
“Back into Life—With a Power Wheelchair”: Learning from People with Severe Stroke through a Participatory Photovoice Study in a Metropolitan Area in Germany


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Recruitment of Co-Researchers
- stroke or traumatic brain injury (acquired after the age of 18);
- acute event at least 1 year ago;
- motor, cognitive, and/or communication impairments as a result of the acute event,
- living in an outpatient living arrangement in Berlin for at least 6 months (with or without assistance);
- provided with a power wheelchair (PWC) during rehabilitation and using a PWC outside the home;
- interest and willingness to actively participate in a research project that includes several group meetings;
- enjoyment of photography.
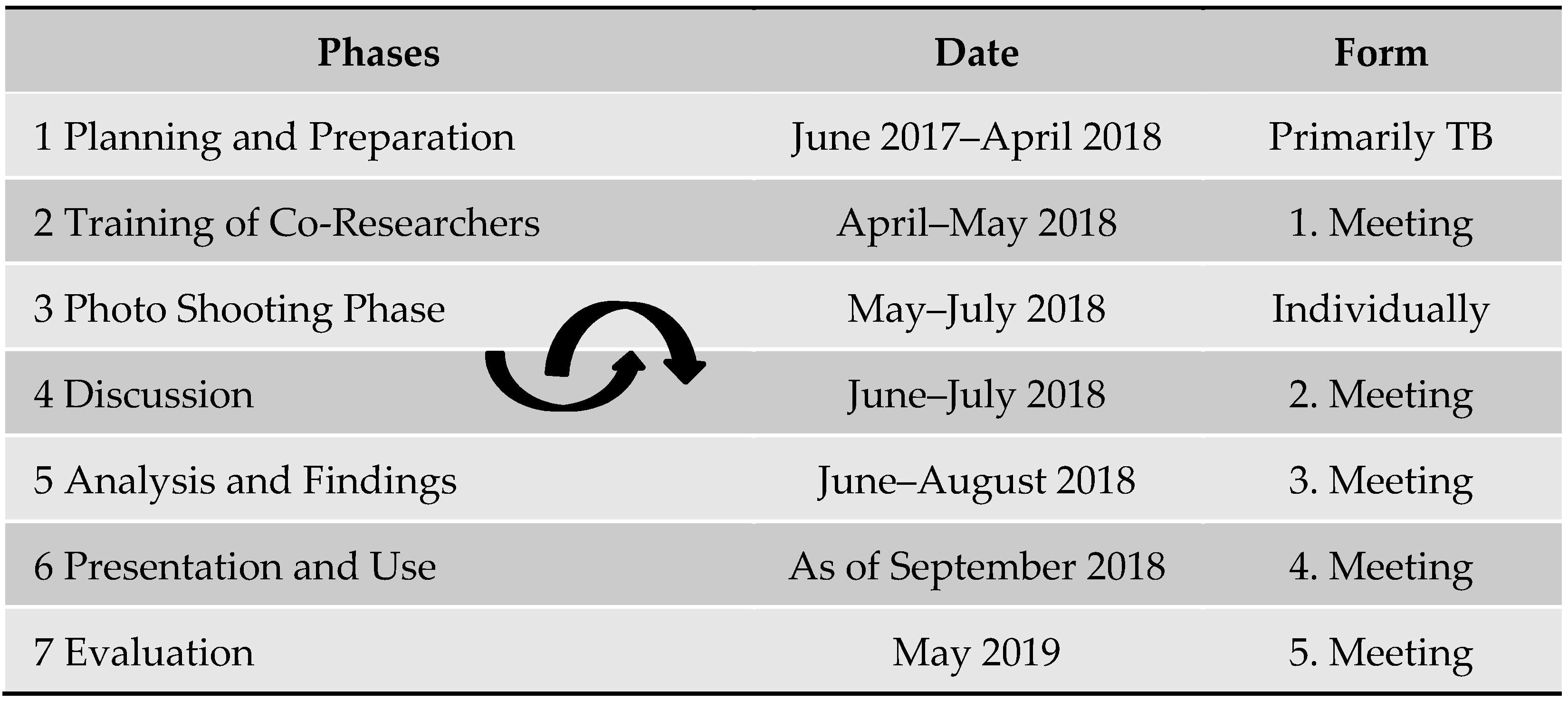
2.3. Photovoice Process
3. Results
3.1. Co-Researcher Characteristics
3.2. Back into Life—With a Power Wheelchair—Themes from Photos
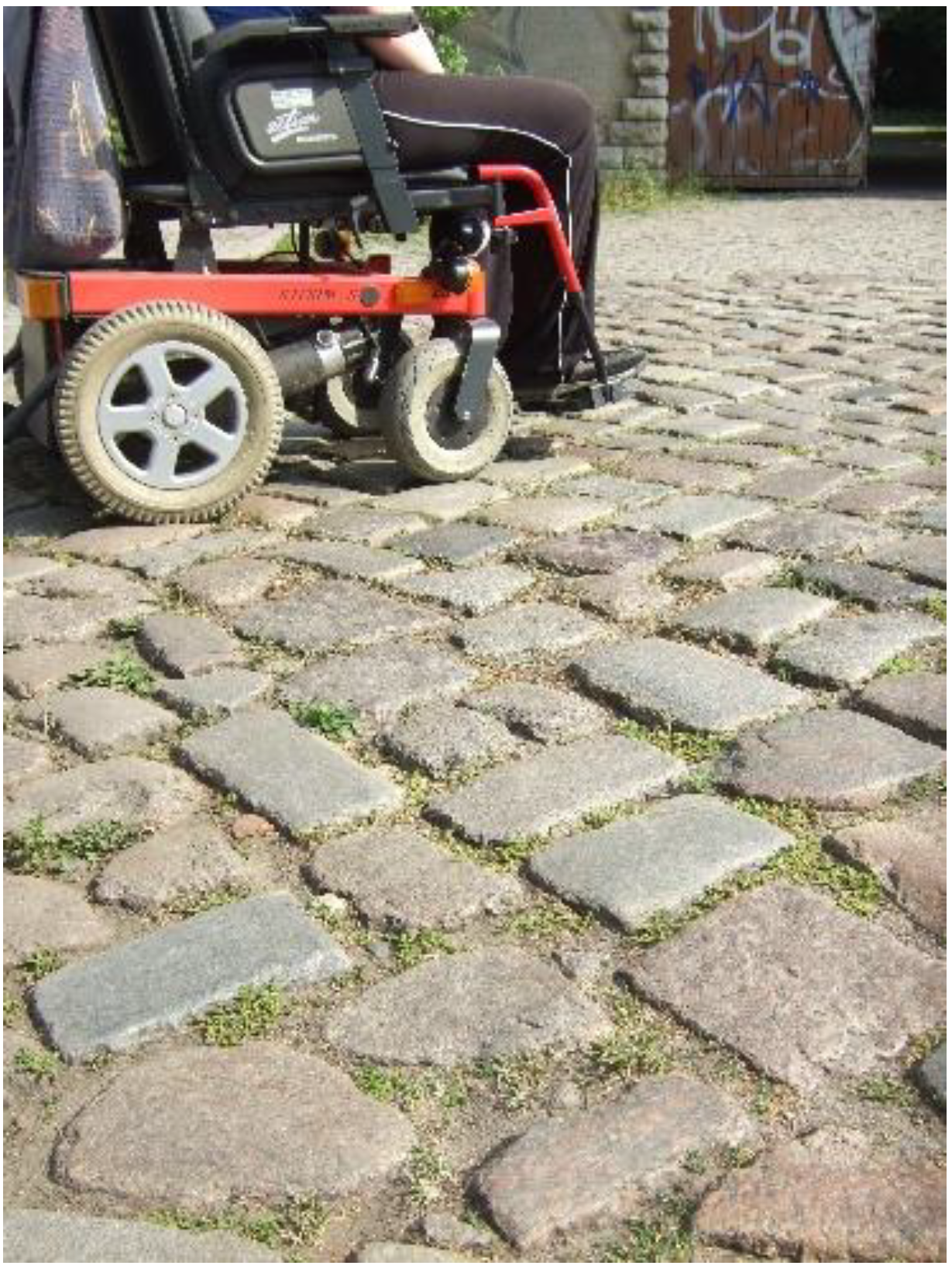
3.2.1. Theme 1: Built Environment
“Yes, … there are pedestrian paths. But they are relatively narrow, everything is relatively green. That means you always have to circle back and forth. And in between there are always these (.) “Huckelpflaster” (cobblestones). When there are driveways.”(Charlie, M2).


“I usually go (.) when I (.) visit friends or (.) go for a walk. Or logo (.) [speech and language therapy] do. Yes.”(Mika, M2).

3.2.2. Theme 2: Personal Freedom
“You can see the cinema there. Alexanderplatz. And I did that because I’m there quite often. (.) … Because all the cinemas there are barrier-free. … In the PWC or wheelchair you sit in the back. And you have a good view of the screen. That’s why I think it’s so good.”(Lukas, M3).

“I enjoy that (.) when I (.) go to market hall. And (.) then (.) people arrive. And watch (moves her head to do so). And (.) people approach me. “What did you do” and dedede (.) … But (.) this is (..) my home (gestures with her hand). (.) Yes. (.) Like this.”(Mika, M2).
“I like to be outside with my PWC. I like to go to the Schlosspark. I love the trees—always have. I like to be in nature. I can’t get there on foot. With my PWC, I can go there by myself when I want. My wish: Despite my physical limitations, I would like to do the things I like to do. And that do me good. The PWC helps me to do that.”

