
Endothelial Function Assessment by Flow-Mediated Dilation Method: A Valuable Tool in the Evaluation of the Cardiovascular System


 ,
,  and
and 
Abstract
:1. Introduction
1.1. Cardiovascular Diseases
1.2. Endothelial Dysfunction and Its Role in the Pathogenesis of Cardiovascular Diseases
1.3. Methods of the Endothelial Function Assessment
1.4. The Purpose of This Paper
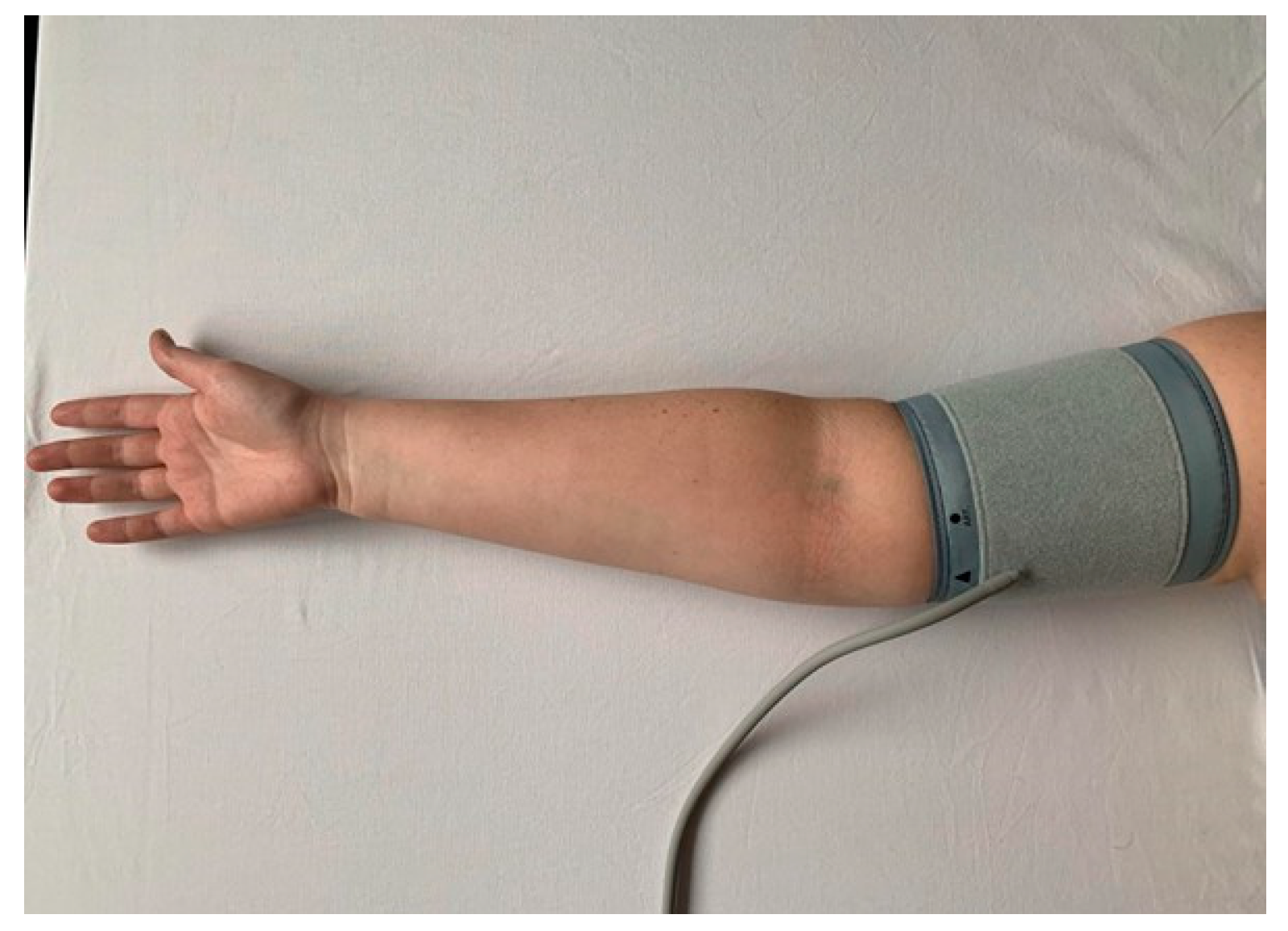
2. Methodology of the FMD Procedure
2.1. Preparation for Examination
2.2. Technical Background
2.3. Procedure of the Examination
2.4. Reference Range
3. FMD in Patients with Obesity, Metabolic Syndrome, and Its Components
3.1. FMD Results in Patients with Obesity
3.2. FMD Results in Patients with Metabolic Syndrome
3.3. FMD Results in Patients with Diabetes Mellitus
3.4. FMD Results in Patients with Hypertension
3.5. FMD Results in Patients with Dyslipidemia
4. FMD in Patients with Cardiovascular Disease
4.1. Coronary Artery Disease
4.2. Peripheral Arterial Disease
4.3. Chronic Kidney Disease
5. FMD Results and Biochemical Changes
6. FMD Results and Physical Activity
7. FMD Results in Pregnancy
8. FMD Results in Patients with COVID-19
9. Current Limitations of FMD Procedure and Future Trends
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Townsend, N.; Kazakiewicz, D.; Lucy Wright, F.; Timmis, A.; Huculeci, R.; Torbica, A.; Gale, C.P.; Achenbach, S.; Weidinger, F.; Vardas, P. Epidemiology of cardiovascular disease in Europe. Nat. Rev. Cardiol. 2022, 19, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D. Epidemiological features of cardiovascular disease in Asia. JACC Asia 2021, 1, 1–13. [Google Scholar] [CrossRef]
- Flores-Gomez, D.; Bekkering, S.; Netea, M.G.; Riksen, N.P. Trained immunity in atherosclerotic cardiovascular disease. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 62–69. [Google Scholar] [CrossRef]
- Cismaru, G.; Serban, T.; Tirpe, A. Ultrasound methods in the evaluation of atherosclerosis: From pathophysiology to clinic. Biomedicines 2021, 9, 418. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Chronic lower extremity ischemia and its association with the frailty syndrome in patients with diabetes. Int. J. Environ. Res. Public Health 2020, 17, 9339. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Pathogenesis and clinical significance of in-stent restenosis in patients with diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef]
- Cahill, P.A.; Redmond, E.M. Vascular endothelium–gatekeeper of vessel health. Atherosclerosis 2016, 248, 97–109. [Google Scholar] [CrossRef]
- Stanek, A.; Fazeli, B.; Bartuś, S.; Sutkowska, E. The Role of endothelium in physiological and pathological states: New data. BioMed Res. Int. 2018, 2018, 1098039. [Google Scholar] [CrossRef]
- Ushiyama, A.; Kataoka, H.; Iijima, T. Glycocalix and its involvement in clinical pathophysiologies. J. Intens. Care 2016, 4, 59. [Google Scholar] [CrossRef]
- Krüger-Genge, A.; Blocki, A.; Franke, R.P.; Jung, F. Vascular endothelial cell biology: An update. Int. J. Mol. Sci. 2019, 20, 4411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Vanhoutte, P.M.; Leung, S.W. Vascular nitric oxide: Beyond eNOS. J. Pharmacol. Sci. 2015, 129, 83–94. [Google Scholar] [CrossRef]
- Mitchell, J.A.; Kirkby, N.S. Eicosanoids, prostacyclin and cyclooxygenase in the cardiovascular system. Br. J. Pharmacol. 2019, 176, 1038–1050. [Google Scholar] [CrossRef] [PubMed]
- Kostov, K. The causal relationship between endothelin-1 and hypertension: Focusing on endothelial dysfunction, arterial stiffness, vascular remodeling, and blood pressure regulation. Life 2021, 11, 986. [Google Scholar] [CrossRef] [PubMed]
- Khurana, V.; Goswami, B. Angiotensin converting enzyme (ACE). Clin. Chim. Acta 2022, 524, 113–122. [Google Scholar] [CrossRef]
- Ambrosino, P.; Bachetti, T.; Ennio, S.; D’Anna, S.E.; Galloway, B.; Bianco, A.; D’Agnano, V.; Papa, A.; Motta, A.; Perrotta, F.; et al. Mechanisms and clinical implications of endothelial dysfunction in arterial hypertension. J. Cardiovasc. Dev. Dis. 2022, 9, 136. [Google Scholar] [CrossRef]
- Blaya, D.; Rubio-Tomás, T.; Rodrigo-Torres, D.; Lozano, J.; Coll, M.; Argemi, J.; Altamirano, J.; Affò, S.; Morales-Ibanez, O.; Gratacós-Ginès, J.; et al. Endothelial dysfunction markers predict short-term mortality in patients with severe alcoholic hepatitis. Hepatol. Int. 2021, 15, 1006–1017. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.; Saha, A.; Dubey, N.K.; Kapoor, K.; Anubhuti Batra, V.V.; Upadhayay, A.D. Endothelial dysfunction in children with idiopathic nephrotic syndrome. Atherosclerosis 2014, 233, 704–706. [Google Scholar] [CrossRef]
