
Characteristics of Individuals in Japan Who Regularly Manage Their Oral Health by Having a Family Dentist: A Nationwide Cross-Sectional Web-Based Survey



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Outcome Variable
2.3. Explanatory Variables
2.4. Statistical Analysis
2.5. Ethical Consideration
3. Results
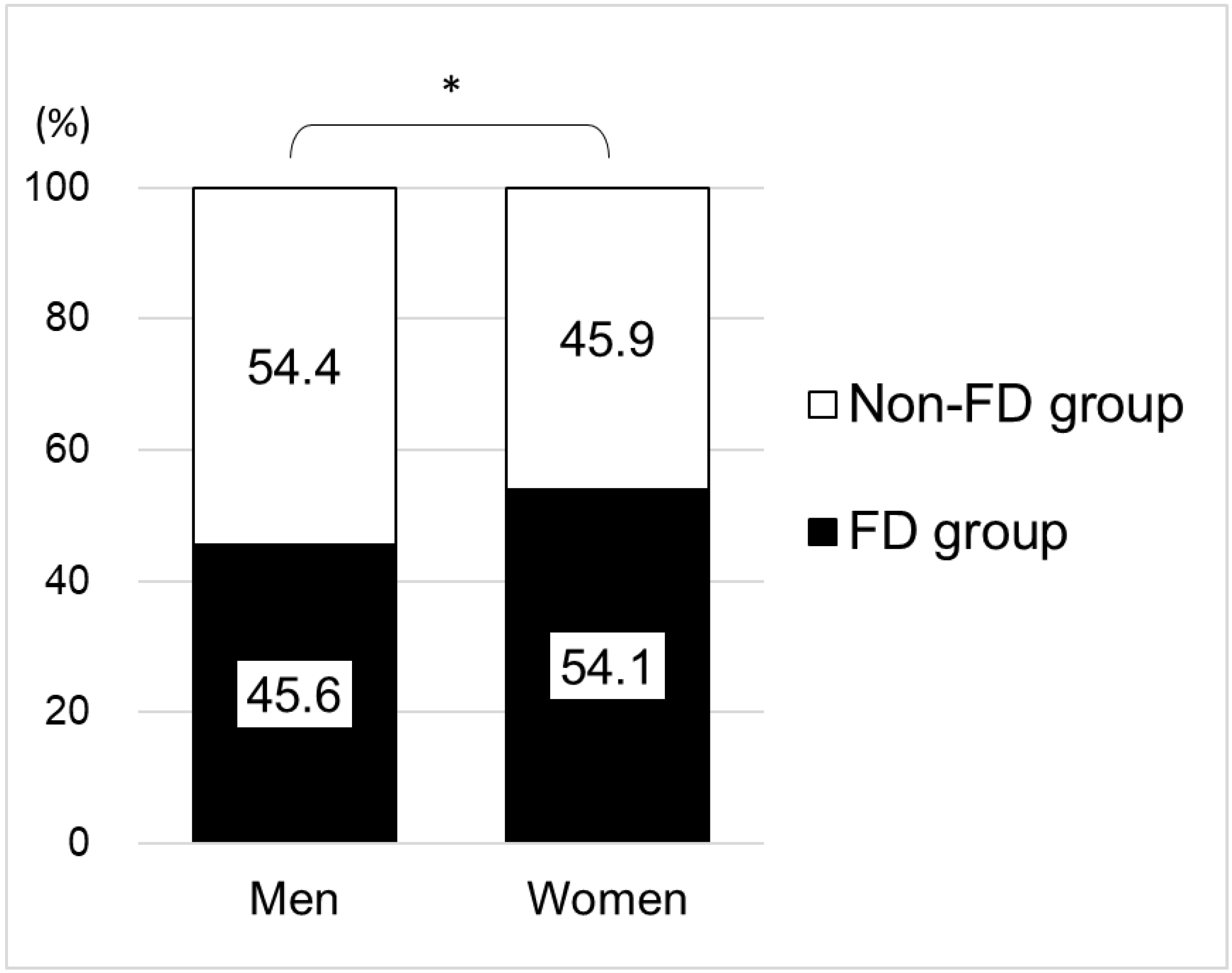
3.1. Characteristics of the Study Participants and Proportion of the FD Group by Gender
3.2. Relationship between Belonging to the FD Group or Not, and Characteristics of the Study Participants
3.3. Characteristics of Participants in the FD Group
4. Discussion
4.1. Main Findings
4.2. Proportion of the FD Group
4.3. Relationship between the FD Group and Individual Socioeconomic Factors
4.4. Relationship between the FD Group and Oral Health Status Factors
4.5. Implications of the Study
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomson, W.M.; Williams, S.M.; Broadbent, J.M.; Poulton, R.; Locker, D. Long-term dental visiting patterns and adult oral health. J. Dent. Res. 2010, 89, 307–311. [Google Scholar] [CrossRef]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Tooth loss and oral health-related quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [PubMed]
- Åstrøm, A.N.; Ekback, G.; Ordell, S.; Nasir, E. Long-term routine dental attendance: Influence on tooth loss and oral health-related quality of life in Swedish older adults. Community Dent. Oral Epidemiol. 2014, 42, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Anikeeva, O.; Brennan, D.S.; Teusner, D.N. Household income modifies the association of insurance and dental visiting. BMC Health Serv. Res. 2013, 13, 432. [Google Scholar] [CrossRef] [PubMed]
