


The Impact of Colleague Suicide and the Current State of Postvention Guidance for Affected Co-Workers: A Critical Integrative Review

 , , ,
, , ,
Abstract
:1. Introduction
Review Aims
- What is the impact on staff of a colleague death by suicide?
- What is the current guidance for providing postvention support to staff following a colleague suicide and has this guidance been evaluated?
- What kinds of postvention have been offered, or ought to be offered, to staff affected by a colleague suicide and what are staff experiences of that postvention?
2. Methods
2.1. Eligibility Criteria
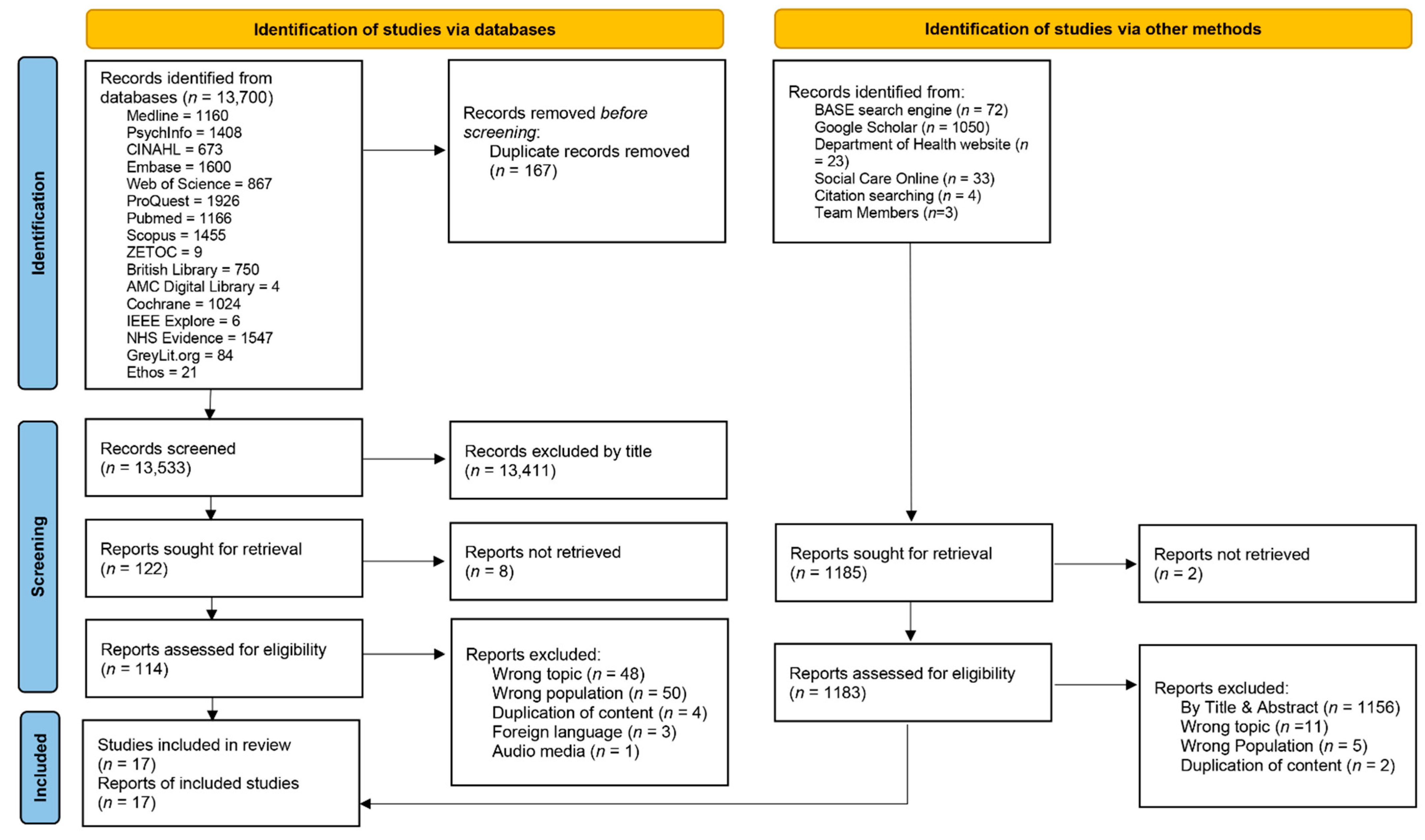
2.2. Search Strategy
2.3. Article Screening
2.4. Quality Appraisal
2.5. Data Extraction
2.6. Data Analysis
2.6.1. Coding the Material
2.6.2. Identifying the Themes
2.6.3. Constructing the Networks
2.6.4. Describe and Explore the Thematic Networks
2.6.5. Summarize the Thematic Network
2.6.6. Interpret Patterns
3. Results
3.1. Quality Appraisal of Included Articles
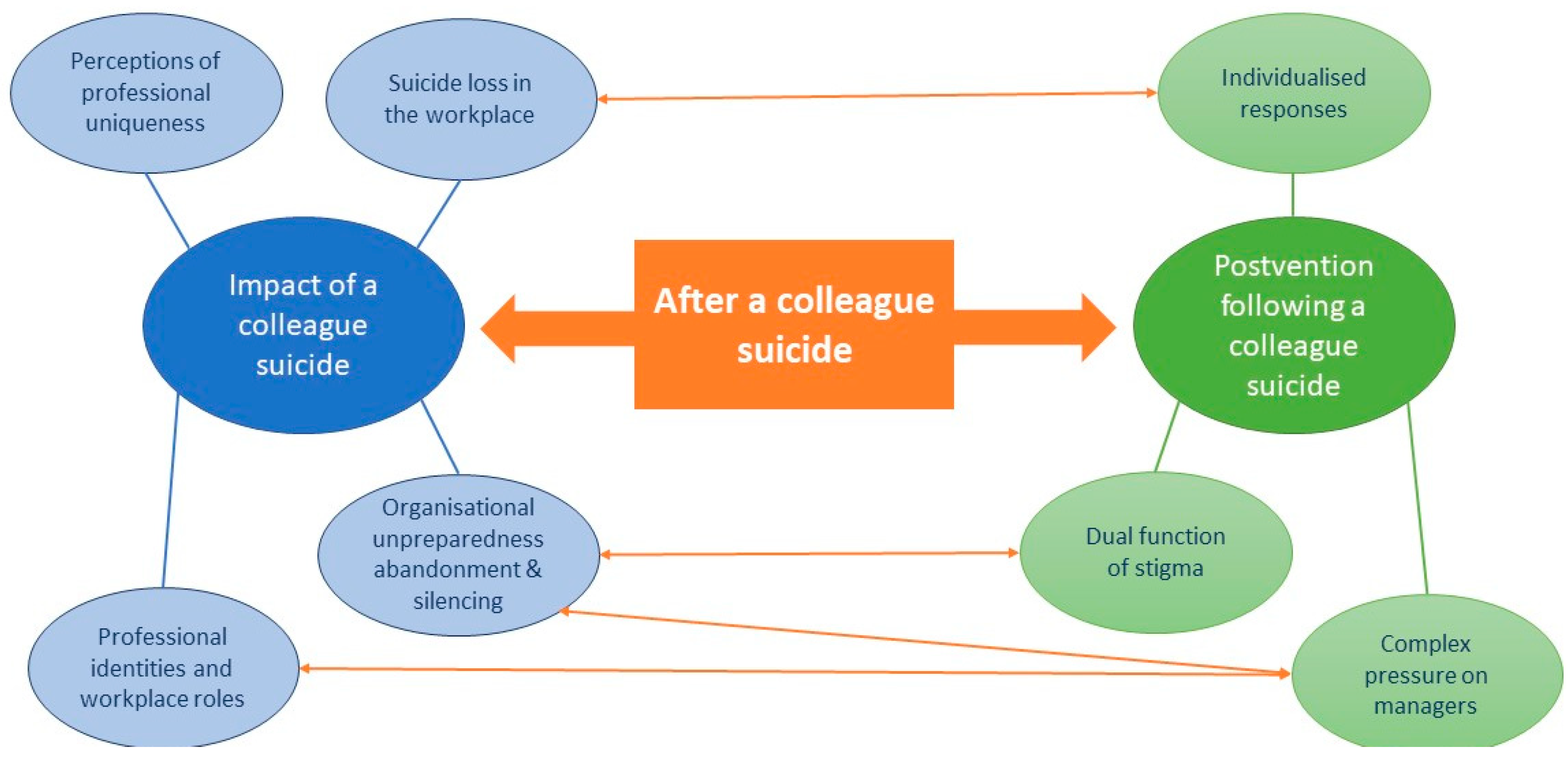
3.2. Thematic Network Analysis
3.2.1. Global Theme 1: Impact of the Loss of a Colleague to Suicide
Suicide Loss in the Workplace
Bereavement after suicide is often called ‘grief with the volume turned up’.[63]
as the same emotional burden experienced after the death of a family member.[65]
Sometimes the rationale for this increase in suicide or suicidal behavior occurs out of guilt, a distorted sense of loyalty, or a perceived false “permission” to do so.[60] (p. 3)
Professional Identities and Workplace Roles
the ambulance staff that attend the scene could have additional needs in relation to their efforts to help their colleague. There may have been a resuscitation attempt, for example. This places an increased burden on the clinicians present.[63]
As the line manager, when a colleague dies suddenly you have a responsibility to all team members to assist them in coming to terms with the sudden death, whilst dealing with your own emotions.[62]
It was already on social media, but the senior manager said it wasn’t our place to tell colleagues, as the family may not know yet, so then you’re chastised by staff for not letting people know. […] It all got very messy. And all that was on me. It was a lonely place that day.[63] (p. 22)