3.2.3. Theme 3: Me and My Power Wheelchair (PWC)
“Uh (runs her hand over the armrest of her PWC and considers) (…) Bonita. And (..) I love (..) (taps hand on armrest in time to speaking) PWC.”(Mika, M2).

“I … have always given my car a name. So, I think I would then also, if I can identify with that, somehow. … If I can then say that it is mine. (.) Then I would also give it a name.”(Charlie, M2).
“If I … drive into the café (.) too briskly (.) … then I drive into the tables. (.) A path of destruction in”(Chris, M2).

3.2.4. Theme 4: Demands on Users of a Power Wheelchair (PWC)
3.2.5. Theme 5: Demands on Other Persons
“Sure, with my brother I would manage that. (.) Well, I would also be able to walk 2, 3 steps (.) to the toilet. That would not be a problem. (.) But I wouldn’t do that with a complete stranger. … (laughs). I don’t say to the waitress: “Yes, go with me to the toilet!”(Charlie, M3).
“That it is not enough (.) to have such an expensive part [PWC] there. But that you also have to get it adequately adapted. … Yes. And now I just sit in the shack. (.) It’s really like that.”(Charlie, M2).

3.2.6. Theme 6: Desires for Change
“I was healthy until five years ago, too. And jumped around. And now I am sitting in one of these. I imagined it differently, too. And tomorrow you could be hit by a stroke!”(Charlie, M3).
“This is the place [rehabilitation center] where you are made fit again… for life (.) And (.) … I’m sure some people have already resigned. (..) There’s no progress at all. And (..) And yes, everything sucks. And so on. (.) But (.) the people should also see that it (.) goes up. That there are assistive devices.”(Chris, M3).
3.3. Dissemination of Findings
3.4. Evaluation
4. Discussion
4.1. Complexity of Community Mobility Using a Power Wheelchair
4.1.1. Accessible Environment and Transport Possibilities
4.1.2. Invisible and Unexpected Challenging Experiences
4.1.3. Individually Meaning of Community Mobility
4.2. Identification with the Power Wheelchair
4.3. Methodological Considerations
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krishnamurthi, R.V.; Ikeda, T.; Feigin, V.L. Global, Regional and Country-Specific Burden of Ischaemic Stroke, Intracerebral Haemorrhage and Subarachnoid Haemorrhage: A Systematic Analysis of the Global Burden of Disease Study 2017. Neuroepidemiology 2020, 54, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Hay, S.I.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef] [Green Version]
- Busch, M.A.; Kuhnert, R. 12-Monats-Prävalenz von Schlaganfall oder chronischen Beschwerden infolge eines Schlaganfalls in Deutschland: Robert Koch-Institut. J. Health Monit. 2017, 2, 70–76. [Google Scholar] [CrossRef]
- Shaughnessy, M.; Michael, K.M.; Sorkin, J.D.; Macko, R.F. Steps after stroke: Capturing ambulatory recovery. Stroke 2005, 36, 1305–1307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jørgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Vive-Larsen, J.; Støier, M.; Olsen, T.S. Outcome and time course of recovery in stroke. Part II: Time course of recovery. The copenhagen stroke study. Arch. Phys. Med. Rehabil. 1995, 76, 406–412. [Google Scholar] [CrossRef]
- McGlinchey, M.P.; James, J.; McKevitt, C.; Douiri, A.; Sackley, C. The effect of rehabilitation interventions on physical function and immobility-related complications in severe stroke: A systematic review. BMJ Open 2020, 10, e033642. [Google Scholar] [CrossRef] [Green Version]
- Wesselhoff, S.; Hanke, T.A.; Evans, C.C. Community mobility after stroke: A systematic review. Top. Stroke Rehabil. 2018, 25, 224–238. [Google Scholar] [CrossRef]
- Nanninga, C.S.; Meijering, L.; Postema, K.; Schönherr, M.C.; Lettinga, A.T. Unpacking community mobility: A preliminary study into the embodied experiences of stroke survivors. Disabil. Rehabil. 2018, 40, 2015–2024. [Google Scholar] [CrossRef]
- Hesse, S.; Staats, M.; Werner, C.; Bestmann, A.; Lingnau, M.L. Ambulante Krankengymnastik von Schlaganfallpatienten zu Hause. Nervenarzt 2001, 72, 950–954. [Google Scholar] [CrossRef]
- Logan, P.A.; Dyas, J.; Gladman, J.R.F. Using an interview study of transport use by people who have had a stroke to inform rehabilitation. Clin. Rehabil. 2004, 18, 703–708. [Google Scholar] [CrossRef]
- Logan, P.A.; Armstrong, S.; Avery, T.J.; Barer, D.; Barton, G.R.; Darby, J.; Gladman, J.R.F.; Horne, J.; Leach, S.; Lincoln, N.B.; et al. Rehabilitation aimed at improving outdoor mobility for people after stroke: A multicentre randomised controlled study (the Getting out of the House Study). Health Technol. Assess. 2014, 18, 1–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF. Available online: https://apps.who.int/iris/handle/10665/42407 (accessed on 18 July 2022).