- Gnanamanickam, E.; Teusner, D.; Arrow, P.; Gnanamanickam, E.; Brennan, D.S.; Teusner, D.; Arrow, P. Dental insurance, service use and health outcomes in Australia: A systematic review. Aust. Dent. J. 2018, 63, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Zivkovic, N.; Aldossri, M.; Gomaa, N.; Farmer, J.W.; Singhal, S.; Quiñonez, C.; Ravaghi, V. Providing dental insurance can positively impact oral health outcomes in Ontario. BMC Health Serv. Res. 2020, 20, 124. [Google Scholar] [CrossRef]
- Lutfiyya, M.N.; Gross, A.J.; Soffe, B.; Lipsky, M.S. Dental care utilization: Examining the associations between health services deficits and not having a dental visit in past 12 months. BMC Public Health 2019, 19, 265. [Google Scholar] [CrossRef]
- Bernabé, E.; Masood, M.; Vujicic, M. The impact of out-of-pocket payments for dental care on household finances in low and middle income countries. BMC Public Health 2017, 17, 109. [Google Scholar] [CrossRef]
- World Health Organization. Health. Systems Financing: The Path to Universal Coverage World Health Report 2010. World Health Organization. 2010. Available online: https://www.who.int/publications/i/item/9789241564021 (accessed on 5 June 2022).
- United Nations Development Programme. The SDGs in Action. Available online: https://www.undp.org/sustainable-development-goals (accessed on 5 April 2022).
- Ministry of Health, Labour and Welfare. Health Insurance. Available online: https://www.mhlw.go.jp/english/policy/health-medical/health-insurance/index.html (accessed on 11 June 2022).
- Ministry of Health, Labour and Welfare. Survey of Medical Institutions. Available online: https://www.mhlw.go.jp/english/database/db-hss/smi.html (accessed on 11 April 2022).
- Health Japan 21 (The Second Term). Analysis and Assessments Project. Available online: https://www.nibiohn.go.jp/eiken/kenkounippon21/en/kenkounippon21/mokuhyou.html (accessed on 2 April 2022).
- Japan Dental Association. About the Family Dentist. Available online: https://www.jda.or.jp/jda/other/kakaritsuke.html (accessed on 15 June 2022).