Perceptions of Professional Uniqueness in Bereavement
military suicide may have an even greater impact than bereavement experienced in most collegial relationships due to the proximity and intimacy required for a unit to function in a combat environment … It is not uncommon for service members to refer to one another as “brother”, “sister”, “brother-in-arms”.(p. 189)
“You feel the closeness of death, as in every funeral. However, as a Muslim, I do not find this right. According to our religion, it (suicide) is a rebellion against God.”[58]
Professional Unpreparedness, Abandonment, and Silencing
“It was very surreal–I had to deal with all of this, and I just acted on instinct. There was no help or guidance given to me. Suddenly I was in charge of everybody else’s feelings and just expected to carry on as normal.”[28] (p. 7)
In the absence of any guidance, our interviewees were obliged to ‘ring round’ desperately hoping to receive help which was not forthcoming. This clearly intensified their distress and the difficulties that practices, especially small practices, experienced.[28] (p. 17)
[participants] described absent or poor support and in some cases, deliberate attempts to prevent or stifle discussion and/or debriefing, although in some cases the issue of protecting the deceased’s confidentiality and/or sparing the family further anguish was mentioned.[59]
As long as you’re doing your job, doing what you need to do and say, administration would acknowledge if you lost your life in the line of duty. You’d be a hero. But the moment [an officer] loses their life because of suicide, it’s unspoken.[51] (p. 97)
3.2.2. Global Theme 2: Postvention Following a Colleague Suicide
Individualised Responses
‘We’re all adults. You have entrusted us with the authority to take people’s freedom and the authority to take lives, if necessary. […] So aside from offering programs, there’s nothing anybody can do to stop them’.[51] (p. 106)
the important information is that the person mistakenly felt that they could not get help for his or her problems, when in fact help was possible.[33] (p. 163)
Military leaders can be encouraged and taught to recognize that to compartmentalize the unit suicide and to ignore it in the short-term, may also place their units at risk.
