
Digital Help for Substance Users (SU): A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Overview
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Extraction Steps
2.4. Data Extraction
2.5. Synthesis
3. Results
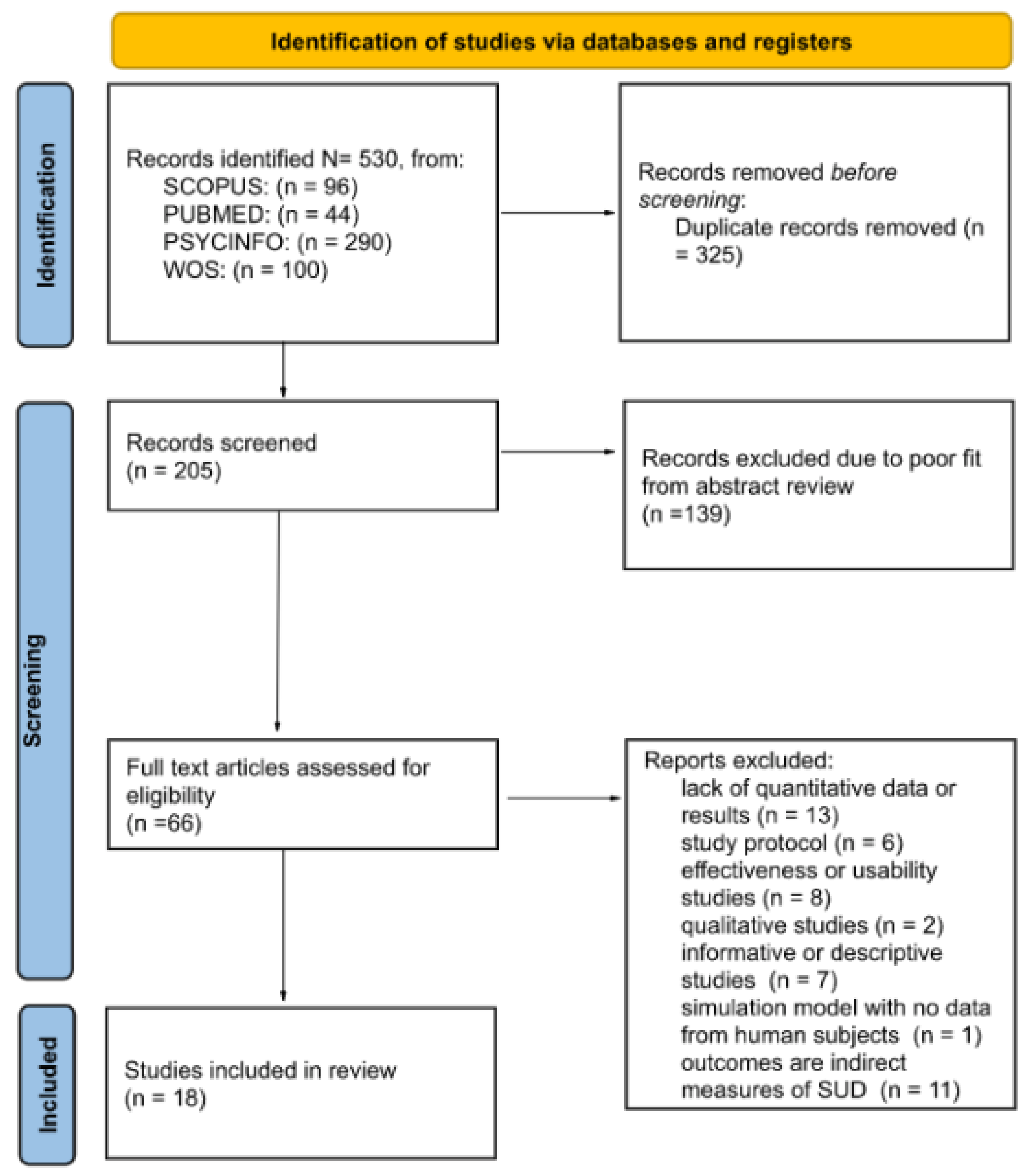
3.1. Study Selections and Extractions
3.2. Study Characteristics
4. Discussion
4.1. Outcomes and Measurements
4.2. Models and Approaches
4.3. Methodology and Intervention Design
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Satre, D.D.; Meacham, M.C.; Asarnow, L.D.; Fisher, W.S.; Fortuna, L.R.; Iturralde, E. Opportunities to Integrate Mobile App-Based Interventions into Mental Health and Substance Use Disorder Treatment Services in the Wake of COVID-19. Am. J. Health Promot. 2021, 35, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Boumparis, N.; Schulte, M.H.J.; Riper, H. Digital Mental Health for Alcohol and Substance Use Disorders. Curr. Treat. Options Psychiatry 2019, 6, 352–366. [Google Scholar] [CrossRef]
- Boumparis, N.; Loheide-Niesmann, L.; Blankers, M.; Ebert, D.D.; Korf, D.; Schaub, M.P.; Spijkerman, R.; Tait, R.J.; Riper, H. Short- and Long-Term Effects of Digital Prevention and Treatment Interventions for Cannabis Use Reduction: A Systematic Review and Meta-Analysis. Drug Alcohol Depend. 2019, 200, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Marsch, L.A. Digital Health and Addiction. Curr. Opin. Syst. Biol. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Steinkamp, J.M.; Goldblatt, N.; Borodovsky, J.T.; LaVertu, A.; Kronish, I.M.; Marsch, L.A.; Schuman-Olivier, Z. Technological Interventions for Medication Adherence in Adult Mental Health and Substance Use Disorders: A Systematic Review. JMIR Ment. Health 2019, 6, e12493. [Google Scholar] [CrossRef]
- Bonfiglio, N.S.; Mascia, M.L.; Penna, M.P. Digital Treatment Paths for Substance Use Disorders (SUDs). Int. J. Environ. Res. Public Health 2022, 19, 7322. [Google Scholar] [CrossRef]
- Musyoka, C.M.; Mbwayo, A.; Donovan, D.M.; Mathai, M. mHealth-Based Peer Mentoring for Prevention of Alcohol and Substance Abuse among First Year University Students: Protocol for Quasi-Experimental Intervention. J. Subst. Use 2021, 26, 53–59. [Google Scholar] [CrossRef]
- Dick, S.; O’Connor, Y.; Thompson, M.J.; O’Donoghue, J.; Hardy, V.; Joseph Wu, T.S.; O’Sullivan, T.; Chirambo, G.B.; Heavin, C. Considerations for Improved Mobile Health Evaluation: Retrospective Qualitative Investigation. JMIR mHealth uHealth 2020, 8, e12424. [Google Scholar] [CrossRef] [PubMed]
- Berrouiguet, S.; Baca-García, E.; Brandt, S.; Walter, M.; Courtet, P. Fundamentals for Future Mobile-Health (mHealth): A Systematic Review of Mobile Phone and Web-Based Text Messaging in Mental Health. J. Med. Internet Res. 2016, 18, e5066. [Google Scholar] [CrossRef]
- Anastasiadou, D.; Folkvord, F.; Lupiañez-Villanueva, F. A Systematic Review of MHealth Interventions for the Support of Eating Disorders. Eur. Eat. Disord. Rev. 2018, 26, 394–416. [Google Scholar] [CrossRef]
- Hutton, A.; Prichard, I.; Whitehead, D.; Thomas, S.; Rubin, M.; Sloand, E.; Powell, T.W.; Frisch, K.; Newman, P.; Goodwin Veenema, T. MHealth Interventions to Reduce Alcohol Use in Young People: A Systematic Review of the Literature. Compr. Child Adolesc. Nurs. 2020, 43, 171–202. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, D.M.; Troutman-Jordan, M.; Whitfield, J.E.; Pappa, E.V. Effectiveness of EHealth Technology-Based Interventions in Reducing Substance Misuse among Older Adults: A Systematic Review. J. Gerontol. Nurs. 2021, 47, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, D.M.; Borsari, B.; Levine, M.J.; Li, S.; Lamberson, K.A.; Matta, L.A. A Systematic Review of the MHealth Interventions to Prevent Alcohol and Substance Abuse. J. Health Commun. 2017, 22, 413–432. [Google Scholar] [CrossRef] [PubMed]
- Rathbone, A.L.; Prescott, J. The Use of Mobile Apps and SMS Messaging as Physical and Mental Health Interventions: Systematic Review. J. Med. Internet Res. 2017, 19, e7740. [Google Scholar] [CrossRef]
- Batra, S.; Baker, R.A.; Wang, T.; Forma, F.; Dibiasi, F.; Peters-Strickland, T. Digital Health Technology for Use in Patients with Serious Mental Illness: A Systematic Review of the Literature. Med. Devices 2017, 10, 237. [Google Scholar] [CrossRef]
