
Public Health Workforce Gaps, Impacts, and Improvement Strategies from COVID-19

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Qualitative Data
2.1.1. Moderator Training
2.1.2. Analysis
2.2. Quantitative Data
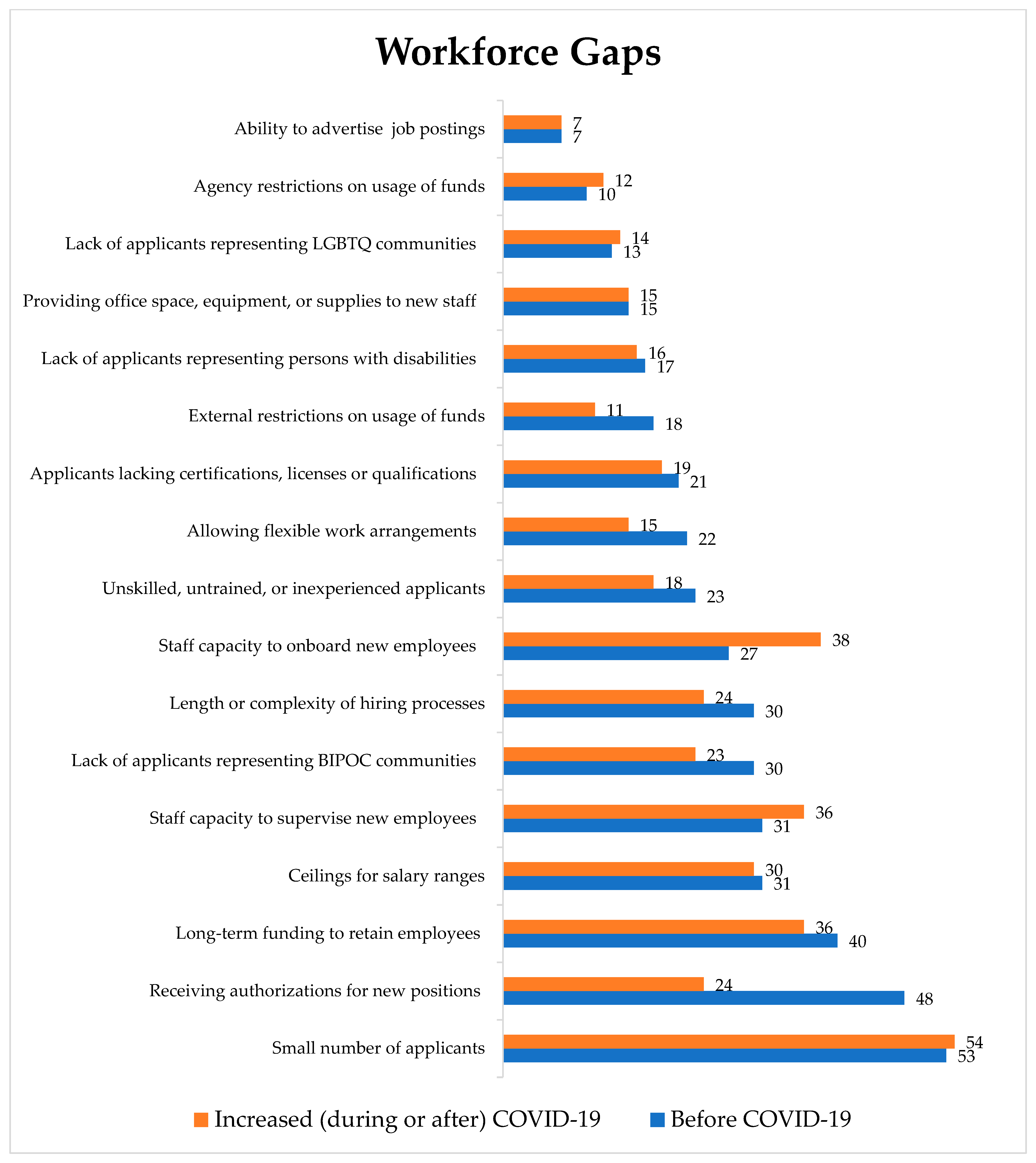
- “Before the COVID-19 pandemic (i.e., before March 2020), if and when adequate funding was available to increase staff capacity, were you concerned about any of the following items?” (survey respondents were given 17 different choices and were instructed to select all that apply);
- “Which of the following concerns increased during or after the pandemic, i.e., after March 2020?” (survey respondents