
COVID-19, Non-Communicable Diseases, and Behavioral Factors in the Peruvian Population ≥ 15 Years: An Ecological Study during the First and Second Year of the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Area Study
2.2. Risk Factors in Peru
2.3. COVID-19 Data Collection
2.4. Confounding Factors
2.5. Statistical Analysis
2.6. Ethics
3. Results
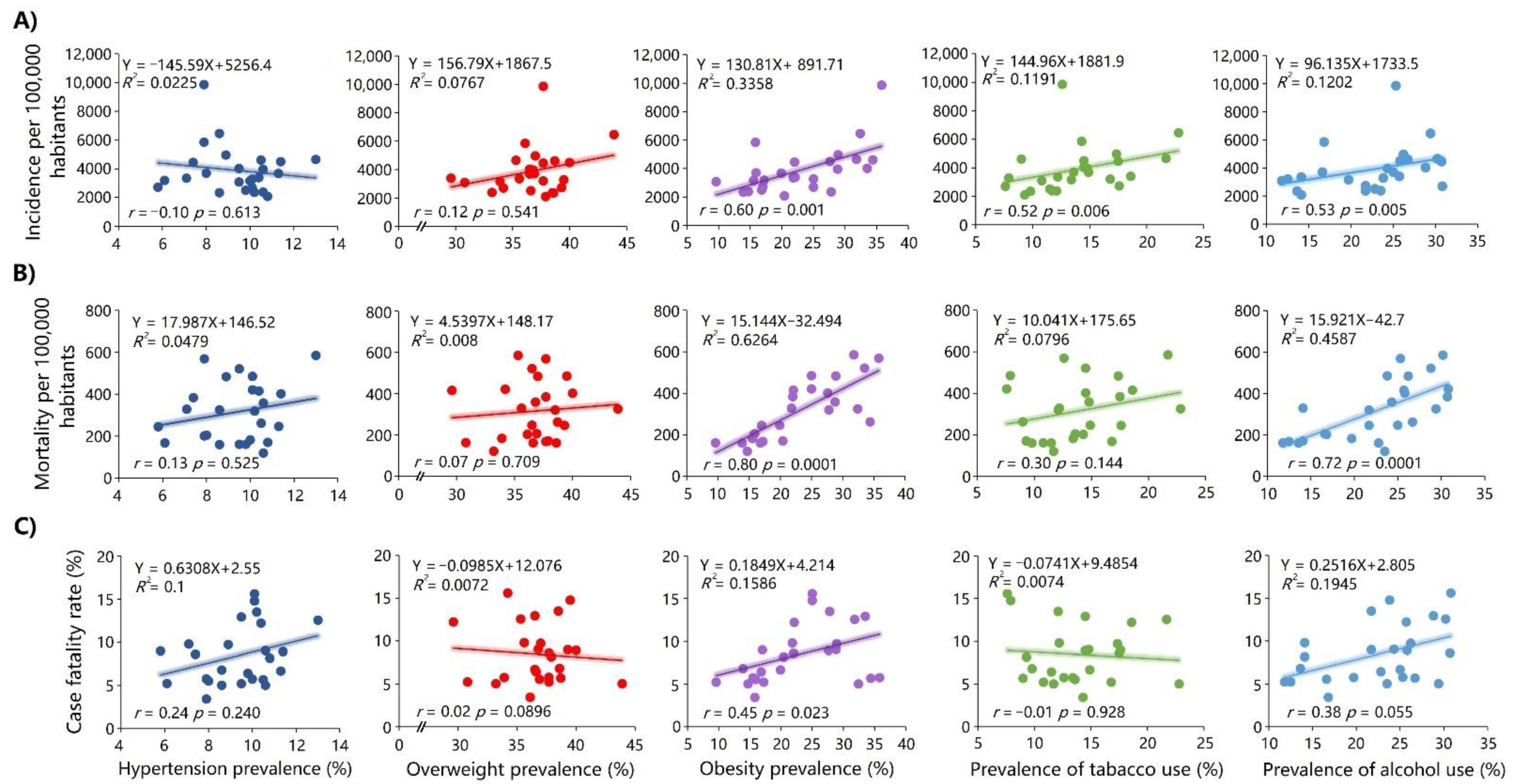
3.1. Correlation between the Study Variables and COVID-19 Measures in 2020
3.2. Regression Analysis in 2020
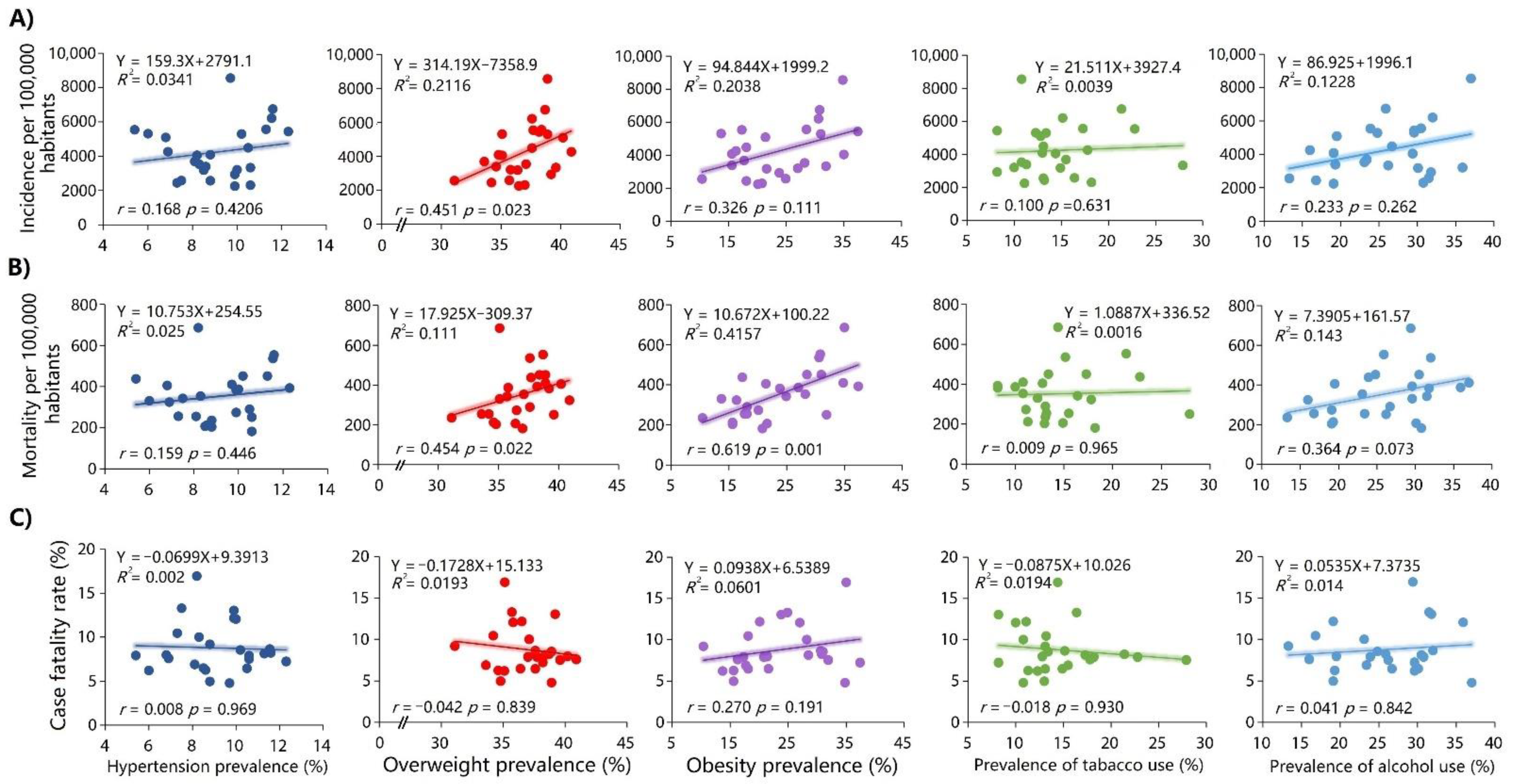
3.3. Correlation between the Study Variables and COVID-19 Measures in 2021
3.4. Regression Analysis in 2021
4. Discussion
4.1. Potential Explanations and Implications
4.2. Limitations
4.3. Implications for Public Health
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Item No | Recommendation | |
|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | ||
| Introduction | ||
| Background/rationale | 1 | Explain the scientific background and rationale for the investigation being reported |
| Objectives | 2 | State specific objectives, including any prespecified hypotheses |
| Methods | ||
| Study design | 2 | Present key elements of study design early in the paper |
| Setting | 2 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection |
| Participants | 2–3 | (a) Ecological study Case-control study—Give the eligibility criteria and the sources and methods of case ascertainment and control selection. Give the rationale for the choice of cases and controls Cross-sectional study—Give the eligibility criteria and the sources and methods of selection of participants |
| (b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed Case-control study—For matched studies, give matching criteria and the number of controls per case | ||
| Variables | 3 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable |
| Data sources/measurement | 3 * | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group |
| Bias | NA | Describe any efforts to address potential sources of bias |
| Study size | NA | Explain how the study size was arrived at |