- Wiseman, S.J.; Doubal, F.N.; Chappell, F.M.; Valdés-Hernández, M.C.; Wang, X.; Rumley, A.; Lowe, G.D.; Dennis, M.S.; Wardlaw, J.M. Plasma biomarkers of inflammation, endothelial function and hemostasis in cerebral small vessel disease. Cerebrovasc. Dis. 2015, 40, 157–164. [Google Scholar] [CrossRef]
- Di Minno, A.; Gentile, M.; Iannuzzo, G.; Calcaterra, I.; Tripaldella, M.; Porro, B.; Cavalca, V.; Di Taranto, M.D.; Tremoli, E.; Fortunato, G.; et al. Endothelial function improvement in patients with familial hypercholesterolemia receiving PCSK-9 inhibitors on top of maximally tolerated lipid lowering therapy. Thromb. Res. 2020, 194, 229–236. [Google Scholar] [CrossRef]
- Williams, S.B.; Goldfine, A.B.; Timimi, F.K.; Ting, H.H.; Roddy, M.A.; Simonson, D.C.; Creager, M.A. Acute hyperglycemia attenuates endothelium-dependent vasodilation in humans in vivo. Circulation 1998, 97, 1695–1701. [Google Scholar] [CrossRef] [Green Version]
- AlBadri, A.; Wei, J.; Mehta, P.K.; Landes, S.; Petersen, J.W.; Anderson, R.D.; Samuels, B.; Azarbal, B.; Handberg, E.M.; Li, Q.; et al. Acetylcholine versus cold pressor testing for evaluation of coronary endothelial function. PLoS ONE 2017, 12, e0172538. [Google Scholar] [CrossRef]
- Chia, P.Y.; Teo, A.; Yeo, T.W. Overview of the assessment of endothelial function in humans. Front. Med. 2020, 7, 542567. [Google Scholar] [CrossRef]
- Chevalier, L.; Selim, J.; Castro, C.; Cuvilly, F.; Baste, J.M.; Richard, V.; Pareige, P.; Bellien, J. Combined electron microscopy approaches for arterial glycocalyx visualization. Front. Cardiovasc. Med. 2022, 9, 840689. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Gu, S.; Song, Y.; Ji, X.; Zeng, W.; Wang, X.; Wang, Y.; Feng, Q. The impact of cardiomotor rehabilitation on endothelial function in elderly patients with chronic heart failure. BMC Cardiovasc. Disord. 2021, 21, 524. [Google Scholar] [CrossRef]
- Wautier, J.L.; Wautier, M.P. Endothelial cell participation in inflammatory reaction. Int. J. Mol. Sci. 2021, 22, 6341. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, D.H.J.; Bruno, R.M.; van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, C.M.; Aznaouridis, K.A.; Karatzis, E.N.; Karatzi, K.N.; Stamatelopoulos, K.S.; Vamvakou, G.; Lekakis, J.P.; Mavrikakis, M.E. Effect of coffee on endothelial function in healthy subjects: The role of caffeine. Clin. Sci. 2005, 109, 55–60. [Google Scholar] [CrossRef]
- Shechter, M.; Shalmon, G.; Scheinowitz, M.; Koren-Morag, N.; Feinberg, M.S.; Harats, D.; Sela, B.A.; Sharabi, Y.; Chouraqui, P. Impact of acute caffeine ingestion on endothelial function in subjects with and without coronary artery disease. Am. J. Cardiol. 2011, 107, 1255–1261. [Google Scholar] [CrossRef] [PubMed]
- Bau, P.F.D.; Bau, C.H.D.; Naujorks, A.A.; Rosito, G.A. Early and late effects of alcohol ingestion on blood pressure and endothelial function. Alcohol 2005, 37, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Dawson, E.A.; Green, D.J.; Cable, N.T.; Thijssen, D.H.J. Effects of acute exercise on flow-mediated dilatation in healthy humans. J. Appl. Physiol. 2013, 115, 1589–1598. [Google Scholar] [CrossRef]
- George, J.; Hussain, M.; Vadiveloo, T.; Ireland, S.; Hopkinson, P.; Struthers, A.D.; Donnan, P.T.; Khan, F.; Lang, C.C. Cardiovascular effects of switching from tobacco cigarettes to electronic cigarettes. J. Am. Coll. Cardiol. 2019, 74, 3112–3120. [Google Scholar] [CrossRef]
- Ghiadoni, L.; Donald, A.E.; Cropley, M.; Mullen, M.J.; Oakley, G.; Taylor, M.; O’Connor, G.; Betteridge, J.; Klein, N.; Steptoe, A.; et al. Mental stress induces transient endothelial dysfunction in humans. Circulation 2000, 102, 2473–2478. [Google Scholar] [CrossRef] [PubMed]
- Flammer, A.J.; Anderson, T.; Celermajer, D.S.; Creager, M.A.; Deanfield, J.; Ganz, P.; Hamburg, N.M.; Lüscher, T.F.; Shechter, M.; Taddei, S.; et al. The assessment of endothelial function: From research into clinical practice. Circulation 2012, 126, 753–767. [Google Scholar] [CrossRef]
- Donald, A.E.; Charakida, M.; Cole, T.J.; Friberg, P.; Chowienczyk, P.J.; Millasseau, S.C.; Deanfield, J.E.; Halcox, J.P. Non-invasive assessment of endothelial function: Which technique? J. Am. Coll. Cardiol. 2006, 48, 1846–1850. [Google Scholar] [CrossRef] [PubMed]