- López-Pelayo, H.; Aubin, H.-J.; Drummond, C. “The Post-COVID Era”: Challenges in the Treatment of Substance Use Disorder (SUD) after the Pandemic. BMC Med. 2020, 18, 241. [Google Scholar] [CrossRef]
- Bergman, B.G.; Kelly, J.F. Online Digital Recovery Support Services: An Overview of the Science and Their Potential to Help Individuals with Substance Use Disorder during COVID-19 and Beyond. J. Subst. Abuse Treat. 2021, 120, 108152. [Google Scholar] [CrossRef]
- Balcombe, L.; de Leo, D.; Bustin, S. Digital Mental Health Amid COVID-19. Encyclopedia 2021, 1, 1047–1057. [Google Scholar] [CrossRef]
- Srivastava, V.K. Anatomy of Stigma: Understanding COVID-19. Soc. Chang. 2020, 50, 385–398. [Google Scholar] [CrossRef]
- Marsch, L.A.; Campbell, A.; Campbell, C.; Chen, C.H.; Ertin, E.; Ghitza, U.; Lambert-Harris, C.; Hassanpour, S.; Holtyn, A.F.; Hser, Y.I.; et al. The Application of Digital Health to the Assessment and Treatment of Substance Use Disorders: The Past, Current, and Future Role of the National Drug Abuse Treatment Clinical Trials Network. J. Subst. Abuse Treat. 2020, 112, 4–11. [Google Scholar] [CrossRef]
- Copeland, J.; Martin, G. Web-Based Interventions for Substance Use Disorders: A Qualitative Review. J. Subst. Abuse Treat. 2004, 26, 109–116. [Google Scholar] [CrossRef]
- Nesvåg, S.; Mckay, J.R. Feasibility and Effects of Digital Interventions to Support People in Recovery From Substance Use Disorders: Systematic Review. J. Med. Internet Res. 2018, 20, e9873. [Google Scholar] [CrossRef] [PubMed]
- Eilert, N.; Wogan, R.; Leen, A.; Richards, D. Internet-Delivered Interventions for Depression and Anxiety Symptoms in Children and Young People: Systematic Review and Meta-Analysis. JMIR Pediatrics Parent. 2022, 5, e33551. [Google Scholar] [CrossRef] [PubMed]
- Dugdale, S.; Davies, E.-D. Glyn Are Computer-Based Treatment Programs Effective at Reducing Symptoms of Substance Misuse and Mental Health Difficulties Within Adults? A Systematic Review. J. Dual Diagn. 2019, 15, 291–311. [Google Scholar] [CrossRef] [PubMed]
- Tofighi, B.; Abrantes, A.; Stein, M.D. The Role of Technology-Based Interventions for Substance Use Disorders in Primary Care: A Review of the Literature. Med. Clin. 2018, 102, 715–731. [Google Scholar] [CrossRef]
- Wang, K.; Varma, D.S.; Prosperi, M. A Systematic Review of the Effectiveness of Mobile Apps for Monitoring and Management of Mental Health Symptoms or Disorders. J. Psychiatr. Res. 2018, 107, 73–78. [Google Scholar] [CrossRef]
- O’brien, C. Addiction and Dependence in DSM-V. Addiction 2010, 106, 866–867. [Google Scholar] [CrossRef]
- Page, M.J.; Mckenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Cohen, J.F.; Deeks, J.J.; Hooft, L.; Salameh, J.P.; Korevaar, D.A.; Gatsonis, C.; Hopewell, S.; Hunt, H.A.; Hyde, C.J.; Leeflang, M.M.; et al. Preferred Reporting Items for Journal and Conference Abstracts of Systematic Reviews and Meta-Analyses of Diagnostic Test Accuracy Studies (PRISMA-DTA for Abstracts): Checklist, Explanation, and Elaboration. BMJ 2021, 372, n265. [Google Scholar] [CrossRef]
- dos Santos, W.M.; Secoli, S.R.; de Araújo Püschel, V.A. The Joanna Briggs Institute Approach for Systematic Reviews. Rev. Lat. Am. Enferm. 2018, 26, e3074. [Google Scholar] [CrossRef] [Green Version]
- Chander, G.; Hutton, H.E.; Xu, X.; Canan, C.E.; Gaver, J.; Finkelstein, J.; Lesko, C.R.; McCaul, M.E.; Lau, B. Computer Delivered Intervention for Alcohol and Sexual Risk Reduction among Women Attending an Urban Sexually Transmitted Infection Clinic: A Randomized Controlled Trial. Addict. Behav. Rep. 2021, 14, 100367. [Google Scholar] [CrossRef] [PubMed]
- Cucciare, M.A.; Combs, A.S.; Joshi, G.; Han, X.; Humphreys, K. Computer-Delivered Brief Alcohol Intervention for Patients with Liver Disease: A Randomized Controlled Trial. Addiction 2021, 116, 1076–1087. [Google Scholar] [CrossRef] [PubMed]
- Curtis, B.; Bergman, B.; Brown, A.; McDaniel, J.; Harper, K.; Eisenhart, E.; Hufnagel, M.; Heller, A.T.; Ashford, R. Characterizing Participation and Perceived Engagement Benefits in an Integrated Digital Behavioral Health Recovery Community for Women: A Cross-Sectional Survey. JMIR Ment. Health 2019, 6, e13352. [Google Scholar] [CrossRef] [PubMed]
- Danaher, B.G.; Tyler, M.S.; Crowley, R.C.; Brendryen, H.; Seeley, J.R. Outcomes and Device Usage for Fully Automated Internet Interventions Designed for a Smartphone or Personal Computer: The Mobilequit Smoking Cessation Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, e13290. [Google Scholar] [CrossRef]