were presented with the same list of choices as the previous question and were instructed to select all that apply); and
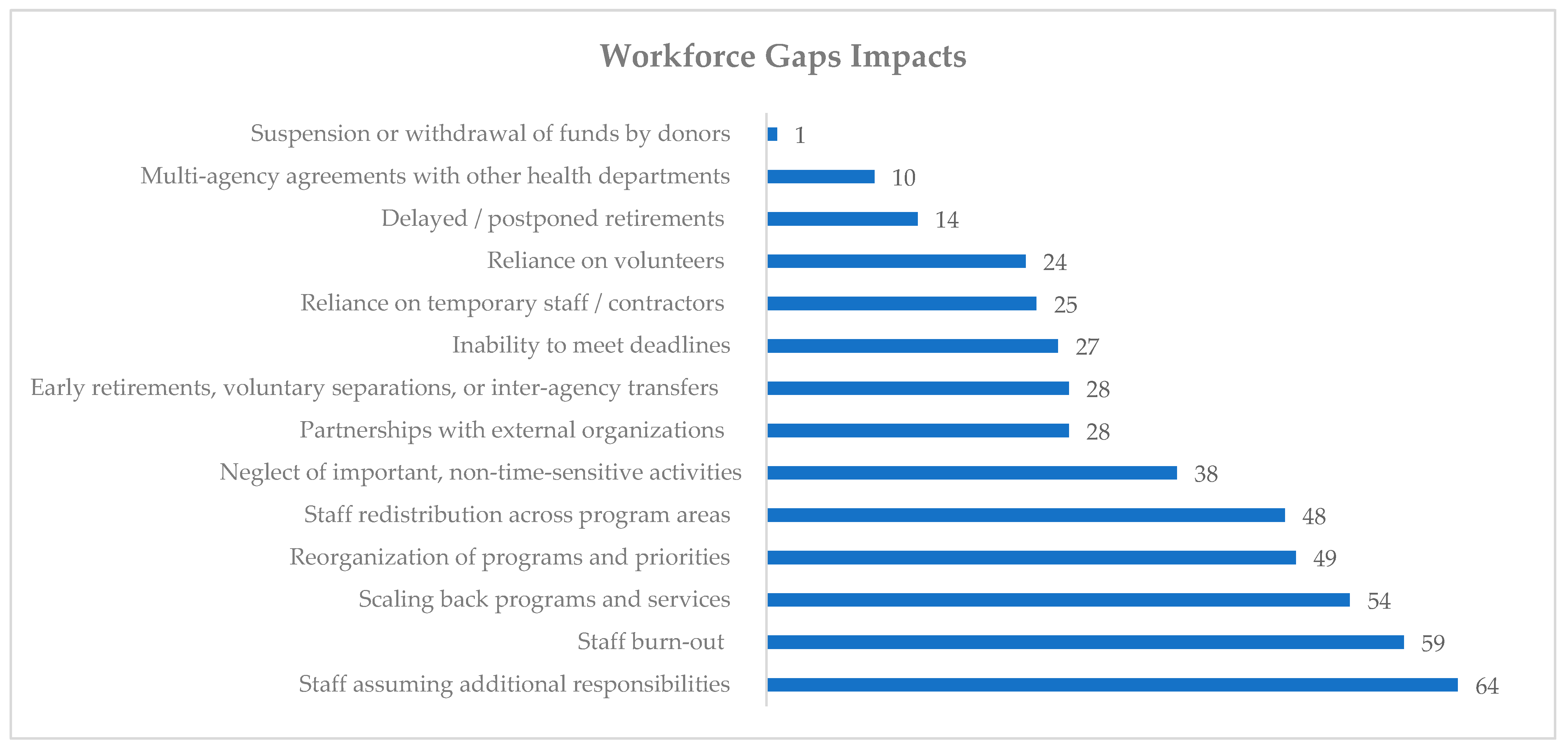
- “After the COVID-19 pandemic started (i.e., after March 2020), did staffing shortages at your agency lead to any of the following?” (survey respondents were provided 14 different choices and again instructed to select all that apply).
2.3. Data Integration
3. Results
3.1. Domain 1: Workforce Gaps
[Name] did it before. I don’t know how to do it and she didn’t have time to teach people before she left. So we’ve had to kind of cut out the ability to share a lot of data with the county.
