


Relationship between the Duration of Urban Nature and a Lower Waist-Hip Ratio
 , and
, and 
Abstract
:1. Introduction
1.1. Obesity and Human Health
1.2. Urban Nature and Obesity
1.3. Critical Knowledge Gap: Doses and Demographics
- RQ.1. To what extent do the participants’ demographics and doses of urban nature (including distance, duration, and frequency) predict the WHR?
- RQ.2. To what extent do the participants’ demographics and doses of urban nature (including distance, duration, and frequency) predict odds of high-risk WHR?
2. Methods
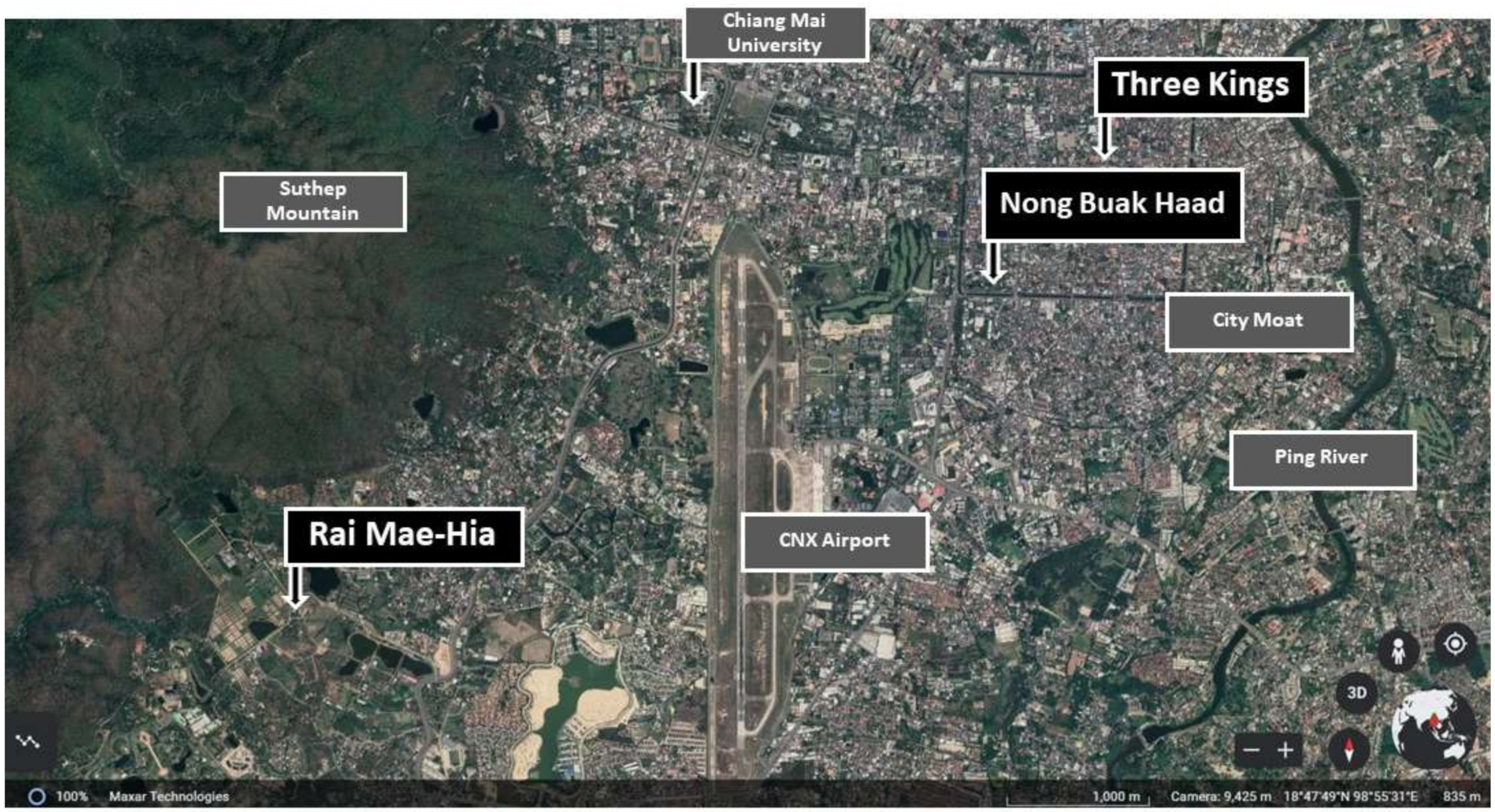
2.1. Study Site Selection
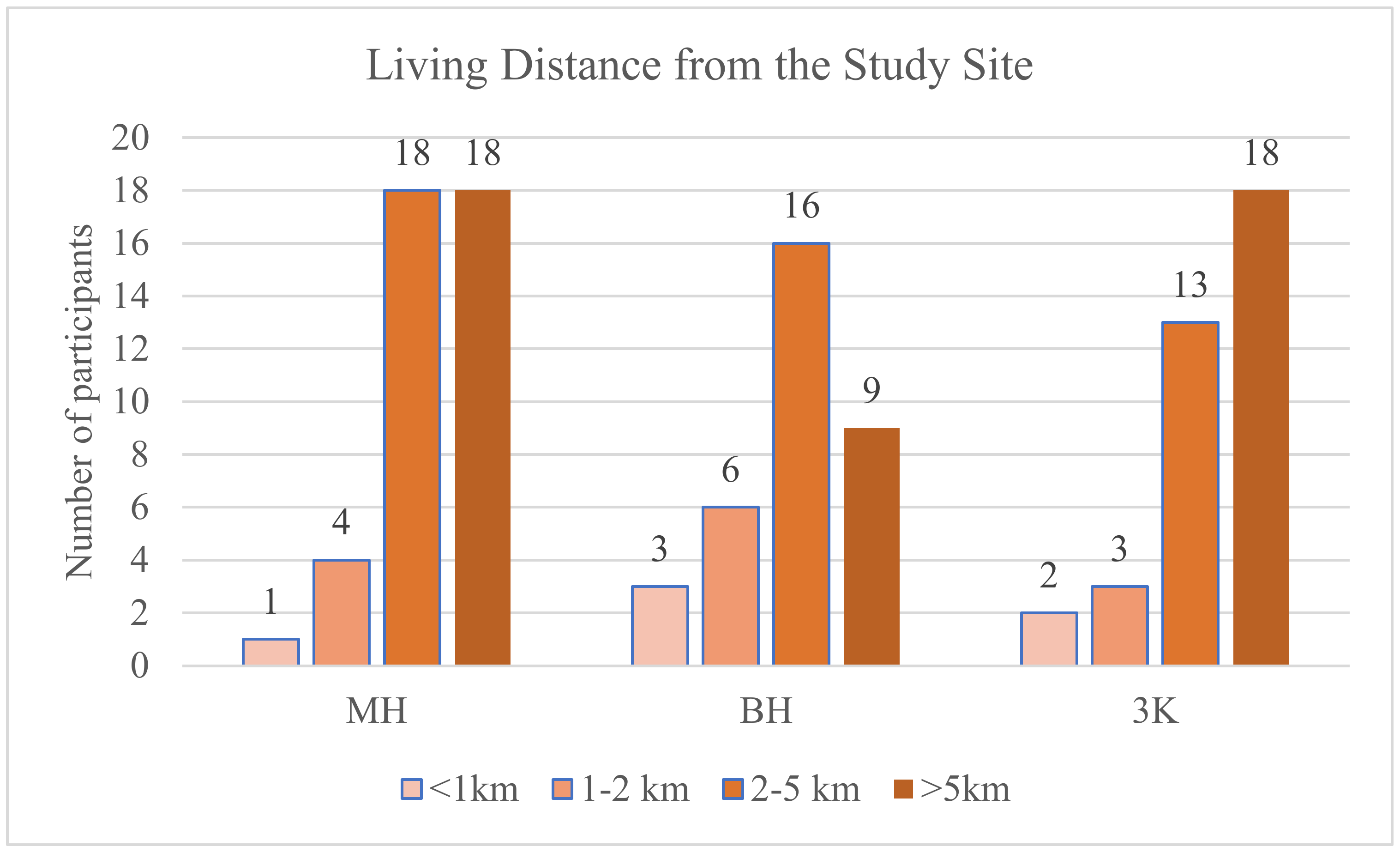
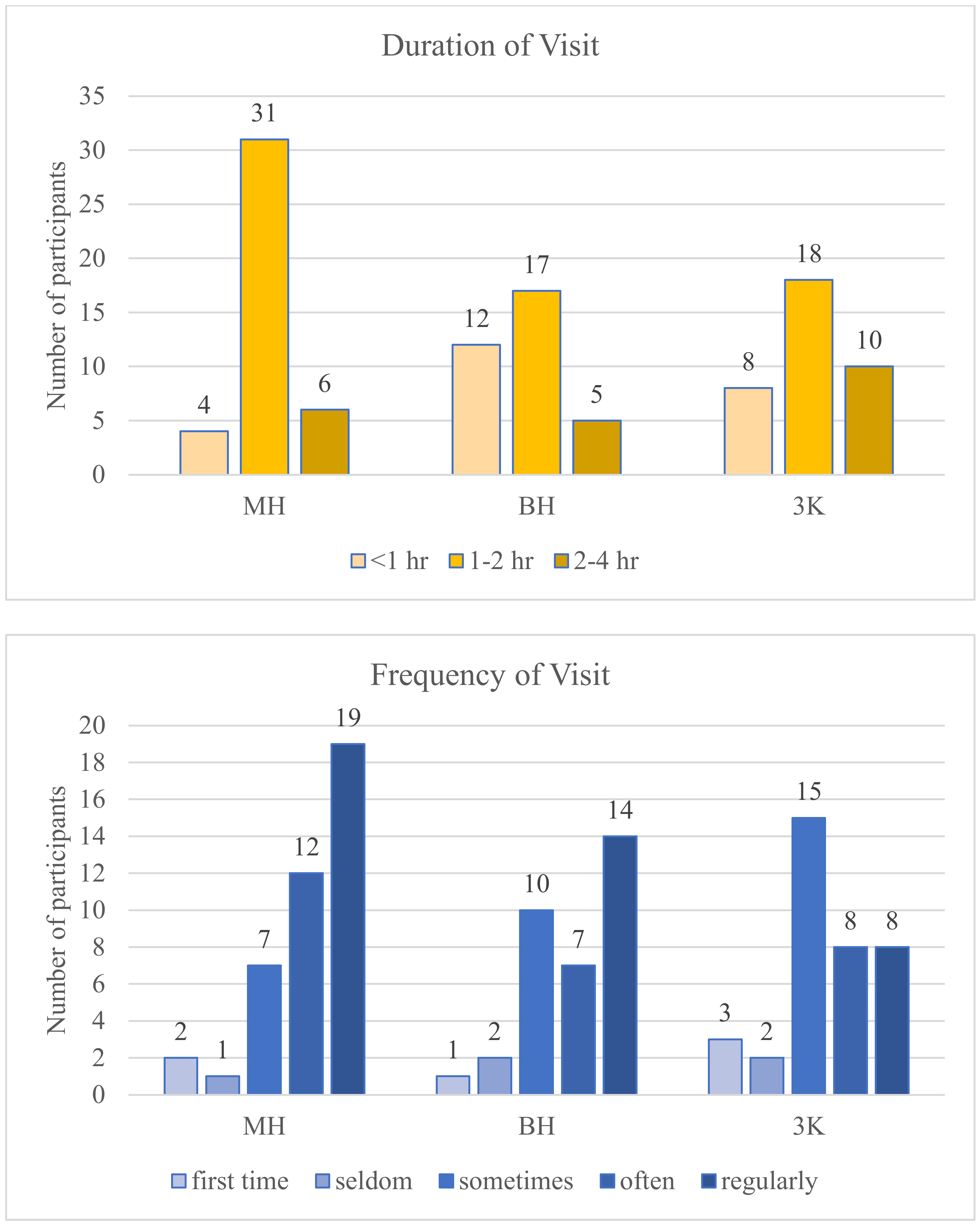
2.2. Participants and Recruitment
2.3. Survey Questions
2.4. Statistical Analysis