- Graham, M.A.; Logan, H.L.; Tomar, S.L. Is trust a predictor of having a dental home? J. Am. Dent. Assoc. 2004, 135, 1550–1558. [Google Scholar] [CrossRef]
- Morita, I.; Nakagaki, H.; Toyama, A.; Hayashi, M.; Shimozato, M.; Watanabe, T.; Tohmatsu, S.; Igo, J.; Sheiham, A. Behavioral factors to include in guidelines for lifelong oral healthiness: An observational study in Japanese adults. BMC Oral Health. 2006, 6, 15. [Google Scholar] [CrossRef]
- Hanibuchi, T.; Aida, J.; Nakade, M.; Hirai, H.; Kondo, K. Geographical accessibility to dental care in the Japanese elderly. Community Dent. Health 2011, 28, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Kondo, K.; Hirai, H.; Nakade, M.; Aida, J.; Hirata, Y. Association between self-reported dental health status and onset of dementia: A 4-year prospective cohort study of older Japanese adults from the Aichi Gerontological Evaluation Study (AGES) Project. Psychosom. Med. 2012, 74, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Ueno, M.; Ohara, S.; Sawada, N.; Inoue, M.; Tsugane, S.; Kawaguchi, Y. The association of active and secondhand smoking with oral health in adults: Japan public health center-based study. Tob. Induc. Dis. 2015, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Gaber, A.; Galarneau, C.; Feine, J.S.; Emami, E. Rural-urban disparity in oral health-related quality of life. Community Dent. Oral Epidemiol. 2018, 46, 132–142. [Google Scholar] [CrossRef]
- Reynolds, J.C.; McKernan, S.C.; Sukalski, J.M.C.; Damiano, P.C. Evaluation of enrollee satisfaction with Iowa’s Dental Wellness Plan for the Medicaid expansion population. J. Public Health Dent. 2018, 78, 78–85. [Google Scholar] [CrossRef]
- Saadaldina, S.A.; Eldwakhly, E.; Alnazzawi, A.A.; Alharbi, R.A.; Alghamdi, B.K.; Abu Hammad, O.A.; Soliman, M. Awareness and Practice of Oral Health Measures in Medina, Saudi Arabia: An Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 9112. [Google Scholar] [CrossRef]
- Alhozgi, A.; Feine, J.S.; Tanwir, F.; Shrivastava, R.; Galarneau, C.; Emami, E. Rural-urban disparities in patient satisfaction with oral health care: A provincial survey. BMC Oral Health 2021, 21, 261. [Google Scholar] [CrossRef]
- Jessani, A.; Quadri, M.; Lefoka, P.; El-Rabbany, A.; Hooper, K.; Lim, H.; Ndobe, E.; Brondani, M.; Laronde, D. Oral Health Status and Patterns of Dental Service Utilization of Adolescents in Lesotho, Southern Africa. Children 2021, 8, 120. [Google Scholar] [CrossRef]
- Macromill, Inc. Available online: https://www.macromill.com (accessed on 20 June 2022).
- Ministry of Internal Affairs and Communications. Population Census. Available online: https://www.stat.go.jp/english/data/kokusei/index.html (accessed on 15 June 2022).
- Ministry of Health, Labour and Welfare. Interim Report of the “Conference on Enhancing the Qualities of the Dentists”. Available online: https://www.mhlw.go.jp/stf/shingi2/0000189587.html (accessed on 22 June 2022).
- Ministry of Health, Labour and Welfare. About Family Physician. Available online: https://kakarikata.mhlw.go.jp/kakaritsuke/motou.html (accessed on 23 June 2022).
- Ministry of Health, Labour and Welfare. National Health and Nutrition Survey. Available online: https://www.mhlw.go.jp/toukei/itiran/gaiyo/k-eisei.html (accessed on 16 June 2022).
- Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions. Available online: https://www.mhlw.go.jp/english/database/db-hss/cslc-tables.html (accessed on 17 June 2022).
- Ueno, M.; Zaitsu, T.; Shinada, K.; Ohara, S.; Kawaguchi, Y. Validity of the self-reported number of natural teeth in Japanese adults. J. Investig. Clin. Dent. 2010, 1, 79–84. [Google Scholar] [CrossRef]
- Matsui, D.; Yamamoto, T.; Nishigaki, M.; Miyatani, F.; Watanabe, I.; Koyama, T.; Ozaki, E.; Kuriyama, N.; Kanamura, N.; Watanabe, Y. Validity of self-reported number of teeth and oral health variables. BMC Oral Health 2016, 17, 17. [Google Scholar] [CrossRef]
- Macromill, Inc. Privacy Policy. Available online: https://www.macromill.com/privacy.html (accessed on 20 June 2022).
- Reda, S.F.; Reda, S.M.; Thomson, W.M.; Schwendicke, F. Inequality in Utilization of Dental Services: A Systematic Review and Meta-analysis. Am. J. Public Health 2018, 108, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, M.S.; Su, S.; Crespo, C.J.; Hung, M. Men and Oral Health: A Review of Sex and Gender Differences. Am. J. Men’s Health 2021, 15, 15579883211016361. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Survey of Dental Diseases. Available online: https://www.mhlw.go.jp/toukei/list/62-17.html (accessed on 13 June 2022).
- Ministry of Health, Labour and Welfare. Patient Survey. Available online: https://www.mhlw.go.jp/english/database/db-hss/ps.html (accessed on 13 June 2022).