3.2. Domain 2: Workforce Gaps Impacts
3.3. Domain 3: Improvement Strategies
…leadership matters when they see that I’m in the trenches with them and we’re making decisions as a team and providing those thank you’s and providing that support and those resources to them. That matters in retention. Because I can’t do anything about the money.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Public Health National Center for Innovation. Revising the Foundational Public Health Services in 2022. Available online: https://phnci.org/transformation/fphs (accessed on 8 October 2022).
- Pilkington, W.; Kumar, D. Public Health Departments Face Formidable Issues During COVID19 Pandemic. Homel. Secur. Aff. 2020, 16, 17. [Google Scholar]
- Pourshaban, D.; Basurto-Davila, R.; Shih, M. Building and Sustaining Strong Public Health Agencies: Determinants of Workforce Turnover. J. Public Health Manag. Pract. 2015, 21 (Suppl. 6), S80–S90. [Google Scholar] [CrossRef] [PubMed]
- Leider, J.P.; Sellers, K.; Owens-Young, J.; Guerrero-Ramirez, G.; Bogaert, K.; Gendelman, M.; Castrucci, B.C. Determinants of workplace perceptions among federal, state, and local public health staff in the US, 2014 to 2017. BMC Public Health 2021, 21, 1654. [Google Scholar] [CrossRef]
- Leider, J.P.; Harper, E.; Shon, J.W.; Sellers, K.; Castrucci, B.C. Job Satisfaction and Expected Turnover Among Federal, State, and Local Public Health Practitioners. Am. J. Public Health 2016, 106, 1782–1788. [Google Scholar] [CrossRef]
- Scales, S.E.; Patrick, E.; Stone, K.W.; Kintziger, K.W.; Jagger, M.A.; Horney, J.A. A Qualitative Study of the COVID-19 Response Experiences of Public Health Workers in the United States. Health Secur. 2021, 19, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.A.; Stone, E.M.; Mui, P.; Resnick, B. Pandemic-Related Workplace Violence and Its Impact on Public Health Officials, March 2020–January 2021. Am. J. Public Health 2022, 112, e1–e11. [Google Scholar] [CrossRef]
- Topazian, R.J.; McGinty, E.E.; Han, H.; Levine, A.S.; Anderson, K.E.; Presskreischer, R.; Barry, C.L. US Adults’ Beliefs About Harassing or Threatening Public Health Officials During the COVID-19 Pandemic. JAMA Netw. Open 2022, 5, e2223491. [Google Scholar] [CrossRef]
- Bogaert, K.; Castrucci, B.C.; Gould, E.; Sellers, K.; Leider, J.P.; Whang, C.; Whitten, V. The Public Health Workforce Interests and Needs Survey (PH WINS 2017): An Expanded Perspective on the State Health Agency Workforce. J. Public Health Manag. Pract. 2019, 25 (Suppl. 2), S13–S27. [Google Scholar] [CrossRef] [PubMed]
- Bryant-Genevier, J.; Rao, C.Y.; Lopes-Cardozo, B.; Kone, A.; Rose, C.; Thomas, I.; Orquiola, D.; Lynfield, R.; Shah, D.; Freeman, L. Symptoms of depression, anxiety, post-traumatic stress disorder, and suicidal ideation among state, tribal, local, and territorial public health workers during the COVID-19 Pandemic—United States, March–April 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 947. [Google Scholar] [CrossRef]
- de Beaumont Foundation. Rising Stress and Burnout in Public Health: Results of a National Survey of the Public Health Workforce; de Beaumont Foundation: Bethesda, MD, USA, 2022. [Google Scholar]
- de Beaumont Foundation. Public Health Workforce Interests and Needs Survey; de Beaumont Foundation: Bethesda, MD, USA, 2021. [Google Scholar]
- Wilson, R.T.; Trosis, C.L.; Gary-Webb, T.L. A Deficit of More Than 250,000 Public Health Workers is No Way to Fight COVID-19. COVID-19 Res. 2020. Available online: https://www.statnews.com/2020/04/05/deficit-public-health-workers-no-way-to-fight-covid-19/ (accessed on 22 August 2022).
