
Training, Wellbeing and Recovery Load Monitoring in Female Youth Athletes


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Literature Review
2.1. Youth Athletes and the Long-Term Development Model
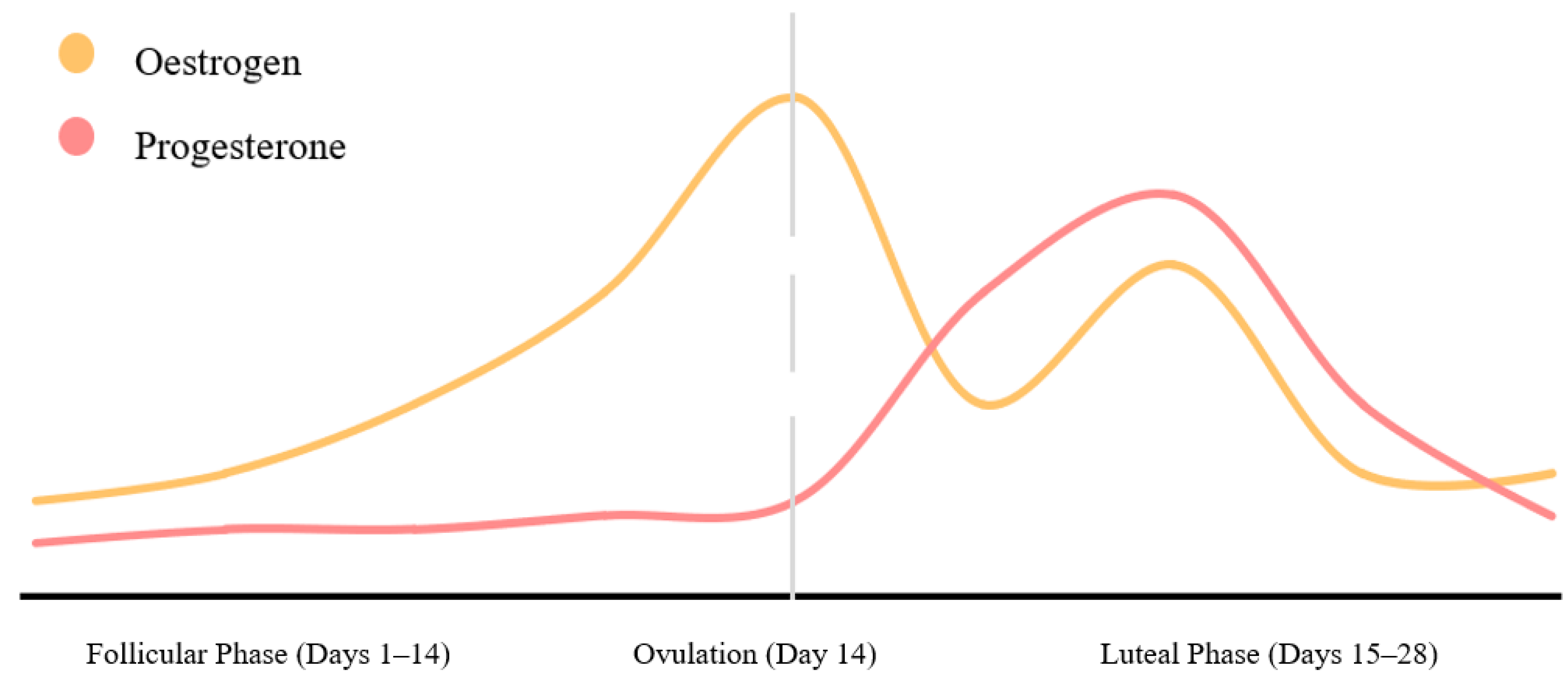
2.2. Menstrual Cycle Monitoring
2.3. Wellbeing Monitoring
2.4. Training Load
2.5. Recovery Monitoring
2.6. Injury Reporting
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bourdon, P.C.; Cardinale, M.; Murray, A.; Gastin, P.; Kellmann, M.; Varley, M.C.; Gabbett, T.J.; Coutts, A.J.; Burgess, D.J.; Gregson, W.; et al. Monitoring athlete training loads: Consensus statement. Int. J. Sports Physiol. Perform. 2017, 12, S2-161–S2-170. [Google Scholar] [CrossRef] [PubMed]
- McFarland, M.; Bird, S.P. A wellness monitoring tool for youth athletes. J. Aust. Strength Cond. 2014, 22, 22–26. [Google Scholar]
- Halson, S.L. Monitoring training load to understand fatigue in athletes. Sports Med. 2014, 44, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Mckeown, I.; Ball, N. Current practices of long term athlete development of junior athletes in high performance sport environments. J. Aust. Strength Cond. 2013, 21, 16–25. [Google Scholar]
- Bergeron, M.F.; Mountjoy, M.; Armstrong, N.; Chia, M.; Côté, J.; Emery, C.A.; Faigenbaum, A.; Hall, G.; Kriemler, S.; Léglise, M.; et al. International olympic committee consensus statement on youth athletic development. Br. J. Sports Med. 2015, 49, 843–851. [Google Scholar] [CrossRef]
- Taylor, J.; Wright, M.; Hurst, C.; Best, R. Contribution of planned and unplanned training to overall load in elite youth female football players. In Proceedings of the World Congress of Science in Soccer, Copenhagen, Denmark, 23–24 May 2015. [Google Scholar]
- Difiori, J.P.; Benjamin, H.J.; Brenner, J.; Gregory, A.; Jayanthi, N.; Landry, G.L.; Luke, A. Overuse injuries and burnout in youth sports: A position statement from the American medical society for sports medicine. Clin. J. Sport Med. 2014, 24, 3–20. [Google Scholar] [CrossRef]
- Witt, P.A.; Dangi, T. Why children/youth drop out of sports. J. Park Recreat. Adm. 2018, 36, 191–199. [Google Scholar] [CrossRef]
- Malisoux, L.; Frisch, A.; Urhausen, A.; Seil, R.; Theisen, D. Monitoring of sport participation and injury risk in young athletes. J. Sci. Med. Sport 2013, 16, 504–508. [Google Scholar] [CrossRef]
- Theisen, D.; Malisoux, L.; Seil, R.; Urhausen, A. Injuries in youth sports: Epidemiology, risk factors and prevention. Dtsch. Z. Sportmed. 2014, 65, 248–252. [Google Scholar] [CrossRef]
- Ridenour, R.; Hennrikus, W. Overuse injuries in pediatric athletes. Adv. Pediatr. 2020, 67, 171–182. [Google Scholar] [CrossRef]