| Quantitative variables | 3 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why |
| Statistical methods | 3 | (a) Describe all statistical methods, including those used to control for confounding |
| (b) Describe any methods used to examine subgroups and interactions | ||
| (c) Explain how missing data were addressed | ||
| (d) Cohort study—If applicable, explain how loss to follow-up was addressed Case-control study—If applicable, explain how matching of cases and controls was addressed Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy | ||
| (e) Describe any sensitivity analyses | ||
| Results | ||
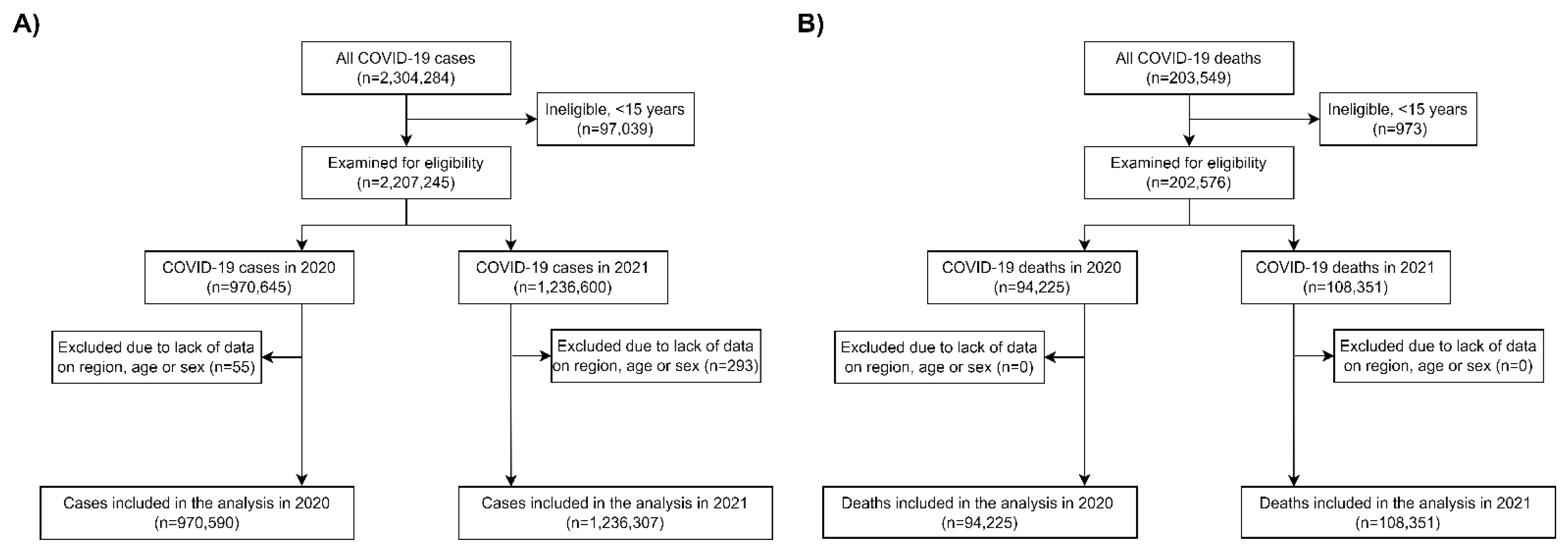
| Participants | 3 * | (a) Report numbers of individuals at each stage of study—e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analyzed |
| (b) Give reasons for non-participation at each stage | ||
| (c) Consider use of a flow diagram | ||
| Descriptive data | 4 * | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders |
| (b) Indicate number of participants with missing data for each variable of interest | ||
| (c) Cohort study—Summarize follow-up time (e.g., average and total amount) | ||
| Outcome data | 4–9 * | Cohort study—Report numbers of outcome events or summary measures over time |
| Case-control study—Report numbers in each exposure category or summary measures of exposure | ||
| Cross-sectional study—Report numbers of outcome events or summary measures | ||
| Main results | 4–9 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included |
| (b) Report category boundaries when continuous variables were categorized | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | ||
| Other analyses | 4–9 | Report other analyses done—e.g., analyses of subgroups and interactions and sensitivity analyses |
| Discussion | ||
| Key results | 9–10 | Summarize key results with reference to study objectives |
| Limitations | 11 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias |
| Interpretation | 9–11 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence |
| Generalizability | 9–11 | Discuss the generalizability (external validity) of the study results |
| Other information | ||
| Funding | 11 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based |
References
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019–COVID-19. Clin. Microbiol. Rev. 2020, 33, 1–48. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhu, L.; Liu, L.; Zhao, X.; Zhang, Z.; Xue, L.; Yan, X.; Huang, S.; Li, Y.; Cheng, J.; et al. Overweight and Obesity are Risk Factors of Severe Illness in Patients with COVID-19. Obesity 2020, 28, 2049. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Piernas, C.; Astbury, N.M.; Hippisley-Cox, J.; O’Rahilly, S.; Aveyard, P.; Jebb, S.A. Associations between body-mass index and COVID-19 severity in 6·9 million people in England: A prospective, community-based, cohort study. Lancet Diabetes Endocrinol. 2021, 9, 350–359. [Google Scholar] [CrossRef]
- Westheim, A.J.F.; Bitorina, A.V.; Theys, J.; Shiri-Sverdlov, R. COVID-19 infection, progression, and vaccination: Focus on obesity and related metabolic disturbances. Obes Rev. 2021, 22, e13313. [Google Scholar] [CrossRef]
- Hendren, N.S.; de Lemos, J.A.; Ayers, C.; Das, S.R.; Rao, A.; Carter, S.; Rosenblatt, A.; Walchok, J.; Omar, W.; Khera, R.; et al. Association of Body Mass Index and Age with Morbidity and Mortality in Patients Hospitalized With COVID-19. Circulation 2021, 143, 135–144. [Google Scholar] [CrossRef]
- Sarmadi, M.; Ahmadi-Soleimani, S.M.; Fararouei, M.; Dianatinasab, M. COVID-19, body mass index and cholesterol: An ecological study using global data. BMC Public Health. 2021, 21, 1–14. [Google Scholar] [CrossRef]
- Rosoff, D.B.; Yoo, J.; Lohoff, F.W. A genetically-informed study disentangling the relationships between tobacco smoking, cannabis use, alcohol consumption, substance use disorders and respiratory infections, including COVID-19. medRxiv 2021. [CrossRef]
- Simons, D.; Shahab, L.; Brown, J.; Perski, O. The association of smoking status with SARS-CoV-2 infection, hospitalization and mortality from COVID-19: A living rapid evidence review with Bayesian meta-analyses (version 7). Addiction 2021, 116, 1319. [Google Scholar] [CrossRef]