- Barna, M. Minnesota prepares to launch public health corps at 60 locations statewide. Nation’s Health 2022, 52, 17. [Google Scholar]
- Smith, T.U.S. Senators Tina Smith, Susan Collins, Cory Booker, and Lisa Murkowski introduce bipartisan legistlation to rebuild public health workforce amidst shortages. Int. J. Environ. Res. Public Health 2022, 19, 4836. [Google Scholar]
- Minnesota Department of Health. Workforce Summary for Minnesota’s Local Public Health System in 2019; Minnesota Department of Health: St. Paul, MN, USA, 2021. [Google Scholar]
- Center for Public Health Practice. Public Health Workforce Assessment: Local Public Health and Higher Education in Minnesota; Minnesota Department of Health: St. Paul, MN, USA, 2019. [Google Scholar]
- Local Public Health Association. LPHA COVID-19 Survey; Local Public Health Association: St. Paul, MN, USA, 2020. [Google Scholar]
- Knudsen, J.; Chokshi, D.A. COVID-19 and the Safety Net—Moving from Straining to Sustaining. N. Engl. J. Med. 2021, 385, 2209–2211. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage Publications Inc.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Gibbs, A. Focus groups. Soc. Res. Update 1997, 19, 1–8. [Google Scholar]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research, 5th ed.; Sage Publication, Inc.: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Bingham, A.J.; Patricia, W. Deductive and inductive approaches to qualitative data analysis. In Analyzing and Interpreting Qualitative Data: After the Interview; Vanover, C., Mihas, P., Saldaña, J., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2022; pp. 133–146. [Google Scholar]
- Saldaña, J. The Coding Manual for Qualitative Researchers, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Institute of Medicine. The Future of Public Health; National Academy Press: Washington, DC, USA, 1988; Volume 88. [Google Scholar]
- Institute of Medicine. The Future of the Public’s Health in the 21st Century; National Academy Press: Washington, DC, USA, 2003. [Google Scholar]
- de Beaumont Foundation; PHNCI. Staffing up: Workforce Levels Needed to Provide Basic Public Health Services for All Americans; Trust for America’s Health: Washington, DC, USA, 2021. [Google Scholar]
- Hajat, A.; Stewart, K.; Hayes, K.L. The local public health workforce in rural communities. J. Public Health Manag. Pract. 2003, 9, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Draper, D.; Hurley, R.E.; Lauer, J.R. Public Health Workforce Shortages Imperil Nation’s Health; Center for Studying Health System Change: Washington, DC, USA, 2008. [Google Scholar]
- Leider, J.P.; Resnick, B.; Bishai, D.; Scutchfield, F.D. How Much Do We Spend? Creating Historical Estimates of Public Health Expenditures in the United States at the Federal, State, and Local Levels. Annu. Rev. Public Health 2018, 39, 471–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sellers, K.; Leider, J.P.; Gould, E.; Castrucci, B.C.; Beck, A.; Bogaert, K.; Coronado, F.; Shah, G.; Yeager, V.; Beitsch, L.M.; et al. The State of the US Governmental Public Health Workforce, 2014-2017. Am J Public Health 2019, 109, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, J.K.; Kneipp, S.M.; Campbell, L. A call to action for public health nurses during the COVID-19 pandemic. Public Health Nurs. 2020, 37, 323–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Primary Health Care Research Institute. Retention Strategies & Incentives for Health Workers in Rural and Remote Areas: What Works? The Australian National Univeristy: Canberra, Australia, 2009. [Google Scholar]
- Beck, A.J.; Boulton, M.; Lemmings, J.; Clayton, J.L. Challenges to recruitment and retention of the state health department epidemiology workforce. Am. J. Prev. Med. 2012, 42, 76–80. [Google Scholar] [CrossRef]
- Stone, K.W.; Kintziger, K.W.; Horney, J.A. Public Health Workforce Burnout in the COVID-19 Response in the U.S. Int. J. Environ. Res. Public Health 2021, 18, 4369. [Google Scholar] [CrossRef] [PubMed]
- Sellers, K.; Leider, J.P.; Lamprecht, L.; Liss-Levinson, R.; Castrucci, B.C. Using Public Health Workforce Surveillance Data to Prioritize Retention Efforts for Younger Staff. Am. J. Prev. Med. 2020, 59, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Cosgrave, C. The whole-of-person retention improvement framework: A guide for addressing health workforce challenges in the rural context. Int. J. Environ. Res. Public Health 2020, 17, 2698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, B.L.H.; Siepmann, I.; Chen, T.T.; Fisher, S.; Weitzel, T.S.; Nathan, N.L.; Saminarsih, D.S. Rebuilding to shape a better future: The role of young professionals in the public health workforce. Hum. Resour. Health 2021, 19, 82. [Google Scholar] [CrossRef] [PubMed]
- Yeager, V.A.; Beitsch, L.M.; Hasbrouck, L. A mismatch between the educational pipeline and public health workforce: Can it be reconciled? Public Health Rep. 2016, 131, 507–509. [Google Scholar] [CrossRef]
- Locke, R.; McGinty, M.; Guerrero Ramirez, G.; Sellers, K. Attracting New Talent to the Governmental Public Health Workforce: Strategies for Improved Recruitment of Public Health Graduates. J. Public Health Manag. Pract. 2022, 28, E235–E243. [Google Scholar] [CrossRef]
- Institute of Medicine. Primary Care and Public Health: Exploring Integration to Improve Population Health. Available online: http://www.iom.edu/Reports/2012/Primary-Care-and-Public-Health.aspx (accessed on 19 August 2022).