- AOTA. Occupational Therapy Practice Framework: Domain and Process—Fourth Edition. Am. J. Occup. Ther. 2020, 74, 7412410010p1–7412410010p87. [Google Scholar] [CrossRef]
- Eriksson, G.; Kottorp, A.; Borg, J.; Tham, K. Relationship between occupational gaps in everyday life, depressive mood and life satisfaction after acquired brain injury. J. Rehabil. Med. 2009, 41, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendel, K.; Ståhl, A.; Risberg, J.; Pessah-Rasmussen, H.; Iwarsson, S. Post-stroke functional limitations and changes in use of mode of transport. Scand. J. Occup. Ther. 2010, 17, 162–174. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, C.; Chard, G. An exploration of participation in leisure activities post-stroke. Aust. Occup. Ther. J. 2010, 57, 159–166. [Google Scholar] [CrossRef]
- Burton, C.R. Living with stroke: A phenomenological study. J. Adv. Nurs. 2000, 32, 301–309. [Google Scholar] [CrossRef]
- Balakrishnan, R.; Kaplan, B.; Negron, R.; Fei, K.; Goldfinger, J.Z.; Horowitz, C.R. Life after Stroke in an Urban Minority Population: A Photovoice Project. Int. J. Environ. Res. Public Health 2017, 14, 293. [Google Scholar] [CrossRef] [Green Version]
- Salter, K.; Hellings, C.; Foley, N.; Teasell, R. The experience of living with stroke: A qualitative meta-synthesis. J. Rehabil. Med. 2008, 40, 595–602. [Google Scholar] [CrossRef] [Green Version]
- Barker, D.J.; Reid, D.; Cott, C. The Experience of Senior Stroke Survivors: Factors in Community Participation among Wheelchair Users. Can. J. Occup. Ther. 2006, 73, 18–25. [Google Scholar] [CrossRef]
- Evans, R. The Effect of Electrically Powered Indoor/Outdoor Wheelchairs on Occupation: A Study of Users’ Views. Br. J. Occup. Ther. 2000, 63, 547–553. [Google Scholar] [CrossRef]
- Edwards, K.; McCluskey, A. A survey of adult power wheelchair and scooter users. Disabil. Rehabil. Assist. Technol. 2010, 5, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Wressle, E.; Samuelsson, K. User Satisfaction with Mobility Assistive Devices. Scand. J. Occup. Ther. 2004, 11, 143–150. [Google Scholar] [CrossRef]
- Pettersson, I.; Törnquist, K.; Ahlström, G. The effect of an outdoor powered wheelchair on activity and participation in users with stroke. Disabil. Rehabil. Assist. Technol. 2006, 1, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Buning, M.E.; Angelo, J.A.; Schmeler, M.R. Occupational Performance and the Transition to Powered Mobility: A Pilot Study. Am. J. Occup. Ther. 2001, 55, 339–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandt, A.; Iwarsson, S.; Ståhle, A. Older people’s use of powered wheelchairs for activity and participation. J. Rehabil. Med. 2004, 36, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Deutsche Gesellschaft für Allgemeinmedizin und Familienmedizin. Schlaganfall S3-Leitlinie: DEGAM-Leitlinie Nr. 8. Available online: https://www.awmf.org/uploads/tx_szleitlinien/053-011l_S3_Schlaganfall_2021-03.pdf (accessed on 25 June 2022).
- Bestmann, A.; Lingnau, M.L.; Staats, M.; Hesse, S. Phasenspezifische Hilfsmittelverordnungen in der neurologischen Rehabilitation. Rehabilitation 2001, 6, 346–351. [Google Scholar] [CrossRef]
- Reuther, P.; Wallesch, C.-W. Teilhabesicherung nach Schlaganfall. Gesundheitswesen 2015, 77, 513–523. [Google Scholar] [CrossRef]
- Perotti, L.; Klebbe, R.; Maier, A.; Eicher, C. Evaluation of the quality and the provision process of wheelchairs in Germany. Results from an online survey. Disabil. Rehabil. Assist. Technol. 2020, 1–10. [Google Scholar] [CrossRef]
- Deutsche Vereinigung für Rehabilitation. Für eine optimierte Versorgung mit Hilfsmitteln: Eine Expertise der Deutschen Vereinigung für Rehabilitation zu aktuellen Problemen bei der Versorgung mit Hilfsmitteln. 2006. Available online: https://www.dvfr.de/fileadmin/user_upload/DVfR/Downloads/Stellungnahmen/DVfR-Hilfsmittel-Expertise_061017.pdf (accessed on 18 June 2022).