- De Ruijter, D.; Hoving, C.; Evers, S.; Hudales, R.; de Vries, H.; Smit, E. An Economic Evaluation of a Computer-Tailored e-Learning Program to Promote Smoking Cessation Counseling Guideline Adherence among Practice Nurses. Patient Educ. Couns. 2019, 102, 1802–1811. [Google Scholar] [CrossRef]
- Drislane, L.E.; Waller, R.; Martz, M.E.; Bonar, E.E.; Walton, M.A.; Chermack, S.T.; Blow, F.C. Therapist and Computer-Based Brief Interventions for Drug Use within a Randomized Controlled Trial: Effects on Parallel Trajectories of Alcohol Use, Cannabis Use and Anxiety Symptoms. Addiction 2020, 115, 158–169. [Google Scholar] [CrossRef]
- Elison-Davies, S.; Märtens, K.; Yau, C.; Davies, G.; Ward, J. Associations between Baseline Opioid Use Disorder Severity, Mental Health and Biopsychosocial Functioning, with Clinical Responses to Computer-Assisted Therapy Treatment. Am. J. Drug Alcohol Abus. 2021, 47, 360–372. [Google Scholar] [CrossRef]
- Elison-Davies, S.; Hayhurst, K.; Jones, A.; Welch, Z.; Davies, G.; Ward, J. Associations between Participant Characteristics, Digital Intervention Engagement and Recovery Outcomes for Participants Accessing ‘Breaking Free Online’ at ‘Change Grow Live’. J. Subst. Use 2021, 26, 497–504. [Google Scholar] [CrossRef]
- Elison-Davies, S.; Wardell, J.D.; Quilty, L.C.; Ward, J.; Davies, G. Examining Correlates of Cannabis Users’ Engagement with a Digital Intervention for Substance Use Disorder: An Observational Study of Clients in UK Services Delivering Breaking Free Online. J. Subst. Abuse Treat. 2021, 123, 108261. [Google Scholar] [CrossRef]
- Elison, S.; Jones, A.; Ward, J.; Davies, G.; Dugdale, S. Examining Effectiveness of Tailorable Computer-Assisted Therapy Programmes for Substance Misuse: Programme Usage and Clinical Outcomes Data from Breaking Free Online. Addict. Behav. 2017, 74, 140–147. [Google Scholar] [CrossRef]
- Han, H.; Zhang, J.Y.; Hser, Y.I.; Liang, D.; Li, X.; Wang, S.S.; Du, J.; Zhao, M. Feasibility of a Mobile Phone App to Support Recovery from Addiction in China: Secondary Analysis of a Pilot Study. JMIR mHealth uHealth 2018, 6, e46. [Google Scholar] [CrossRef] [PubMed]
- Kay-Lambkin, F.J.; Simpson, A.L.; Bowman, J.; Childs, S. Dissemination of a Computer-Based Psychological Treatment in a Drug and Alcohol Clinical Service: An Observational Study. Addict. Sci. Clin. Pract. 2014, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Leightley, D.; Puddephatt, J.A.; Jones, N.; Mahmoodi, T.; Chui, Z.; Field, M.; Drummond, C.; Rona, R.J.; Fear, N.T.; Goodwin, L. A Smartphone App and Personalized Text Messaging Framework (InDex) to Monitor and Reduce Alcohol Use in Ex-Serving Personnel: Development and Feasibility Study. JMIR mHealth uHealth 2018, 6, e10074. [Google Scholar] [CrossRef] [PubMed]
- Wernette, G.T.; Plegue, M.; Kahler, C.W.; Sen, A.; Zlotnick, C. A Pilot Randomized Controlled Trial of a Computer-Delivered Brief Intervention for Substance Use and Risky Sex during Pregnancy. J. Women’s Health 2018, 27, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Wodarski, J.S.; MacMaster, S.; Miller, N.K. The Use of Computer Technology to Reduce and Prevent College Drinking. Soc. Work Public Health 2012, 27, 270–282. [Google Scholar] [CrossRef]
- Wu, Q.; Parrott, S.; Godfrey, C.; Gilbert, H.; Nazareth, I.; Leurent, B.; Sutton, S.; Morris, R. Cost-Effectiveness of Computer-Tailored Smoking Cessation Advice in Primary Care: A Randomized Trial (ESCAPE). Nicotine Tob. Res. 2014, 16, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.W.B.; Heng, S.; Song, G.; Fung, D.S.S.; Smith, H.E. Development of a Co-Designed Gamified Attention Bias Modification App for Individuals with Opioid Use Disorder. Technol. Health Care 2021, 29, 521–526. [Google Scholar] [CrossRef]
- Zhu, Y.; Jiang, H.; Su, H.; Zhong, N.; Li, R.; Li, X.; Chen, T.; Tan, H.; Du, J.; Xu, D.; et al. A Newly Designed Mobile-Based Computerized Cognitive Addiction Therapy App for the Improvement of Cognition Impairments and Risk Decision Making in Methamphetamine Use Disorder: Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e10292. [Google Scholar] [CrossRef]
- Carroll, K.M. Methodological Issues and Problems in the Assessment of Substance Use. Psychol. Assess. 1995, 7, 349–358. [Google Scholar] [CrossRef]