- Ghiadoni, L.; Faita, F.; Salvetti, M.; Cordiano, C.; Biggi, A.; Puato, M.; Di Monaco, A.; De Siati, L.; Volpe, M.; Ambrosio, G.; et al. Assessment of flow-mediated dilation reproducibility: A nationwide multicenter study. J. Hypertens. 2012, 30, 1399–1405. [Google Scholar] [CrossRef]
- Kobayashi, K.; Akishita, M.; Yu, W.; Hashimoto, M.; Ohni, M.; Toba, K. Interrelationship between non-invasive measurements of atherosclerosis: Flow-mediated dilation of brachial artery, carotid intima-media thickness and pulse wave velocity. Atherosclerosis 2004, 173, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Charakida, M.; Masi, S.; Lüscher, T.F.; Kastelein, J.J.P.; Deanfield, J.E. Assessment of atherosclerosis: The role of flow-mediated dilatation. Eur. Heart J. 2010, 31, 2854–2861. [Google Scholar] [CrossRef] [PubMed]
- Woodman, R.J.; Playford, D.A.; Watts, G.F.; Cheetham, C.; Reed, C.; Taylor, R.R.; Puddey, I.B.; Beilin, L.J.; Burke, V.; Mori, T.A.; et al. Improved analysis of brachial artery ultrasound using a novel edge-detection software system. J. Appl. Physiol. 2001, 91, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Greyling, A.; van Mil, A.C.C.M.; Zock, P.L.; Green, D.J.; Ghiadoni, L.; Thijssen, D.H. Adherence to guidelines strongly improves reproducibility of brachial artery flow-mediated dilation. Atherosclerosis 2016, 248, 196–202. [Google Scholar] [CrossRef]
- Green, D.J.; Jones, H.; Thijssen, D.; Cable, N.T.; Atkinson, G. Flow-mediated dilation and cardiovascular event prediction: Does nitric oxide matter? Hypertension 2011, 57, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Kannenkeril, D.; Bosch, A.; Kolwelter, J.; Jung, S.; Striepe, K.; Ott, C.; Delles, C.; Schmieder, R.E. Dependency of flow-mediated vasodilatation from basal nitric oxide activity. Clin. Physiol. Funct. Imaging 2021, 41, 310–316. [Google Scholar] [CrossRef]
- Yang, Y.; Xu, J.; Wang, Y.; Tang, X.; Gao, P. Brachial flow-mediated dilation predicts subclinical target organ damage progression in essential hypertensive patients: A 3-year follow-up study. J. Hypertens. 2014, 32, 2393–2400. [Google Scholar] [CrossRef] [PubMed]
- Van Mil, A.C.C.M.; Greyling, A.; Zock, P.L.; Geleijnse, J.M.; Hopman, M.T.; Mensink, R.P.; Reesink, K.D.; Green, D.J.; Ghiadoni, L.; Thijssen, D.H. Impact of volunteer-related and methodology-related factors on the reproducibility of brachial artery flow-mediated vasodilation: Analysis of 672 individual repeated measurements. J. Hypertens. 2016, 34, 1738–1745. [Google Scholar] [CrossRef]
- Charakida, M.; de Groot, E.; Loukogeorgakis, S.P.; Khan, T.; Lüscher, T.; Kastelein, J.J.; Gasser, T.; Deanfield, J.E. Variability and reproducibility of flow-mediated dilatation in a multicentre clinical trial. Eur. Heart J. 2013, 34, 3501–3507. [Google Scholar] [CrossRef]
- Tomiyama, H.; Kohro, T.; Higashi, Y.; Takase, B.; Suzuki, T.; Ishizu, T.; Ueda, S.; Yamazaki, T.; Furumoto, T.; Kario, K.; et al. Reliability of measurement of endothelial function across multiple institutions and establishment of reference values in Japanese. Atherosclerosis 2015, 242, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Holder, S.M.; Bruno, R.M.; Shkredova, D.A.; Dawson, E.A.; Jones, H.; Hopkins, N.D.; Hopman, M.T.E.; Bailey, T.G.; Coombes, J.S.; Askew, C.D.; et al. Reference intervals for brachial artery flow-mediated dilation and the relation with cardiovascular risk factors. Hypertension 2021, 77, 1469–1480. [Google Scholar] [CrossRef] [PubMed]
- Li, A.M.; Celermajer, D.S.; Chan, M.H.; Sung, R.Y.; Woo, K.S. Reference range for brachial artery flow-mediated dilation in healthy Chinese children and adolescents. Hong Kong Med. J. 2018, 24, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Maruhashi, T.; Kajikawa, M.; Kishimoto, S.; Hashimoto, H.; Takaeko, Y.; Yamaji, T.; Harada, T.; Han, Y.; Aibara, Y.; Mohamad Yusoff, F.; et al. Diagnostic criteria of flow-mediated vasodilation for normal endothelial function and nitroglycerin-induced vasodilation for normal vascular smooth muscle function of the brachial artery. J. Am. Heart Assoc. 2020, 9, e013915. [Google Scholar] [CrossRef]
- Suzuki, T.; Hirata, K.; Elkind, M.S.V.; Jin, Z.; Rundek, T.; Miyake, Y.; Boden-Albala, B.; Di Tullio, M.R.; Sacco, R.; Homma, S. Metabolic syndrome, endothelial dysfunction, and risk of cardiovascular events: The Northern Manhattan Study (NOMAS). Am. Heart J. 2008, 156, 405–410. [Google Scholar] [CrossRef]