- Kelly, J.D.; Bravata, D.M.; Bent, S.; Wray, C.M.; Leonard, S.J.; Boscardin, W.J.; Myers, L.J.; Keyhani, S. Association of Social and Behavioral Risk Factors with Mortality Among US Veterans With COVID-19. JAMA Netw. Open 2021, 4, e2113031. [Google Scholar] [CrossRef]
- Peruvian Ministry of Health (MINSA). Available online: https://covid19.minsa.gob.pe/ (accessed on 8 September 2022).
- Ramírez-Soto, M.C.; Ortega-Cáceres, G.; Arroyo-Hernández, H. Original research: Excess all-cause deaths stratified by sex and age in Peru: A time series analysis during the COVID-19 pandemic. BMJ Open 2022, 12, e057056. [Google Scholar] [CrossRef]
- Ramírez-Soto, M.C.; Alarcón-Arroyo, M.; Chilcon-Vitor, Y.; Chirinos-Pérez, Y.; Quispe-Vargas, G.; Solsol-Jacome, K.; Zavaleta, E.Q. Association between Obesity and COVID-19 Mortality in Peru: An Ecological Study. Trop Med Infect Dis. 2021, 6, 182. [Google Scholar] [CrossRef] [PubMed]
- Acosta, G.; Escobar, G.; Bernaola, G.; Alfaro, J.; Taype, W.; Marcos, C.; Amado, J. Description of patients with severe COVID-19 treated in a national referral hospital in Peru. Rev. Peru. Med. Exp. Salud Publica 2020, 37, 253–258. [Google Scholar] [CrossRef] [PubMed]
- The Peruvian. Peru Starts Vaccination Plan against COVID-19; The Peruvian: Lima, Peru, 2021. [Google Scholar]
- Escobar-Agreda, S.; Vargas Herrera, J.; Rojas-Mezarina, L. Preliminary evidence on the effect of vaccination against COVID-19 in Peru. Bol. Inst. Nac. Salud 2021, 27, 35–44. [Google Scholar]
- Escobar-Agreda, S.; Silva-Valencia, J.; Rojas-Mezarina, L.; Vargas-Herrera, J. Survival of health workers infected by SARS-CoV-2 in the context of vaccination against COVID-19 in Peru. An. Fac. Med. 2021, 82, 106–112. [Google Scholar]
- National Institute of Statistics and Informatics (INEI). Peruvian Population. Available online: https://www.inei.gob.pe/estadisticas/indice-tematico/population-estimates-and-projections/ (accessed on 3 June 2021).