- Shorter, G.W.; Heather, N.; Bray, J.W.; Giles, E.L.; Holloway, A.; Barbosa, C.; Berman, A.H.; O’Donnell, A.J.; Clarke, M.; Stockdale, K.J.; et al. The “Outcome Reporting in Brief Intervention Trials: Alcohol” (ORBITAL) Framework: Protocol to Determine a Core Outcome Set for Efficacy and Effectiveness Trials of Alcohol Screening and Brief Intervention. Trials 2017, 18, 611. [Google Scholar] [CrossRef] [Green Version]
- Bonfiglio, N.S.; Renati, R.; Agus, M.; Penna, M.P. Validation of a Substance Craving Questionnaire (SCQ) in Italian Population. Addict. Behav. Rep. 2019, 9, 100172. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Liu, J. Education in and After Covid-19: Immediate Responses and Long-Term Visions. Postdigital Sci. Educ. 2020, 2, 695–699. [Google Scholar] [CrossRef]
- Prendergast, M.; Podus, D.; Finney, J.; Greenwell, L.; Roll, J. Contingency Management for Treatment of Substance Use Disorders: A Meta-Analysis. Addiction 2006, 101, 1546–1560. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, M.L.; Podus, D.; Chang, E.; Urada, D. The Effectiveness of Drug Abuse Treatment: A Meta-Analysis of Comparison Group Studies. Drug Alcohol Depend. 2002, 67, 53–72. [Google Scholar] [CrossRef]
- van Gemert-Pijnen, J.E.; Nijland, N.; Van Limburg, M.; Ossebaard, H.C.; Saskia, M.; Kelders, M.; Eysenbach, G.; Seydel, E.R. A Holistic Framework to Improve the Uptake and Impact of EHealth Technologies. J. Med. Internet Res. 2011, 13, e111. [Google Scholar] [CrossRef]
- Mazzoleni, M.; Previdi, F.; Bonfiglio, N.S. Classification Algorithms Analysis for Brain–Computer Interface in Drug Craving Therapy. Biomed. Signal. Process Control. 2019, 52, 463–472. [Google Scholar] [CrossRef]
- Gulliksen, J.; Göransson, B.; Boivie, I.; Blomkvist, S.; Persson, J.; Cajander, Å. Key Principles for User-Centred Systems Design. Behav. Inf. Technol. 2010, 22, 397–409. [Google Scholar] [CrossRef]
- Tait, R.J.; Kirkman, J.J.L.; Schaub, M.P. A Participatory Health Promotion Mobile App Addressing Alcohol Use Problems (The Daybreak Program): Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2018, 7, e148. [Google Scholar] [CrossRef]
- Tait, R.J.; McKetin, R.; Kay-Lambkin, F.; Carron-Arthur, B.; Bennett, A.; Bennett, K.; Christensen, H.; Griffiths, K.M. A Web-Based Intervention for Users of Amphetamine-Type Stimulants: 3-Month Outcomes of a Randomized Controlled Trial. JMIR Ment. Health 2014, 1, e1. [Google Scholar] [CrossRef]
- Renati, R.; Salvatore Bonfiglio, N.; Patrone, L.; Rollo, D.; Pietronilla Penna, M. The Use of Cognitive Training and TDCS for the Treatment of an High Potential Subject: A Case Study. In Proceedings of the 2021 IEEE International Symposium on Medical Measurements and Applications (MeMeA 2021–Conference Proceedings 2021), Lausanne, Switzerland, 23–25 June 2021. [Google Scholar] [CrossRef]
- Bonfiglio, N.S.; Rollo, D.; Renati, R.; Penna, M.P.; Di Lucia, K. The Use of Cognitive Training, Combined with TDCS, for Craving Reduction and Inhibitory Control Improvement in Cocaine Dependence: A Case Study. In Proceedings of the 2021 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Lausanne, Switzerland, 23–25 June 2021. [Google Scholar] [CrossRef]
- Bonfiglio, N.S.; Parodi, D.; Rollo, D.; Renati, R.; Pessa, E.; Penna, M.P. Use of Training with BCI (Brain Computer Interface) in the Management of Impulsivity. In Proceedings of the IEEE Medical Measurements and Applications (MeMeA 2020—Conference Proceedings 2020), Bari, Italy, 1 June–1 July 2020. [Google Scholar] [CrossRef]


{kind=link}
| Study | Participants (n), Mean Age (SD), Characteristics, Type of Dependence/Abuse | Tool/s | Outcome(s) and Measure(s) | Treatment(s) with Digital Technology | Results |
|---|---|---|---|---|---|
| Chander et al., 2021 [31] | n = 439, women; median age = 31 years; women were randomized as follows: 146 were assigned to the CBI + IVR/Text group, 145 to the CBI only group, and 148 to the control group; type of dependence: alcohol. | PC |