3. Results
3.1. To What Extent Do Obesity Measurements Agree?
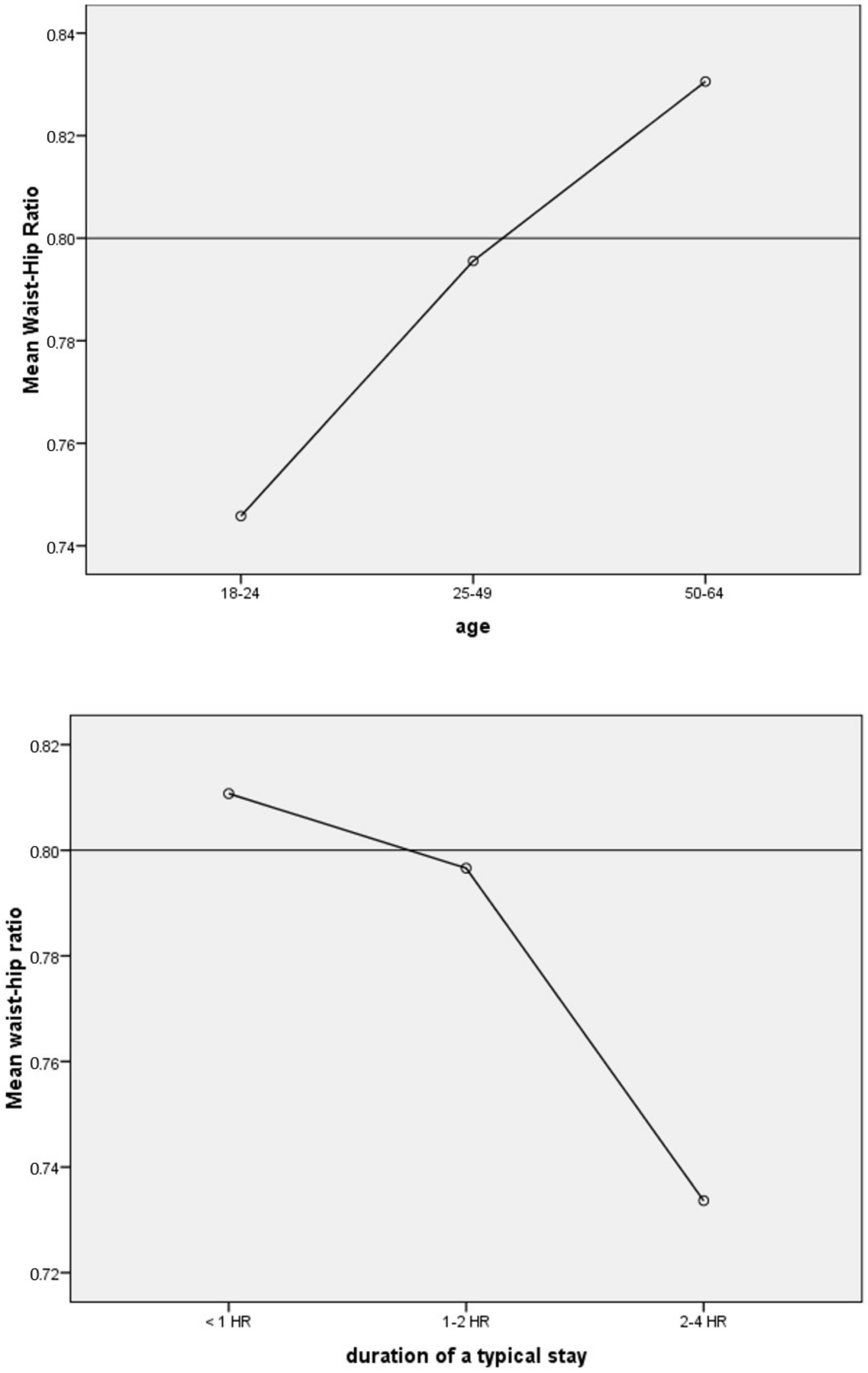
3.2. Doses, Demographics, and WHR
3.3. Doses, Demographics, and Odds of High-Risk WHR
4. Discussion
4.1. Key Findings
4.2. Contribution to the Field
4.3. Recommendations for Practitioners
4.4. Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Teerawattananon, Y.; Luz, A. Obesity in Thailand and its Economic Cost Estimation; Asian Development Bank Institute: Bangkok, Thailand, 2017. [Google Scholar]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, E.; Wright, E.; Kushner, B. In young adults with COVID-19, obesity is associated with adverse outcomes. West. J. Emerg. Med. 2020, 21, 752. [Google Scholar] [CrossRef]