- Hadler-Olsen, E.; Jonsson, B. Oral health and use of dental services in different stages of adulthood in Norway: A cross sectional study. BMC Oral Health 2021, 21, 257. [Google Scholar] [CrossRef] [PubMed]
- Okawa, Y.; Hirata, S. Trends in the geographic distribution on dental clinics in Japan. Community Dent. Health 2014, 31, 62–64. [Google Scholar] [CrossRef]
- Marchesan, J.; Morelli, T.; Moss, K.; Preisser, J.; Zandona, A.; Offenbacher, S.; Beck, J. Interdental cleaning is associated with decreased oral disease prevalence. J. Dent. Res. 2018, 97, 773–778. [Google Scholar] [CrossRef]
- Ministry of Internal Affairs and Communications. Internet Usage. Available online: https://www.soumu.go.jp/johotsusintokei/whitepaper/ja/r03/html/nd242120.html (accessed on 22 June 2022).
- Ahmad, T.; Haroon, H.; Baig, M.; Hui, J. Coronavirus Disease 2019 (COVID-19) Pandemic and Economic Impact. Pak. J. Med. Sci. 2020, 36, S73–S78. [Google Scholar] [CrossRef]


{kind=link}
| Total | Men | Women | ||||
|---|---|---|---|---|---|---|
| Variable | Number | (%) | Number | (%) | Number | (%) |
| Total | 3556 | (100.0) | 1708 | (100.0) | 1848 | (100.0) |
| Age | ||||||
| 20–29 years | 430 | (12.1) | 218 | (12.8) | 212 | (11.4) |
| 30–39 years | 545 | (15.0) | 271 | (15.9) | 264 | (14.3) |
| 40–49 years | 629 | (17.7) | 317 | (18.5) | 312 | (16.9) |
| 50–59 years | 529 | (14.9) | 263 | (15.4) | 266 | (14.4) |
| 60–69 years | 618 | (17.4) | 302 | (17.7) | 316 | (17.1) |
| ≥70 years | 815 | (22.9) | 337 | (19.7) | 478 | (25.9) |
| Household income | ||||||
| <JPY 2000 K | 299 | (8.4) | 114 | (6.7) | 185 | (10.0) |
| JPY 2000 K–< 4000 K | 850 | (23.9) | 427 | (25.0) | 423 | (22.9) |
| JPY 4000 K–< 6000 K | 703 | (19.8) | 371 | (21.7) | 332 | (18.0) |
| JPY 6000 K–< 8000 K | 455 | (12.8) | 241 | (14.1) | 214 | (11.6) |
| ≥JPY 8000 K | 478 | (13.4) | 284 | (16.6) | 194 | (10.5) |
| Unknown | 771 | (21.7) | 271 | (15.9) | 500 | (27.0) |
| Employment status | ||||||
| Regular employee | 1351 | (38.0) | 947 | (55.4) | 404 | (21.9) |
| Non-regular employee | 454 | (12.8) | 112 | (6.6) | 342 | (18.5) |
| Homemaker | 756 | (21.3) | 5 | (0.3) | 751 | (40.6) |
| Self-employed and others | 339 | (9.5) | 212 | (12.4) | 127 | (6.8) |
| Not working | 656 | (18.4) | 432 | (25.3) | 224 | (12.1) |
| Marital status | ||||||
| Married | 2296 | (64.6) | 1073 | (62.8) | 1223 | (66.2) |
| Single | 1260 | (35.4) | 635 | (37.2) | 625 | (33.8) |
| Child status | ||||||
| With children | 2233 | (62.8) | 958 | (56.1) | 1275 | (69.0) |
| No children | 1323 | (37.2) | 750 | (43.9) | 573 | (31.0) |
| Municipalities | ||||||
| Metropolis (pop 500,000+) | 1242 | (34.9) | 597 | (34.9) | 645 | (34.9) |
| Core cities (pop 200,000+) | 685 | (19.3) | 337 | (19.7) | 348 | (18.8) |
| Cities (pop 50,000+) | 1417 | (39.8) | 669 | (39.2) | 748 | (40.5) |
| Towns and villages | 212 | (6.0) | 105 | (6.2) | 107 | (5.8) |