Dual Function of Stigma
‘To have training on officer suicide would mean that [suicide] would have to be talked about. And that’s not going to happen.’[51] (p. 96)
Personnel allowed to attend the service were limited […]. Restricting access to the memorial service created a sense of shame about the death.[52]
…sometimes led to misguided efforts to maintain secrecy after a suicide death, including blaming or stigmatizing the deceased.[33] (p. 168)
Complex Pressure on Managers
3.2.3. Unifying Global Theme
4. Discussion
4.1. Workplace Cultures, Professional Contexts, and Individualised Responses
4.2. Unpreparedness, Abandonment, Silencing, and the Perpetuation of Stigma
4.3. Managers: Identities, Roles, and Complex Pressures
- Physical and emotional time and space for processing and grieving ought to be provided in workplaces to accommodate the emotional work that may follow a colleague suicide.
- Postvention guidance must be developed for specific professional groups, drawing on the lived experiences of that group, so that the specific needs of professional cultures and traits are understood.
- Guidance ought to include education around the dangers of stigma, the misunderstanding or misuse of ‘contagion’, and the protective factors of acknowledging and talking openly about suicide.
- Postvention guidance should acknowledge the competing pressures that managers experience following a colleague suicide and provide guidance for the support of managers whilst they, in turn, support their teams.
- Guidance could offer alternative models to the ‘postvention team’ to accommodate the limited resources of smaller or less resource-rich organisations. This may include accessing external expertise and support, if such a service is available.
- Postvention team members, managers, and team leaders should be offered training around topics such as suicide stigma, risk, and ‘contagion’. This should include strategies for supporting teams and individuals.
- Future researchers may wish to explore the impact of colleague suicide on those with pre-existing mental health conditions (such as military personnel with PTSD).
- Development and evaluation of postvention guidance that is informed by empirical evidence for specific professional groups is needed
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 30 August 2022).
- World Health Organisation. One in 100 Deaths Is by Suicide. Available online: https://www.who.int/news/item/17-06-2021-one-in-100-deaths-is-by-suicide (accessed on 30 August 2022).
- Spillane, A.; Matvienko-Sikar, K.; Larkin, C.; Corcoran, P.; Arensman, E. What are the physical and psychological health effects of suicide bereavement on family members? An observational and interview mixed-methods study in Ireland. BMJ Open 2018, 8, e019472. [Google Scholar] [CrossRef]
- Suicide Berveament UK. PABBS: Evidence-Based Suicide Bereavement Training 2019. Available online: https://suicidebereavementuk.com/ (accessed on 31 August 2022).
- Sveen, C.-A.; Walby, F.A. Suicide survivors’ mental health and grief reactions: A systematic review of controlled studies. Suicide Life-Threat. Behav. 2008, 38, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.L. Estimating the population of survivors of suicide: Seeking an evidence base. Suicide Life-Threat. Behav. 2011, 41, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Cerel, J.; Brown, M.M.; Maple, M.; Singleton, M.; Van de Venne, J.; Moore, M.; Flaherty, C. How many people are exposed to suicide? Not six. Suicide Life-Threat. Behav. 2019, 49, 529–534. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, S.; Flynn, S.; Shaw, J.; Smith, S.; McGale, B.; Hunt, I.M. Suicide bereavement in the UK: Descriptive findings from a national survey. Suicide Life-Threat. Behav. 2022. ahead of print. [Google Scholar] [CrossRef]
- McDonnell, S.; Nelson, P.A.; Leonard, S.; McGale, B.; Chew-Graham, C.A.; Kapur, N.; Shaw, J.; Smith, S.; Cordingley, L. Evaluation of the impact of the PABBS suicide bereavement training on clinicians’ knowledge and skills. Crisis 2020, 41, 351–358. [Google Scholar] [CrossRef]
- Pitman, A.; Osborn, D.; King, M.; Erlangsen, A. Effects of suicide bereavement on mental health and suicide risk. Lancet Psychiatr. 2014, 1, 86–94. [Google Scholar] [CrossRef]
- Pitman, A.L.; Osborn, D.P.; King, M.B.; Rantell, K. The stigma perceived by people bereaved by suicide and other sudden deaths: A cross-sectional UK study of 3432 bereaved adults. J. Psychosom. Res. 2016, 87, 22–29. [Google Scholar] [CrossRef]
- Swanson, S.A.; Colman, I. Association between exposure to suicide and suicidality outcomes in youth. Can. Med. Assoc. J. 2013, 185, 870–877. [Google Scholar] [CrossRef]
- Pitman, A.; Putri, A.K.; De Souza, T.; Stevenson, F.; King, M.; Osborn, D.; Morant, N. The impact of suicide bereavement on educational and occupational functioning: A qualitative study of 460 bereaved adults. Int. J. Environ. Res. Public Health 2018, 15, 643. [Google Scholar] [CrossRef] [Green Version]
- Hunt, Q.A.; Young, T.A.; Hertlein, K.M. The process of long-term suicide bereavement: Responsibility, familial support, and meaning making. Contemp. Fam. Ther. 2019, 41, 335–346. [Google Scholar] [CrossRef]
- Oexle, N.; Sheehan, L. Perceived social support and mental health after suicide loss. Crisis 2019, 41, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Owens, C.; Lambert, H.; Lloyd, K.; Donovan, J. Tales of biographical disintegration: How parents make sense of their sons’ suicides. Sociol. Health Illn. 2008, 30, 237–254. [Google Scholar] [CrossRef] [PubMed]
- Spillane, A.; Larkin, C.; Corcoran, P.; Matvienko-Sikar, K.; Riordan, F.; Arensman, E. Physical and psychosomatic health outcomes in people bereaved by suicide compared to people bereaved by other modes of death: A systematic review. BMC Public Health 2017, 17, 939. [Google Scholar] [CrossRef]
- Bartik, W.; Maple, M.; Edwards, H.; Kiernan, M. The psychological impact of losing a friend to suicide. Australas. Psychiatr. 2013, 21, 545–549. [Google Scholar] [CrossRef]
- Kim, J.E. Korean teachers’ bereavement experience following student suicide. Crisis 2019, 40, 287–293. [Google Scholar] [CrossRef]
- Causer, H. A Critical Exploration of Staff Experiences and Roles Following a Student Death by Suicide within Two United Kingdom Higher Education Institutions. Ph.D. Thesis, Worcester University, Worcester, UK, 2020. Available online: https://eprints.worc.ac.uk/10637/1/PhD%20Thesis%20-%20Hilary%20Causer.pdf (accessed on 26 July 2022).