- Gustafsson, H.; Kenttä, G.; Hassmén, P.; Lundqvist, C. Prevalence of burnout in competitive adolescent athletes. Sport Psychol. 2007, 21, 21–37. [Google Scholar] [CrossRef]
- Thorpe, R.T.; Atkinson, G.; Drust, B.; Gregson, W. Monitoring fatigue status in elite team-sport athletes: Implications for practice. Int. J. Sports Physiol. Perform. 2017, 12, S2-27–S2-34. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, J.R.; Kaminsky, M. Use of performance testing for monitoring overtraining in elite youth basketball players. Strength Cond. J. 2000, 22, 54–62. [Google Scholar] [CrossRef]
- Knicker, A.; Renshaw, I.; Oldham, A.; Cairns, S. Interactive processes link the multiple symptoms of fatigue in sport competition. Sports Med. 2011, 41, 307–328. [Google Scholar] [CrossRef]
- Corcoran, G.; Bird, S.P. Monitoring overtraining in athletes: A brief review and practical applications for strength and conditioning coaches. J. Aust. Strength Cond. 2012, 20, 39–51. [Google Scholar]
- Pind, R.; Mäestu, J. Monitoring training load: Necessity, methods and applications. Acta Kinesiol. Univ. Tartu. 2018, 23, 7–18. [Google Scholar] [CrossRef]
- Wing, C. Monitoring athlete load: Data collection methods and practical recommendations. Strength Cond. J. 2018, 40, 26–39. [Google Scholar] [CrossRef]
- Nimphius, S. Exercise and sport science failing by design in understanding female athletes. Int. J. Sports Physiol. Perform. 2019, 14, 1157–1158. [Google Scholar] [CrossRef]
- Emmonds, S.; Heyward, O.; Jones, B. The challenge of applying and undertaking research in female sport. Sport. Med.-Open 2019, 5, 1–4. [Google Scholar] [CrossRef]
- Constantini, N.W.; Dubnov, G.; Lebrun, C.M. The menstrual cycle and sport performance. Clin. Sports Med. 2005, 24, e51–e82. [Google Scholar] [CrossRef]
- Eime, R.M.; Harvey, J.T.; Charity, M.J.; Payne, W.R. Population levels of sport participation: Implications for sport policy. BMC Public Health 2016, 16, 1–8. [Google Scholar] [CrossRef]
- Katzmarzyk, P.; Denstel, K.; Beals, K.; Carlson, J.; Crouter, S.; McKenzie, T.; Pate, R. Results from the United States 2018 report card on physical activity for children and youth. J. Phys. Act. Heal. 2018, 15, S422–S424. [Google Scholar] [CrossRef]
- Westerbeek, H.; Eime, R. The physical activity and sport participation framework—a policy model toward being physically active across the lifespan. Front. Sport. Act. Living 2021, 3, 90. [Google Scholar] [CrossRef]
- Sport New Zealand. Active NZ 2018 Participation Report. Available online: https://sportnz.org.nz/media/1440/published-final-active-nz-main-report-the-new-zealand-participation-survey-2018-12-august-2019.pdf (accessed on 25 June 2020).