- Williams, I.L.; Chowienczyk, P.J.; Wheatcroft, S.B.; Patel, A.G.; Sherwood, R.A.; Momin, A.; Shah, A.M.; Kearney, M.T. Endothelial function and weight loss in obese humans. Obes. Surg. 2005, 15, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Gluszewska, A.; Gryglewska, B.; Rewiuk, K.; Zarzycki, B.; Dzieza-Grudnik, A.; Kwater, A.; Major, P.; Budzynski, A.; Gasowski, J.; Grodzicki, T. Arterial structure and function and its short- and long-term changes after bariatric surgery. J. Physiol. Pharmacol. 2019, 70, 909–916. [Google Scholar] [CrossRef]
- Domienik-Karłowicz, J.; Lisik, W.; Rymarczyk, Z.; Dzikowska-Diduch, O.; Chmura, A.; Demkow, U.; Pruszczyk, P. The short-term effect of bariatric surgery on non-invasive markers of artery function in patients with metabolic syndrome. Diabetol. Metab. Syndr. 2015, 7, 76. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Larson, M.G.; Keyes, M.J.; Mitchell, G.F.; Vasan, R.S.; Keaney, J.F.J.; Lehman, B.T.; Fan, S.; Osypiuk, E.; Vita, J.A. Clinical correlates and heritability of flow-mediated dilation in the community: The Framingham Heart Study. Circulation 2004, 109, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Lambert, G.; de Oliveira Lima, M.M.; Felici, A.C.; Pareja, J.C.; Vasques, A.C.J.; Novaes, F.S.; Rodovalho, S.; Hirsch, F.F.P.; Matos-Souza, J.R.; Chaim, É.A.; et al. Early regression of carotid intima-media thickness after bariatric surgery and its relation to serum leptin reduction. Obes. Surg. 2018, 28, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Stanek, A.; Brożyna-Tkaczyk, K.; Myśliński, W. The role of obesity-induced perivascular adipose tissue (PVAT) dysfunction in vascular homeostasis. Nutrients 2021, 13, 3843. [Google Scholar] [CrossRef] [PubMed]
- Ne, J.Y.A.; Cai, T.Y.; Celermajer, D.S.; Caterson, I.D.; Gill, T.; Lee, C.M.Y.; Skilton, M.R. Obesity, arterial function and arterial structure—A systematic review and meta-analysis. Obes. Sci. Pract. 2017, 3, 171–184. [Google Scholar] [CrossRef]
- Wycherley, T.P.; Thompson, C.H.; Buckley, J.D.; Luscombe-Marsh, N.D.; Noakes, M.; Wittert, G.A.; Brinkworth, G.D. Long-term effects of weight loss with a very-low carbohydrate, low saturated fat diet on flow mediated dilatation in patients with type 2 diabetes: A randomised controlled trial. Atherosclerosis 2016, 252, 28–31. [Google Scholar] [CrossRef]
- Magliano, D.J.; Shaw, J.E.; Zimmet, P.Z. How to best define the metabolic syndrome. Ann. Med. 2006, 38, 34–41. [Google Scholar] [CrossRef]
- Engin, A. The definition and prevalence of obesity and metabolic syndrome. Adv. Exp. Med. Biol. 2017, 960, 1–17. [Google Scholar] [CrossRef]
- Min, Y.-I.; Gao, Y.; Anugu, P.; Anugu, A.; Correa, A. Obesity and overall mortality: Findings from the Jackson Heart Study. BMC Public Health 2021, 21, 50. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Kasperczyk, S.; Osadnik, T.; Pawlas, N. Oxidative stress in association with metabolic health and obesity in young adults. Oxid. Med. Cell. Longev. 2021, 2021, 9987352. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Osadnik, T.; Goławski, M.; Lewandowski, P.; Pawlas, N. “Obesity and insulin resistance” is the component of the metabolic syndrome most strongly associated with oxidative stress. Antioxidants 2022, 11, 79. [Google Scholar] [CrossRef]
- Pennathur, S.; Heinecke, J.W. Oxidative stress and endothelial dysfunction in vascular disease. Curr. Diab. Rep. 2007, 7, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Victor, V.M.; Rocha, M.; Solá, E.; Bañuls, C.; Garcia-Malpartida, K.; Hernández-Mijares, A. Oxidative stress, endothelial dysfunction and atherosclerosis. Curr. Pharm. Des. 2009, 15, 2988–3002. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, G.K.; Cieślar, G.; Stanek, A. Nitrotyrosine, nitrated lipoproteins, and cardiovascular dysfunction in patients with type 2 diabetes: What do we know and what remains to be explained? Antioxidants 2022, 11, 856. [Google Scholar] [CrossRef]