| Computer-delivered brief alcohol intervention (CBI). This interactive 20-min intervention was delivered in a motivational interviewing style by a three-dimensional avatar, using the Motivational Enhancement System (MES) Platform. CBI was delivered using interactive voice response technology (IVR) and text messages. | Assessments at baseline and 3, 6, and 12 months. Participants in all three study conditions significantly reduced their heavy drinking days, drinking days, drinks per drinking day, and drinks per week over the follow-up period (p ≤ 0.001), with no statistically significant differences between study conditions. CBI with or without IVR+text messages did not results in greater reduction in alcohol use compared to the control group. |
| Cucciare et al., 2021 [32] | n = 138, veterans; mean age = 63.18 years; men were randomized as follows: 71 in standard intervention and 67 in CBI intervention; type of dependence: alcohol. | PC |
| Computer-delivered brief alcohol intervention (CBI), as described previously. | Subjects were tested at baseline and 3- and 6-month follow-up. Participants in the CBI condition reported significantly fewer drinking days and unhealthy drinking days than participants enrolled into the standard care condition (p ≤ 0.05). Participants in the CBI condition reported significantly fewer unhealthy drinking days at 3-month follow-up compared to participants in the standard care condition (p ≤ 0.05). |
| Curtis et al., 2019 [33] | n = 729 women; mean age = 46.83 years; type of dependence: alcohol, opioids, heroin, benzodiazepines, cocaine, amphetamine, marijuana. | Digital recovery support service accessing on-line |
| SHE RECOVERS (SR) as a Digital Recovery Support Services (DRSS). It is a digital community that includes a public Facebook page, two private Facebook groups, digital training events, digital recovery coaching, a website, and an email listserv. | Subjects were tested at 1, 1 to 5, and 5+ years. Participants of SR community and other DRSSs with less than 1 and 1 to 5 years in recovery reported pathways of abstinence-based 12-step mutual aid at higher rates (p ≤ 0.001). |
| Danaher et al., 2019 [34] | n = 1271 participants; mean age = 44.9 years; participants were randomized as follows: 633 on MobileQuit and 638 on QuitOnline; type of dependence: nicotine. | Mobile app (for smartphone) and nonmobile PC |
| The MobileQuit intervention optimized for smartphones. QuitOnline intervention designed primarily for use on mobile PCs. These two interventions present very similar best practice smoking cessation content based on cognitive behavior therapy (CBT) features. | Participants were screened at baseline and 3 and 6 months. At 3 (p ≤ 0.001) and 6 (p = 0.02) months, participants in the MobileQuit condition displayed greater smoking abstinence than those in QuitOnline and used repeated point prevalence at 3 and 6 months (p ≤ 0.001). MobileQuit participants displayed greater smoking abstinence at 3 months (p ≤ 0.001) and at both 3 and 6 months (p ≤ 0.001), but not at 6 months. |
| de Ruijter et al., 2019 [35] | n = 269 practice nurses; mean age = 47.3 years; participants were randomized, 147 in the intervention group and 122 in the control group; type of dependence: nicotine. | PC |
| Computer-tailored e-learning program. It consisted of five e-learning modules with tailored advice, a forum, and smoking cessation counseling materials; three general modules containing project information, frequently asked questions about the trial, and a counseling checklist to self-report application of guideline steps. | Tests were administered at baseline and at 6 and at 12 months. A significant difference was found at 6 months on the FTND (p = 0.01), reporting a lower score as a means of reducing dependence for the intervention group, compared to the control group. |
| Drislane et al., 2020 [36] | n = 780 patients aged 18 to 60; participants were randomized as follows: 266 in the Therapist-Delivered Brief Intervention (TBI), 257 in the Computer-Guided Brief Intervention (CBI), and 257 in the enhanced usual care (EUC) as control group; type of dependence: alcohol and cannabis. | PC |
| Therapist-delivered brief-intervention (TBI). Computer-guided brief-intervention (CBI). Intervention with TBI and CBIs involved touchscreen-delivered and audio-assisted content. The TBI was administered by a Master’s-level therapist, whereas the CBI was self-administered using a virtual health counselor. | Assessment was administered at baseline and 3, 6, and 12 months. There was a significant reduction in cannabis use over time in the TBI group (p ≤ 0.05), but not in the EUC group. Only participants aged 18 to 25 years who received TBI showed significant reductions in cannabis use. Moreover, the reductions in alcohol use after TBI were found among men (p ≤ 0.01), but not among women. Although CBI reduced cannabis use days when examined as a sole outcome, it did not result in significant reductions in severity of alcohol use and cannabis use relative to EUC. |