| Number of teeth | ||||||
| 0–9 | 183 | (5.2) | 111 | (6.5) | 72 | (3.9) |
| 10–19 | 369 | (10.4) | 176 | (10.3) | 193 | (10.4) |
| 20–27 | 1392 | (39.1) | 673 | (39.4) | 719 | (38.9) |
| ≥28 | 1612 | (45.3) | 748 | (43.8) | 864 | (46.8) |
| Frequency of brushing teeth | ||||||
| ≥Three times daily | 928 | (26.1) | 328 | (19.2) | 600 | (32.5) |
| Twice daily | 1894 | (53.3) | 885 | (51.8) | 1009 | (54.6) |
| Once daily | 674 | (18.9) | 442 | (25.9) | 232 | (12.5) |
| Sometimes/No brushing | 60 | (1.7) | 53 | (3.1) | 7 | (0.4) |
| Interdental cleaning | ||||||
| Yes | 2040 | (57.6) | 832 | (49.1) | 1208 | (65.4) |
| No | 1500 | (42.4) | 862 | (50.9) | 638 | (34.6) |
| Men | Women | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Total Number | FD Group | Non-FD Group | χ2-Value | p-Value | Total Number | FD Group | Non-FD Group | Χ2 Value | p-Value | ||||
| Total, n (%) | 1708 | 779 | (45.6) | 929 | (54.4) | 1848 | 999 | (54.1) | 849 | (45.9) | ||||
| Age, n (%) | ||||||||||||||
| 20–29 years | 218 | 76 | (34.9) | 142 | (65.1) | χ2(5) = 71.58 | <0.001 | 212 | 84 | (39.6) | 128 | (60.4) | χ2(5) = 68.86 | <0.001 |
| 30–39 years | 271 | 96 | (35.4) | 175 | (64.6) | 264 | 124 | (47.0) | 140 | (53.0) | ||||
| 40–49 years | 317 | 133 | (42.0) | 184 | (58.0) | 312 | 160 | (51.3) | 152 | (48.7) | ||||
| 50–59 years | 263 | 108 | (41.1) | 155 | (58.9) | 266 | 119 | (44.7) | 147 | (55.3) | ||||
| 60–69 years | 302 | 152 | (50.3) | 150 | (49.7) | 316 | 198 | (62.7) | 118 | (37.3) | ||||
| ≥70 years | 337 | 214 | (63.5) | 123 | (36.5) | 478 | 314 | (65.7) | 164 | (34.3) | ||||
| Household income, n (%) | ||||||||||||||
| <JPY 2000 K | 114 | 42 | (36.8) | 72 | (63.2) | χ2(5) = 27.54 | <0.001 | 185 | 89 | (48.1) | 96 | (51.9) | χ2(5) = 12.40 | 0.030 |
| JPY 2000 K–<4000 K | 427 | 212 | (49.6) | 215 | (50.4) | 423 | 233 | (55.1) | 190 | (44.9) | ||||
| JPY 4000 K–<6000 K | 371 | 165 | (44.5) | 206 | (55.5) | 332 | 194 | (58.4) | 138 | (41.6) | ||||
| JPY 6000 K–<8000 K | 241 | 113 | (46.9) | 128 | (53.1) | 214 | 121 | (56.5) | 93 | (43.5) | ||||
| ≥JPY 8000 K | 284 | 153 | (53.9) | 131 | (46.1) | 194 | 115 | (59.3) | 79 | (40.7) | ||||
| Unknown | 271 | 94 | (34.7) | 177 | (65.3) | 500 | 247 | (49.4) | 253 | (50.6) | ||||
| Employment status, n (%) | ||||||||||||||
| Regular employee | 947 | 415 | (43.8) | 532 | (56.2) | χ2(4) = 9.52 | 0.049 | 404 | 194 | (48.0) | 210 | (52.0) | χ2(4) = 13.48 | 0.090 |
| Non-regular employee | 112 | 45 | (40.2) | 67 | (59.8) | 342 | 188 | (55.0) | 154 | (45.0) | ||||
| Homemaker | 5 | 3 | (60.0) | 2 | (40.0) | 751 | 439 | (58.5) | 312 | (41.5) | ||||
| Self-employed and others | 212 | 93 | (43.9) | 119 | (56.1) | 127 | 64 | (50.4) | 63 | (49.6) | ||||
| Not working | 432 | 223 | (51.6) | 209 | (48.4) | 224 | 114 | (50.9) | 110 | (49.1) | ||||
| Marital status, n (%) | ||||||||||||||