- Causer, H.; Bradley, E.; Muse, K.; Smith, J. Bearing witness: A grounded theory of the experiences of staff at two United Kingdom Higher Education Institutions following a student death by suicide. PLoS ONE 2021, 16, e0251369. [Google Scholar] [CrossRef]
- Causer, H.; Muse, K.; Smith, J.; Bradley, E. What is the experience of practitioners in health, education or social care roles following a death by suicide? A qualitative research synthesis. Int. J. Environ. Res. Public Health 2019, 16, 3293. [Google Scholar] [CrossRef]
- Christianson, C.L.; Everall, R.D. Constructing bridges of support: School counsellors’ experiences of student suicide. Can. J. Couns. Psychother. 2008, 42, 209–221. [Google Scholar]
- Saini, P.; Chantler, K.; While, D.; Kapur, N. Do GPs want or need formal support following a patient suicide?: A mixed methods study. Fam. Pract. 2016, 33, 414–420. [Google Scholar] [CrossRef]
- ONS. Suicide by Occupation, England: 2011 to 2015 Analysis of Deaths from Suicide in Different Occupational Groups for People Aged 20 to 64 Years, Based on Deaths Registered in England between 2011 and 2015. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/suicidebyoccupation/england2011to2015/pdf (accessed on 16 October 2021).
- Andriessen, K. Can postvention be prevention? Crisis 2009, 30, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Manthey, T.; Kaess, M.; Brockmann, E.; Zimmermann, F.; Plener, P.L. Suicide postvention: What mental health professionals need to know. Z. Kinder Jugendpsychiatrie Psychother. 2017, 45, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Kinman, G.; Torry, R. Developing a suicide postvention framework for staff in primary healthcare. Occup. Med. 2021, 71, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Leaune, E.; Cuvillier, B.; Vieux, M.; Pacaut-Troncin, M.; Chalancon, B.; Perez, A.-F.; Haesebaert, J.; Chauliac, N.; Poulet, E.; Durif-Bruckert, C. The SUPPORT-S protocol study: A postvention program for professionals after patient or user suicide. Front. Psychol. 2020, 11, 805–816. [Google Scholar] [CrossRef]
- Hill, N. Evaluation of the Primary Care Navigator (PCN) Model for People Bereaved by Suicide in the Peel and Rockingham, Kwinana (PaRK) Region in WA.; Telethon Kids Institute: Nedlands, Australia, 2021. [Google Scholar]
- Lestienne, L.; Leaune, E.; Haesebaert, J.; Poulet, E.; Andriessen, K. An integrative systematic review of online resources and interventions for people bereaved by suicide. Prev. Med. 2021, 152, 106583. [Google Scholar] [CrossRef]
- Austin, C.; McGuinness, B. Breaking the Silence in the Workplace: A Guide for Employers on Responding to Suicide in the Workplace; Irish Hospice Foundation: Dublin, Ireland, 2012. [Google Scholar]
- Berkowitz, L.; McCauley, J.; Schuurman, D.L.; Jordan, J.R. Organizational postvention after suicide death. In Grief after Suicide: Understanding the Consequences and Caring for the Survivors; Jordan, J.R., McIntosh, J.L., Eds.; Routledge: New York, NY, USA, 2011; pp. 157–178. [Google Scholar]
- Marsh, I. Critiquing contemporary suicidology. In Critical Suicidology: Transforming Suicide Research and Prevention for the 21st Century; White, J., Marsh, I., Kral, M.J., Morris, J., Eds.; UBC Press: Vancouver, BC, Canada, 2016; pp. 15–30. [Google Scholar]
- White, J. What can critical suicidology do? Death Stud. 2017, 41, 472–480. [Google Scholar] [CrossRef]
- Gulliver, S.B.; Pennington, M.L.; Leto, F.; Cammarata, C.; Ostiguy, W.; Zavodny, C.; Kimbrel, N.A.; Flynn, E.J. In the wake of suicide: Developing guidelines for suicide postvention in fire service. Death Stud. 2016, 40, 121–128. [Google Scholar] [CrossRef]
- Marzetti, H.; Oaten, A.; Chandler, A.; Jordan, A. Self-inflicted. Deliberate. Death-intentioned. A critical policy analysis of UK suicide prevention policies 2009–2019. J. Public Ment. Health 2022, 21, 4–14. [Google Scholar] [CrossRef]
- Bantjes, J.; Swartz, L. The cultural turn in critical suicidology: What can we claim and what do we know? Death Stud. 2017, 41, 512–520. [Google Scholar] [CrossRef]
- Marsh, I. ‘Critical suicidology’: Toward an inclusive, inventive and collaborative (post) suicidology. Soc. Epis. Rev. Reply Collect. 2015, 4, 6–9. [Google Scholar]
- Dhollande, S.; Taylor, A.; Meyer, S.; Scott, M. Conducting integrative reviews: A guide for novice nursing researchers. J. Res. Nurs. 2021, 26, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Torraco, R.J. Writing integrative reviews of the literature: Methods and purposes. Int. J. Adult Vocat. Educ. Technol. 2016, 7, 62–70. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Chao, A.; Jang, M.; Minges, K.E.; Park, C. Methods for knowledge synthesis: An overview. Heart Lung 2014, 43, 453–461. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Noblit, G.; Hare, R. A meta-ethnographic approach. In Meta-Ethnography; SAGE: Newbury Park, CA, USA, 1988; Volume 11. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef]
- AGREE Next Steps Consortium. The AGREE II Instrument [Electronic Version]. Available online: http://www.agreetrust.org (accessed on 30 November 2021).