- Ryliškytė, L.; Navickas, R.; Šerpytis, P.; Puronaitė, R.; Zupkauskienė, J.; Jucevičienė, A.; Badarienė, J.; Rimkienė, M.A.; Ryliškienė, K.; Skiauterytė, E.; et al. Association of aortic stiffness, carotid intima-media thickness and endothelial function with cardiovascular events in metabolic syndrome subjects. Blood Press 2019, 28, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Guven, B.; Demirpence, S.; Yilmazer, M.M.; Carti, O.U.; Tavli, V.; Mese, T.; Oner, T. Arterial function and anatomy in obese children with cardiovascular risk factors. Pediatr. Int. 2013, 55, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, C.J.; Agnew, C.E.; McCann, A.; Hamilton, P.K.; Quinn, C.E.; McCall, D.O.; Plumb, R.D.; McClenaghan, V.C.N.; McGivern, R.C.; Harbinson, M.T.; et al. Impaired flow-mediated dilatation response in uncomplicated type 1 diabetes mellitus: Influence of shear stress and microvascular reactivity. Clin. Sci. 2011, 121, 129–139. [Google Scholar] [CrossRef]
- Hamilton, P.; Lockhart, C.J.; McCann, A.J.; Agnew, C.E.; Harbinson, M.T.; McClenaghan, V.; Bleakley, C.; McGivern, R.C.; McVeigh, G. Flow-mediated dilatation of the brachial artery is a poorly reproducible indicator of microvascular function in type I diabetes mellitus. QJM 2011, 104, 589–597. [Google Scholar] [CrossRef]
- Shivalkar, B.; Dhondt, D.; Goovaerts, I.; Van Gaal, L.; Bartunek, J.; Van Crombrugge, P.; Vrints, C. Flow mediated dilatation and cardiac function in type 1 diabetes mellitus. Am. J. Cardiol. 2006, 97, 77–82. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, H.; Li, P. Cardiovascular risk factors in children with type 1 diabetes mellitus. J. Pediatr. Endocrinol. Metab. 2019, 32, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Ono, T.; Miyoshi, T.; Ohno, Y.; Osawa, K.; Takaya, Y.; Miki, T.; Ichikawa, K.; Ito, H. Brachial intima-media thickness is associated with coronary artery atherosclerosis in patients with diabetes mellitus. Heart Vessel. 2019, 34, 1405–1411. [Google Scholar] [CrossRef] [PubMed]
- Barchetta, I.; Ciccarelli, G.; Barone, E.; Cimini, F.A.; Ceccarelli, V.; Bertoccini, L.; Sentinelli, F.; Tramutola, A.; Del Ben, M.; Angelico, F.; et al. Greater circulating DPP4 activity is associated with impaired flow-mediated dilatation in adults with type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Ghardashi Afousi, A.; Izadi, M.R.; Rakhshan, K.; Mafi, F.; Biglari, S.; Gandomkar Bagheri, H. Improved brachial artery shear patterns and increased flow-mediated dilatation after low-volume high-intensity interval training in type 2 diabetes. Exp. Physiol. 2018, 103, 1264–1276. [Google Scholar] [CrossRef] [PubMed]
- Bai, Q.; Lai, X.; Zhang, A.-H.; Lu, X.-H.; Tian, S.-L.; Fan, M.-H.; Wang, Y.; Wang, T. Metabolic syndrome and its components associated with endothelial dysfunction in chronic kidney disease patients. Vasc. Health Risk Manag. 2012, 8, 15–21. [Google Scholar] [CrossRef]
- Kawano, N.; Emoto, M.; Mori, K.; Yamazaki, Y.; Urata, H.; Tsuchikura, S.; Motoyama, K.; Morioka, T.; Fukumoto, S.; Shoji, T.; et al. Association of endothelial and vascular smooth muscle dysfunction with cardiovascular risk factors, vascular complications, and subclinical carotid atherosclerosis in type 2 diabetic patients. J. Atheroscler. Thromb. 2012, 19, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Moriguchi, J.; Itoh, H.; Harada, S.; Takeda, K.; Hatta, T.; Nakata, T.; Sasaki, S. Low frequency regular exercise improves flow-mediated dilatation of subjects with mild hypertension. Hypertens. Res. 2005, 28, 315–321. [Google Scholar] [CrossRef]
- Nagai, K.; Shibata, S.; Akishita, M.; Sudoh, N.; Obara, T.; Toba, K.; Kozaki, K. Efficacy of combined use of three non-invasive atherosclerosis tests to predict vascular events in the elderly; carotid intima-media thickness, flow-mediated dilation of brachial artery and pulse wave velocity. Atherosclerosis 2013, 231, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Evrengul, H.; Tanriverdi, H.; Kilic, I.D.; Dursunoglu, D.; Ozcan, E.E.; Kaftan, A.; Kilic, M. Aortic stiffness and flow-mediated dilatation in normotensive offspring of parents with hypertension. Cardiol. Young 2012, 22, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Çetin, M.; Erdoğan, T.; Kırış, T.; Özyıldız, A.G.; Ergül, E.; Durakoğlugil, E.; Durak, H.; Kalaycıoğlu, E.; Çiçek, Y. Endothelial dysfunction, subclinical atherosclerosis and LDL cholesterol are the independent predictors of left atrial functions in hypertension. Int. J. Cardiovasc. Imaging 2020, 36, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Rinkūnienė, E.; Butkutė, E.; Puronaitė, R.; Petrulionienė, Ž.; Dženkevičiūtė, V.; Kasiulevičius, V.; Laucevičius, A. Arterial function parameters in patients with metabolic syndrome and severe hypertriglyceridemia. J. Clin. Lipidol. 2017, 11, 901–907. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Rueda-Clausen, C.F.; López-Jaramillo, P.; Luengas, C.; del Pilar Oubiña, M.; Cachofeiro, V.; Lahera, V. Inflammation but not endothelial dysfunction is associated with the severity of coronary artery disease in dyslipidemic subjects. Mediat. Inflamm. 2009, 2009, 469169. [Google Scholar] [CrossRef] [PubMed]