- Lloyd, R.S.; Cronin, J.B.; Faigenbaum, A.D.; Haff, G.; Howard, R.; Kraemer, W.J.; Micheli, L.J.; Myer, G.D.; Oliver, J.L. National strength and conditioning position statement on long-term athletic development. J. Strength Cond. Res. 2016, 30, 1491–1509. [Google Scholar] [CrossRef]
- Carlman, P.; Wagnsson, S.; Patriksson, G. Causes and consequences of dropping out from organized youth sports. Swedish J. Sport Res. 2013, 2, 26–54. [Google Scholar]
- Ford, P.; de Ste Croix, M.; Lloyd, R.; Meyers, R.; Moosavi, M.; Oliver, J.; Till, K.; Williams, C. The long-term athlete development model: Physiological evidence and application. J. Sports Sci. 2011, 29, 389–402. [Google Scholar] [CrossRef]
- Brenner, J.S.; LaBella, C.R.; Brooks, M.A.; Diamond, A.; Hennrikus, W.; Weiss Kelly, A.K.; LaBotz, M.; Logan, K.; Loud, K.J.; Moffatt, K.A.; et al. Sports specialization and intensive training in young athletes. Pediatrics 2016, 138, e20162148. [Google Scholar] [CrossRef]
- Myer, G.D.; Jayanthi, N.; DiFiori, J.P.; Faigenbaum, A.D.; Kiefer, A.W.; Logerstedt, D.; Micheli, L.J. Sports specialization, part II: Alternative solutions to early sport specialization in youth athletes. Sports Health 2016, 8, 65–73. [Google Scholar] [CrossRef]
- Law, M.P.; Côté, J.; Ericsson, K.A. Characteristics of expert development in rhythmic gymnastics: A retrospective study. Int. J. Sport Exerc. Psychol. 2007, 5, 82–103. [Google Scholar] [CrossRef]
- Jayanthi, N.; Schley, S.; Cumming, S.; Myer, G.; Saffel, H.; Hartwig, T.; Gabbett, T. Developmental training model for the sport specialized youth athlete: A dynamic strategy for individualizing load-response during maturation. Sports Health 2022, 14, 142–153. [Google Scholar] [CrossRef]
- McGowan, J.; Whatman, C.; Walters, S. The associations of early specialisation and sport volume with musculoskeletal injury in New Zealand children. J. Sci. Med. Sport 2020, 23, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, R.S.; Oliver, J.L.; Faigenbaum, A.D.; Myer, G.D.; De Ste Croix, M.B.A. Chronological age vs. biological maturation: Implications for exercise programming in youth. J. Strength Cond. Res. 2014, 28, 1454–1464. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, D.; Metheny, J. Overuse injuries in youth sports: Biomechanical considerations. Med. Sci. Sports Exerc. 2001, 33, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Baxter-jones, A.D.C. Common skeletal injuries in young athletes. Sports Med. 1995, 19, 137–149. [Google Scholar] [CrossRef]
- Julian, R.; Hecksteden, A.; Fullagar, H.H.K.; Meyer, T. The effects of menstrual cycle phase on physical performance in female soccer players. PLoS ONE 2017, 12, e0173951. [Google Scholar] [CrossRef]
- İmamoglu, O.; Akyol, P.; Kishali, N.F.; Katkat, D.; Atan, T. Effects of menstrual cycle on sports performance. Int. J. Neurosci. 2006, 116, 1549–1563. [Google Scholar] [CrossRef]
- Sarwar, R.; Niclos, B.B.; Rutherford, O.M. Changes in muscle strength, relaxation rate and fatiguability during the human menstrual cycle. J. Physiol. 1996, 493, 267–272. [Google Scholar] [CrossRef]
- Romero-Moraleda, B.; Del Coso, J.; Gutiérrez-Hellín, J.; Ruiz-Moreno, C.; Grgic, J.; Lara, B. The influence of the menstrual cycle on muscle strength and power performance. J. Hum. Kinet. 2019, 68, 123–133. [Google Scholar] [CrossRef]
- Paludo, A.; Cook, C.; Owen, J.; Woodman, T.; Irwin, J.; Crewther, B. The impact of menstrual-cycle phase on basal and exercise-induced hormones, mood, anxiety and exercise performance in physically active women. J. Sports Med. Phys. Fitness 2021, 61, 461–467. [Google Scholar] [CrossRef]
- Sunitha, G.; Ravi, B.; Sudhir, G. Study of Vo2 max during phases of menstruation in young female athletes. J. Evol. Med. Dent. Sci. 2013, 2, 4070–4078. [Google Scholar] [CrossRef]
- Vescovi, J.D. The menstrual cycle and anterior cruciate ligament injury risk. Sports Med. 2010, 41, 91–101. [Google Scholar] [CrossRef]
- Balachandar, V.; Marciniak, J.L.; Wall, O.; Balachandar, C. Effects of the menstrual cycle on lower-limb biomechanics, neuromuscular control, and anterior cruciate ligament injury risk: A systematic review. Muscles Ligaments Tendons J. 2017, 7, 136–146. [Google Scholar] [CrossRef]
- Herzberg, S.D.; Motu’apuaka, M.L.; Lambert, W.; Fu, R.; Brady, J.; Guise, J.M. The effect of menstrual cycle and contraceptives on ACL injuries and laxity: A systematic review and meta-analysis. Orthop. J. Sport. Med. 2017, 5, 1–10. [Google Scholar] [CrossRef]
- Brown, K.A.; Dewoolkar, A.V.; Baker, N.; Dodich, C. The female athlete triad: Special considerations for adolescent female athletes. Transl. Pediatr. 2017, 6, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Nattiv, A.; Loucks, A.B.; Manore, M.; Sanborn, C.; Sundgot-borgen, J.; Warren, M. The female athlete triad. Med. Sci. Sports Exerc. 2007, 39, 1867–1883. [Google Scholar] [CrossRef]
- Nichols, J.F.; Rauh, M.J.; Lawson, M.J.; Ji, M.; Barkai, H. Prevalence of the female athlete triad syndrome among high school athletes. Arch. Pediatr. Adolesc. Med. 2006, 160, 137–142. [Google Scholar] [CrossRef]