- Dempsey, S.; Lyons, S.; Nolan, A. Urban green space and obesity in older adults: Evidence from Ireland. SSM-Popul. Health 2018, 4, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Mears, M.; Brindley, P.; Baxter, I.; Maheswaran, R.; Jorgensen, A. Neighbourhood greenspace influences on childhood obesity in Sheffield, UK. Pediatric Obes. 2020, 15, e12629. [Google Scholar] [CrossRef]
- De la Fuente, F.; Saldías, M.A.; Cubillos, C.; Mery, G.; Carvajal, D.; Bowen, M.; Bertoglia, M.P. Green space exposure association with type 2 diabetes mellitus, physical activity, and obesity: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 97. [Google Scholar]
- Sullivan, W.C.; Frumkin, H.; Jackson, R.J.; Chang, C.-Y. Gaia meets Asclepius: Creating healthy places. Landsc. Urban Plan. 2014, 127, 182–184. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 27 January 2022).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Prentice, A.M. The emerging epidemic of obesity in developing countries. Int. J. Epidemiol. 2006, 35, 93–99. [Google Scholar] [CrossRef]
- Kitzinger, H.; Karle, B. The epidemiology of obesity. Eur. Surg. 2013, 45, 80–82. [Google Scholar] [CrossRef]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef]
- Smith, K.B.; Smith, M.S. Obesity statistics. Prim. Care Clin. Off. Pract. 2016, 43, 121–135. [Google Scholar] [CrossRef]
- Lobstein, T.; Jackson-Leach, R. Planning for the worst: Estimates of obesity and comorbidities in school-age children in 2025. Pediatric Obes. 2016, 11, 321–325. [Google Scholar] [CrossRef]
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 21 July 2022).