| Married | 1073 | 549 | (51.2) | 524 | (48.8) | χ2(1) = 35.91 | <0.001 | 1223 | 698 | (57.1) | 525 | (42.9) | χ2(1) = 13.23 | <0.001 |
| Single | 635 | 230 | (36.2) | 405 | (63.8) | 625 | 301 | (48.2) | 324 | (51.8) | ||||
| Child status, n (%) | ||||||||||||||
| With children | 958 | 484 | (50.5) | 474 | (49.5) | χ2(1) = 21.23 | <0.001 | 1275 | 732 | (57.4) | 543 | (42.6) | χ2(1) = 18.62 | <0.001 |
| No children | 750 | 295 | (39.3) | 455 | (60.7) | 573 | 267 | (46.6) | 306 | (53.4) | ||||
| Municipalities, n (%) | ||||||||||||||
| Metropolis (pop 500,000+) | 597 | 275 | (46.1) | 322 | (53.9) | χ2(3) = 6.13 | 0.105 | 645 | 369 | (57.2) | 276 | (42.8) | χ2(3) = 4.42 | 0.219 |
| Core cities (pop 200,000+) | 337 | 161 | (47.8) | 176 | (52.2) | 348 | 181 | (52.0) | 167 | (48.0) | ||||
| Cities (pop 50,000+) | 669 | 307 | (45.9) | 362 | (54.1) | 748 | 396 | (52.9) | 352 | (47.1) | ||||
| Towns and villages | 105 | 36 | (34.3) | 69 | (65.7) | 107 | 53 | (49.5) | 54 | (50.5) | ||||
| Number of teeth, n (%) | ||||||||||||||
| 0–9 | 111 | 40 | (36.0) | 71 | (64.0) | χ2(3) = 18.23 | <0.001 | 72 | 28 | (38.9) | 44 | (61.1) | χ2(3) = 12.79 | 0.005 |
| 10–19 | 176 | 98 | (55.7) | 78 | (44.3) | 193 | 111 | (57.5) | 82 | (42.5) | ||||
| 20–27 | 673 | 328 | (48.7) | 345 | (51.3) | 719 | 413 | (57.4) | 306 | (42.6) | ||||
| ≥28 | 748 | 313 | (41.8) | 435 | (58.2) | 864 | 447 | (51.7) | 417 | (48.3) | ||||
| Frequency of brushing teeth, n (%) | ||||||||||||||
| ≥Three times daily | 328 | 191 | (58.2) | 137 | (41.8) | χ2(3) = 42.26 | <0.001 | 600 | 368 | (61.3) | 232 | (38.7) | χ2(3) = 23.95 | <0.001 |
| Twice daily | 885 | 405 | (45.8) | 480 | (54.2) | 1009 | 520 | (51.5) | 489 | (48.5) | ||||
| Once daily | 442 | 172 | (38.9) | 270 | (61.1) | 232 | 110 | (47.4) | 122 | (52.6) | ||||
| Sometimes/no brushing | 53 | 11 | (20.8) | 42 | (79.2) | 7 | 1 | (14.3) | 6 | (85.7) | ||||
| Interdental cleaning, n (%) | ||||||||||||||
| Yes | 832 | 524 | (63.0) | 308 | (37.0) | χ2(1) = 192.85 | <0.001 | 1208 | 798 | (66.1) | 410 | (33.9) | χ2(1) = 202.56 | <0.001 |
| No | 862 | 253 | (29.4) | 609 | (70.6) | 638 | 200 | (31.3) | 438 | (68.7) |
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p Value | OR | 95% CI | p-Value |
| Age | ||||||
| 20–29 years | 0.90 | (0.61–1.32) | 0.582 | 1.03 | (0.69–1.55) | 0.880 |
| 30–39 years | 0.79 | (0.57–1.12) | 0.185 | 0.84 | (0.58–1.20) | 0.328 |
| 40–49 years | 1.00 | Reference | 1.00 | Reference | ||
| 50–59 years | 0.92 | (0.66–1.29) | 0.638 | 0.99 | (0.69–1.42) | 0.947 |
| 60–69 years | 1.46 | (1.04–2.05) | 0.030 | 1.33 | (0.92–1.92) | 0.124 |
| ≥70 years | 2.50 | (1.68–3.72) | <0.001 | 2.41 | (1.56–3.71) | <0.001 |
| Household income | ||||||
| <JPY 2000 K | 0.74 | (0.46–1.18) | 0.204 | 0.95 | (0.57–1.59) | 0.835 |
| JPY 2000 K–<4000 K | 1.10 | (0.82–1.48) | 0.530 | 1.12 | (0.81–1.53) | 0.495 |
| JPY 4000 K–<6000 K | 1.00 | Reference | 1.00 | Reference | ||
