Raut, A.; Dakshindas, D.; Wankhade, S. Guided endodontic therapy: Management of pulp canal obliteration in the maxillary central incisor. J. Conserv. Dent. 2019, 22, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Connert, T.; Zehnder, M.S.; Amato, M.; Weiger, R.; Kuhl, S.; Krastl, G. Microguided Endodontics: A method to achieve minimally invasive access cavity preparation and root canal location in mandibular incisors using a novel computer-guided technique. Int. Endododontics J. 2018, 51, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Bastos, J.V.; Côrtes, M.I.S. Pulp canal obliteration after traumatic injuries in permanent teeth—Scientific fact or fiction? Braz. Oral Res. 2018, 32 (Suppl. 1), e75. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.O.; Abreu MG, L.; Antunes, L.S.; Antunes, L.A.A. Factors associated with pulp canal obliteration due to traumatic injuries in deciduous teeth: A retrospective study. Int. J. Burn. Trauma 2021, 11, 304–311. [Google Scholar]
- McCabe, P.S.; Dummer, P.M. Pulp canal obliteration: An endodontic diagnosis and treatment challenge. Int. Endod. J. 2012, 45, 177–197. [Google Scholar] [CrossRef] [PubMed]
- Zehnder, M.S.; Connert, T.; Weiger, R.; Krastl, G.; Kühl, S. Guided endodontics: Accuracy of a novel method for guided access cavity preparation and root canal location. Int. Endod. J. 2016, 49, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, F.M. Pulpal healing after luxation injuries and root fracture in the permanent dentition. Endod. Dent. Traumatol. 1989, 5, 111–131. [Google Scholar] [CrossRef]
- Tchorz, J.P.; Wrbas, K.T.; Hellwig, E. Guided endodontic access of a calcified mandibular central incisor using a software-based three-dimensional treatment plan. Int. J. Comput. Dent. 2019, 22, 273–281. [Google Scholar] [PubMed]