- Finkelstein, E.A.; Strombotne, K.L. The economics of obesity. Am. J. Clin. Nutr. 2010, 91, 1520S–1524S. [Google Scholar] [CrossRef] [PubMed]
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N. Relationships between changes in self-reported physical activity, sedentary behaviour and health during the coronavirus (COVID-19) pandemic in France and Switzerland. J. Sports Sci. 2021, 39, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Dominski, F.H.; Brandt, R. Do the benefits of exercise in indoor and outdoor environments during the COVID-19 pandemic outweigh the risks of infection? Sport Sci. Health 2020, 16, 583–588. [Google Scholar] [CrossRef]
- Mogaji, E.; Adekunle, I.; Aririguzoh, S.; Oginni, A. Dealing with impact of COVID-19 on transportation in a developing country: Insights and policy recommendations. Transp. Policy 2021, 116, 304–314. [Google Scholar] [CrossRef]
- Kyrou, I.; Tsigos, C. Chronic stress, visceral obesity and gonadal dysfunction. Hormones 2008, 7, 287–293. [Google Scholar] [CrossRef]
- McSharry, D.; Malhotra, A. Potential influences of obstructive sleep apnea and obesity on COVID-19 severity. J. Clin. Sleep Med. 2020, 16, 1645. [Google Scholar] [CrossRef]
- Huang, W.-Z.; Yang, B.-Y.; Yu, H.-Y.; Bloom, M.S.; Markevych, I.; Heinrich, J.; Knibbs, L.D.; Leskinen, A.; Dharmage, S.C.; Jalaludin, B. Association between community greenness and obesity in urban-dwelling Chinese adults. Sci. Total Environ. 2020, 702, 135040. [Google Scholar] [CrossRef]
- Villeneuve, P.J.; Jerrett, M.; Su, J.G.; Weichenthal, S.; Sandler, D.P. Association of residential greenness with obesity and physical activity in a US cohort of women. Environ. Res. 2018, 160, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Miralles-Guasch, C.; Dopico, J.; Delclòs-Alió, X.; Knobel, P.; Marquet, O.; Maneja-Zaragoza, R.; Schipperijn, J.; Vich, G. Natural landscape, infrastructure, and health: The physical activity implications of urban green space composition among the elderly. Int. J. Environ. Res. Public Health 2019, 16, 3986. [Google Scholar] [CrossRef]
- Richardson, E.A.; Pearce, J.; Mitchell, R.; Kingham, S. Role of physical activity in the relationship between urban green space and health. Public Health 2013, 127, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Oka, M. Toward designing an environment to promote physical activity. Landsc. J. 2011, 30, 280–298. [Google Scholar] [CrossRef]
- Lu, Y. The association of urban greenness and walking behavior: Using google street view and deep learning techniques to estimate residents’ exposure to urban greenness. Int. J. Environ. Res. Public Health 2018, 15, 1576. [Google Scholar] [CrossRef]
- Adhikari, B.; Delgado-Ron, J.A.; Van den Bosch, M.; Dummer, T.; Hong, A.; Sandhu, J.; Demlow, E.; Hu, Y.; Frank, L.D. Community design and hypertension: Walkability and park access relationships with cardiovascular health. Int. J. Hyg. Environ. Health 2021, 237, 113820. [Google Scholar] [CrossRef]
- Groenewegen, P.P.; Van den Berg, A.E.; De Vries, S.; Verheij, R.A. Vitamin G: Effects of green space on health, well-being, and social safety. BMC Public Health 2006, 6, 149. [Google Scholar] [CrossRef]
- Hong, A.; Sallis, J.F.; King, A.C.; Conway, T.L.; Saelens, B.; Cain, K.L.; Fox, E.H.; Frank, L.D. Linking green space to neighborhood social capital in older adults: The role of perceived safety. Soc. Sci. Med. 2018, 207, 38–45. [Google Scholar] [CrossRef]
- Knobel, P.; Maneja, R.; Bartoll, X.; Alonso, L.; Bauwelinck, M.; Valentin, A.; Zijlema, W.; Borrell, C.; Nieuwenhuijsen, M.; Dadvand, P. Quality of urban green spaces influences residents’ use of these spaces, physical activity, and overweight/obesity. Environ. Pollut. 2021, 271, 116393. [Google Scholar] [CrossRef]
- Vitaliano, P.P.; Scanlan, J.M.; Zhang, J.; Savage, M.V.; Hirsch, I.B.; Siegler, I.C. A path model of chronic stress, the metabolic syndrome, and coronary heart disease. Psychosom. Med. 2002, 64, 418–435. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, D.F.; Fuller, R.A.; Bush, R.; Lin, B.B.; Gaston, K.J. The health benefits of urban nature: How much do we need? BioScience 2015, 65, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Sullivan, W.C. Impact of views to school landscapes on recovery from stress and mental fatigue. Landsc. Urban Plan. 2016, 148, 149–158. [Google Scholar] [CrossRef]