- Moran, C.; McEniery, C.M.; Schoenmakers, N.; Mitchell, C.; Sleigh, A.; Watson, L.; Lyons, G.; Burling, K.; Barker, P.; Chatterjee, K. Dyslipidemia, insulin resistance, ectopic lipid accumulation, and vascular function in resistance to thyroid hormone β. J. Clin. Endocrinol. Metab. 2021, 106, e2005–e2014. [Google Scholar] [CrossRef]
- Inaba, Y.; Chen, J.A.; Bergmann, S.R. Prediction of future cardiovascular outcomes by flow-mediated vasodilatation of brachial artery: A meta-analysis. Int. J. Cardiovasc. Imaging 2010, 26, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Giri, S.; Rathi, V.; Ranga, G.S. Flow mediated dilatation, carotid intima media thickness, ankle brachial pressure index and pulse pressure in young male post myocardial infarction patients in India. J. Clin. Diagn. Res. 2016, 10, OC35–OC39. [Google Scholar] [CrossRef] [PubMed]
- Mangiacapra, F.; Bressi, E.; Viscusi, M.M.; Creta, A.; Di Gioia, G.; Capuano, M.; Colaiori, I.; Di Sciascio, G.; Ussia, G.P.; Grigioni, F. Non-invasive functional and anatomic vascular evaluation for the prediction of coronary artery disease: The NINFA Study. Int. J. Cardiol. 2021, 322, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarczyk, P.; Maga, P.; Niżankowski, R.; Januszek, R.; Frołow, M.; Maga, M.; Kościelniak, J.; Belowski, A. The relationship between pulse waveform analysis indices, endothelial function and clinical outcomes in patients with peripheral artery disease treated using percutaneous transluminal angioplasty during a one-year follow-up period. Cardiol. J. 2020, 27, 142–151. [Google Scholar] [CrossRef]
- Schiffrin, E.L.; Lipman, M.L.; Mann, J.F.E. Chronic kidney disease: Effects on the cardiovascular system. Circulation 2007, 116, 85–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theodorakopoulou, M.P.; Dipla, K.; Zafeiridis, A.; Sarafidis, P. Εndothelial and microvascular function in CKD: Evaluation methods and associations with outcomes. Eur. J. Clin. Investig. 2021, 51, e13557. [Google Scholar] [CrossRef]
- Poulikakos, D.; Ross, L.; Recio-Mayoral, A.; Cole, D.; Andoh, J.; Chitalia, N.; Sharma, R.; Carlos Kaski, J.; Banerjee, D. Left ventricular hypertrophy and endothelial dysfunction in chronic kidney disease. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 56–61. [Google Scholar] [CrossRef]
- Dogra, G.; Irish, A.; Chan, D.; Watts, G. Insulin resistance, inflammation, and blood pressure determine vascular dysfunction in CKD. Am. J. Kidney Dis. 2006, 48, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Verbeke, F.H.; Pannier, B.; Guérin, A.P.; Boutouyrie, P.; Laurent, S.; London, G.M. Flow-mediated vasodilation in end-stage renal disease. Clin. J. Am. Soc. Nephrol. 2011, 6, 2009. [Google Scholar] [CrossRef] [PubMed]
- Hellman, T.; Lankinen, R.; Järvisalo, M.J.; Hakamäki, M.; Koivuviita, N.S.; Raitakari, O.T.; Metsärinne, K. Arterial endothelial function, carotid artery intima-media thickness and abdominal aortic calcification in diabetic and nondiabetic CKD stage 4-5 patients not on dialysis. Diabetes Res. Clin. Pract. 2021, 171, 108559. [Google Scholar] [CrossRef] [PubMed]
- Lankinen, R.; Hakamäki, M.; Metsärinne, K.; Koivuviita, N.S.; Pärkkä, J.P.; Hellman, T.; Kartiosuo, N.; Raitakari, O.T.; Järvisalo, M.J. Cardiovascular determinants of mortality in advanced chronic kidney disease. Am. J. Nephrol. 2020, 51, 726–735. [Google Scholar] [CrossRef]
- Miyagi, T.; Kohagura, K.; Ishiki, T.; Kochi, M.; Kinjyo, T.; Kinjyo, K.; Maehara, Y.; Sakima, A.; Iseki, K.; Ohya, Y. Interrelationship between brachial artery function and renal small artery sclerosis in chronic kidney disease. Hypertens. Res. 2014, 37, 863–869. [Google Scholar] [CrossRef]
- Sharma, J.; Kapoor, A.; Muthu, R.; Prasad, N.; Sinha, A.; Khanna, R.; Kumar, S.; Garg, N.; Tewari, S.; Sharma, R.K.; et al. Assessment of endothelial dysfunction in Asian Indian patients with chronic kidney disease and changes following renal transplantation. Clin. Transplant. 2014, 28, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Bartoli, F.; Blagojevic, J.; Bacci, M.; Fiori, G.; Tempestini, A.; Conforti, M.L.; Guiducci, S.; Miniati, I.; Di Chicco, M.; Del Rosso, A.; et al. Flow-mediated vasodilation and carotid intima-media thickness in systemic sclerosis. Ann. N. Y. Acad. Sci. 2007, 1108, 283–290. [Google Scholar] [CrossRef]