- Thein-Nissenbaum, J.M.; Carr, K.E. Female athlete triad syndrome in the high school athlete. Phys. Ther. Sport 2011, 12, 108–116. [Google Scholar] [CrossRef]
- Nose-Ogura, S.; Yoshino, O.; Dohi, M.; Kigawa, M.; Harada, M.; Kawahara, T.; Osuga, Y.; Saito, S. Low bone mineral density in elite female athletes with a history of secondary amenorrhea in their teens. Clin. J. Sport Med. 2020, 30, 245–250. [Google Scholar] [CrossRef]
- Rauh, M.J.; Nichols, J.F.; Barrack, M.T. Relationships among injury and disordered eating, menstrual dysfunction, and low bone mineral density in high school athletes: A prospective study. J. Athl. Train. 2010, 45, 243–252. [Google Scholar] [CrossRef]
- Janse DE Jonge, X.; Thompson, B.; Han, A. Methodological recommendations for menstrual cycle research in sports and exercise. Med. Sci. Sports Exerc. 2019, 51, 2610–2617. [Google Scholar] [CrossRef]
- Barron, M.L.; Fehring, R.J. Basal body temperature assessment: Is it useful to couples seeking pregnancy? MCN Am. J. Matern./Child Nurs. 2005, 30, 290–298. [Google Scholar] [CrossRef]
- Bull, J.R.; Rowland, S.; Berglund Scherwitzl, E.; Scherwitzl, R.; Gemzell Danielsson, K.; Harper, J. Real-world menstrual cycle characteristics of more than 600,000 menstrual cycles. NPJ Digit. Med. 2019, 2, 1–8. [Google Scholar] [CrossRef]
- Gandara, B.K.; Leresche, L.; Mancl, L. Patterns of salivary estradiol and progesterone across the menstrual cycle. Ann. N. Y. Acad. Sci. 2007, 1098, 446–450. [Google Scholar] [CrossRef]
- Gordon, D.; Scruton, A.; Barnes, R.; Baker, J.; Prado, L.; Merzbach, V. The effects of menstrual cycle phase on the incidence of plateau at VO2max and associated cardiorespiratory dynamics. Clin. Physiol. Funct. Imaging 2018, 38, 689–698. [Google Scholar] [CrossRef]
- Allen, A.M.; McRae-Clark, A.L.; Carlson, S.; Saladin, M.E.; Gray, K.M.; Wetherington, C.L.; McKee, S.A.; Allen, S.S. Determining menstrual phase in human biobehavioral research: A review with recommendations. Exp. Clin. Psychopharmacol. 2016, 24, 1–11. [Google Scholar] [CrossRef]
- Metcalf, M.G.; Evans, J.J.; Mackenzie, J.A. Indices of ovulation: Comparison of plasma and salivary levels of progesterone with urinary pregnanediol. J. Endocrinol. 1984, 100, 75–80. [Google Scholar] [CrossRef]
- Celec, P.; Ostatníková, D.; Skokňová, M.; Hodosy, J. Salivary sex hormones during menstrual cycle. Endocr. J. 2009, 56, 521–523. [Google Scholar] [CrossRef]
- Ackerman, K.E.; Stellingwerff, T.; Elliott-Sale, K.J.; Baltzell, A.; Cain, M.; Goucher, K.; Fleshman, L.; Mountjoy, M.L. #REDS (relative energy deficiency in sport): Time for a revolution in sports culture and systems to improve athlete health and performance. Br. J. Sports Med. 2020, 54, 369–370. [Google Scholar] [CrossRef]
- Coelho, A.R.; Cascais, M.J. The female athlete triad relative energy deficiency in sports (RED-S). Rev. Bras. Ginecol. Obs. 2021, 43, 395–402. [Google Scholar] [CrossRef]
- Brown, N.; Knight, C.J.; Forrest, L.J. Elite female athletes’ experiences and perceptions of the menstrual cycle on training and sport performance. Scand. J. Med. Sci. Sports 2020, 00, 1–18. [Google Scholar] [CrossRef]
- Hamlin, M.J.; Wilkes, D.; Elliot, C.A.; Lizamore, C.A.; Kathiravel, Y. Monitoring training loads and perceived stress in young elite university athletes. Front. Physiol. 2019, 10, 34. [Google Scholar] [CrossRef] [PubMed]
- Malone, S.; Owen, A.; Newton, M.; Mendes, B.; Tiernan, L.; Hughes, B.; Collins, K. Wellbeing perception and the impact on external training output among elite soccer players. J. Sci. Med. Sport 2018, 21, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Matos, N.F.; Winsley, R.J.; Williams, C.A. Prevalence of nonfunctional overreaching/overtraining in young english athletes. Med. Sci. Sports Exerc. 2011, 43, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Pyne, D.B. Respiratory inflammation and infections in high-performance athletes. Immunol. Cell Biol. 2016, 94, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Kellmann, M.; Bertollo, M.; Bosquet, L.; Brink, M.; Coutts, A.J.; Duffield, R.; Erlacher, D.; Halson, S.L.; Hecksteden, A.; Heidari, J.; et al. Recovery and performance in sport: Consensus statement. Int. J. Sports Physiol. Perform. 2018, 13, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Walsh, N.P.; Gleeson, M.; Shephard, R.J.; Gleeson, M.; Woods, J.A.; Bishop, N.C.; Fleshner, M.; Green, C.; Pedersen, B.K.; Hoffman-Goetz, L.; et al. Position statement part one: Immune function and exercise. Exerc. Immunol. Rev. 2011, 17, 6–63. [Google Scholar]
- Gastin, P.; Meyer, D.; Robinson, D. Perceptions of wellness in monitoring adaptive responses to training and competition in elite australian football. J. Strength Cond. Res. 2013, 27, 2518–2526. [Google Scholar] [CrossRef]
- Taylor, K.; Chapman, D.; Cronin, J.; Newton, M.; Gill, N. Fatigue monitoring in high performance sport: A survey of current trends. J. Aust. Strength Cond. 2012, 20, 12–23. [Google Scholar]
- Saw, A.; Main, L.; Robertson, S.; Gastin, P. Athlete self-report measure use and associated psychological alterations. Sports 2017, 5, 54. [Google Scholar] [CrossRef]