| JPY 6000 K–<8000 K | 1.15 | (0.82–1.61) | 0.416 | 1.09 | (0.76–1.55) | 0.637 |
| ≥JPY 8000 K | 1.58 | (1.14–2.18) | 0.006 | 1.47 | (1.05–2.08) | 0.027 |
| Unknown | 0.76 | (0.54–1.07) | 0.119 | 0.80 | (0.56–1.15) | 0.230 |
| Employment status | ||||||
| Regular employee | 1.00 | Reference | 1.00 | Reference | ||
| Non–regular employee | 0.86 | (0.56–1.34) | 0.516 | 0.85 | (0.53–1.35) | 0.483 |
| Homemaker | 1.61 | (0.25–10.56) | 0.619 | 1.49 | (0.20–11.26) | 0.698 |
| Self–employed and others | 0.83 | (0.59–1.15) | 0.260 | 0.82 | (0.57–1.16) | 0.258 |
| Not working | 0.96 | (0.70–1.32) | 0.808 | 0.92 | (0.65–1.30) | 0.633 |
| Marital status | ||||||
| Married | 1.36 | (1.00–1.85) | 0.052 | 1.32 | (0.95–1.83) | 0.099 |
| Single | 1.00 | Reference | Reference | |||
| Child status | ||||||
| With children | 0.90 | (0.67–1.20) | 0.462 | 0.88 | (0.65–1.19) | 0.409 |
| No children | 1.00 | Reference | Reference | |||
| Municipalities | ||||||
| Metropolis (pop 500,000+) | 1.00 | (0.79–1.26) | 0.980 | 0.90 | (0.70–1.15) | 0.388 |
| Core cities (pop 200,000+) | 1.08 | (0.82–1.42) | 0.588 | 1.08 | (0.81–1.44) | 0.614 |
| Cities (pop 50,000+) | 1.00 | Reference | 1.00 | Reference | ||
| Towns and villages | 0.56 | (0.36–0.87) | 0.010 | 0.52 | (0.32–0.83) | 0.007 |
| Number of teeth | ||||||
| 0–9 | 1.00 | Reference | ||||
| 10–19 | 1.57 | (0.90–2.72) | 0.110 | |||
| 20–27 | 1.21 | (0.75–1.93) | 0.436 | |||
| ≥28 | 1.07 | (0.66–1.72) | 0.794 | |||
| Frequency of brushing teeth | ||||||
| ≥Three times daily | 1.60 | (1.16–2.20) | 0.004 | |||
| Twice daily | 1.27 | (0.99–1.64) | 0.064 | |||
| Once daily | 1.00 | Reference | ||||
| Sometimes/no brushing | 0.55 | (0.24–1.30) | 0.176 | |||
| Interdental cleaning | ||||||
| Yes | 3.66 | (2.95–4.54) | <0.001 | |||
| No | 1.00 | Reference | ||||
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p Value | OR | 95% CI | p-Value |
| Age | ||||||
| 20–29 years | 0.69 | (0.48–0.99) | 0.045 | 0.85 | (0.57–1.25) | 0.410 |
| 30–39 years | 0.84 | (0.60–1.17) | 0.297 | 0.93 | (0.65–1.32) | 0.678 |
| 40–49 years | 1.00 | Reference | 1.00 | Reference | ||
| 50–59 years | 0.76 | (0.55–1.07) | 0.112 | 0.71 | (0.50–1.00) | 0.052 |
| 60–69 years | 1.67 | (1.20–2.32) | 0.002 | 1.52 | (1.07–2.16) | 0.020 |
| ≥70 years | 2.01 | (1.46–2.78) | <0.001 | 1.73 | (1.22–2.46) | 0.002 |
| Household income | ||||||
| <JPY 2000 K | 0.61 | (0.41–0.90) | 0.014 | 0.61 | (0.40–0.92) | 0.019 |
| JPY 2000 K–<4000 K | 0.81 | (0.60–1.10) | 0.174 | 0.79 | (0.57–1.09) | 0.147 |
| JPY 4000 K–<6000 K | 1.00 | Reference | 1.00 | Reference | ||
| JPY 6000 K–<8000 K | 0.96 | (0.67–1.38) | 0.838 | 0.96 | (0.66–1.40) | 0.818 |
| ≥JPY 8000 K | 1.07 | (0.74–1.55) | 0.724 | 0.91 | (0.62–1.35) | 0.649 |
| Unknown | 0.79 | (0.59–1.05) | 0.106 | 0.77 | (0.57–1.05) | 0.094 |
| Employment status | ||||||