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- National Institute of Statistics and Informatics (INEI). Peru—National Demographic and Health Survey (ENDES) 2020. Noncommunicable and Communicable Diseases. 2020. Available online: https://proyectos.inei.gob.pe/endes/2020/SALUD/ENFERMEDADES_ENDES_2020.pdf (accessed on 8 September 2022).
- National Institute of Statistics and Informatics (INEI). Peru—National Demographic and Health Survey (ENDES) 2021. Noncommunicable and Communicable Diseases. 2021. Available online: https://proyectos.inei.gob.pe/endes/2021/SALUD/ENFERMEDADES_ENDES_2021.pdf (accessed on 8 September 2022).
- Peruvian Ministry of Health (MINSA). COVID-19 deaths. National System of Deaths (SINADEF). Available online: https://www.datosabiertos.gob.pe/dataset/fallecidos-por-covid-19-ministerio-de-salud-minsa (accessed on 3 June 2021).
- Superintendencia Nacional de Salud, Peru (SUSALUD). Daily Report on Form F500.2, App. for Centralized Management of the Availability of Hospitalization and ICU Beds at the National Level and of All Subsystems (Application F500.2); SUSALUD: Lima, Peru, 2020; Available online: http://portal.susalud.gob.pe/seguimiento-del-registro-de-camas-f500-2/ (accessed on 26 December 2021).
- Peruvian Ministry of Health (MINSA). Single National Health Information Repository (REUNIS). COVID-19 vaccine in Peru. Available online: https://www.minsa.gob.pe/reunis/data/vacunas-covid19.asp (accessed on 8 September 2022).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Al-Benna, S. Association of high level gene expression of ACE2 in adipose tissue with mortality of COVID-19 infection in obese patients. Obes. Med. 2020, 19, 100283. [Google Scholar] [CrossRef]
- Schwalb, A.; Seas, C. The COVID-19 Pandemic in Peru: What Went Wrong? Am. J. Trop. Med. Hyg. 2021, 104, 1176–1178. [Google Scholar] [CrossRef]
- Taylor, L. COVID-19: Why Peru suffers from one of the highest excess death rates in the world. BMJ 2021, 372, n611. [Google Scholar] [CrossRef]
- Townsend, M.J.; Kyle, T.K.; Stanford, F.C. COVID-19 Vaccination and Obesity: Optimism and Challenges. Obesity 2021, 29, 634. [Google Scholar] [CrossRef]
- Egawa, Y.; Ohfuji, S.; Fukushima, W.; Yamazaki, Y.; Morioka, T.; Emoto, M.; Maeda, K.; Inaba, M.; Hirota, Y. Immunogenicity of influenza A(H1N1)pdm09 vaccine in patients with diabetes mellitus: With special reference to age, body mass index, and HbA1c. Hum. Vaccin. Immunother. 2014, 10, 1187. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [PubMed]
- Widdifield, J.; Kwong, J.C.; Chen, S.; Eder, L.; Benchimol, E.I.; Kaplan, G.G.; Hitchon, C.; Aviña-Zubieta, J.A.; Lacaille, D.; Chung, H. Vaccine effectiveness against SARS-CoV-2 infection and severe outcomes among individuals with immune-mediated inflammatory diseases tested between March 1 and Nov 22, 2021, in Ontario, Canada: A population-based analysis. Lancet Rheumatol. 2022, 4, e430–e440. [Google Scholar] [CrossRef]