- Tibana, R.A.; de Sousa, N.M.F.; Prestes, J.; Feito, Y.; Ferreira, C.E.; Voltarelli, F.A. Monitoring training load, well-being, heart rate variability, and competitive performance of a functional-fitness female athlete: A case study. Sports 2019, 7, 35. [Google Scholar] [CrossRef]
- Coutts, A.J.; Reaburn, P. Monitoring changes in rugby league players perceived stress and recovery during intensified training. Percept. Mot. Skills 2008, 106, 904–916. [Google Scholar] [CrossRef]
- Gallo, T.F.; Cormack, S.J.; Gabbett, T.J.; Lorenzen, C.H. Self-reported wellness profiles of professional australian football players during the competition phase of the season. J. Strength Cond. Res. 2017, 31, 495–502. [Google Scholar] [CrossRef]
- Hooper, S.L.; Mackinnon, L.T. Monitoring overtraining in athletes: Recommendations. Sports Med. 1995, 20, 321–327. [Google Scholar] [CrossRef]
- McLean, B.D.; Coutts, A.J.; Kelly, V.; McGuigan, M.R.; Cormack, S.J. Neuromuscular, endocrine, and perceptual fatigue responses during different length between-match microcycles in professional rugby league players. Int. J. Sports Physiol. Perform. 2010, 5, 367–383. [Google Scholar] [CrossRef]
- Thorpe, R.T.; Strudwick, A.J.; Buchheit, M.; Atkinson, G.; Drust, B.; Gregson, W. The tracking of monitoring fatigue status across in-season training weeks in elite soccer players. Int. J. Sports Physiol. Perform. 2016, 11, 947–952. [Google Scholar] [CrossRef]
- Borresen, J.; Lambert, M. The quantification of training load, the training response and the effect on performance. Sports Med. 2009, 39, 779–795. [Google Scholar] [CrossRef]
- Haddad, M.; Stylianides, G.; Djaoui, L.; Dellal, A.; Chamari, K. Session-RPE method for training load monitoring: Validity, ecological usefulness, and influencing factors. Front. Neurosci. 2017, 11, 612. [Google Scholar] [CrossRef]
- Clarke, N.; Farthing, J.; Norris, S.; Arnold, B.; Lanovaz, K. Quantification of training load in canadian football:application of session-rpe in collision-based team sports. J. Strength Cond. Res. 2013, 27, 2198–2205. [Google Scholar] [CrossRef]
- Foster, C. Monitoring training in athletes with reference to overtraining syndrome. Med. Sci. Sports Exerc. 1998, 30, 1164–1168. [Google Scholar] [CrossRef]
- Day, M.L.; McGuigan, M.R.; Brice, G.; Foster, C. Monitoring resistance training using the session RPE scale. J. strength Cond. Res. 2004, 18, 353–358. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Naidu, S.; Fanchini, M.; Cox, A.; Smeaton, J.; Hopkins, W.G.; Serpiello, F. Validity of session rating of perceived exertion assessed via the CR100 scale to track internal load in elite youth football players. Int. J. Sports Physiol. Perform. 2018, 14, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Padulo, J.; Salernitano, G.; Maurino, L.; Stefano, V.; Gevat, C. Validity of Rpe session in young male karate athletes. Sci. Mov. Health 2014, 14, 182–185. [Google Scholar]
- Scantlebury, S.; Till, K.; Sawczuk, T.; Phibbs, P.; Jones, B. The validity of retrospective session-rating of perceived exertion to quantify training load in youth athletes. J. Strength Cond. Res. 2017, 32, 1975–1980. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, J.C.; Tenenbaum, G. Perceived effort—Can it be considered gestalt? Psychol. Sport Exerc. 2006, 7, 463–476. [Google Scholar] [CrossRef]
- McLaren, S.J.; Macpherson, T.W.; Coutts, A.J.; Hurst, C.; Spears, I.R.; Weston, M. The relationships between internal and external measures of training load and intensity in team sports: A meta-analysis. Sports Med. 2018, 48, 641–658. [Google Scholar] [CrossRef]
- Stagno, K.M.; Thatcher, R.; van Someren, K.A. A Modified TRIMP to quantify the in-season training load of team sport players. J. Sports Sci. 2007, 25, 629–634. [Google Scholar] [CrossRef]
- Sanders, D. Quantification of training load in endurance sports: Additional considerations. Strength Cond. J. 2018, 40, 115–116. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Rampinini, E.; Coutts, A.J.; Sassi, A.; Marcora, S.M. Use of RPE-based training load in soccer. Med. Sci. Sports Exerc. 2004, 36, 1042–1047. [Google Scholar] [CrossRef]
- Hopkins, W.G. Mesaures of reliability in sports medicine and science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef]
- Fox, J.L.; Scanlan, A.T.; Stanton, R. A review of player monitoring approaches in basketball: Current trends and future directions. J. Strength Cond. Res. 2017, 31, 2021–2029. [Google Scholar] [CrossRef]
- Duggan, J.D.; Moody, J.A.; Byrne, P.J.; Cooper, S.; Ryan, L. Training load monitoring considerations for female gaelic team sports: From theory to practice. Spoprts 2021, 9, 84. [Google Scholar] [CrossRef]
- Murray, A. Managing the training load in adolescent athletes athlete development: A modern training young athletes. Int. J. Sports Physiol. Perform. 2017, 12, S2-42–S2-49. [Google Scholar] [CrossRef]
- Hulin, B.T.; Gabbett, T.J.; Lawson, D.W.; Caputi, P.; Sampson, J.A. The acute: Chronic workload ratio predicts injury: High chronic workload may decrease injury risk in elite rugby league players. Br. J. Sports Med. 2016, 50, 231–236. [Google Scholar] [CrossRef]
- Gabbett, T.J. The training—injury prevention paradox: Should athletes be training smarter and harder? Br. J. Sports Med. 2016, 50, 273–280. [Google Scholar] [CrossRef]