- Joanna BrIggs Institute. Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 30 November 2021).
- Hong, Q.; Pluye, P.; F‘abregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 10 February 2022).
- Protogerou, C.; Hagger, M.S. A checklist to assess the quality of survey studies in psychology. Method. Psychol. 2020, 3, 100031. [Google Scholar] [CrossRef]
- Bogle, C.L. The Impact of a Law Enforcement Suicide on Colleagues. Ph.D. Thesis, The George Washington University, Ann Arbor, MI, USA, 2018. Available online: https://www.proquest.com/dissertations-theses/impact-law-enforcement-suicide-on-colleagues/docview/2029929333/se-2?accountid=8630 (accessed on 2 November 2021).
- Carr, R.B. When a soldier commits suicide in Iraq: Impact on unit and caregivers. Psychiatry 2011, 74, 95–106. [Google Scholar] [CrossRef]
- Deheegher, J. Suicide of a Service Member: How to Organize Support for the Bereaved Service Members in the Emotional Aftermath. In Lowering Suicide Risk in Returning Troops: Wounds of War; Wiederhold, B.K., Ed.; Ios Press: Amsterdam, The Netherlands, 2008; pp. 149–161. [Google Scholar]
- Kleespies, P.M.; Van Orden, K.A.; Bongar, B.; Bridgeman, D.; Bufka, L.F.; Galper, D.I.; Hillbrand, M.; Yufit, R.I. Psychologist Suicide: Incidence, Impact, and Suggestions for Prevention, Intervention, and Postvention. Prof. Psychol. Res. Pract. 2011, 42, 244. [Google Scholar] [CrossRef]
- Lynn, C.W. When a coworker completes suicide. AAOHN J. 2008, 56, 459–469. [Google Scholar] [CrossRef]
- Małecka, K.A. “Have you heard about X?”: (Mis) management of mortality in academia. Death Stud. 2022, 46, 1678–1688. [Google Scholar] [CrossRef] [PubMed]
- Pak, K.; Ferreira, K.E.; Ghahramanlou-Holloway, M. Suicide postvention for the United States military: Literature review, conceptual model, and recommendations. Arch. Suicide Res. 2019, 23, 179–202. [Google Scholar] [CrossRef] [PubMed]
- Sever, M.; Ozdemir, S. How an academic’s death by suicide impacts coworkers and an organization. Death Stud. 2019, 46, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Yentis, S.M.; Shinde, S.; Plunkett, E.; Mortimore, A. Suicide amongst anaesthetists—An Association of Anaesthetists survey. Anaesthesia 2019, 74, 1365–1373. [Google Scholar] [CrossRef]
- VandePol, B.; Beyer, C. Leading a Company in the Aftermath of a Suicide Loss; CMFA Building Profits: Princeton, NJ, USA, 2019. [Google Scholar]
- Carson J Spencer Foundation; National Action Alliance for Suicide Prevention; American Association of Suicidology. A Manager’s Guide to Suicide Postvention in the Workplace: 10 Action Steps for Dealing with the Aftermath of Suicide; Carson J Spencer Foundation: Denver, CO, USA, 2013. [Google Scholar]
- Business in the Community. Crisis Management in the Event of a Suicide: A Postvention Toolkit for Employers; Samaritans: London, UK, 2017. [Google Scholar]
- Samaritans. Ambulance Service Employee Suicide: A Postvention Toolkit to Help Manage the Impact and Provide Support; Samaritans: Surrey, UK, 2021. [Google Scholar]
- Attride-Stirling, J. Thematic networks: An analytic tool for qualitative research. Qual. Res. 2001, 1, 385–405. [Google Scholar] [CrossRef]
- Mericle, B.P. When a colleague commits suicide. J. Psychosoc. Nurs. 1993, 31, 11–13. [Google Scholar] [CrossRef]
- Cerel, J.; Maple, M.; Van De Venne, J.; Brown, M.; Moore, M.; Flaherty, C. Suicide exposure in the population: Perceptions of impact and closeness. Suicide Life-Threat. Behav. 2017, 47, 696–708. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.; Kavanagh, M.; Russo, K. A qualitative systematic review of the bereavement process following suicide. OMEGA-J. Death Dying 2017, 74, 426–454. [Google Scholar] [CrossRef]
- Törnblom, A.W.; Werbart, A.; Rydelius, P.-A. Shame behind the masks: The parents’ perspective on their sons’ suicide. Arch. Suicide Res. 2013, 17, 242–261. [Google Scholar] [CrossRef]
- Zisook, S.; Iglewicz, A.; Avanzino, J.; Maglione, J.; Glorioso, D.; Zetumer, S.; Seay, K.; Vahia, I.; Young, I.; Lebowitz, B.; et al. Bereavement: Course, consequences, and care. Curr. Psychiatr. Rep. 2014, 16, 482. [Google Scholar] [CrossRef]
- Spiers, J.; Buszewicz, M.; Chew-Graham, C.; Gerada, C.; Kessler, D.; Leggett, N.; Manning, C.; Taylor, A.K.; Thornton, G.; Riley, R. Who cares for the clinicians? The mental health crisis in the GP workforce. Br. J. Gen. Pract. 2016, 66, 344–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, R.; Spiers, J.; Buszewicz, M.; Taylor, A.K.; Thornton, G.; Chew-Graham, C. What are the Sources of Stress and Distress for General Practitioners Working in England? A Qualitative Study. BMJ Open 2018, 8, e017361. [Google Scholar] [CrossRef] [PubMed]
- Bento, R.F. When the show must go on: Disenfranchised grief in organisations. J. Manag. Psychol. 1994, 9, 35–44. [Google Scholar] [CrossRef]
- Hochschild, A.R. The Managed Heart: Commercialization of Human Feeling; University California Press: Berkeley, CA, USA, 1983. [Google Scholar]
- Hochschild, A.R. The Managed Heart: Commercialization of Human Feeling; University California Press: Berkeley, CA, USA, 2010. [Google Scholar]
- Doka, K.J. Introduction. In Disenfranchised Grief: New Directions, Challenges, and Strategies for Practice; Doka, K.J., Ed.; Research Press: Champaign, IL, USA, 2002. [Google Scholar]
- Jacobsen, M.H.; Petersen, A. Introduction: Towards a sociology of grief—Historical, cultural and social explorations of grief as an emotion. In Exploring Grief: Toward a Sociology of Sorrow; Jacobsen, M.H., Petersen, A., Eds.; Routledge: London, UK, 2019. [Google Scholar]
- Grandey, A.A. Emotional regulation in the workplace: A new way to conceptualize emotional labor. J. Occup. Health Psychol. 2000, 5, 95–110. [Google Scholar] [CrossRef]
- Morris, J.A.; Feldman, D.C. The dimensions, antecedents, and consequences of emotional labor. Acad. Manag. Rev. 1996, 21, 986–1010. [Google Scholar] [CrossRef]
- Zapf, D.; Holz, M. On the positive and negative effects of emotion work in organizations. Eur. J. Work Organ. Psychol. 2006, 15, 1–28. [Google Scholar] [CrossRef]