- Deutsche Vereinigung für Rehabilitation. Empfehlungen zur Verbesserung des Teilhabeorientierten Versorgungsprozesses Mobilitätseingeschränkter Menschen mit Rollstühlen. 2018. Available online: https://www.dvfr.de/fileadmin/user_upload/DVfR/Downloads/Stellungnahmen/DVfR-Stellungnahme_Rollstuhlversorgung_-_Juni_2018_bf.pdf (accessed on 18 June 2022).
- Hesse, S.; Gahein-Sama, A.L.; Mauritz, K.-H. Technical aids in hemiparetic patients: Prescription, costs and usage. Clin. Rehabil. 1996, 10, 328–333. [Google Scholar] [CrossRef]
- Hoeß, U.; Schupp, W.; Schmidt, R.; Gräßel, E. Versorgung von Schlaganfallpatienten mit ambulanten Heil- und Hilfsmitteln im Langzeitverlauf nach stationärer neurologischer Rehabilitation. Phys. Med. Rehabil. Kurortmed. 2008, 18, 115–121. [Google Scholar] [CrossRef]
- UN General Assembly. Convention on the Rights of Persons with Disabilities: Resolution/Adopted by the General Assembly, 24 January 2007, A/RES/61/106. Available online: https://www.refworld.org/docid/45f973632.html (accessed on 18 July 2022).
- Bundesministerium für Arbeit und Soziales. “Unser Weg in eine Inklusive Gesellschaft”: Nationaler Aktionsplan 2.0 der Bundesregierung zur UN-Behindertenrechtskonvention (UN-BRK). 2016. Available online: https://www.bmas.de/DE/Soziales/Teilhabe-und-Inklusion/Nationaler-Aktionsplan/nationaler-aktionsplan-2-0.html (accessed on 25 June 2022).
- Deutsche Vereinigung für Rehabilitation. Stellungnahme: Partizipation an der Forschung–Eine Matrix zur Orientierung. Available online: https://www.dvfr.de/arbeitsschwerpunkte/stellungnahmen-der-dvfr/detail/artikel/dvfr-stellungnahme-partizipation-an-der-forschung-eine-matrix-zur-orientierung/ (accessed on 25 June 2022).
- Wright, M.T. Partizipative Gesundheitsforschung: Ursprünge und heutiger Stand. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2021, 64, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Munde, V.; Tillmann, V. Partizipative Forschung: Umsetzungsbeispiele und Zukunftsperpektiven. Teilhabe 2022, 61, 74–80. [Google Scholar]
- Wang, C.; Burris, M.A. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef] [Green Version]
- Catalani, C.; Minkler, M. Photovoice: A review of the literature in health and public health. Health Educ. Behav. 2010, 37, 424–451. [Google Scholar] [CrossRef] [PubMed]
- Dassah, E.; Aldersey, H.M.; Norman, K.E. Photovoice and Persons With Physical Disabilities: A Scoping Review of the Literature. Qual. Health Res. 2017, 27, 1412–1422. [Google Scholar] [CrossRef] [PubMed]
- Lal, S.; Jarus, T.; Suto, M.J. A Scoping Review of the Photovoice Method: Implications for Occupational Therapy Research. Can. J. Occup. Ther. 2012, 79, 181–190. [Google Scholar] [CrossRef]
- Evans-Agnew, R.A.; Rosemberg, M.-A.S. Questioning Photovoice Research: Whose Voice? Qual. Health Res. 2016, 26, 1019–1030. [Google Scholar] [CrossRef]
- Levin, T.; Scott, B.M.; Borders, B.; Hart, K.; Lee, J.; Decanini, A. Aphasia Talks: Photography as a means of communication, self-expression, and empowerment in persons with aphasia. Top. Stroke Rehabil. 2007, 14, 72–84. [Google Scholar] [CrossRef]
- Lorenz, L.S. Visual metaphors of living with brain injury: Exploring and communicating lived experience with an invisible injury. Vis. Stud. 2010, 25, 210–223. [Google Scholar] [CrossRef]
- Barclay-Goddard, R.; Ripat, J.; Mayo, N.E. Developing a model of participation post-stroke: A mixed-methods approach. Qual. Life Res. 2012, 21, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Hebblethwaite, S.; Curley, L. Exploring the role of community recreation in stroke recovery using participatory action research and photovoice. Ther. Recreat. J. 2015, 49, 1–17. [Google Scholar]
- Maratos, M.; Huynh, L.; Tan, J.; Lui, J.; Jarus, T. Picture This: Exploring the Lived Experience of High-Functioning Stroke Survivors Using Photovoice. Qual. Health Res. 2016, 26, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Törnbom, K.; Lundälv, J.; Palstam, A.; Sunnerhagen, K.S. “My life after stroke through a camera lens”—A photovoice study on participation in Sweden. PLoS ONE 2019, 14, e0222099. [Google Scholar] [CrossRef] [PubMed]
- Dietz, A.; Mamlekar, C.R.; Bakas, K.L.; McCarthy, M.J.; Harley, D.; Bakas, T. A scoping review of PhotoVoice for people with post-stroke aphasia. Top. Stroke Rehabil. 2021, 28, 219–235. [Google Scholar] [CrossRef]
- International Collaboration for Participatory Health Research. Position Paper 1: What Is Participatory Health Research? International Collaboration for Participatory Health Research: Berlin, Germany, 2013; Available online: http://www.icphr.org/uploads/2/0/3/9/20399575/ichpr_position_paper_1_defintion_-_version_may_2013.pdf (accessed on 5 June 2022).