- Williams, S.; West, S.; Cross, M.; Stokes, K.A. Better way to determine the acute: Chronic workload ratio? Br. J. Sports Med. 2016, 51, 209–210. [Google Scholar] [CrossRef]
- Hunter, J.S. The exponentially weighted moving average. J. Qual. Technol. 1986, 18, 203–210. [Google Scholar] [CrossRef]
- Griffin, A.; Kenny, I.C.; Comyns, T.M.; Lyons, M. The association between the acute: Chronic workload ratio and injury and its application in team sports: A systematic review. Sports Med. 2020, 50, 561–580. [Google Scholar] [CrossRef]
- Malone, S.; Owen, A.; Newton, M.; Mendes, B.; Collins, K.D.; Gabbett, T.J. The acute: Chonic workload ratio in relation to injury risk in professional soccer. J. Sci. Med. Sport 2017, 20, 561–565. [Google Scholar] [CrossRef]
- Murray, N.B.; Gabbett, T.J.; Townshend, A.D.; Hulin, B.T.; McLellan, C.P. Individual and combined effects of acute and chronic running loads on injury risk in elite australian footballers. Scand. J. Med. Sci. Sports 2016, 27, 990–998. [Google Scholar] [CrossRef]
- Bahr, R. Why screening tests to predict injury do not work-and probably never will.: A critical review. Br. J. Sports Med. 2016, 50, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Pepe, M.S.; Janes, H.; Longton, G.; Leisenring, W.; Newcomb, P. Limitations of the odds ratio in gauging the performance of a diagnostic, prognostic, or screening marker. Am. J. Epidemiol. 2004, 159, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Fanchini, M.; Rampinini, E.; Riggio, M.; Coutts, A.J.; Pecci, C.; McCall, A. Despite association, the acute: Chronic work load ratio does not predict non-contact injury in elite footballers. Sci. Med. Footb. 2018, 2, 108–114. [Google Scholar] [CrossRef]
- Crowcroft, S.; McCleave, E.; Slattery, K.; Coutts, A.J. Assessing the measurement sensitivity and diagnostic characteristics of athlete-monitoring tools in national swimmers. Int. J. Sports Physiol. Perform. 2017, 12, S2-95–S2-100. [Google Scholar] [CrossRef]
- Dalen-Lorentsen, T.; Andersen, T.E.; Bjørneboe, J.; Vagle, M.; Martin, K.N.; Kleppen, M.; Fagerland, M.W.; Clarsen, B. A cherry tree ripe for picking: The relationship between the acute-chronic workload ratio and health problems. J. Orthop. Sports Phys. Ther. 2021, 51, 162–173. [Google Scholar] [CrossRef]
- Aughey, R.J. Applications of GPS technologies to field sports. Int. J. Sports Physiol. Perform. 2011, 6, 295–310. [Google Scholar] [CrossRef]
- Jennings, D.; Cormack, S.; Coutts, A.J.; Boyd, L.; Aughey, R.J. The validity and reliability of GPS units for measuring distance in team sport specific running patterns. Int. J. Sports Physiol. Perform. 2010, 5, 328–341. [Google Scholar] [CrossRef] [Green Version]
- Cummins, C.; Orr, R.; O’Connor, H.; West, C. Global positioning systems (GPS) and microtechnology sensors in team sports: A Systematic review. Sports Med. 2013, 43, 1025–1042. [Google Scholar] [CrossRef]
- Evans, J.; Soma, D.; Sikka, R. Motion analysis of youth soccer players using global position system tracking. Pediatrics 2019, 144, 186. [Google Scholar] [CrossRef]
- Vescovi, J.D. Motion characteristics of youth women soccer matches: Female athletes in motion (FAiM) study. Int. J. Sports Med. 2014, 35, 110–117. [Google Scholar] [CrossRef]
- Busbridge, A.R.; Hamlin, M.J.; Jowsey, J.A.; Vanner, M.H.; Olsen, P.D. Running demands of provincial women’s rugby union matches in New Zealand. J. Strength Cond. Res. 2020, 36, 1059–1063. [Google Scholar] [CrossRef]
- McFadden, B.A.; Walker, A.J.; Bozzini, B.N.; Sanders, D.J.; Arent, S.M. Comparison of internal and external training loads in male and female collegiate soccer players during practices vs. games. J. strength Cond. Res. 2020, 34, 969–974. [Google Scholar] [CrossRef]
- Bradley, P.S.; Vescovi, J.D. Velocity thresholds for women’s soccer matches: Sex specificity dictates high-speed-running and sprinting thresholds-female athletes in motion (FAiM). Int. J. Sports Physiol. Perform. 2015, 10, 112–116. [Google Scholar] [CrossRef]
- Lambert, M.; Borresen, J. Measuring training load in sports. Int. J. Sports Physiol. Perform. 2010, 5, 406–411. [Google Scholar] [CrossRef]
- Rampinini, E.; Alberti, G.; Fiorenza, M.; Riggio, M.; Sassi, R.; Borges, T.O.; Coutts, A.J. Accuracy of GPS devices for measuring high-intensity running in field base team sports. Int. J. Sports Med. 2015, 36, 49–53. [Google Scholar]
- Coutts, A.J.; Duffield, R. Validity and reliability of GPS devices for measuring movement demands of team sports. J. Sci. Med. Sport 2010, 13, 133–135. [Google Scholar] [CrossRef]
- Lacome, A.M.; Peeters, A.; Mathieu, B.; Marrier, B.; Piscione, J. Assessing sprinting performance in rugby sevens using GPS. Biol. Sport 2019, 36, 25–29. [Google Scholar] [CrossRef]
- Flatt, A.A.; Howells, D. Effects of varying training load on heart rate variability and running performance among an olympic rugby sevens team. J. Sci. Med. Sport 2018, 22, 222–226. [Google Scholar] [CrossRef]
- Flatt, A.; Esco, M. Evaluating individual training adaptation with smartphone-derived heart rate variability in a collegiate female soccer team. J. Strength Cond. Res. 2016, 30, 378–385. [Google Scholar] [CrossRef]