| Region | Hypertension Prevalence (%) | Overweight Prevalence (%) | Obesity Prevalence (%) | Prevalence of Tobacco Use (%) | Prevalence of Alcohol Use (%) | Population ≥ 15 Years in 2020 | Incidence Rate (per 100,000 Habitants) | Mortality Rate (per 100,000 Habitants) | Case Fatality Rate (%) | Gender Balance in Deaths (Men/Women) * | Mean Age in Deaths (Years) * | Mean Monthly Income (PEN) * | No. of ICU Beds in 2020 *† |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amazonas | 7.9 | 36.1 | 15.8 | 14.3 | 16.8 | 289,802 | 5852.62 | 201.52 | 3.44 | 2.0 | 64.8 | 992.9 | 14 |
| Ancash | 7.1 | 35.6 | 21.8 | 12.2 | 14.1 | 876,703 | 3351.65 | 328.5 | 9.8 | 2.1 | 68.2 | 1057.2 | 44 |
| Apurímac | 10.6 | 33.2 | 14.7 | 11.7 | 23.5 | 300,395 | 2384.53 | 119.84 | 5.03 | 1.5 | 68.1 | 1004.5 | 26 |
| Arequipa | 10.6 | 36.8 | 28.8 | 14.8 | 24.3 | 1,187,931 | 3962.01 | 358.1 | 9.04 | 1.2 | 68.9 | 1530.3 | 70 |
| Ayacucho | 10 | 33.9 | 15.5 | 13.4 | 19.7 | 464,136 | 3162.87 | 182.06 | 5.76 | 2.1 | 66.3 | 1095.4 | 20 |
| Cajamarca | 8.6 | 38.6 | 13.9 | 9.8 | 13.6 | 1,016,792 | 2348.66 | 159.82 | 6.8 | 2.1 | 68.1 | 850.2 | 26 |
| Callao | 13 | 35.3 | 31.8 | 21.7 | 30.2 | 902,609 | 4655.17 | 584.53 | 12.56 | 2.1 | 67.4 | 1355.6 | 84 |
| Cusco | 9.8 | 36.6 | 16.8 | 11.5 | 22.8 | 988,897 | 2504.61 | 160.89 | 6.42 | 1.3 | 66.0 | 963.1 | 17 |
| Huancavelica | 9.5 | 30.8 | 9.6 | 10.8 | 11.8 | 236,955 | 3083.29 | 161.21 | 5.23 | 2.0 | 66.6 | 669.0 | 10 |
| Huánuco | 8 | 36.9 | 15.9 | 13.6 | 16.6 | 524,371 | 3701.39 | 205.01 | 5.54 | 1.6 | 67.5 | 892.4 | 49 |
| Ica | 9.5 | 36.5 | 33.5 | 14.5 | 28.8 | 725,610 | 4025.72 | 520.67 | 12.93 | 1.7 | 67.1 | 1478.2 | 48 |
| Junín | 5.8 | 39.3 | 17 | 17.6 | 21.7 | 982,199 | 2728.06 | 245.16 | 8.99 | 1.8 | 65.7 | 1082.7 | 43 |
| La Libertad | 10.2 | 38.5 | 27.8 | 12.1 | 21.7 | 1,531,668 | 2366.96 | 319.46 | 13.5 | 1.9 | 67.1 | 1167.2 | 63 |
| Lambayeque | 10.1 | 39.5 | 25 | 7.9 | 23.8 | 991,121 | 3280.23 | 484.7 | 14.78 | 1.7 | 67.1 | 1159.6 | 39 |
| Lima | 8.9 | 37 | 28.9 | 17.35 | 26.2 | 8,750,417 | 4967.75 | 482.94 | 9.72 | 1.8 | 66.9 | 1653.5 | 739 |
| Loreto | 10.4 | 29.6 | 22.1 | 18.6 | 25.7 | 680,927 | 3396.69 | 415.02 | 12.22 | 2.0 | 65.6 | 1180.4 | 8 |
| Madre de Dios | 8.6 | 43.9 | 32.4 | 22.8 | 29.4 | 135,428 | 6460.26 | 324.9 | 5.03 | 2.8 | 63.0 | 1399.9 | 8 |
| Moquegua | 7.9 | 37.7 | 35.8 | 12.6 | 25.3 | 155,545 | 9861.45 | 568.32 | 5.76 | 2.6 | 68.8 | 1693.7 | 18 |
| Pasco | 6.1 | 37.7 | 17.2 | 16.8 | 12.5 | 195,114 | 3198.64 | 167.59 | 5.24 | 1.7 | 63.7 | 834.8 | 12 |
| Piura | 10.1 | 34.2 | 25 | 7.6 | 30.8 | 1,535,433 | 2694.29 | 420.4 | 15.6 | 1.9 | 66.8 | 992.6 | 81 |
| Puno | 10.8 | 37.9 | 20.4 | 9.3 | 14.1 | 904,267 | 2088.54 | 170.41 | 8.16 | 1.7 | 63.4 | 809.8 | 20 |
| San Martín | 11.3 | 36.5 | 19.9 | 14.9 | 25 | 639,533 | 3682.53 | 245.96 | 6.68 | 2.1 | 65.8 | 983.3 | 17 |
| Tacna | 10.5 | 38.7 | 34.4 | 9 | 26.7 | 303,701 | 4613.42 | 262.1 | 5.68 | 2.3 | 65.5 | 1259.9 | 26 |
| Tumbes | 11.4 | 40 | 27.6 | 14.5 | 25.8 | 191,850 | 4501.43 | 401.36 | 8.92 | 1.9 | 65.9 | 1142.6 | 8 |
| Ucayali | 7.4 | 37.7 | 22 | 17.5 | 30.7 | 416,932 | 4454.68 | 383.52 | 8.61 | 1.9 | 64.3 | 1203.1 | 18 |