- Pitimson, N. Work after death: An examination of the relationship between grief, emotional labour, and the lived experience of returning to work after bereavement. Sociol. Res. Online 2021, 26, 469–484. [Google Scholar] [CrossRef]
- Lattanzi-Licht, M. Grief and the workplace: Positive approaches. In Disenfranchised Grief: New Directions, Challenges, and Strategies for Practice; Doka, K.J., Ed.; Research Press: Champaign, IL, USA, 2002. [Google Scholar]
- Doka, K.J. Disenfranchised Grief. In Disenfranchised Grief: Recognizing Hidden Sorrow; Doka, K.J., Ed.; Lexington Books: Lanham, MD, USA, 1989. [Google Scholar]
- Chapple, A.; Ziebland, S.; Hawton, K. Taboo and the different death? Perceptions of those bereaved by suicide or other traumatic death. Sociol. Health Illn. 2015, 37, 610–625. [Google Scholar] [CrossRef]
- Eyetsemitan, F. Stifled grief in the workplace. Death Stud. 1998, 22, 469–479. [Google Scholar] [CrossRef]
- Hazen, M.A. Grief and the workplace. Acad. Manag. Perspect. 2008, 22, 78–86. [Google Scholar] [CrossRef]
- Peticca-Harris, A. Managing compassionately? Managerial narratives about grief and compassion. Hum. Relat. 2019, 72, 588–612. [Google Scholar] [CrossRef]
- Tehan, M.; Thompson, N. Loss and grief in the workplace: The challenge of leadership. OMEGA-J. Death Dying 2013, 66, 265–280. [Google Scholar] [CrossRef] [PubMed]
- Tsui, A.S. Presidential address—On compassion in scholarship: Why should we care? Acad. Manag. Rev. 2013, 38, 176–180. [Google Scholar] [CrossRef]
- Kanov, J.M.; Maitlis, S.; Worline, M.C.; Dutton, J.E.; Forst, P.J.; Lilius, J.M. Compassion in organizational life. Am. Behav. Sci. 2004, 47, 808–827. [Google Scholar] [CrossRef]
- Dutton, J.E.; Workman, K.M.; Hardin, A.E. Compassion at work. Ann. Rev. Organ. Psychol. 2014, 1, 277–304. [Google Scholar] [CrossRef]
- Granek, L. Mourning sickness: The politicizations of grief. Rev. Gen. Psychol. 2014, 18, 61–68. [Google Scholar] [CrossRef]
- Gabriel, Y. The caring leader: What followers expect of their leaders and why? Leadership 2015, 11, 316–334. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Reported on the experiences of people following a colleague suicide | Reported experiences following the suicide of a client, patient, service-user, student, family member, or anyone outside of work |
| Reported responses to an incident of, or set out guidance or policy in response to, the suicide of an employee or colleague | Reported only on prevention or intervention of colleague or employee suicide or on causes of suicidal ideation or behaviour |
| Qualitative, quantitative, or mixed methods research studies, reviewed original data, reported a first-person account, case study, or opinion piece | |
| Reported or evaluated the implementation of postvention guidance or support programmes for staff | |
| Published in the English language | |
| Contributed usefully to addressing the review problem |
| Databases | Grey Literature Databases | Search Terms |
|---|---|---|
| Medline | BASE | suicide |
| PsycINFO | Google Scholar | AND |
| CINAHL | British Library | [colleague* OR co-worker* OR staff OR personnel OR employee OR workplace] |
| Embase | Ethos | AND |
| Web of Science | ZETOC | [postvention OR guidance OR guidelines OR support* OR therap* OR response OR policy OR evaluat*] |
| ProQuest | AMC Digital Library | |
| PubMed | Cochrane Library | |
| Scopus | IEEE Xplore | |
| NHS Evidence | ||
| Social Care Online | ||
| Social Science Research Network | ||
| United Kingdom Department of Health | ||
| GreyLit.org |
| Author & Date | Location | Type of Study | Study Aim/Research Question | Setting and Participant Details | Data Collection | Data Analysis | Results/Findings |
|---|---|---|---|---|---|---|---|
| Bogle, C.L. (2018) [51] | US | Qualitative study | Exploring the lived experiences of law enforcement officers concerning colleague suicide and the impact a suicide has on a law enforcement agency/department. | Police Department Law enforcement officers n = 11 Male = 7 African American = 10 Caucasian = 1 | Semi-structured interviews | Thematic analysis | Four major themes: (1) Uniqueness of the law enforcement community (2) Lack of available resources regarding mental health services (3) Reactive response to the suicide event and (4) The necessity for consistent mental health services. |
| Carr, R.B. (2011) [52] | Iraq | First-person account | Reporting the author’s first-hand experience of supporting a US army unit in Iraq after a soldier suicide. | US Army Psychiatrist in support role. n = 1 Male | N/A | N/A | Acute effects of suicide and effects over the subsequent four months. |
| Deheeger, J. (2008) [53] | Belgium | Report | Reporting the incidence, impact and postvention response following a colleague suicide in the Belgian Defence. | Belgian Armed Forces No Participants | N/A | N/A | Grief, guilt, and feelings of blame Fear of social stigma The service member’s need for help Postvention trajectory of care: Pre-incident education Post-incident procedure of psychosocial care for victims Structure of the postvention crisis intervention procedure. |
| Gulliver et al. (2016) [36] | US | Evaluation | To subject the New York City Fire Department (FDNY) standard operating procedure (SOP) to an iterative process to develop a national guideline for suicide postvention. | US Fire Department Initial Expert Review Group: n = 5 Female = 1 All = at least two years exp in fire service | Expert review group and 90-min focus groups, video recorded. | Data were taken at face value and used to inform the development of the guidance. | The expert review group discussed the need for more depth in the FDNY SOP as well as adding more information and procedures around responding to family and department members. Focus groups suggested making the SOP more operational and directive and breaking it up into two documents: (1) educational material (to be shortened into a pamphlet) and (2) the SOP. They also suggested calling it a guideline rather than an SOP. Feedback was incorporated into the final version of the SOP guidelines. |