- Krastl, G.; Zehnder, M.S.; Connert, T.; Weiger, R.; Kühl, S. Guided Endodontics: A novel treatment approach for teeth with pulp canal calcification and apical pathology. Dent. Traumatol. 2016, 32, 240–246. [Google Scholar] [CrossRef]
- Connert, T.; Krug, R.; Eggmann, F.; Emsermann, I.; ElAyouti, A.; Weiger, R.; Kühl, S.; Krastl, G. Guided Endodontics versus Conventional Access Cavity Preparation: A Comparative Study on Substance Loss Using 3-dimensional-printed Teeth. J. Endod. 2019, 45, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Patel, S. The use of cone beam computed tomography in the conservative management of dens invaginatus: A case report. Int. Endod. J. 2010, 43, 707–713. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, W.J.; Vissink, A.; Ng, Y.L.; Gulabivala, K. 3D Computer aided treatment planning in endodontics. J. Dent. 2016, 45, 67–72. [Google Scholar] [CrossRef]
- Keßler, A.; Dosch, M.; Reymus, M.; Folwaczny, M. Influence of 3D- printing method, resin material, and sterilization on the accuracy of virtually designed surgical implant guides. J. Prosthet. Dent. 2021, 8, S0022-3913(20)30621-1. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.S.; Mayfield-Donahoo, T.; Vanderven, F.J.; Jeffcoat, M.K. A comparison of the diagnostic advantages of panoramic radiography and computed tomography scanning for placement of root form dental implants. Clin. Oral Implant. Res. 1994, 5, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Buchgreitz, J.; Buchgreitz, M.; Bjørndal, L. Guided root canal preparation using cone beam computed tomography and optical surface scans—An observational study of pulp space obliteration and drill path depth in 50 patients. Int. Endod. J. 2019, 52, 559–568. [Google Scholar] [CrossRef]
- Moreno-Rabié, C.; Torres, A.; Lambrechts, P.; Jacobs, R. Clinical applications, accuracy, and limitations of guided endodontics: A systematic review. Int. Endod. J. 2020, 53, 214–223. [Google Scholar] [CrossRef]