- Sedky Abdou, M.M.; El Desouky, S.M.; Helmy El Kaffas, K.M.; Ahmed Hassan, A.M. Premature atherosclerosis in systemic sclerosis patients: Its relation to disease parameters and to traditional risk factors. Int. J. Rheum. Dis. 2017, 20, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Pacholczak-Madej, R.; Kuszmiersz, P.; Bazan-Socha, S.; Kosałka-Wêgiel, J.; Iwaniec, T.; Zarêba, L.; Kielczewski, S.; Rams, A.; Walocha, J.A.; Musiał, J.; et al. Endothelial dysfunction in patients with systemic sclerosis. Postepy Dermatol. Alergol. 2020, 37, 495–502. [Google Scholar] [CrossRef]
- Majer, M.; Gackowski, D.; Różalski, R.; Siomek-Górecka, A.; Oliński, R.; Budzyński, J. Systemic oxidoreductive balance and vascular function in individuals without clinical manifestation of atherosclerosis. Arch. Med. Sci. Atheroscler. Dis. 2017, 2, e37–e45. [Google Scholar] [CrossRef] [PubMed]
- Joris, P.J.; Mensink, R.P. Effects of supplementation with the fat-soluble vitamins E and D on fasting flow-mediated vasodilation in adults: A meta-analysis of randomized controlled trials. Nutrients 2015, 7, 1728–1743. [Google Scholar] [CrossRef] [PubMed]
- Qasemi, R.; Ghavamzadeh, S.; Faghfouri, A.H.; Valizadeh, N.; Mohammadi, A.; Sayyadi, H. The effect of vitamin D supplementation on flow-mediated dilatation, oxidized LDL and intracellular adhesion molecule 1 on type 2 diabetic patients with hypertension: A randomized, placebo-controlled, double-blind trial. Diabetes Metab. Syndr. 2021, 15, 102200. [Google Scholar] [CrossRef]
- Brandenburg, V.M.; Vervloet, M.G.; Marx, N. The Role of Vitamin D in cardiovascular disease: From present evidence to future perspectives. Atherosclerosis 2012, 225, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Dalan, R.; Liew, H.; Tan, W.K.A.; Chew, D.E.K.; Leow, M.K.-S. Vitamin D and the endothelium: Basic, translational and clinical research updates. IJC Metab. Endocr. 2014, 4, 4–17. [Google Scholar] [CrossRef]
- Casey, D.P.; Schneider, A.C.; Ueda, K. Influence of chronic endurance exercise training on conduit artery retrograde and oscillatory shear in older adults. Eur. J. Appl. Physiol. 2016, 116, 1931–1940. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef]
- Santos, L.P.; Umpierre, D. Exercise, cardiovascular health, and risk factors for atherosclerosis: A narrative review on these complex relationships and caveats of literature. Front. Physiol. 2020, 11, 840. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, K.; Zmijewski, P.; Czajkowska, A.; Lutosławska, G. Gender differences in carotid artery intima-media thickness and flow-mediated dilatation in young, physically active adults. J. Sports Med. Phys. Fit. 2014, 54, 298–306. [Google Scholar]
- Januszek, R.; Mika, P.; Konik, A.; Petriczek, T.; Nowobilski, R.; Niżankowski, R. Effect of treadmill training on endothelial function and walking abilities in patients with peripheral arterial disease. J. Cardiol. 2014, 64, 145–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Januszek, R.; Mika, P.; Nowobilski, R.; Maga, P.; Niżankowski, R. The improvement of walking abilities and endothelial function after the supervised training treadmill program (STTP) in patients with peripheral artery disease (PAD) is not related to prostacyclin and thromboxane release. Int. J. Cardiol. 2016, 222, 813–818. [Google Scholar] [CrossRef]
- Quinton, A.E.; Peek, M.J.; Cook, C.-M.; Kirby, A. Flow-mediated dilatation assessment in women with preeclampsia compared to women with gestational hypertension. Hypertens. Pregnancy 2012, 31, 377–386. [Google Scholar] [CrossRef]
- Weissgerber, T.L.; Milic, N.M.; Milin-Lazovic, J.S.; Garovic, V.D. Impaired flow-mediated dilation before, during, and after preeclampsia: A systematic review and meta-analysis. Hypertension 2016, 67, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.S.; Goel, P.; Chaudhary, A.; Kochhar, S.; Kaur, G.; Bhagat, A. Serial profile of flow-mediated dilatation in primigravida for prediction of preeclampsia and gestational hypertension. Hypertens. Pregnancy 2018, 37, 212–219. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Bjedov, S.; Jaksic, N.; Jakovljevic, I. COVID-19 pandemia and public and global mental health from the perspective of global health securit. Psychiatr. Danub. 2020, 32, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Lima-Martínez, M.M.; Carrera Boada, C.; Madera-Silva, M.D.; Marín, W.; Contreras, M. COVID-19 and diabetes: A bidirectional relationship. Clin. Investig. Arterioscler. 2021, 33, 151–157. [Google Scholar] [CrossRef]