| Six focus groups: n = 61 75% male Mean age = 47 years 22.9% Hispanic 9.8% African American 72/1% Caucasian | Six focus groups in three test cities reviewed the SOP manual and provided feedback on barriers to implementation | ||||||
| Kleespies et al. (2011) [54] | US | Literature review, interviews, and review of case reports | To investigate the incidence of psychologist suicide and its impact on colleagues, students or interns, patients or clients and the profession. | US Psychologists. Reports that 14 cases of suicide were identified but does not clarify the number of participants interviewed nor participant details. | Interviews | Not reported | Postvention efforts to address the needs of all survivors are needed. Professionals can help colleagues by clarifying the wishes of the deceased for closing their practice. The extent to which colleagues may experience a complicated bereavement and need support is undetermined. |
| Lynn, C.W. (2008) [55] | US | Case study | To explore the role of the occupational health nurse in supporting staff following the death co-worker suicide. | US Hospital Health workers | Case Study | N/A | Occupational health nurses can be the guiding force for first-line nurses after a suicide. Preparation begins with recognising that suicide is a genuine health emergency and requires the same planning as any other safety-related issue. Education and resources through EAP can prevent suicide and facilitate postvention. |
| Malecka, K.A. (2020) [56] | Poland | Qualitative multiple case study | Exploring how four Polish universities managed suicides. Presenting the lived experiences of participants holistically. | Higher Education Institutions Colleagues of deceased HE workers. n = 7 Academic staff = 5 Administrative staff = 2 Polish = 5 ‘Of foreign descent’ = 2 | Semi-structured interviews | Thematic data explication | Eight thematic areas: Notification of the deaths Personal responses to the deaths Institutional & managerial responses Professional help Formal and informal acknowledgements Administrative matters The reality of organisationally sponsored loss of education Mortality (mis)management: additional loss stories |
| Pak et al. (2019) [57] | US | Literature review | Providing a summary of the postvention literature with special emphasis placed on the military organisation; proposing a conceptual model for understanding Military-Unit Suicide Survivorship; and highlighting postvention strategies within the DoD. | US Army No participants | Qualitative, narrative, and evaluative review. Methods of data collection and analysis are not reported. | Proposes a conceptual model for military unit suicide survivorship based on the literature. Proposes postvention strategies and recommendations. Makes research, clinical, and policy recommendations. | |
| Sever & Ozdemir (2019) [58] | Turkey | Qualitative study | Exploring the impact of a staff member’s suicide on the organisation, faculty, and administration in a Turkish academic institution. Highlighting the influence of culture and belief in responses to suicide, where many people are Sunni Muslims, a belief system that strongly disapproves of suicide. | Higher Education Institution n = 7 Male = 4 Colleagues n = 5 Administrators n = 2 | Open questions provided by email | Interpretative phenomenological design | Two categories, seven themes Personal: Shock Questioning and feeling responsible Stigmatisation or asking for forgiveness Personal lessons Regrets Organisational: Solidarity and administrative support What needs to be changed |
| Yentis, Shinde, Plunkett & Mortimore (2019) [59] | UK | Survey | A working party to review anaesthetist suicide and provide guidance for anaesthetists, departments, and employers. | Survey sent to anaesthetists working in the UK. n = 3638 | Anonymous online survey | Descriptive statistics | Most respondents were unaware of the existence of policies on mental illness, addiction, or suicide. 1916 cases of suicide were reported by 1397 respondents. A third of respondents who reported a suicide had experienced more than one case. Most reported suicide in the last 10 years involving anaesthetic drugs. Deficiencies were noted in support and how deaths were handled, although examples of good support were also described. |
| Authors, Date & Title | Location | Type of Article | Setting | Aims | Evidence Base | Guidance/ Recommendations |
|---|---|---|---|---|---|---|
| Vanderpol & Beyer (2019) [60] | US | Guidance | Construction industry | To share perspectives, strategies, resources, and tools to help contractors respond appropriately to a colleague suicide. | Draws on existing knowledge and guidance. No reference list or evidence base cited. | Defines postvention. Presents key points for critical incident management and strategies to support colleagues following a suicide. Q&A with the authors. Signposts to support websites and articles. |
| Leading a company in the aftermath of a suicide loss | ||||||
| Berkowitz et al. (2014) [33] | US | Guidance (book chapter) | Organisations | Not stated | Draws on existing literature. | Concludes: Organisational postvention is recommended, but guidance is sparse. Various factors complicate the work. Postvention should be an evolving process that attends to the guidelines and principles in this chapter. Longitudinal and comparative studies are needed. Qualitative studies are needed to understand need and inform postvention interventions. |
| Organizational postvention after suicide death | ||||||
| Austin & McGuinness (2012) [32] Console & The Irish Hospice Foundation | Ireland | Guidance | The workplace | To help organisations increase their understanding and confidence in responding to workplace suicide. | Presents case studies but does not cite sources, so they could be fictionalised. Cites three references. | Provides guidance for employee suicide on-site and off-site, when an employee is affected by the suicide of someone close and when a former employee dies by suicide. Guidance also provided for developing a bereavement policy for dealing with suicide. Signposts to suicide support organisations. |