- Ishak, G.; Habib, M.; Tohme, H.; Patel, S.; Bordone, A.; Perez, C.; Zogheib, C. Guided Endodontic Treatment of Calcified Lower Incisors: A Case Report. Dent. J. 2020, 8, 74. [Google Scholar] [CrossRef] [PubMed]
- Decurcio, D.A.; Bueno, M.R.; Silva, J.A.; Loureiro, M.; Damião Sousa-Neto, M.; Estrela, C. Digital Planning on Guided Endodontics Technology. Braz. Dent. J. 2021, 32, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Perez, C.; Sayeh, A.; Etienne, O.; Gros, C.I.; Mark, A.; Couvrechel, C.; Meyer, F. Microguided endodontics: Accuracy evaluation for access through intraroot fibre-post. Aust. Endod. J. 2021, 47, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Mena-Álvarez, J.; Rico-Romano, C.; Lobo-Galindo, A.B.; Zubizarreta-Macho, Á. Endodontic treatment of dens evaginatus by performing a splint guided access cavity. J. Esthet. Restor. Dent. 2017, 29, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Arslan, H. Guided endodontics: A case report of maxillary lateral incisors with multiple dens invaginatus. Restor. Dent. Endod. 2019, 44, e38. [Google Scholar] [CrossRef] [PubMed]