- Lambadiari, V.; Mitrakou, A.; Kountouri, A.; Thymis, J.; Katogiannis, K.; Korakas, E.; Varlamos, C.; Andreadou, I.; Tsoumani, M.; Triantafyllidi, H.; et al. Association of COVID-19 with impaired endothelial glycocalyx, vascular function and myocardial deformation 4 months after infection. Eur. J. Heart Fail. 2021, 23, 1916–1926. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Ochab-Jakubiak, J.; Cieślar, G.; Stanek, A. Gastrointestinal symptoms in the course of COVID-19. Postepy Hig. Med. Dosw. 2020, 74, 498–503. [Google Scholar] [CrossRef]
- Ergül, E.; Yılmaz, A.S.; Öğütveren, M.M.; Emlek, N.; Kostakoğlu, U.; Çetin, M. COVID 19 disease independently predicted endothelial dysfunction measured by flow-mediated dilatation. Int. J. Cardiovasc. Imaging 2022, 38, 25–32. [Google Scholar] [CrossRef]
- Riou, M.; Oulehri, W.; Momas, C.; Rouyer, O.; Lebourg, F.; Meyer, A.; Enache, I.; Pistea, C.; Charloux, A.; Marcot, C.; et al. Reduced flow-mediated dilatation is not related to COVID-19 severity three months after hospitalization for SARS-CoV-2 infection. J. Clin. Med. 2021, 10, 1318. [Google Scholar] [CrossRef] [PubMed]
- Stoner, L.; Tarrant, M.A.; Fryer, S.; Faulkner, J. How should flow-mediated dilation be normalized to its stimulus? Clin. Physiol. Funct. Imaging 2013, 33, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Credeur, D.; Fryer, S.; Stoner, L. The use of shear rate-diameter dose-response curves as an alternative to the flow-mediated dilation test. Med. Hypotheses 2015, 84, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, J.C.; Pyke, K.E. Flow-mediated dilation stimulated by sustained increases in shear stress: A useful tool for assessing endothelial function in humans? Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H508–H520. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Over the course of obesity, significantly lower FMD values are observed and, after successful bariatric treatment, a significant increase in FMD values was observed [49,50,51,52,53]. |
| FMD is significantly associated with cardiovascular risk in patients with metabolic syndrome (MS) [66]. |
| FMD is significantly reduced compared to controls in patients with type 1 diabetes [68,69,70,71] and in patients with type 2 diabetes [73,74,76]. |
| The FMD test confirms endothelial dysfunction in patients with hypertension [78,79] which is associated with cardiovascular dysfunction assessed by other methods, such as intima-media thickness and pulse wave velocity [79]. |
| The influence of dyslipidemia on the value of FMD is not fully clear [84,85]. |
| FMD is a valuable method for assessing patients with already diagnosed cardiovascular disease [87,88] or chronic renal failure [94,95,96,97,98]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mućka, S.; Miodońska, M.; Jakubiak, G.K.; Starzak, M.; Cieślar, G.; Stanek, A. Endothelial Function Assessment by Flow-Mediated Dilation Method: A Valuable Tool in the Evaluation of the Cardiovascular System. Int. J. Environ. Res. Public Health 2022, 19, 11242. https://doi.org/10.3390/ijerph191811242
Mućka S, Miodońska M, Jakubiak GK, Starzak M, Cieślar G, Stanek A. Endothelial Function Assessment by Flow-Mediated Dilation Method: A Valuable Tool in the Evaluation of the Cardiovascular System. International Journal of Environmental Research and Public Health. 2022; 19(18):11242. https://doi.org/10.3390/ijerph191811242
Chicago/Turabian StyleMućka, Szymon, Martyna Miodońska, Grzegorz K. Jakubiak, Monika Starzak, Grzegorz Cieślar, and Agata Stanek. 2022. "Endothelial Function Assessment by Flow-Mediated Dilation Method: A Valuable Tool in the Evaluation of the Cardiovascular System" International Journal of Environmental Research and Public Health 19, no. 18: 11242. https://doi.org/10.3390/ijerph191811242
APA StyleMućka, S., Miodońska, M., Jakubiak, G. K., Starzak, M., Cieślar, G., & Stanek, A. (2022). Endothelial Function Assessment by Flow-Mediated Dilation Method: A Valuable Tool in the Evaluation of the Cardiovascular System. International Journal of Environmental Research and Public Health, 19(18), 11242. https://doi.org/10.3390/ijerph191811242