- Plews, D.J.; Laursen, P.B.; Kilding, A.E.; Buchheit, M. Heart rate variability in elite triathletes, is variation in variability the key to effective training? A case comparison. Eur. J. Appl. Physiol. 2012, 112, 3729–3741. [Google Scholar] [CrossRef]
- Flatt, A.A.; Esco, M.R. Smartphone-derived heart-rate variability and training load in a women’s soccer team. Int. J. Sports Physiol. Perform. 2015, 10, 994–1000. [Google Scholar] [CrossRef]
- Nakamura, F.Y.; Pereira, L.A.; Cal Abad, C.C.; Cruz, I.F.; Flatt, A.A.; Esco, M.R.; Loturco, I. Adequacy of the ultra-short-term HRV to assess adaptive processes in youth female basketball players. J. Hum. Kinet. 2017, 56, 73–80. [Google Scholar] [CrossRef]
- Perrotta, A.S.; Jeklin, A.T.; Hives, B.A.; Meanwell, L.E.; Warburton, D.E.R. Validity of the elite HRV smartphone application for examining heart rate variability in a field-based setting. J. Strength Cond. Res. 2017, 31, 2296–2302. [Google Scholar] [CrossRef]
- Kallus, K.W.; Kellmann, M.; Bochum, R. The Recovery-Stress Questionnaires: User Manual; Pearson: Frankfurt, Germany, 2016; pp. 27–48. [Google Scholar]
- Nederhof, E.; Brink, M.S.; Lemmink, K.A.P.M. Reliability and validity of the dutch recovery stress questionnaire for athletes. Int. J. Sport Psychol. 2008, 39, 301–311. [Google Scholar]
- Bouget, M.; Rouveix, M.; Michaux, O.; Pequignot, J.M.; Filaire, E. Relationships among training stress, mood and dehydroepiandrosterone sulphate/cortisol ratio in female cyclists. J. Sports Sci. 2006, 24, 1297–1302. [Google Scholar] [CrossRef]
- Coutts, A.J.; Wallace, L.K.; Slattery, K.M. Monitoring changes in performance, physiology, biochemistry, and psychology during overreaching and recovery in triathletes. Int. J. Sports Med. 2007, 28, 125–134. [Google Scholar] [CrossRef]
- Purge, P.; Jürimäe, J.; Jürimäe, T. Hormonal and psychological adaptation in elite male rowers during prolonged training. J. Sports Sci. 2006, 24, 1075–1082. [Google Scholar] [CrossRef]
- Coutts, A.J.; Reaburn, P.; Piva, T.J.; Rowsell, G.J. Monitoring for overreaching in rugby league players. Eur. J. Appl. Physiol. 2007, 99, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Kellmann, M.; Altenburg, D.; Lormes, W.; Steinacker, J. Assessing stress and recovery during preparation for the world championships in rowing. Sport Psychol. 2001, 15, 151–167. [Google Scholar] [CrossRef]
- Tibbert, S.; Morris, T.; Andersen, M. Validity of the recovery stress questionnaire. J. Sci. Med. Sport 2009, 12, S32–S33. [Google Scholar] [CrossRef]
- Nakhostin-Roohi, B.; Nasirvand Moradlou, A.; Mahmoodi Hamidabad, S.; Ghanivand, B. The effect of curcumin supplementation on selected markers of delayed onset muscle soreness (DOMS). Ann. Appl. Sport Sci. 2016, 4, 25–31. [Google Scholar] [CrossRef]
- Lau, W.Y.; Blazevich, A.J.; Newton, M.J.; Xuan Wu, S.S.; Nosaka, K. Assessment of muscle pain induced by elbow-flexor eccentric exercise. J. Athl. Train. 2015, 50, 1140–1148. [Google Scholar] [CrossRef]
- Nicol, L.M.; Rowlands, D.S.; Fazakerly, R.; Kellett, J. Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS). Eur. J. Appl. Physiol. 2015, 115, 1769–1777. [Google Scholar] [CrossRef]
- Slater, H.; Thériault, E.; Ronningen, B.O.; Clark, R.; Nosaka, K. Exercise-induced mechanical hypoalgesia in musculotendinous tissues of the lateral elbow. Man. Ther. 2010, 15, 66–73. [Google Scholar] [CrossRef]
- Myles, P.S.; Myles, D.B.; Galagher, W.; Boyd, D.; Chew, C.; MacDonald, N.; Dennis, A. Measuring acute postoperative pain using the visual analog scale: The minimal clinically important difference and patient acceptable symptom state. Br. J. Anaesth. 2017, 118, 424–429. [Google Scholar] [CrossRef]
- Gallagher, E.J.; Bijur, P.E.; Latimer, C.; Silver, W. Reliability and validity of a visual analog scale for acute abdominal pain in the ED. Am. J. Emerg. Med. 2002, 20, 287–290. [Google Scholar] [CrossRef]
- Sindhu, B.S.; Shechtman, O.; Tuckey, L. Validity, reliability, and responsiveness of a digital version of the visual analog scale. J. Hand Ther. 2011, 24, 356–364. [Google Scholar] [CrossRef]
- Keogh, E.; Herdenfeldt, M. Gender, coping and the perception of pain. Pain 2002, 97, 195–201. [Google Scholar] [CrossRef]
- Kölling, S.; Hitzschke, B.; Holst, T.; Ferrauti, A.; Meyer, T.; Pfeiffer, M.; Kellmann, M. Validity of the acute recovery and stress scale: Training monitoring of the German junior national field hockey team. Int. J. Sports Sci. Coach. 2015, 10, 529–542. [Google Scholar] [CrossRef] [Green Version]
- Colvin, A.; Lynn, A. Sport related injuries in the young female athlete. J. Transl. Pers. Med. A J. Transl. Pers. Med. 2010, 77, 307–314. [Google Scholar] [CrossRef]
- Ivković, A.; Franić, M.; Bojanić, I.; Pećina, M. Overuse injuries in female athletes. Croat. Med. J. 2007, 48, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Accident Claim Corporation. Significant Surge in Kiwi Kids Side-Lined by Sport Injuries [Media Release]. Available online: https://www.acc.co.nz/assets/Newsroom-documents/3f3d7ed2ab/mr-significant-surge-in-kiwi-kids-side-lined-by-sports-injuries.pdf (accessed on 14 June 2020).