- Halverson, P.K. Ensuring a Strong Public Health Workforce for the 21st Century: Reflections on PH WINS 2017. J. Public Health Manag. Pract. 2019, 25 (Suppl. 2), S1–S3. [Google Scholar] [CrossRef] [Green Version]
- Dean, H.D.; Myles, R.L.; Spears-Jones, C.; Bishop-Cline, A.; Fenton, K.A. A strategic approach to public health workforce development and capacity building. Am. J. Prev. Med. 2014, 47, S288–S296. [Google Scholar] [CrossRef] [Green Version]
- Bork, R.H.; Robins, M.; Schaffer, K.; Leider, J.P.; Castrucci, B.C. Workplace Perceptions and Experiences Related to COVID-19 Response Efforts Among Public Health Workers—Public Health Workforce Interests and Needs Survey. Morb. Mortal. Wkly. Rep. 2022, 71, 920–924. [Google Scholar] [CrossRef]
- Liss-Levinson, R. Continued Impact of COVID-19 on Public Sector Employee Job and Financial Outlook, Satisfaction, and Retention; MissionSquare Research Institute: Washington DC, USA, 2022. [Google Scholar]



{kind=link}
{kind=link}
| Domain | Theme | Definition | Example Quote |
|---|---|---|---|
| 1. Workforce gaps | 1.1 Local Infrastructure gaps | Structural or procedural deficiencies that participants identified within their local public health agencies | “do we have the current infrastructure and staffing to support all of that extra and ongoing work? I would say no, not at this time”. |
| 1.2 Workforce capability and capacity gaps | Needing professionals with appropriate skills (“capability”) and having enough staff to deliver services (“capacity”) | “one of the worries is, is that there won’t be enough people. And we may have to make some decisions about what we can and/or should do as a Health and Human Services Agency and what should the community to do”. | |
| 2. Workforce gaps impacts | 2.1 Poor operational outcomes due to workforce gaps | Consequences to operational outcomes at agencies due to unfilled staff positions | “One of the things that we have been struggling with for some time is staff, in particular nursing staff, public health nurses who are representative of the community we serve. So that is a huge gap to being able to deliver the most effective service”. |
| 2.2 Adverse personnel impacts | Negative effects experienced by participants’ agencies due to unfilled staff positions | “It is that stress level again and it’s being understaffed already and having to take on more and more and being asked. I shouldn’t say asked. I let everyone know I know they’re one individual and they can only do so much in one day. But the feeling when you’re passionate about the work that you do of wanting to take on more and more. And yet we don’t have the staff to cover it and so they try and cover it themselves. And then as was indicated just previously, the burnout that happens from that”. | |
| 3. Improvement strategies | 3.1 Retention strategies | Approaches taken by participants’ agencies to decrease workforce turnover | “assuring that there’s a balance…providing the opportunity to work from home has been a big driver” |
| 3.2 Systems-level changes | Modifications participants’ agencies made on a system-wide level resulting in agency improvement | “I think the other piece and the recovery period is looking at just sort of re-strengthening the reputation and integrity of public health”. | |
| 3.3 Recruitment/hiring strategies | New or innovative methods participants’ agencies used to recruit and hire staff for open positions | “We’ve been talking about this far, probably a little bit pre-COVID. We had started having these conversations and moved it little bits here and there, and just getting HR [human resources] to allow a little bit more flexibility and recognize that. I would say we’re still in the process of updating formally job descriptions and what’s listed as minimum quals. But having those substitutions and things”. |