| Region | Hypertension Prevalence (%) | Overweight Prevalence (%) | Obesity Prevalence (%) | Prevalence of Tobacco Use (%) | Prevalence of Alcohol Use (%) | Population ≥ 15 Years in 2021 | Incidence Rate (per 100,000 Habitants) | Mortality Rate (per 100,000 Habitants) | Case Fatality Rate (%) | Gender Balance in Deaths (Men/Women) * | Mean Age in Deaths (Years) * | No. of ICU Beds in 2021 *† | Vaccination Coverage in Individuals ≥ 18 Years (%) * |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amazonas | 8.8 | 34.8 | 15.6 | 13.0 | 19.1 | 340,717 | 4084.33 | 203.39 | 4.98 | 1.7 | 66.4 | 20 | 68.0 |
| Ancash | 6.8 | 40.2 | 21.4 | 12.8 | 19.5 | 953,816 | 5092.07 | 405.21 | 7.96 | 1.7 | 67.3 | 49 | 88.4 |
| Apurímac | 6.0 | 35.1 | 13.7 | 12.3 | 29.6 | 351,074 | 5305.15 | 330.41 | 6.23 | 1.6 | 69.5 | 36 | 82.1 |
| Arequipa | 11.3 | 38.4 | 28.5 | 17.3 | 30.5 | 1,215,179 | 5560.17 | 451.29 | 8.12 | 1.6 | 65.9 | 53 | 84.5 |
| Ayacucho | 8.1 | 33.6 | 17.7 | 15.5 | 23.4 | 519,656 | 3685.52 | 254.59 | 6.91 | 1.6 | 68.2 | 20 | 70.6 |
| Cajamarca | 8.6 | 34.6 | 15.6 | 11.3 | 19.3 | 1,201,697 | 3387.38 | 212.62 | 6.28 | 1.7 | 68.0 | 54 | 75.4 |
| Callao | 11.6 | 38.7 | 30.8 | 21.4 | 25.9 | 877,161 | 6741.64 | 553.38 | 8.21 | 1.7 | 65.4 | 90 | 90.0 |
| Cusco | 10.5 | 37.6 | 18.1 | 13.1 | 26.7 | 1,111,868 | 4482.73 | 290.05 | 6.47 | 1.7 | 67.5 | 34 | 79.0 |
| Huancavelica | 8.8 | 31.1 | 10.4 | 13.1 | 13.3 | 330,566 | 2563.78 | 235.35 | 9.18 | 1.7 | 67.8 | 21 | 73.3 |
| Huánuco | 7.3 | 34.2 | 18.1 | 13.2 | 16.8 | 645,200 | 2445.44 | 255.27 | 10.44 | 1.9 | 67.1 | 31 | 69.7 |
| Ica | 8.2 | 35.1 | 35.0 | 14.4 | 29.4 | 700,394 | 4047.44 | 686.04 | 16.95 | 1.5 | 65.3 | 95 | 92.8 |
| Junín | 5.4 | 37.7 | 17.3 | 22.8 | 23.9 | 1,063,849 | 5538.47 | 437.66 | 7.9 | 1.8 | 66.2 | 64 | 81.2 |
| La Libertad | 8.3 | 37.1 | 28.2 | 10.8 | 23.1 | 1,544,977 | 3533.45 | 353.6 | 10.01 | 1.6 | 66.9 | 99 | 83.0 |
| Lambayeque | 9.9 | 39.2 | 23.8 | 8.2 | 31.8 | 1,050,982 | 2935.35 | 382.5 | 13.03 | 1.8 | 66.4 | 54 | 80.8 |
| Lima | 11.6 | 37.6 | 30.6 | 15.2 | 32.0 | 8,796,347 | 6206.02 | 536.17 | 8.64 | 1.7 | 65.5 | 662 | 88.8 |
| Loreto | 10.6 | 37.0 | 20.8 | 18.2 | 30.8 | 785,301 | 2301.03 | 181.71 | 7.9 | 1.5 | 64.4 | 36 | 64.5 |
| Madre de Dios | 10.6 | 39.6 | 31.9 | 27.9 | 26.2 | 129,465 | 3332.17 | 251.03 | 7.53 | 2.2 | 62.0 | 25 | 57.8 |
| Moquegua | 9.7 | 38.9 | 34.8 | 10.8 | 37.0 | 157,704 | 8552.1 | 410.26 | 4.8 | 1.8 | 66.9 | 24 | 83.7 |
| Pasco | 6.9 | 40.9 | 16.3 | 17.8 | 16.0 | 222,411 | 4259.23 | 323.72 | 7.6 | 1.4 | 64.0 | 29 | 81.4 |
| Piura | 10.0 | 35.8 | 27.0 | 10.0 | 35.9 | 1,521,251 | 3209.07 | 387.12 | 12.06 | 1.5 | 66.4 | 122 | 83.4 |
| Puno | 9.9 | 36.5 | 20.1 | 11.1 | 19.1 | 989,125 | 2248.05 | 273.47 | 12.16 | 2.1 | 64.5 | 40 | 57.5 |
| San Martín | 8.5 | 36.4 | 21.6 | 14.9 | 30.1 | 701,517 | 3178.97 | 206.55 | 6.5 | 1.6 | 66.2 | 29 | 73.6 |
| Tacna | 12.3 | 38.2 | 37.4 | 8.2 | 29.6 | 301,148 | 5434.54 | 393.16 | 7.23 | 2.0 | 63.8 | 35 | 75.2 |