- Krug, R.; Volland, J.; Reich, S.; Soliman, S.; Connert, T.; Krastl, G. Guided endodontic treatment of multiple teeth with dentin dysplasia: A case report. Head Face Med. 2020, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics: European Society of Endodontology (ESE) developed by. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef] [PubMed]





























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage |
|---|
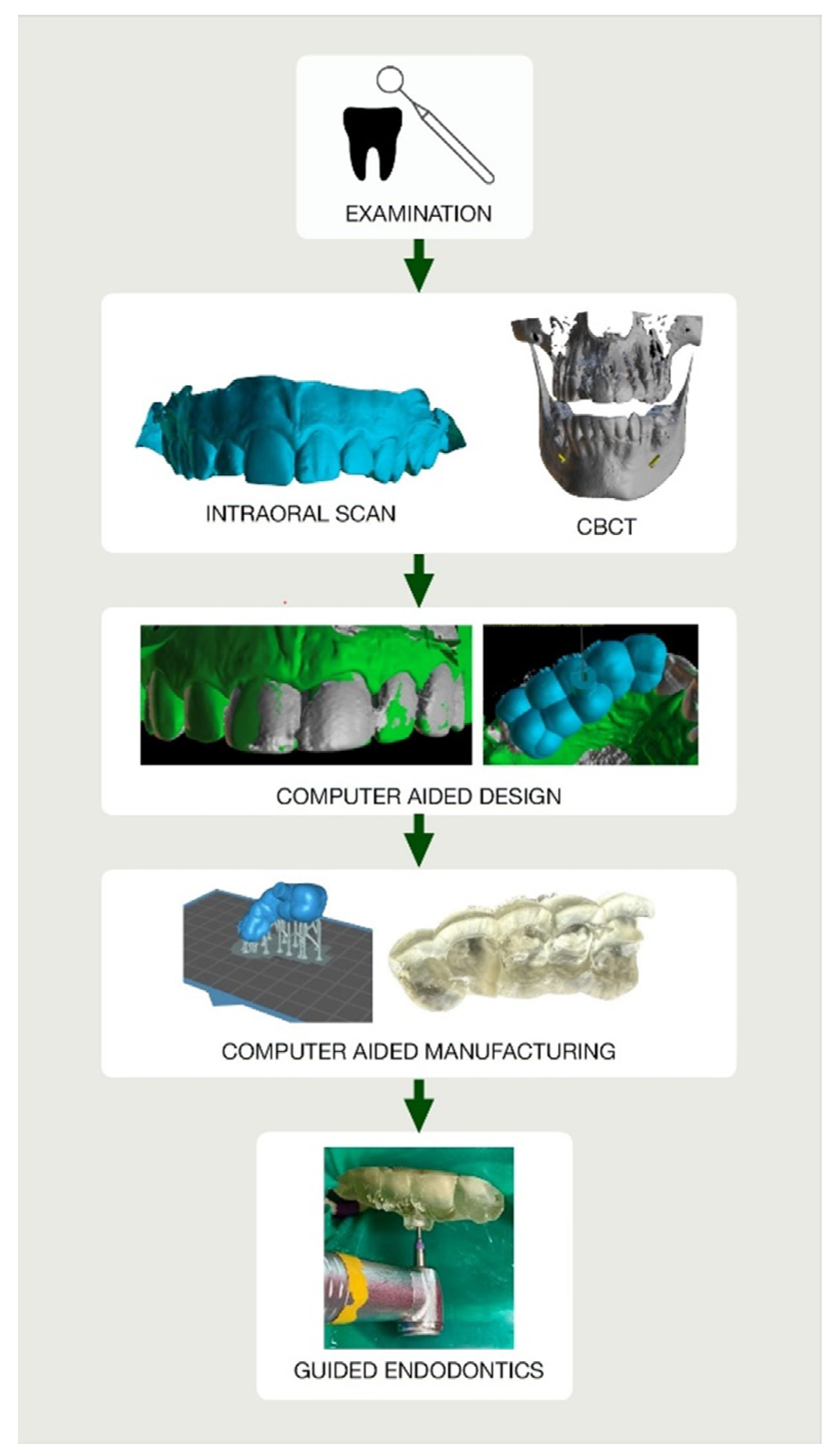
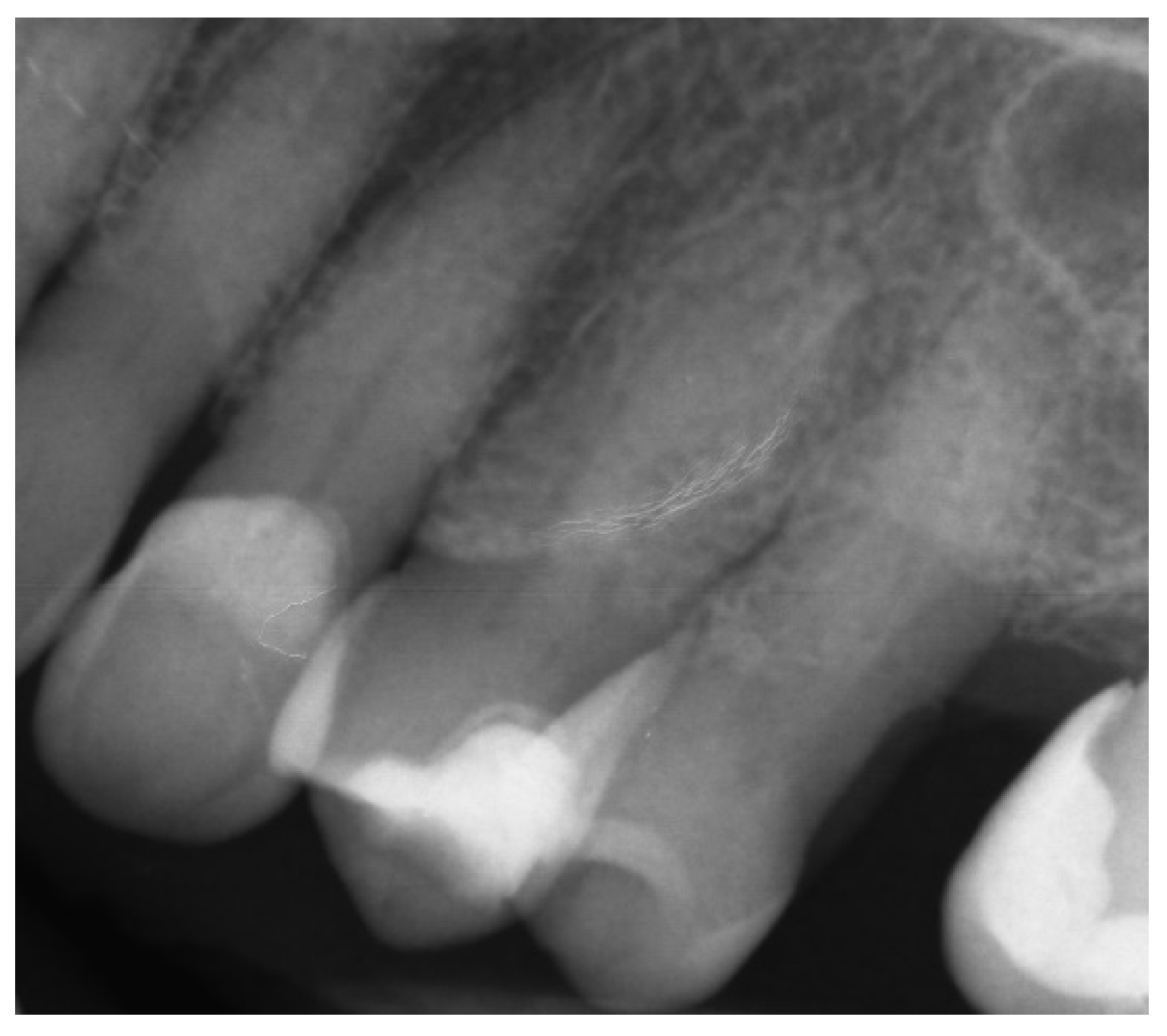
| Examination |
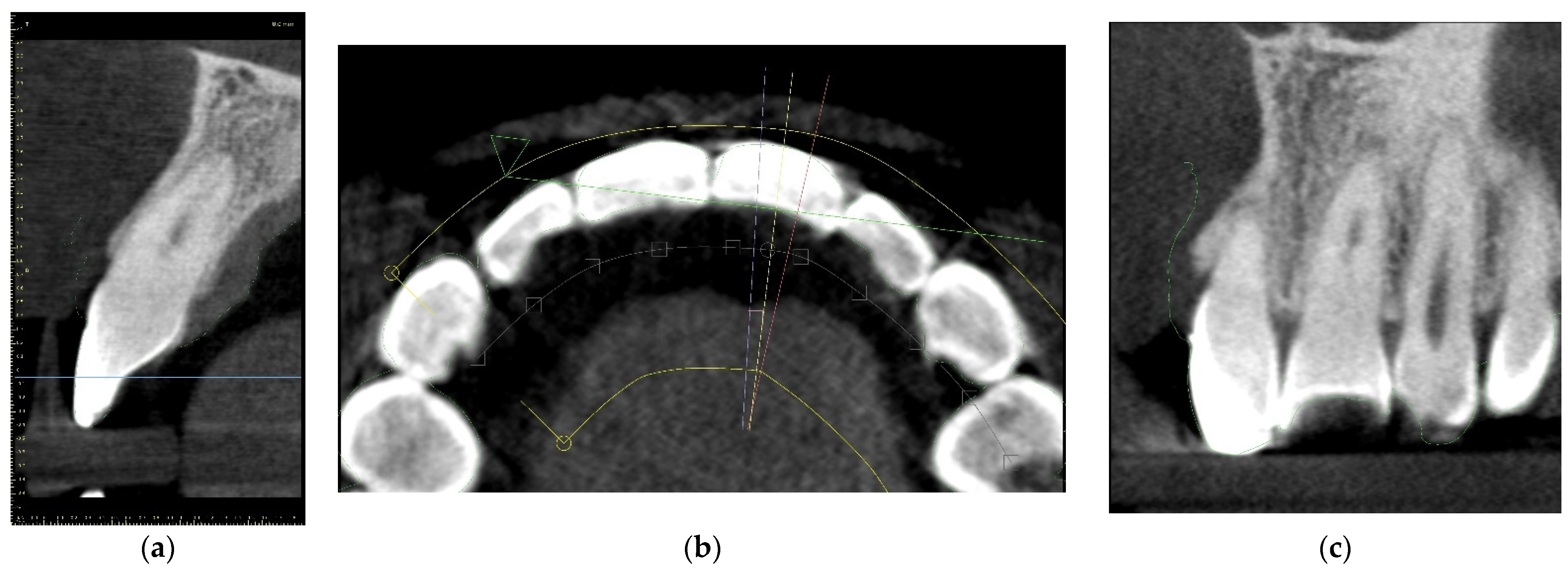
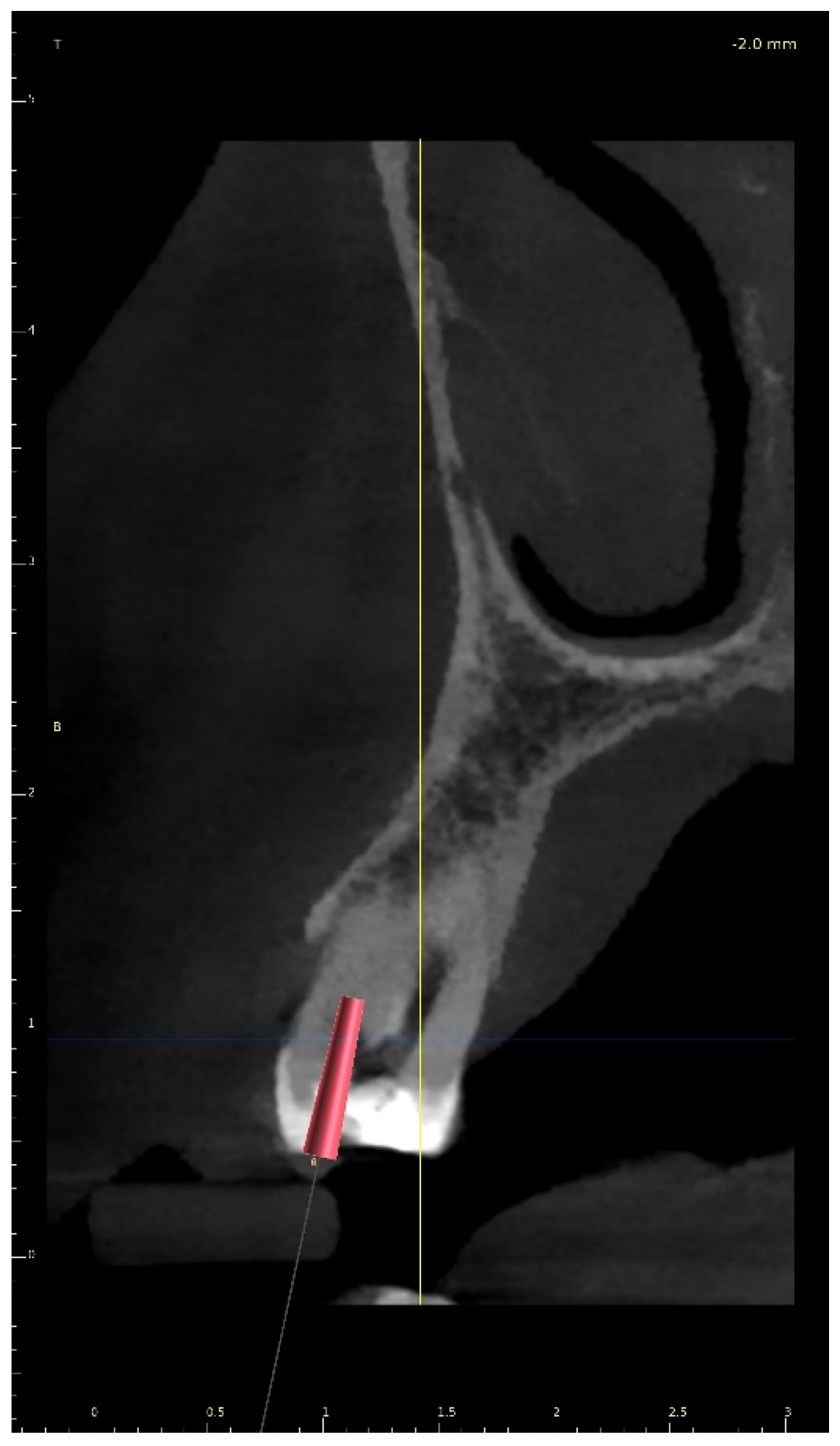
| Cone-beam computed tomographic scan |
| Digital intraoral impression: Directly—intraoral scan Indirectly—scanning impression or plaster model |
| Import DICOM and STL files into digital planning software |