| Workforce Gaps | Before COVID-19 | Increased (during or after) COVID-19 | ||
|---|---|---|---|---|
| n | % | n | % | |
| Local Infrastructure Gaps | 65 | 94% | 55 | 81% |
| Receiving authorizations for new positions | 48 | 70% | 24 | 35% |
| Long-term funding to retain employees | 40 | 58% | 36 | 53% |
| Ceilings for salary ranges | 31 | 45% | 30 | 44% |
| Length or complexity of hiring processes | 30 | 43% | 24 | 35% |
| Allowing flexible work arrangements | 22 | 32% | 15 | 22% |
| External restrictions on usage of funds | 18 | 26% | 11 | 16% |
| Providing office space, equipment, or supplies to new staff | 15 | 22% | 15 | 22% |
| Agency restrictions on usage of funds | 10 | 14% | 12 | 18% |
| Workforce Capability and Capacity Gaps | 64 | 93% | 64 | 94% |
| Small number of applicants | 53 | 77% | 54 | 79% |
| Staff capacity to supervise new employees | 31 | 45% | 36 | 53% |
| Lack of applicants representing BIPOC communities | 30 | 43% | 23 | 34% |
| Staff capacity to onboard new employees | 27 | 39% | 38 | 56% |
| Unskilled, untrained, or inexperienced applicants | 23 | 33% | 18 | 26% |
| Applicants lacking certifications, licenses or qualifications | 21 | 30% | 19 | 28% |
| Lack of applicants representing persons with disabilities | 17 | 25% | 16 | 24% |
| Lack of applicants representing LGBTQ communities | 13 | 19% | 14 | 21% |
| Ability to advertise job postings | 7 | 10% | 7 | 10% |
| Workforce Gaps Impacts | n | % |
|---|---|---|
| Poor Operational Outcomes from Workforce Gaps | 66 | 94% |
| Scaling back programs and services | 54 | 77% |
| Reorganization of programs and priorities | 49 | 70% |
| Neglect of important, non-time-sensitive activities | 38 | 54% |
| Inability to meet deadlines | 27 | 39% |
| Reliance on temporary staff/contractors | 25 | 36% |
| Reliance on volunteers | 24 | 34% |
| Suspension or withdrawal of funds by donors | 1 | 1% |
| Staff assuming additional responsibilities | 64 | 91% |
| Staff redistribution across program areas | 48 | 69% |
| Adverse Personnel Impacts | 60 | 86% |
| Staff burnout | 59 | 84% |
| Early retirements, voluntary separations, or inter-agency transfers | 28 | 40% |
| Delayed/postponed retirements | 14 | 20% |
| Other | 31 | 44% |
| Partnerships with external organizations | 28 | 40% |
| Multi-agency agreements with other health departments | 10 | 14% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kirkland, C.; Oldfield-Tabbert, K.; Karnik, H.; Orr, J.; Martin, S.; Leider, J.P. Public Health Workforce Gaps, Impacts, and Improvement Strategies from COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 13084. https://doi.org/10.3390/ijerph192013084
Kirkland C, Oldfield-Tabbert K, Karnik H, Orr J, Martin S, Leider JP. Public Health Workforce Gaps, Impacts, and Improvement Strategies from COVID-19. International Journal of Environmental Research and Public Health. 2022; 19(20):13084. https://doi.org/10.3390/ijerph192013084
Chicago/Turabian StyleKirkland, Chelsey, Kari Oldfield-Tabbert, Harshada Karnik, Jason Orr, Skky Martin, and Jonathon P. Leider. 2022. "Public Health Workforce Gaps, Impacts, and Improvement Strategies from COVID-19" International Journal of Environmental Research and Public Health 19, no. 20: 13084. https://doi.org/10.3390/ijerph192013084
APA StyleKirkland, C., Oldfield-Tabbert, K., Karnik, H., Orr, J., Martin, S., & Leider, J. P. (2022). Public Health Workforce Gaps, Impacts, and Improvement Strategies from COVID-19. International Journal of Environmental Research and Public Health, 19(20), 13084. https://doi.org/10.3390/ijerph192013084