- Jiang, B.; Chang, C.-Y.; Sullivan, W.C. A dose of nature: Tree cover, stress reduction, and gender differences. Landsc. Urban Plan. 2014, 132, 26–36. [Google Scholar] [CrossRef]
- Jiang, B.; Li, D.; Larsen, L.; Sullivan, W.C. A Dose-Response Curve Describing the Relationship Between Urban Tree Cover Density and Self-Reported Stress Recovery. Environ. Behav. 2016, 48, 607–629. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984; p. 460. [Google Scholar]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef]
- Yaipimol, E.; Suppakittpaisarn, P.; Charoenlertthanakit, N.; Wanitchayapaisit, C.; Surinseng, V. Is 1-Minute of Nature Enough? Durations of Nature during Walking and Attention Restoration. Int. J. Build. Urban Inter. Landsc. Technol. 2022, 19, 51–62. [Google Scholar] [CrossRef]
- Hunter, M.R.; Gillespie, B.W.; Chen, S.Y.-P. Urban nature experiences reduce stress in the context of daily life based on salivary biomarkers. Front. Psychol. 2019, 10, 722. [Google Scholar] [CrossRef]
- Department of Health & Human Services. Physical Activity Guideline for Americans; Department of Health & Human Services: Washington, DC, USA, 2019; p. 118. [Google Scholar]
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2008; p. 47. [Google Scholar]
- Jiang, B.; Mak, C.N.S.; Larsen, L.; Zhong, H. Minimizing the gender difference in perceived safety: Comparing the effects of urban back alley interventions. J. Environ. Psychol. 2017, 51, 117–131. [Google Scholar] [CrossRef]
- Derby, C.A.; Zilber, S.; Brambilla, D.; Morales, K.H.; McKinlay, J.B. Body mass index, waist circumference and waist to hip ratio and change in sex steroid hormones: The Massachusetts Male Ageing Study. Clin. Endocrinol. 2006, 65, 125–131. [Google Scholar] [CrossRef]
- Aekplakorn, W.; Kosulwat, V.; Suriyawongpaisal, P. Obesity indices and cardiovascular risk factors in Thai adults. Int. J. Obes. 2006, 30, 1782–1790. [Google Scholar] [CrossRef]
- Aekplakorn, W.; Hogan, M.C.; Chongsuvivatwong, V.; Tatsanavivat, P.; Chariyalertsak, S.; Boonthum, A.; Tiptaradol, S.; Lim, S.S. Trends in obesity and associations with education and urban or rural residence in Thailand. Obesity 2007, 15, 3113–3121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahti-Koski, M.; Harald, K.; Männistö, S.; Laatikainen, T.; Jousilahti, P. Fifteen-year changes in body mass index and waist circumference in Finnish adults. Eur. J. Prev. Cardiol. 2007, 14, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Mokdad, A.H.; Giles, W.H. Trends in waist circumference among US adults. Obes. Res. 2003, 11, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Shimokata, H.; Tobin, J.D.; Muller, D.C.; Elahi, D.; Coon, P.J.; Andres, R. Studies in the distribution of body fat: I. Effects of age, sex, and obesity. J. Gerontol. 1989, 44, M66–M73. [Google Scholar] [CrossRef] [PubMed]
- Lourdes, K.T.; Gibbins, C.N.; Hamel, P.; Sanusi, R.; Azhar, B.; Lechner, A.M. A review of urban ecosystem services research in Southeast Asia. Land 2021, 10, 40. [Google Scholar] [CrossRef]
- Ji, L.-J.; Peng, K.; Nisbett, R.E. Culture, control, and perception of relationships in the environment. J. Personal. Soc. Psychol. 2000, 78, 943. [Google Scholar] [CrossRef]
- Sasidharan, V.; And, F.W.; Godbey, G. Cultural differences in urban recreation patterns: An examination of park usage and activity participation across six population subgroups. Manag. Leis. 2005, 10, 19–38. [Google Scholar] [CrossRef]
- Williams, R.; Periasamy, M. Genetic and environmental factors contributing to visceral adiposity in Asian populations. Endocrinol. Metab. 2020, 35, 681. [Google Scholar] [CrossRef]
- Diaz, V.; Mainous, A.; Baker, R.; Carnemolla, M.; Majeed, A. How does ethnicity affect the association between obesity and diabetes? Diabet. Med. 2007, 24, 1199–1204. [Google Scholar] [CrossRef]