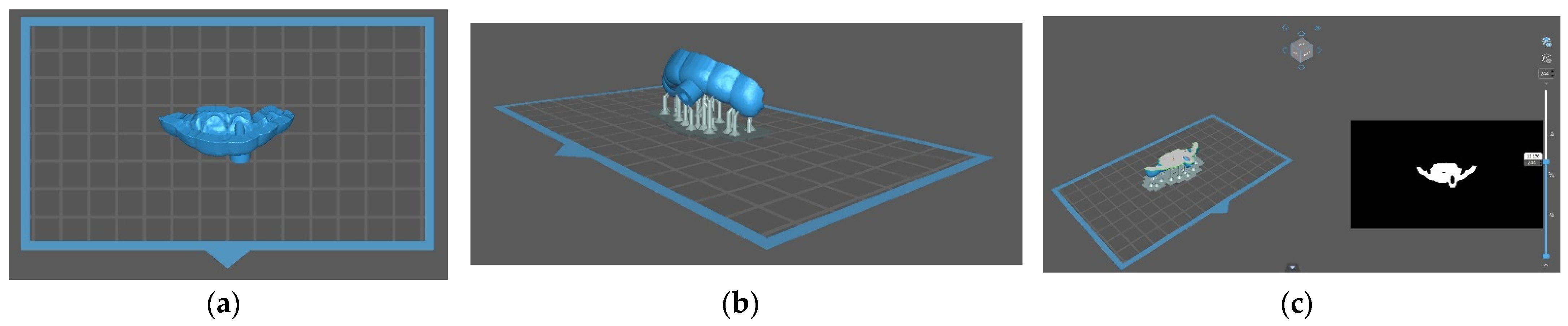
| Design the virtual drill path and the endodontic guide |
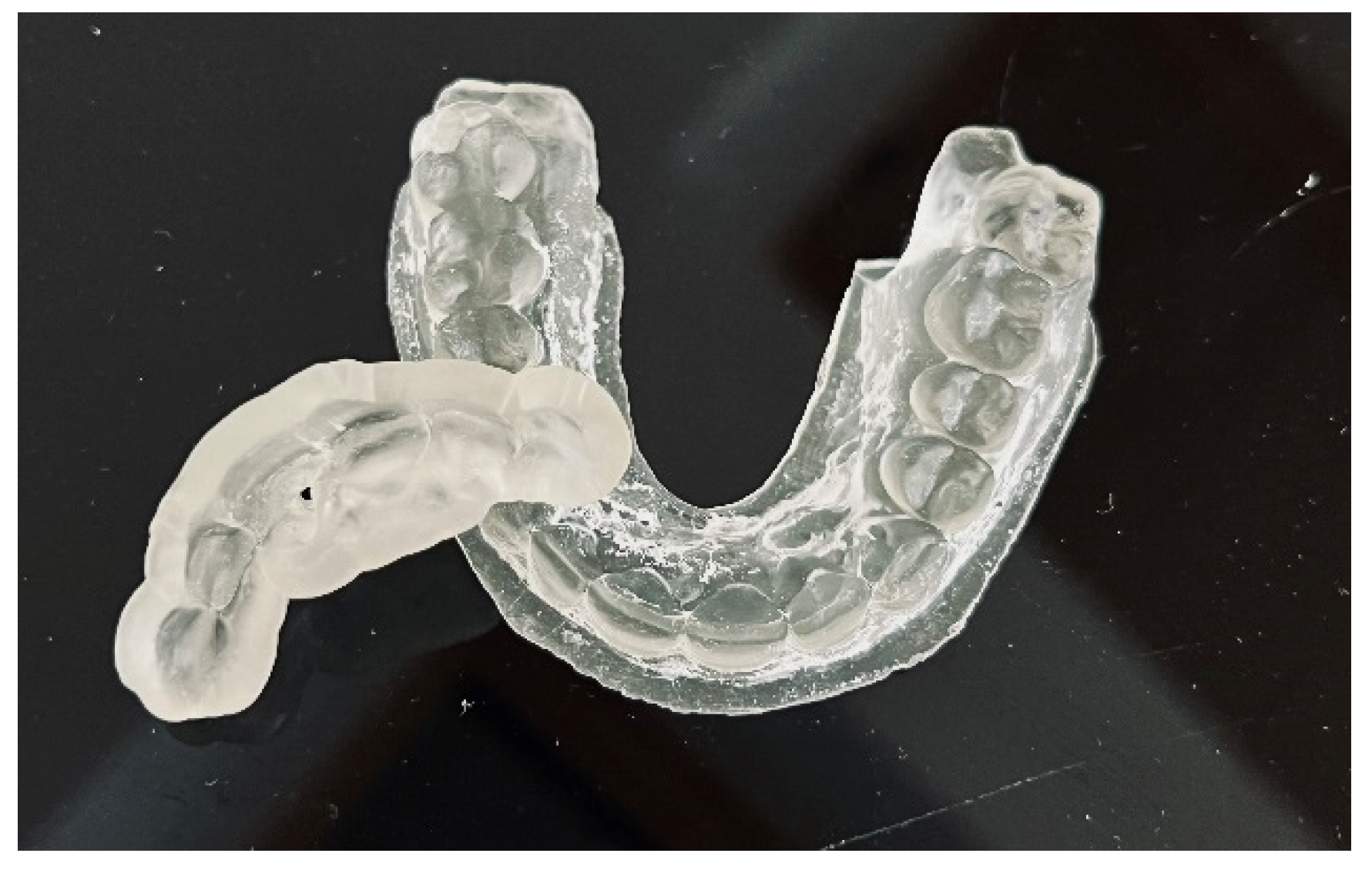
| Three-dimensional printing |
| Control the fit of the guide before and after placing rubber dam |
| Make a sign through the guide to indicate the access point in non-treated teeth |
| Remove the enamel until dentine is exposed |
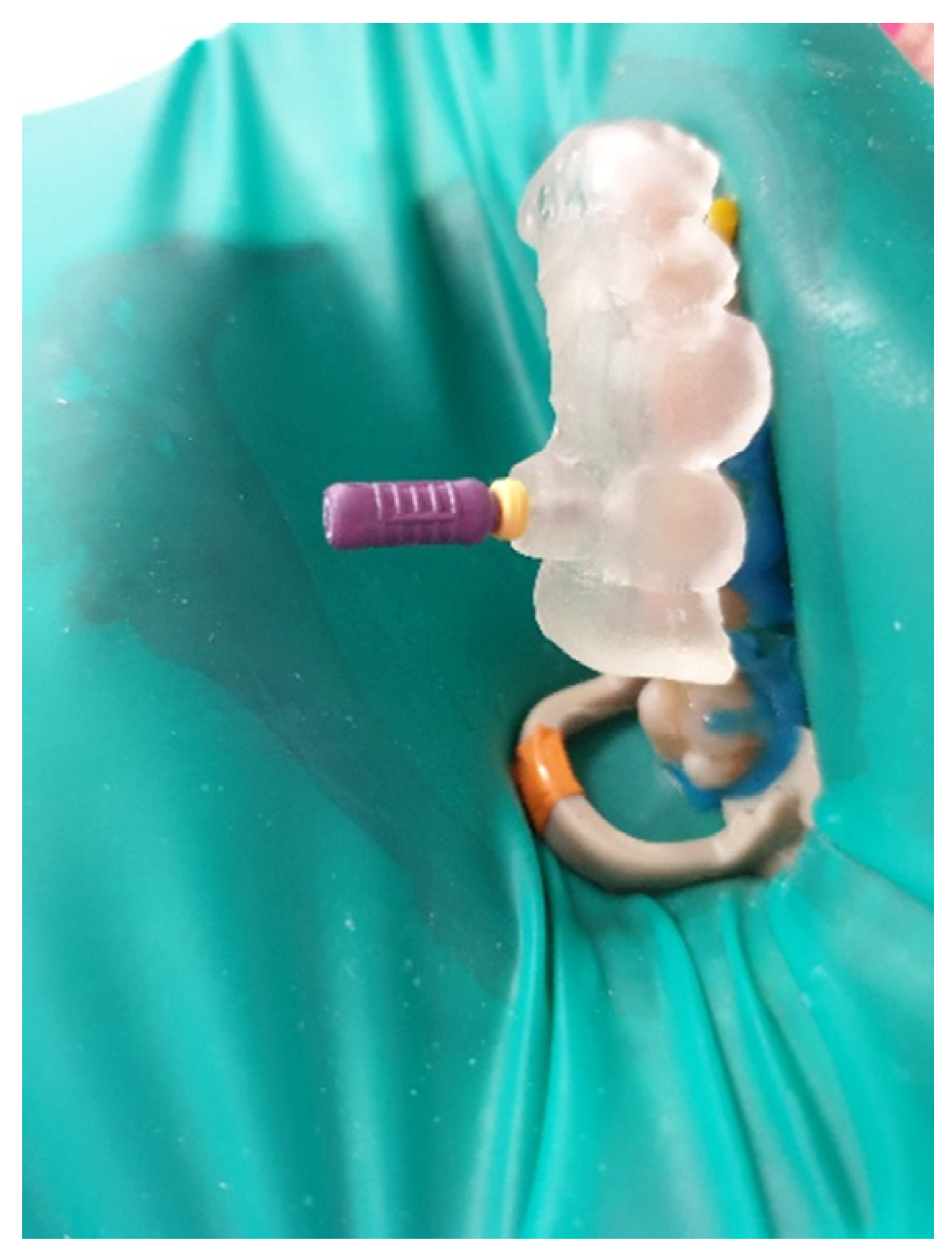
| Place the guide on the teeth |
| Work through the guide: Use rotate burs in dentine, scout the canal through the guide |
| Remove the guide to rinse the cavity and clean the burs, control endodontic access using an optical microscope |
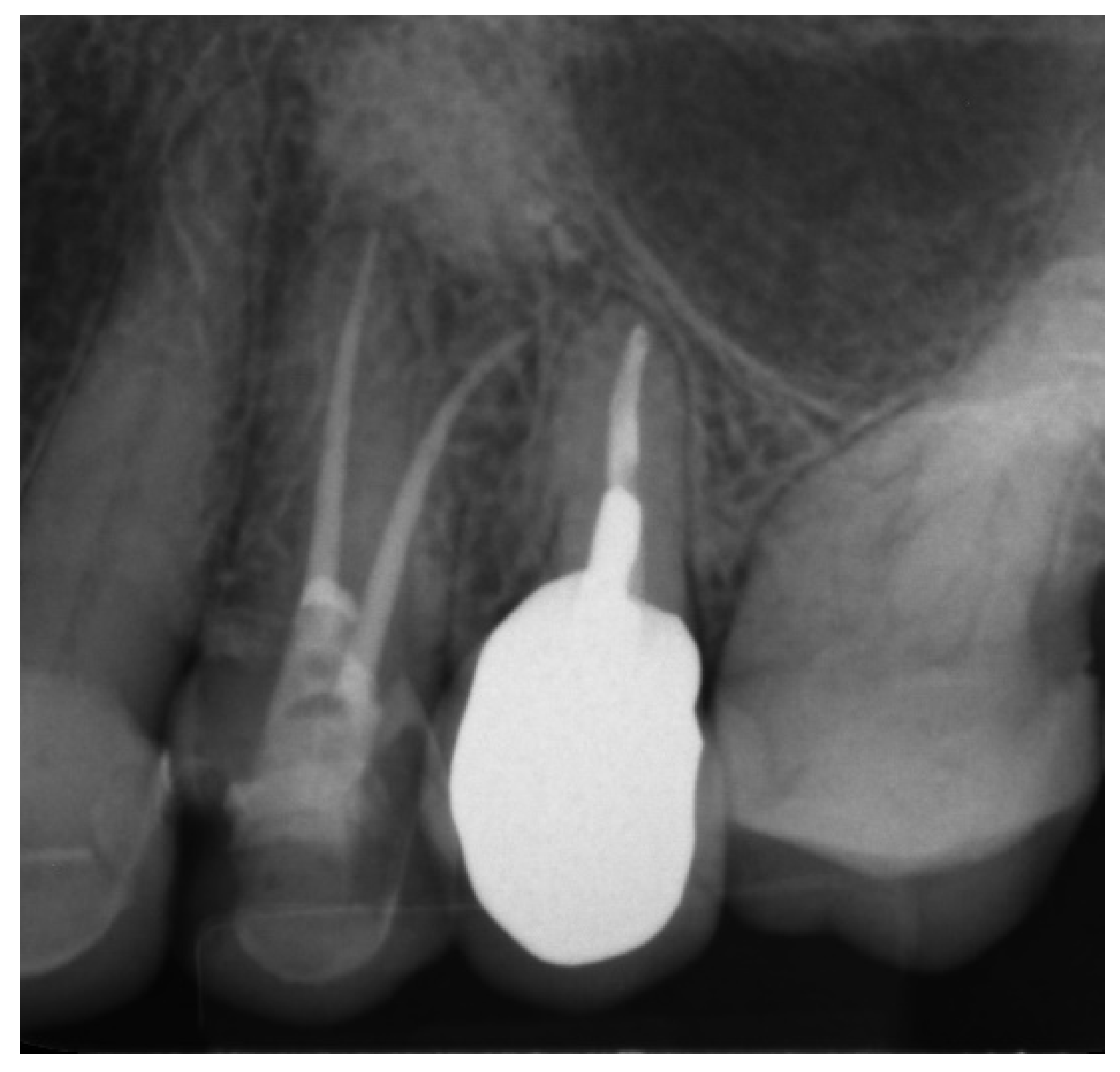
| Perform a radiographic examination to confirm correct canal access |
| Complete the root canal treatment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dąbrowski, W.; Puchalska, W.; Ziemlewski, A.; Ordyniec-Kwaśnica, I. Guided Endodontics as a Personalized Tool for Complicated Clinical Cases. Int. J. Environ. Res. Public Health 2022, 19, 9958. https://doi.org/10.3390/ijerph19169958
Dąbrowski W, Puchalska W, Ziemlewski A, Ordyniec-Kwaśnica I. Guided Endodontics as a Personalized Tool for Complicated Clinical Cases. International Journal of Environmental Research and Public Health. 2022; 19(16):9958. https://doi.org/10.3390/ijerph19169958
Chicago/Turabian StyleDąbrowski, Wojciech, Wiesława Puchalska, Adam Ziemlewski, and Iwona Ordyniec-Kwaśnica. 2022. "Guided Endodontics as a Personalized Tool for Complicated Clinical Cases" International Journal of Environmental Research and Public Health 19, no. 16: 9958. https://doi.org/10.3390/ijerph19169958
APA StyleDąbrowski, W., Puchalska, W., Ziemlewski, A., & Ordyniec-Kwaśnica, I. (2022). Guided Endodontics as a Personalized Tool for Complicated Clinical Cases. International Journal of Environmental Research and Public Health, 19(16), 9958. https://doi.org/10.3390/ijerph19169958