| Elison-Davies et al., 2020 [37] | n = 5792 individuals; mean age = 40.54 years; a total of 1489 (26%) participants provided post-treatment data; type of dependence: nicotine, alcohol, opioids, heroin, benzodiazepines, cocaine, amphetamine, cannabis, novel psychoactive substances, prescribed medications. | on-line PC |
| Breaking Free Online (BFO). It is a digital intervention for individuals with substance misuse, containing 12 main behavioral change techniques that can be delivered with practitioner support as “computer-assisted therapy” or as self-help. The BFO program uses baseline RPM data to populate a visual depiction of a six-domain biopsychosocial model, the “Lifestyle Balance Model” (LBM), which forms the theoretical underpinnings of BFO and is based on the five-factor model used in cognitive behavioral therapy (CBT). | Effect sizes estimation revealed a medium effect size for changes in self-reported weekly alcohol consumption (r = 0.55), and small effect sizes for changes in self-reported drug consumption (r = 0.47), and severity of drug (r = 0.29) and alcohol dependence (r = 0.28). Significant reductions in SDS score and in overall RPM were also found (p ≤ 0.001). |
| Elison-Davies et al., 2021a [38] | n = 2571 individuals; mean age = 38.42 years; a total of 1107 (43%) completed a post-treatment assessment; type of dependence: heroin. | on-line PC |
| Breaking Free Online (BFO), as described previously. | Participants were provided with access to the computer assisted treatment program for 12 months, and engaged with it as self-directed treatment. A medium effect size was found for reductions in weekly opioid use (r = 0.71), and small effect sizes for reductions in severity of opioid dependence (r = 0.42) from baseline to post-treatment. Improvements were also found in all RPM six domains (p ≤ 0.001). |
| Elison-Davies et al., 2021b [39] | n = 1830 participants; mean age = 33.80 years; a total of 460 subjects (25%) completed both at baseline and at follow-up assessment; type of dependence: opioids. | on-line PC |
| Breaking Free Online (BFO), as described previously. | Participants were provided with access to the computer assisted treatment program for 12 months, and engaged with it as self-directed treatment. Differences with small effect sizes were found among baseline and follow-up measures of cannabis use and RPM (r = 0.30 to 0.48; p ≤ 0.001). |
| Elison-Davies et al., 2017 [40] | n = 2311 individuals; mean age = 42.2 years; type of substances: heroin, cocaine, alcohol, prescribed and substitute medications, cannabis, amphetamines, novel psychoactive substances, tobacco, and club drugs. | on-line PC |
| Breaking Free Online (BFO), as described previously. | Participants were provided with access to the computer assisted treatment program for 12 months and engaged with it as self-directed treatment. The psychometric assessment was repeated at a mean of 8.2 weeks from baseline. Medium effect sizes were identified for reductions in alcohol and drug dependence between baseline and follow-up (r = 0.51). Smaller effect sizes were identified for changes in scores for RPM between baseline and follow-up (r = 0.19 to 0.39). Changes in severity of alcohol dependence was associated with completion of some LBM strategies, specifically “lifestyle” (p ≤ 0.012) and “negative thoughts” (p ≤ 0.009). Changes in scores for drug dependence were not associated with the number of times participants completed strategies in the six LBM modules (p ≤ 0.051). Changes in total RPM were associated with the number of times participants completed LBM module strategies, specifically on the “negative thoughts” module (p ≤ 0.001). |
| Han et al., 2018 [41] | n = 75 participants; mean age = 41.6 years; subjects were randomized as follows: 50 in the experimental group and 25 in the control group; type of substances: heroin, amphetamine-type substances (ATS). | smartphone app |