- German Network for Participatory Health Research. PartNet Definition–Partizipative Gesundheitsforschung. Available online: http://partnet-gesundheit.de/ueber-uns/partnet-definition/ (accessed on 24 June 2022).
- Von Unger, H. Partizipative Forschung: Einführung in die Forschungspraxis; Springer: Wiesbaden, Germany, 2014; ISBN 9783658012892. [Google Scholar]
- Chung, K.; Lounsbury, D.W. The role of power, process, and relationships in participatory research for statewide HIV/AIDS programming. Soc. Sci. Med. 2006, 63, 2129–2140. [Google Scholar] [CrossRef]
- Von Unger, H.; Narimani, P. Ethische Reflexivität im Forschungsprozess: Herausforderungen in der Partizipativen Forschung; WZB Discussion Paper SP I 2012-304; Wissenschaftszentrum Berlin für Sozialforschung (WZB): Berlin, Germany, 2012. [Google Scholar]
- Wang, C.C.; Redwood-Jones, Y.A. Photovoice ethics: Perspectives from Flint Photovoice. Health Educ. Behav. 2001, 28, 560–572. [Google Scholar] [CrossRef]
- Abma, T.; Breed, M.; Lips, S.; Schrijver, J. Whose Voice is It Really? Ethics of Photovoice with Children in Health Promotion. Int. J. Qual. Methods 2022, 21, 160940692110724. [Google Scholar] [CrossRef]
- International Collaboration for Participatory Health Research. Position Paper 2: Participatory Health Research: A Guide to Ethical Principals and Practice; International Collaboration for Participatory Health Research: Berlin, Germany, 2013; Available online: http://www.icphr.org/uploads/2/0/3/9/20399575/ichpr_position_paper_2_ethics_-_version_october_2013.pdf (accessed on 5 June 2022).
- Fields, L.M.; Calvert, J.D. Informed consent procedures with cognitively impaired patients: A review of ethics and best practices. Psychiatry Clin. Neurosci. 2015, 69, 462–471. [Google Scholar] [CrossRef]
- Pearl, G.; Cruice, M. Facilitating the Involvement of People with Aphasia in Stroke Research by Developing Communicatively Accessible Research Resources. Top. Lang. Disord. 2017, 37, 67–84. [Google Scholar] [CrossRef]
- Hansen-Schirra, S.; Maaß, C. Easy Language, Plain Language, Easy Language Plus: Perspectives on Comprehensibility and Stigmatisation. In Easy Language Research: Text and User Perspectives, 2nd ed.; Hansen-Schirra, S., Maaß, C., Eds.; Frank & Timme: Berlin, Germany, 2020; pp. 17–38. [Google Scholar]
- Bundesministerium für Arbeit und Soziales. Leichte Sprache. Ein Rat ge ber. Available online: https://www.bmas.de/DE/Service/Publikationen/Broschueren/a752-leichte-sprache-ratgeber.html (accessed on 27 June 2022).
- Arnold, D.; Glässel, A.; Böttger, T.; Sarma, N.; Bethmann, A.; Narimani, P. “What do you need? What are you experiencing?” Relationship building and power dynamics in participatory research projects: Critical self-reflections of researchers. Int. J. Environ. Res. Public Health 2022, 19, 9336. [Google Scholar] [CrossRef]
- Schaefer, I.; Kümpers, S.; Cook, T. “Selten Gehörte“ für partizipative Gesundheitsforschung gewinnen: Herausforderungen und Strategien. Bundesgesundheitsblatt-Gesundh. -Gesundh. 2021, 64, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Allweiss, T.; Perowanowitsch, M.; Burtscher, R.; Wright, M.T. Participatory Exploration of Factors Influencing the Health of People with Intellectual Disabilities in an Urban District: A photovoice study. In Proceedings of the 3rd International Conference on Public Health, Kuala Lumpur, Malaysia, 27–29 July 2017; pp. 237–245. [Google Scholar] [CrossRef]
- Lorenz, L.S. Brain Injury Survivors: Narratives of Rehabilitation and Healing; Lynne Rienner Publishers: Boulder, CO, USA, 2010; ISBN 1588267288. [Google Scholar]
- Lorenz, L.S. What Is Photovoice? A Photovoice Path. Available online: https://www.photovoiceworldwide.com/what-is-photovoice/ (accessed on 26 June 2022).
