
Polish Adaptation and Psychometric Properties of the Long- and Short-Form Interfaith Spirituality Scale

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analyses
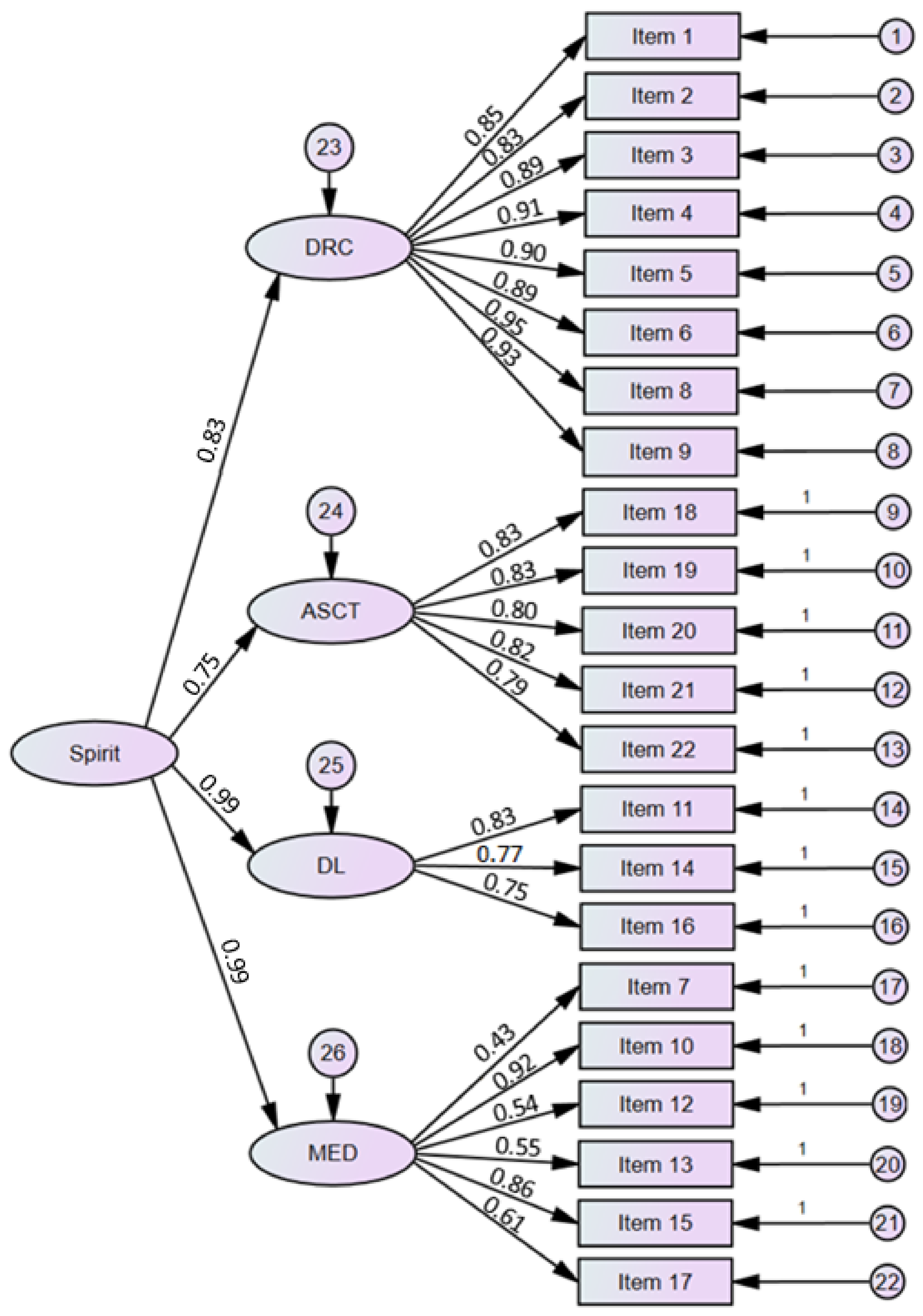
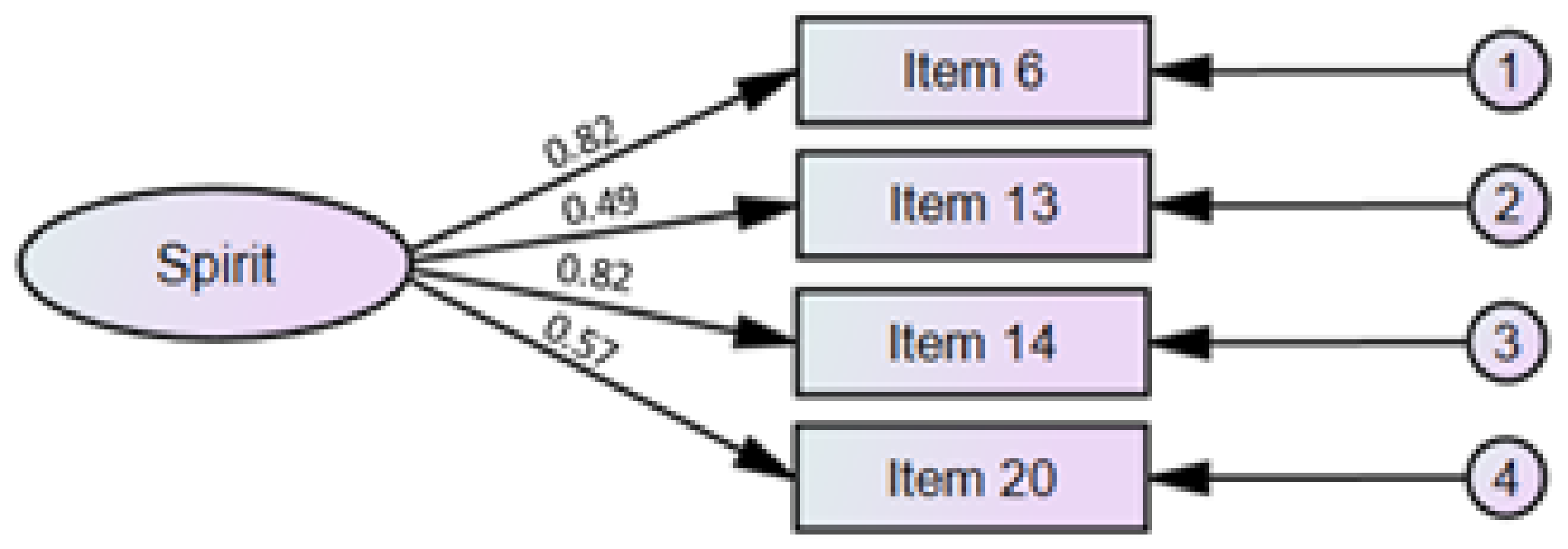
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Statements in Interfaith Spirituality Scale and Its Short Form in Polish
- Czułem (czułam), że jestem blisko Stwórcy (Boga lub bytu wyższego) [I felt close to the creator (or to a Supreme being/power)].
- Bezpośrednio odczułem (odczułam) obecność Stwórcy [I directly sensed God’s (or the Supreme being/power) presence].
- Poczułem (poczułam) więź z moim Stwórcą [I felt a bond with my creator (or the all-powerful force of being)].
- Relacja ze Stwórcą i poczucie samotranscendencji napędzają moje życie [My growing spiritual orientation (My direct relationship with the creator or the Supreme Being/power as I feel or see it and my ability to transcend myself) is a deep motive for me].
- Czuję się dobrze dzięki bezpośredniej i osobistej więzi ze Stwórcą [I feel a sense of well-being from my direct personal relationship with the creator (or to a Supreme being/power].
- Poczucie bezpośredniego kontaktu ze Stwórcą (Bogiem lub bytem wyższym) daje mi spokój ducha [My feeling of direct connection with my creator gives me a sense of inner peace].