- Crane, J.; Temple, V. A systematic review of dropout from organized sport among children and youth. Eur. Phys. Educ. Rev. 2015, 21, 114–131. [Google Scholar] [CrossRef]
- Leppänen, M.; Pasanen, K.; Kannus, P.; Vasankari, T.; Kujala, U.M.; Heinonen, A.; Parkkari, J. Epidemiology of overuse injuries in youth team sports: A 3-year prospective study. Int. J. Sports Med. 2017, 38, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Van Den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef]
- Frisch, A.; Seil, R.; Urhausen, A.; Croisier, J.L.; Lair, M.L.; Theisen, D. Analysis of sex-specific injury patterns and risk factors in young high-level athletes. Scand. J. Med. Sci. Sport. 2009, 19, 834–841. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; Brent, J.L.; Hewett, T.E. The effects of plyometric vs. dynamics stabilization and balance training on power, balance, and landing force in female athletes. J. Strength Cond. Res. 2006, 20, 345–353. [Google Scholar] [CrossRef]
- Griffin, L.Y.; Agel, J.; Albohm, M.J.; Arendt, E.A.; Dick, R.W.; Garrett, W.E.; Garrick, J.G.; Hewett, T.E.; Huston, L.; Ireland, M.L.; et al. Noncontact anterior cruciate ligament injuries: Risk factors and prevention strategies. J. Am. Acad. Orthop. Surg. 2000, 8, 141–150. [Google Scholar] [CrossRef]
- Maffulli, N.; Longo, U.G.; Gougoulias, N.; Loppini, M.; Denaro, V. Long-term health outcomes of youth sports injuries. Br. J. Sports Med. 2010, 44, 21–25. [Google Scholar] [CrossRef]
- Pless, B. Surveillance alone is not the answer. Inj. Prev. 2008, 14, 220–222. [Google Scholar] [CrossRef]
- Emery, C.A. Injury prevention in paediatric sport-related injuries: A scientific approach. Br. J. Sports Med. 2010, 44, 64–69. [Google Scholar] [CrossRef]
- Gabbett, T.J.; Jenkins, D.G. Relationship between training load and injury in professional rugby league players. J. Sci. Med. Sport 2011, 14, 204–209. [Google Scholar] [CrossRef]
- Whatman, C.; Walters, S.; Schluter, P. Coach and player attitudes to injury in youth sport. Phys. Ther. Sport 2018, 32, 1–6. [Google Scholar] [CrossRef]
- Emery, C.A.; Meeuwisse, W.H.; Hartmann, S.E. Evaluation of risk factors for injury in adolescent soccer: Implementation and validation of an injury surveillance system. Am. J. Sports Med. 2005, 33, 1882–1891. [Google Scholar] [CrossRef]
- Hunter, F.; Bray, J.; Christopher, T.; Smith, M.; Barrett, S.; Madden, J.; Abt, G.; Lovell, R. Individualisation of time-motion analysis: A method comparison and case report series. Int. J. Sports Med. 2014, 36, 41–48. [Google Scholar] [CrossRef]
- Till, K.; Lloyd, R.S.; Mccormack, S.; Williams, G.; Baker, J.; Eisenmann, J.C. Optimising long-term athletic development: An investigation of practitioners’ knowledge, adherence, practices and challenges. PLoS ONE 2022, 17, e0262995. [Google Scholar] [CrossRef]
- Starling, L.T.; Lambert, M.I. Monitoring rugby players for fitness and fatigue: What do coaches want? Int. J. Sports Physiol. Perform. 2018, 13, 777–782. [Google Scholar] [CrossRef]
- Lupo, C.; Tessitore, A.; Gasperi, L.; Gomez, M.A.R. Session-RPE for quantifying the load of different youth basketball training sessions. Biol. Sport 2017, 34, 11–17. [Google Scholar] [CrossRef]
- Rodríguez-Marroyo, J.A.; Antoñan, C. Validity of the session rating of perceived exertion for monitoring exercise demands in youth soccer players. Int. J. Sports Physiol. Perform. 2015, 10, 404–407. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Temm, D.A.; Standing, R.J.; Best, R. Training, Wellbeing and Recovery Load Monitoring in Female Youth Athletes. Int. J. Environ. Res. Public Health 2022, 19, 11463. https://doi.org/10.3390/ijerph191811463
Temm DA, Standing RJ, Best R. Training, Wellbeing and Recovery Load Monitoring in Female Youth Athletes. International Journal of Environmental Research and Public Health. 2022; 19(18):11463. https://doi.org/10.3390/ijerph191811463
Chicago/Turabian StyleTemm, Dani A., Regan J. Standing, and Russ Best. 2022. "Training, Wellbeing and Recovery Load Monitoring in Female Youth Athletes" International Journal of Environmental Research and Public Health 19, no. 18: 11463. https://doi.org/10.3390/ijerph191811463
APA StyleTemm, D. A., Standing, R. J., & Best, R. (2022). Training, Wellbeing and Recovery Load Monitoring in Female Youth Athletes. International Journal of Environmental Research and Public Health, 19(18), 11463. https://doi.org/10.3390/ijerph191811463