- The Federal Health Monitoring System. Definition: Degree of Disability. Available online: https://www.gbe-bund.de/gbe/ergebnisse.prc_tab?fid=8296&suchstring=&query_id=&sprache=E&fund_typ=DEF&methode=&vt=&verwandte=1&page_ret=0&seite=1&p_lfd_nr=13&p_news=&p_sprachkz=E&p_uid=gast&p_aid=18602946&hlp_nr=2&p_janein=J (accessed on 25 June 2022).
- The Federal Health Monitoring System. Definition: Severely Handicapped Persons. Available online: https://www.gbe-bund.de/gbe/ergebnisse.prc_tab?fid=2108&suchstring=&query_id=&sprache=E&fund_typ=DEF&methode=&vt=&verwandte=1&page_ret=0&seite=1&p_lfd_nr=15&p_news=&p_sprachkz=E&p_uid=gast&p_aid=18602946&hlp_nr=2&p_janein=J (accessed on 25 June 2022).
- Nieß, M.; Aichele, V. Selbstbestimmt Unterwegs in Berlin? Mobilität von Menschen mit Behinderungen aus Menschenrechtlicher Perspektive. Available online: http://www.institut-fuer-menschenrechte.de/fileadmin/user_upload/Publikationen/BERICHT/Bericht_Selbstbestimmt_unterwegs_in_Berlin.pdf (accessed on 25 June 2022).
- Römisch, K.; Tillmann, V. Mobilität als Voraussetzung für selbstbestimmte Mobilität im Sinnne der UN-BRK. Teilhabe 2017, 56, 100–1006. [Google Scholar]
- Hammel, J.; Jones, R.; Gossett, A.; Morgan, E. Examining barriers and supports to community living and participation after a stroke from a participatory action research approach. Top. Stroke Rehabil. 2006, 13, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.; Sakakibara, B.M.; Miller, W.C. A review of factors influencing participation in social and community activities for wheelchair users. Disabil. Rehabil. Assist. Technol. 2016, 11, 361–374. [Google Scholar] [CrossRef] [Green Version]
- Deutsches Institut für Menschenrechte. Mobilität von Menschen mit Behinderungen in Berlin Verbessern: Empfehlungen für Eine an der UN-Behindertenrechtskonvention Ausgerichtete Mobilitätsplanung. Available online: https://www.institut-fuer-menschenrechte.de/fileadmin/Redaktion/Publikationen/Position/Position_Mobilitaet_von_Menschen_mit_Behinderungen_in_Berlin_verbessern.pdf (accessed on 4 June 2022).
- Deutsche Presse-Agentur. Ist nur Jede Dritte Arztpraxis Behindertengerecht Ausgestattet? Available online: https://www.aerztezeitung.de/Wirtschaft/Ist-nur-jede-dritte-Arztpraxis-behindertengerecht-ausgestattet-409719.html (accessed on 4 June 2022).
- Pharr, J.R.; James, T.; Yeung, Y.-L. Accessibility and accommodations for patients with mobility disabilities in a large healthcare system: How are we doing? Disabil. Health J. 2019, 12, 679–684. [Google Scholar] [CrossRef]
- Ståhl, A.; Månsson Lexell, E. Facilitators for travelling with local public transport among people with mild cognitive limitations after stroke. Scand. J. Occup. Ther. 2018, 25, 108–118. [Google Scholar] [CrossRef] [Green Version]
- Jónasdóttir, S.K.; Egilson, S.Þ.; Polgar, J. Services, systems, and policies affecting community mobility for people with mobility impairments in Northern Iceland: An occupational perspective. J. Occup. Sci. 2018, 25, 309–321. [Google Scholar] [CrossRef]
- Pellichero, A.; Kenyon, L.K.; Best, K.L.; Lamontagne, M.-E.; Lavoie, M.D.; Sorita, É.; Routhier, F. Relationships between Cognitive Functioning and Powered Mobility Device Use: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 12467. [Google Scholar] [CrossRef]
- Christensen, E.R.; Golden, S.L.; Gesell, S.B. Perceived Benefits of Peer Support Groups for Stroke Survivors and Caregivers in Rural North Carolina. North Carol. Med. J. 2019, 80, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Wijekoon, S.; Wilson, W.; Gowan, N.; Ferreira, L.; Phadke, C.; Udler, E.; Bontempo, T. Experiences of Occupational Performance in Survivors of Stroke Attending Peer Support Groups. Can. J. Occup. Ther. 2020, 87, 173–181. [Google Scholar] [CrossRef]
- von Peter, S.; Bär, G.; Behrisch, B.; Bethmann, A.; Hartung, S.; Kasberg, A.; Wulff, I.; Wright, M. Partizipative Gesundheitsforschung in Deutschland–quo vadis? Gesundheitswesen 2020, 82, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Reuther, P. Teilhabe für Schwerbetroffene: Ambulante und mobile neurologische Rehabilitation im Wohn- und Lebensraum. In Teilhaben!!: NeuroRehabilitation und Nachsorge zu Teilhabe und Inklusion, 2nd ed.; Fries, W., Reuther, P., Lössl, H., Eds.; Aktualisierte und Erweiterte Auflage; Hippocampus: Bad Honnef, Germany, 2017; pp. 37–48. [Google Scholar]