| Tumbes | 10.2 | 38.9 | 31.0 | 13.4 | 24.8 | 181,769 | 5291.88 | 451.12 | 8.52 | 1.9 | 65.9 | 21 | 86.8 |
| Ucayali | 7.5 | 35.7 | 24.9 | 16.4 | 31.5 | 436,045 | 2579.09 | 342.63 | 13.28 | 1.8 | 64.5 | 28 | 64.3 |
| No Adjusted Analysis | Full Adjusted Analysis | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Model | Coef. | SE | Beta (β) | t | p | Coef. | SE | Beta (β) | t | p |
| Crude incidence rate per 100,000 habitants | ||||||||||
| Obesity prevalence | 130.81 | 38.36 | 0.579 | 3.41 | 0.002 | 28.31 | 72.89 | 0.125 | 0.39 | 0.7 |
| Smoking prevalence | 144.96 | 82.19 | 0.345 | 1.76 | 0.091 | −54.86 | 80.7 | −0.13 | −0.68 | 0.51 |
| Prevalence of alcohol use | 96.13 | 54.24 | 0.346 | 1.77 | 0.09 | −50.73 | 55.3 | −0.182 | −0.92 | 0.37 |
| Crude mortality rate per 100,000 habitants | ||||||||||
| Obesity prevalence | 15.14 | 2.46 | 0.787 | 6.13 | 0.0001 | 11.18 | 4.98 | 0.582 | 2.25 | 0.037 |
| Prevalence of alcohol use | 15.95 | 3.51 | 0.687 | 4.54 | 0.0001 | 8.09 | 4.47 | 0.348 | 1.81 | 0.087 |
| Fatality case rate (%) | ||||||||||
| Obesity prevalence | 0.185 | 0.089 | 0.397 | 2.08 | 0.049 | 0.463 | 0.171 | 0.993 | 2.70 | 0.014 |
| Crude Mortality Rate per 100,000 Habitants (No Adjusted) | Crude Mortality Rate per 100,000 Habitants (Full Adjusted) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Coef. | SE | Beta (β) | t | p | Coef. | SE | Beta (β) | t | p | |
| Overweight prevalence | 17.92 | 10.57 | 0.333 | 1.69 | 0.104 | 8.84 | 11.07 | 0.164 | 0.80 | 0.434 * |
| Obesity prevalence | 10.67 | 2.63 | 0.644 | 4.05 | 0.001 | 11.80 | 4.9 | 0.713 | 2.37 | 0.028 * |
| Overweight prevalence ** | NA | NA | NA | NA | NA | −18.7 | 6.35 | −0.349 | −2.96 | 0.008 |
| Obesity prevalence ** | NA | NA | NA | NA | NA | 0.52 | 3.94 | 0.031 | 0.13 | 0.895 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canorio, J.; Sánchez, F.; Ramírez-Soto, M.C. COVID-19, Non-Communicable Diseases, and Behavioral Factors in the Peruvian Population ≥ 15 Years: An Ecological Study during the First and Second Year of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 11757. https://doi.org/10.3390/ijerph191811757
Canorio J, Sánchez F, Ramírez-Soto MC. COVID-19, Non-Communicable Diseases, and Behavioral Factors in the Peruvian Population ≥ 15 Years: An Ecological Study during the First and Second Year of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(18):11757. https://doi.org/10.3390/ijerph191811757
Chicago/Turabian StyleCanorio, Jordan, Flor Sánchez, and Max Carlos Ramírez-Soto. 2022. "COVID-19, Non-Communicable Diseases, and Behavioral Factors in the Peruvian Population ≥ 15 Years: An Ecological Study during the First and Second Year of the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 18: 11757. https://doi.org/10.3390/ijerph191811757
APA StyleCanorio, J., Sánchez, F., & Ramírez-Soto, M. C. (2022). COVID-19, Non-Communicable Diseases, and Behavioral Factors in the Peruvian Population ≥ 15 Years: An Ecological Study during the First and Second Year of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(18), 11757. https://doi.org/10.3390/ijerph191811757