- Huxley, R.; James, W.; Barzi, F.; Patel, J.; Lear, S.; Suriyawongpaisal, P.; Janus, E.; Caterson, I.; Zimmet, P.; Prabhakaran, D. Ethnic comparisons of the cross-sectional relationships between measures of body size with diabetes and hypertension. Obes. Rev. 2008, 9, 53–61. [Google Scholar] [CrossRef]
- Martínez-Hernández, A.; Enriquez, L.; Moreno-Moreno, M.J.; Marti, A. Genetics of obesity. Public Health Nutr. 2007, 10, 1138–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaron, D.G.; Stanford, F.C. Medicine, structural racism, and systems. Soc. Sci. Med. 2022, 298, 114856. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.N.; Kerr, J.; Young, J.L. Associations between obesity, obesogenic environments, and structural racism vary by county-level racial composition. Int. J. Environ. Res. Public Health 2019, 16, 861. [Google Scholar] [CrossRef]
- Aaron, D.G.; Stanford, F. Is obesity a manifestation of systemic racism? A ten-point strategy for study and intervention. J. Intern. Med. 2021, 290, 416–420. [Google Scholar] [CrossRef]
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Draper, J.; Kamnuansilpa, P. The Thai Lao question: The reappearance of Thailand’s ethnic Lao community and related policy questions. Asian Ethn. 2018, 19, 81–105. [Google Scholar] [CrossRef]
- Shivaniphat, P.; Ninlawanna, R. Linguistic Strategies for Communicating Otherness’s Ideology in the Ethnic Discourse [in TH]. J. Humanit. Soc. Sci. Nakhon Phanom Univ. 2021, 11, 261–271. [Google Scholar]
- Chuthap, W. Multicultural Identity of Rural Thai Society in Wan Kaew Youth Literature Award [in TH]. J. Humanit. Soc. Sci. Suratthani Rajabhat Univ. 2021, 13, 1–15. [Google Scholar]
- Glassman, J. Class, race, and uneven development in Thailand. In Routledge Handbook of Contemporary Thailand; Routledge: London, UK, 2019; pp. 305–317. [Google Scholar]
- Rackett, T. Buddhist Fury: Religion and Violence in Southern Thailand. J. Relig. Violence 2014, 2, 484–498. [Google Scholar] [CrossRef]
- Scupin, R.; Joll, C.M. Buddhist–Muslim Dynamics in Siam/Thailand. In Buddhist-Muslim Relations in A Theravada World; Springer: Berlin/Heidelberg, Germany, 2020; pp. 101–135. [Google Scholar]
- Hongladarom, K. Competing discourses on hilltribes: Media representation of ethnic minorities in Thailand. In Proceedings of the 7th International Conference on Thai Studies, Amsterdam, The Netherlands, 4–8 July 1999; pp. 4–8. [Google Scholar]
- Suppakittpaisarn, P.; Surinseng, V.; Wanitchayapaisit, C.; Yaipimol, E.; Xu, Q. Healthy Ecosystem Services and Healthy Human Settlements: Opportunities and Challenges in Northern Thailand. Landsc. Archit. J. 2020, 27, 77–88. [Google Scholar]
- Kim, G.; Miller, P.A. The impact of green infrastructure on human health and well-being: The example of the Huckleberry Trail and the Heritage Community Park and Natural Area in Blacksburg, Virginia. Sustain. Cities Soc. 2019, 48, 101562. [Google Scholar] [CrossRef]
- Maruthaveeran, S. The perception of social safety in a green environment: A preliminary study at the Kepong Metropolitan Park. Asian J. Environ. -Behav. Stud. 2016, 1, 99–111. [Google Scholar] [CrossRef]
- Malek, N.A.; Mariapan, M. Visitors perception on vandalism and safety issues in a Malaysian urban park. Theor. Empir. Res. Urban Manag. 2009, 4, 93–107. [Google Scholar]
- Pretty, J.; Peacock, J.; Sellens, M.; Griffin, M. The mental and physical health outcomes of green exercise. Int. J. Environ. Health Res. 2005, 15, 319–337. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health benefits from nature experiences depend on dose. Sci. Rep. 2016, 6, 28551. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rai Mae Hia (n = 41) | Nong Buak Had Park (n = 34) | Three Kings Monument (n = 36) | Total (n = 111) | Percent | ||
|---|---|---|---|---|---|---|
| Age | 18–24 | 13 | 6 | 17 | 36 | 32.43 |
| 25–49 | 19 | 14 | 13 | 46 | 41.44 | |
| 50–64 | 9 | 14 | 6 | 29 | 26.13 | |
| Sex | Male | 21 | 17 | 19 | 57 | 51.35 |
| Female | 20 | 17 | 17 | 54 | 48.65 | |
| Occupation | Physical job | 1 | 3 | 2 | 6 | 5.40 |
| Desk job | 15 | 13 | 9 | 37 | 33.33 | |