| mHealth app, developed specifically to help individuals with SUDs achieve and maintain recovery. The mHealth app is based on cognitive behavior therapy (CBT), which emphasizes triggers and coping strategies for relapse prevention, and self-determination theory (SDT), which motivates people to change and act for themselves. | Drug use results were provided at week 1 (W1), 2 (W2), 3 (W3), and 4 (W4). The number of subjects of the experimental group using/not using substances for each week provided by urine test, LET, and EMA were as follows. Urine use: W1 = 24; W2 = 21; W3 = 15; W4 = 11 not use: W1 = 19; W2 = 22; W3 = 27; W4 = 31 LET use: W1 = 15; W2 = 12; W3 = 10; W4 = 7 not use: W1 = 33; W2 = 36; W3 = 38; W4 = 41 EMA use: W1 = 12; W2 = 10; W3 = 6; W4 = 5 not use: W1 = 28; W2 = 25; W3 = 26; W4 = 25 |
| Kay-Lambkin et al., 2014 [42] | n = 35 clients; mean age = 42.11 years; subjects were divided as follows: 12 exposed to SHADE and 23 not exposed; type of substances: alcohol and cannabis. | PC |
| Self-Help for Alcohol and Other Drug Use and Depression (SHADE). It incorporates cognitive behavioral therapy (CBT) strategies to encourage reductions in depression and AOD (Alcohol and other drugs) use. | Client assessment was collected at baseline and at 15-week follow-up. For alcohol use between baseline and 15-week follow-up assessment. Participants who did not receive the SHADE modules reported a three-standard-drink per day reduction and three-standard-use of cannabis per day reduction between baseline and at 15-week follow-up assessment. Participants who were exposed to SHADE reported an eight-standard-drink per day reduction and nine-standard-use per day reduction in cannabis use over the same time period. |
| Leightley et al., 2018 [43] | n = 150 individuals who served in the UK military; age = 18 to 65 years; type of substances: alcohol. | Smartphone |
| Alongside the app (InDEx app). This app uses daily automated personalized text messages (SMS), corresponding to specific behavior change techniques, with content informed by the Health Action Process Approach (HAPA) for the intended purpose of promoting the use of the drinks’ diary, suggesting alternative behaviors, and providing feedback on goals setting. | Participants completed tests and measures at registration, on days 8, 15, and 22. Participants reduced the alcohol consumption for the following outcomes per week (W): drinking days (*): W1 (median = 4); W2 (median = 3); W3 (median = 3); W4 (median = 3) drink free days: W1 (median = 3); W2 (median = 3); W3 (median = 3); W4 (median = 3) unit per drinking days: W1 (median = 5.6); W2 (median = 6.5); W3 (median = 4.5); W4 (median = 4.7) unit consumed: W1 (median = 22.9); W2 (median = 20.4); W3 (median = 18.1); W4 (median = 15.9) alcoholic drinks per drinking day: W1 (median = 2); W2 (median = 3); W3 (median = 2); W4 (median = 2) binge drinking per day per week: W1 (median = 2); W2 (median = 2); W3 (median = 1); W4 (median = 2) A small change in AUDIT score was observed for participants who self-reported for Day 0 (registration) and Day 28 (final day) based on median score. |
| Wernette et al., 2018 [44] | n = 50 pregnant women at risk for substance use; mean age = 23.3 years; women were randomized as follows: 31 allocated to the intervention condition and 19 allocated to control; type of substances: alcohol and marijuana. | PC |
| Innovative computer-delivered intervention (the Health Checkup for Expectant Moms, HCEM) that targets women at risk for STI/HIV and alcohol/drug use during pregnancy. HCEM is a tailored, motivationally focused STI/HIV and substance use risk reduction intervention, and provides training in several relevant skills, informed by the Information-Motivation-Behavior (IMB) model, which theorizes that information and motivation activate one’s behavioral skills, which in turn lead to risk reduction. | Participants were tested at baseline and at 4-month follow-up. Women in the HCEM condition, compared to controls, had a significantly larger reduction in the odds of any self-reported marijuana or alcohol use from baseline to follow-up (p ≤ 0.015). The odds of alcohol or marijuana use at baseline were 11.7 times higher at baseline, compared with follow-up in women assigned to HCEM (p ≤ 0.001). Of the valid 27 hair samples, 5 were positive for cocaine (all were in the intervention condition), 1 of whom was also positive for opiates, and an additional 3 were positive for marijuana (1 control and 2 intervention). |