| Breaking the silence in the workplace: A guide for employers on responding to suicide in the workplace | ||||||
| The workplace postvention taskforce of the American Association of Suicidology & the workplace taskforce of the national alliance for suicide prevention. In partnership with the Carson J Spenser Foundation & Crisis Care Network. (2013) [61] | US | Guidance | The workplace | Not stated | Cites a source for their definition of postvention. Cites the Individual Differences Models (Mancini & Bonanna, 2009), the ACT Model (VandePol, 2003) and the CDC definitions of ‘suicide’ ‘suicide attempt’ and ‘suicidal ideation’. However, no evidence base cited to underpin the guidance. | Defines postvention. Presents a three-phase (acute, recovery, reconstructing) approach to delivery. Provides sample comms memos; signposts to resources; provides a decision-making flow-chart. |
| A manager’s guide to suicide postvention in the workplace: Ten action steps for dealing with the aftermath of a suicide. | ||||||
| Kinman & Torry (2020) [28] Supporting Occupational Health and Wellbeing Professionals & The Louise Tebboth Foundation. | UK | Guidance | Primary healthcare | Guidelines intended to inform a flexible crisis management strategy that provides information and support to primary care practices at different stages following a colleague suicide. May also be useful to similar small organisations. | In-depth interviews with GPs who have experienced a co-worker suicide, as well as contributions from other stakeholders. Interviews analysed by two researchers independently. A grounded theory approach was used where themes were identified and expanded until saturation. Full list of references included. | Presents postvention guidance for the first day, first week, first month, and longer term. Guidance is presented alongside participant quotes. Presents an Actions Needed summary table. Signposts to other resources. |
| Responding to the death by suicide of a colleague in primary healthcare: A postvention framework | ||||||
| Business in the Community; The Prince’s Responsible Business Network; Public Health England; Samaritans (2017). [62] | UK | Guidance | The workplace | Toolkit to help organisations consider the issues that arise from workplace suicide; mitigate the impact of suicide; design a relevant postvention protocol. | Includes case studies from named organisations but does not cite these as underpinning evidence. No evidence base or references included. | Presents chronological guidance: Be prepared When suicide happens Grieving, post-traumatic phase Legacy phase Reflection time Includes signposts to resources and case studies. |
| Crisis management in the event of a suicide: A postvention toolkit for employers. | ||||||
| Samaritans & Association of Ambulance Chief Executives (2021). [63] | UK | Guidance | Ambulance service | To help ambulance services, particularly leaders in HR and frontline managers, manage the impact of an employee suicide or attempted suicide on colleagues. | Cites six references that explore: mental health problems among UK ambulance workers; paramedic perceptions of distress, stigma, and utilisation of support services; mental health in the ambulance service; effects of exposure to self-harm on social media study; effects of educative suicide prevention websites; contagion. | Presents chronological guidance: Be prepared Communicating after a suicide When suicide happens Grieving, post-traumatic phase Legacy phase Reflection time Further information and resources. |
| Ambulance service employee suicide: A postvention toolkit to help manage the impact and provide support. |
| Organising Themes | Global Themes | Unifying Global Theme |
|---|---|---|
| Suicide loss in the workplace | Impact of the loss of a colleague to suicide | After a colleague suicide |
| Professional identities and workplace roles | ||
| Perceptions of professional uniqueness in bereavement | ||
| Professional unpreparedness, abandonment, and silencing | ||
| Individualised responses | Postvention following a colleague suicide | |
| The dual function of stigma | ||
| Complex pressure on managers |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Causer, H.; Spiers, J.; Efstathiou, N.; Aston, S.; Chew-Graham, C.A.; Gopfert, A.; Grayling, K.; Maben, J.; van Hove, M.; Riley, R. The Impact of Colleague Suicide and the Current State of Postvention Guidance for Affected Co-Workers: A Critical Integrative Review. Int. J. Environ. Res. Public Health 2022, 19, 11565. https://doi.org/10.3390/ijerph191811565
Causer H, Spiers J, Efstathiou N, Aston S, Chew-Graham CA, Gopfert A, Grayling K, Maben J, van Hove M, Riley R. The Impact of Colleague Suicide and the Current State of Postvention Guidance for Affected Co-Workers: A Critical Integrative Review. International Journal of Environmental Research and Public Health. 2022; 19(18):11565. https://doi.org/10.3390/ijerph191811565
Chicago/Turabian StyleCauser, Hilary, Johanna Spiers, Nikolaos Efstathiou, Stephanie Aston, Carolyn A. Chew-Graham, Anya Gopfert, Kathryn Grayling, Jill Maben, Maria van Hove, and Ruth Riley. 2022. "The Impact of Colleague Suicide and the Current State of Postvention Guidance for Affected Co-Workers: A Critical Integrative Review" International Journal of Environmental Research and Public Health 19, no. 18: 11565. https://doi.org/10.3390/ijerph191811565
APA StyleCauser, H., Spiers, J., Efstathiou, N., Aston, S., Chew-Graham, C. A., Gopfert, A., Grayling, K., Maben, J., van Hove, M., & Riley, R. (2022). The Impact of Colleague Suicide and the Current State of Postvention Guidance for Affected Co-Workers: A Critical Integrative Review. International Journal of Environmental Research and Public Health, 19(18), 11565. https://doi.org/10.3390/ijerph191811565