- Doig, E.; Fleming, J.; Kuipers, P. Achieving Optimal Functional Outcomes in Community-Based Rehabilitation following Acquired Brain Injury: A Qualitative Investigation of Therapists’ Perspectives. Br. J. Occup. Ther. 2008, 71, 360–370. [Google Scholar] [CrossRef] [Green Version]
- Hillier, S.; Inglis-Jassiem, G. Rehabilitation for community-dwelling people with stroke: Home or centre based? A systematic review. Int. J. Stroke 2010, 5, 178–186. [Google Scholar] [CrossRef]
- Wilcock, A.A. An Occupational Perspective of Health, 2nd ed.; Slack: London, UK, 2006. [Google Scholar]
- Funke, A.; Grehl, T.; Großkreutz, J.; Münch, C.; Walter, B.; Kettemann, D.; Karnapp, C.; Gajewski, N.; Meyer, R.; Maier, A.; et al. Hilfsmittelversorgung bei der amyotrophen Lateralsklerose. Analyse aus 3 Jahren Fallmanagement in einem internetunterstützten Versorgungsnetzwerk. Nervenarzt 2015, 86, 1007–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sander, M.; Albrecht, M.; Loos, S.; Möllenkamp, M.; Stengel, V.; Igl, G. Leistungsbewilligungen und -Ablehnungen durch Krankenkassen; Studie für den Beauftragten der Bundesregierung für die Belange der Patientinnen und Patienten Sowie Bevollmächtigten für Pflege; IGES Institut: Berlin, Germany, 2017; Available online: https://www.iges.com/sites/igesgroup/iges.de/myzms/content/e6/e1621/e10211/e15829/e20499/e20500/e20502/attr_objs20506/StudiezuLeistungsbewilligungenund-ablehnungen_ger.pdf (accessed on 13 June 2022).
- Sergeant, S.; Peels, H.; Sandvoort, H.; Pseudonym, B.; Schelfhout, P.; de Schauwer, E. A collective biography on working relationships in inclusive research teams. Disabil. Soc. 2022, 1–18. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
|
|
|
|
|
| Alex 1 | Charlie | Chris | Mika | Lukas | |
|---|---|---|---|---|---|
| Age (years) | 49 | 52 | 37 | 54 | 36 |
| Sex (female/male) | f | f | m | f | m |
| Living condition | Alone, Apt. | Alone, Apt. | Alone, Apt. | Ass. LC | Ass. LC |
| Job status | SW | Retired | SW | Retired | SW |
| Year of stroke | 2010 | 2013 | 2012 | 2010 | 2005 |
| Symptoms 2 | Hemiplegia right, Aphasia, Apraxia of speech | Hemiplegia right | Hemiplegia left, Dysarthria | Hemiplegia right, Aphasia, Apraxia of speech | Hemiplegia left, Dysarthria |
| At home since (months) | 50 | 13 | 12 | 64 | 57 |
| Power wheelchair since (months) | 79 | 55 | 69 | 85 | 100 |
| Use of mobility device at home | No | WC | WC | WC, RR | PWC |
| GdB 3 (Degree of disability | 90 | 100 | 100 | 90 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Böttger, T.; Dennhardt, S.; Knape, J.; Marotzki, U. “Back into Life—With a Power Wheelchair”: Learning from People with Severe Stroke through a Participatory Photovoice Study in a Metropolitan Area in Germany. Int. J. Environ. Res. Public Health 2022, 19, 10465. https://doi.org/10.3390/ijerph191710465
Böttger T, Dennhardt S, Knape J, Marotzki U. “Back into Life—With a Power Wheelchair”: Learning from People with Severe Stroke through a Participatory Photovoice Study in a Metropolitan Area in Germany. International Journal of Environmental Research and Public Health. 2022; 19(17):10465. https://doi.org/10.3390/ijerph191710465
Chicago/Turabian StyleBöttger, Tabea, Silke Dennhardt, Julia Knape, and Ulrike Marotzki. 2022. "“Back into Life—With a Power Wheelchair”: Learning from People with Severe Stroke through a Participatory Photovoice Study in a Metropolitan Area in Germany" International Journal of Environmental Research and Public Health 19, no. 17: 10465. https://doi.org/10.3390/ijerph191710465
APA StyleBöttger, T., Dennhardt, S., Knape, J., & Marotzki, U. (2022). “Back into Life—With a Power Wheelchair”: Learning from People with Severe Stroke through a Participatory Photovoice Study in a Metropolitan Area in Germany. International Journal of Environmental Research and Public Health, 19(17), 10465. https://doi.org/10.3390/ijerph191710465