| Wodarski et al., 2015 [45] | n = 5775 college students; type of substance: alcohol and other substances not well specified. | computer-based intervention (merely informative). |
| The intervention provides college students with basic knowledge concerning substance use and abuse, and increases students’ awareness of their own potential risks by giving immediate feedback and individualized recommendations. | Binge drinking has dropped to 27% on campus (48% to 35% reduction in number of student reporting drinking five or more drinks at a time), and frequent binge drinking has dropped to 44% (25% to 14% reduction in the number of students reporting drinking five or more drinks at a time three or more times in the past 2 weeks). |
| Wu et al., 2014 [46] | n = 6911 adult smokers; age = 18 to 65 years; the complete case analysis included 3309 participants, randomized as follows: 1795 in the control group and 1514 in the intervention group; type of substance: nicotine. | PC |
| Effectiveness of computer-tailored Smoking Cessation Advice in Primary Care (ESCAPE), lasting 6 months. | Participants were tested at baseline and at 6-month follow-up. The clinical results showed that the intervention produced a modest increase in quit attempts during the 6-month follow-up compared with the control group (Odds Ratio = 1.13). There were no significant differences in 3-month prolonged abstinence between the treatment groups at the 6-month follow-up. |
| Zhang et al. 2019 [47] | n = 30 individuals; mean age = 43.76 years; type of substances: opioids, alcohol, cannabis and stimulants | app |
| A mobile-based attention bias modification intervention: Visual probe. | Tests and questionnaires were administered only at baseline. Attentional bias was administered on pre- and post-training. On day 1 of the intervention, participants were required to complete both a baseline attention bias assessment task and an attention bias modification training task (intervention). On the subsequent days (days 2 to 7), they completed the attention bias modification training task. Fourteen participants had positive attentional biases at baseline. For these, there was a general decrease in the attention bias scores from baseline to the end of the planned intervention trials. The changes in the scores ranged from 12 to 409.5 milliseconds, comparing the final attention bias scores (upon the completion of the intervention) with the baseline scores (at the start of the intervention). |
| Zhu et al. 2018 [48] | n = 40 subjects; mean age = 33.88 years; subjects were randomized as follows: 20 assigned to a computerized cognitive addiction therapy (CCAT) and 20 to a control group; type of substance: methamphetamine. | iPad |
| Methamphetamine Attention Bias Modification. Participants included in the CCAT group were also undergoing standard treatment; in addition, the participants received the CCAT training program that lasted for 4 weeks (20 sessions, five times a week, each session lasting approximately 60 min). After every CCAT session, a 5-min relaxation session was carried out by playing light music and watching pictures with relaxing effects. | Attentional bias was administered on pre- and post-training. There were no significant differences between the two groups in attention bias. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonfiglio, N.S.; Mascia, M.L.; Cataudella, S.; Penna, M.P. Digital Help for Substance Users (SU): A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11309. https://doi.org/10.3390/ijerph191811309
Bonfiglio NS, Mascia ML, Cataudella S, Penna MP. Digital Help for Substance Users (SU): A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(18):11309. https://doi.org/10.3390/ijerph191811309
Chicago/Turabian StyleBonfiglio, Natale Salvatore, Maria Lidia Mascia, Stefania Cataudella, and Maria Pietronilla Penna. 2022. "Digital Help for Substance Users (SU): A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 18: 11309. https://doi.org/10.3390/ijerph191811309
APA StyleBonfiglio, N. S., Mascia, M. L., Cataudella, S., & Penna, M. P. (2022). Digital Help for Substance Users (SU): A Systematic Review. International Journal of Environmental Research and Public Health, 19(18), 11309. https://doi.org/10.3390/ijerph191811309