| Regular employee | 1.00 | Reference | 1.00 | Reference | ||
| Non-regular employee | 1.12 | (0.82–1.53) | 0.466 | 1.16 | (0.83–1.61) | 0.385 |
| Homemaker | 0.93 | (0.70–1.26) | 0.654 | 0.98 | (0.72–1.34) | 0.899 |
| Self-employed and others | 0.81 | (0.53–1.23) | 0.321 | 0.91 | (0.58–1.43) | 0.691 |
| Not working | 0.86 | (0.59–1.24) | 0.408 | 0.86 | (0.58–1.27) | 0.440 |
| Marital status | ||||||
| Married | 1.15 | (0.89–1.50) | 0.285 | 1.08 | (0.82–1.42) | 0.583 |
| Single | 1.00 | Reference | Reference | |||
| Child status | ||||||
| With children | 1.08 | (0.85–1.38) | 0.529 | 1.10 | (0.86–1.42) | 0.444 |
| No children | 1.00 | Reference | Reference | |||
| Municipalities | ||||||
| Metropolis (pop 500,000+) | 1.19 | (0.96–1.49) | 0.115 | 1.07 | (0.85–1.35) | 0.560 |
| Core cities (pop 200,000+) | 0.96 | (0.74–1.25) | 0.769 | 0.90 | (0.68–1.18) | 0.440 |
| Cities (pop 50,000+) | 1.00 | Reference | 1.00 | Reference | ||
| Towns and villages | 0.86 | (0.57–1.31) | 0.492 | 0.87 | (0.56–1.35) | 0.524 |
| Number of teeth | ||||||
| 0–9 | 1.00 | Reference | ||||
| 10–19 | 1.46 | (0.80–2.67) | 0.216 | |||
| 20–27 | 1.62 | (0.94–2.80) | 0.082 | |||
| ≥28 | 1.46 | (0.85–2.51) | 0.175 | |||
| Frequency of brushing teeth | ||||||
| ≥Three times daily | 1.21 | (0.86–1.69) | 0.275 | |||
| Twice daily | 0.91 | (0.67–1.25) | 0.577 | |||
| Once daily | 1.00 | Reference | ||||
| Sometimes/no brushing | 1.00 | (omitted) | ||||
| Interdental cleaning | ||||||
| Yes | 3.68 | (2.96–4.57) | <0.001 | |||
| No | 1.00 | Reference | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oshima, K.; Miura, H.; Tano, R.; Fukuda, H. Characteristics of Individuals in Japan Who Regularly Manage Their Oral Health by Having a Family Dentist: A Nationwide Cross-Sectional Web-Based Survey. Int. J. Environ. Res. Public Health 2022, 19, 10479. https://doi.org/10.3390/ijerph191710479
Oshima K, Miura H, Tano R, Fukuda H. Characteristics of Individuals in Japan Who Regularly Manage Their Oral Health by Having a Family Dentist: A Nationwide Cross-Sectional Web-Based Survey. International Journal of Environmental Research and Public Health. 2022; 19(17):10479. https://doi.org/10.3390/ijerph191710479
Chicago/Turabian StyleOshima, Katsuo, Hiroko Miura, Rumi Tano, and Hideki Fukuda. 2022. "Characteristics of Individuals in Japan Who Regularly Manage Their Oral Health by Having a Family Dentist: A Nationwide Cross-Sectional Web-Based Survey" International Journal of Environmental Research and Public Health 19, no. 17: 10479. https://doi.org/10.3390/ijerph191710479
APA StyleOshima, K., Miura, H., Tano, R., & Fukuda, H. (2022). Characteristics of Individuals in Japan Who Regularly Manage Their Oral Health by Having a Family Dentist: A Nationwide Cross-Sectional Web-Based Survey. International Journal of Environmental Research and Public Health, 19(17), 10479. https://doi.org/10.3390/ijerph191710479