| Homemaking | 5 | 4 | 2 | 11 | 9.90 | |
| Unemployed | 2 | 3 | 2 | 7 | 6.31 | |
| Student | 11 | 3 | 11 | 25 | 22.52 | |
| Other | 7 | 8 | 10 | 25 | 22.52 | |
| Living Social Condition | With others | 30 | 27 | 33 | 90 | 81.08 |
| Alone | 10 | 7 | 3 | 21 | 18.92 | |
| Race | Central Thai | 11 | 12 | 11 | 34 | 30.63 |
| Northern Thai | 25 | 18 | 17 | 60 | 54.05 | |
| Chinese Thai | 3 | 0 | 4 | 7 | 6.31 | |
| Muslim Thai | 1 | 1 | 1 | 3 | 2.70 | |
| Others | 1 | 3 | 3 | 7 | 6.31 |
| Gender | Height (m) | Weight (kg) | BMI (kg/m2) | Waist (in) | Hip (in) | WHR | |
|---|---|---|---|---|---|---|---|
| Male | mean | 1.70 | 71.02 | 24.74 | 32.88 | 36.77 | 0.90 |
| S.D. | 0.06 | 22.86 | 8.61 | 4.28 | 3.99 | 0.07 | |
| maximum | 1.82 | 180.00 | 69.51 | 43.00 | 45.00 | 1.09 | |
| minimum | 1.55 | 40.00 | 13.21 | 21.00 | 28.00 | 0.72 | |
| Female | mean | 1.59 | 56.30 | 22.30 | 29.47 | 37.23 | 0.79 |
| S.D. | 0.07 | 9.72 | 3.51 | 4.03 | 3.73 | 0.10 | |
| maximum | 1.74 | 97.00 | 32.04 | 43.50 | 48.00 | 1.21 | |
| minimum | 1.45 | 37.00 | 15.60 | 23.00 | 29.00 | 0.64 | |
| Total | mean | 1.65 | 63.93 | 23.56 | 31.22 | 36.99 | 0.85 |
| S.D. | 0.08 | 19.19 | 6.74 | 4.48 | 3.85 | 0.10 | |
| maximum | 1.82 | 180.00 | 69.51 | 43.50 | 48.00 | 1.21 | |
| minimum | 1.45 | 37.00 | 13.21 | 21.00 | 28.00 | 0.64 |
| Independent Variable | Sex | Degree of Freedom | F Value | Assumption of Equal Variances | p-Value (or Welch’s p-Value) |
|---|---|---|---|---|---|
| Age | Men | (2,47) | 2.9 | 0.1 | 0.07 |
| Women | (2,44) | 4.4 | 0.8 | 0.02 * | |
| Occupation | Men | (5,42) | 1.1 | 0.6 | 0.70 |
| Women | (5,44) | 3.4 | 1.0 | 0.48 | |
| Living social condition **** | Men | (1,48) | −0.4 **** | 0.8 | 0.67 |
| Women | (1,46) | −1.4 **** | 0.6 | 0.82 | |
| Race | Men | (3,46) | 0.39 | 0.5 | 0.72 |
| Women | (4,43) | 1.37 | 4.2 | 0.05 | |
| Distance | Men | (3,46) | 0.4 | 0.4 | 0.75 |
| Women | (3,43) | 1.5 | 0.9 | 0.23 | |
| Duration | Men | (2,47) | 1.9 | 0.1 | 0.16 |
| Women | (2,44) | 3.8 | 0.02 ** | 0.003 * | |
| Frequency | Men | (4,45) | 0.4 | - *** | - *** |
| Women | (4,42) | 1.0 | 0.5 | 0.25 |
| Variable | Coefficient | Standard Error | Wald’s Statistics | Degree of Freedom | p-Value | OR [95% CI] |
|---|---|---|---|---|---|---|
| Gender (M) | −1.04 | 0.49 | 4.69 | 1 | 0.04 * | 0.35 [0.13, 0.90] |
| Age | 1.07 | 0.35 | 8.04 | 1 | 0.003 * | 2.91 [1.35, 5.26] |
| Occupation | −0.01 | 0.14 | 0.01 | 1 | 0.93 | 1.0 [0.75, 1.29] |
| Living Social condition | 0.05 | 0.33 | 0.03 | 1 | 0.87 | 1.1 [0.56, 2,00] |
| Race | 0.14 | 0.23 | 0.39 | 1 | 0.53 | 1.2 [0.74, 1.81] |
| Distance | 0.175 | 0.29 | 0.38 | 1 | 0.54 | 1.22 [0.68, 2.08] |
| Duration | −0.78 | 0.39 | 3.90 | 1 | 0.046 * | 0.45 [0.21, 1.99] |
| Constant | −0.59 | 1.64 | 0.00 | 1 | 0.97 | 0.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suppakittpaisarn, P.; Charoenlertthanakit, N.; Yaipimol, E.; Surinseng, V.; Wanitchayapaisit, C.; Kim, G. Relationship between the Duration of Urban Nature and a Lower Waist-Hip Ratio. Int. J. Environ. Res. Public Health 2022, 19, 11606. https://doi.org/10.3390/ijerph191811606
Suppakittpaisarn P, Charoenlertthanakit N, Yaipimol E, Surinseng V, Wanitchayapaisit C, Kim G. Relationship between the Duration of Urban Nature and a Lower Waist-Hip Ratio. International Journal of Environmental Research and Public Health. 2022; 19(18):11606. https://doi.org/10.3390/ijerph191811606
Chicago/Turabian StyleSuppakittpaisarn, Pongsakorn, Nadchawan Charoenlertthanakit, Ekachai Yaipimol, Vipavee Surinseng, Chulalux Wanitchayapaisit, and Gunwoo Kim. 2022. "Relationship between the Duration of Urban Nature and a Lower Waist-Hip Ratio" International Journal of Environmental Research and Public Health 19, no. 18: 11606. https://doi.org/10.3390/ijerph191811606
APA StyleSuppakittpaisarn, P., Charoenlertthanakit, N., Yaipimol, E., Surinseng, V., Wanitchayapaisit, C., & Kim, G. (2022). Relationship between the Duration of Urban Nature and a Lower Waist-Hip Ratio. International Journal of Environmental Research and Public Health, 19(18), 11606. https://doi.org/10.3390/ijerph191811606