- Odczuwam potrzebę refleksji nad życiem i egzystencją [I need to spend periods of time in private thought and reflection about life and existence].
- Czuję wewnętrzny spokój będąc blisko Stwórcy [I feel deep internal peace being so close to my creator].
- Staram się przybliżać do mojego Stwórcy [I seek to get closer to my creator].
- Miłość do Stwórcy wypełnia moje serce [I feel that my creator is closer to me than my heart (My aorta)].
- Wyczuwam miłość Stwórcy bezpośrednio i poprzez innych [I sense my creator’s love directly and through others].
- Obserwowanie piękna przyrody i kosmosu wzbogaciło mnie duchowo [I got enriched spiritually from observing cosmic and natural beauty].
- Rozmyślam nad cudem stworzenia i sensem istnienia [I meditate about the miracle of creation and the meaning of existence].
- Nie jestem w stanie opisać jak wielka jest moja miłości do Stwórcy [I have undescribed love to my creator].
- Rozmyślam nad sobą jako dziełem Stwórcy [I meditate about the creator’s work in myself].
- Istotą mojej duchowości jest bezinteresowna, nieskończona, prawdziwa i czysta miłość [The substance of my spirituality is divine love].
- Poszukiwanie wiedzy o stworzeniu i istnieniu to jeden z celów mojej egzystencji [To know about the creation and my being is one of my goals of existence].
- Ograniczanie skrajnego zamiłowania do rzeczy materialnych rozwija moją duchowość [Controlling my extreme passion for material things promote my spirituality].
- Niemarnowanie i poczucie zadowolenia z małych rzeczy sprzyjają mojej duchowości [Not wasting, and being satisfied with the little thing I may have, promote my spiritual feeling].
- Skromność, znajomość własnych wartości i ograniczeń wspierają moją duchowość [Modesty, being realistic and knowing the real value and limits of me promote my spiritual self].
- Umiejętność kontrolowania zachcianek i pożądania wspiera moją duchowość [The ability to control my wild desires and craves promotes my spiritual self].
- Zadowolenie z siebie, wdzięczność i cnotliwość (np. uprzejmość, sprawiedliwość, otwartość, prawość, mądrość i uczciwość) są częścią mojej duchowości [Being self-satisfied, grateful, and virtuous (e.g., being kind, fair, open-minded, having integrity, wisdom, and honesty) is part of my spiritual self].
References
- Rosmarin, D.H.; Koenig, H.G. Handbook of Spirituality, Religion, and Mental Health; Academic Press: London, UK, 2020. [Google Scholar]
- Hill, P.C.; Pargament, K.I.; Hood, R.W.; Mccullough, M.E.; Swyers, J.P.; Larson, D.B.; Zinnbauer, B.J. Conceptualizing Religion and Spirituality: Points of Commonality, Points of Departure. J. Theory Soc. Behav. 2000, 30, 51–77. [Google Scholar] [CrossRef]
- Pargament, K.; Feuille, M.; Burdzy, D. The Brief RCOPE: Current Psychometric Status of a Short Measure of Religious Coping. Religions 2011, 2, 51–76. [Google Scholar] [CrossRef] [Green Version]
- Villani, D.; Sorgente, A.; Iannello, P.; Antonietti, A. The Role of Spirituality and Religiosity in Subjective Well-Being of Individuals with Different Religious Status. Front. Psychol. 2019, 10, 1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kira, I.; Özcan, N.A.; Shuwiekh, H.; Kucharska, J.; Al-Huwailah, A.H.; Bujold-Bugeaud, M.; Kira, I.; Özcan, N.A.; Shuwiekh, H.; Kucharska, J.; et al. Mental Health Dynamics of Interfaith Spirituality in Believers and Non-Believers: The Two Circuit Pathways Model of Coping with Adversities: Interfaith Spirituality and Will-to Exist, Live and Survive. Psychology 2021, 12, 992–1024. [Google Scholar] [CrossRef]
- Alshraifeen, A.; Alnuaimi, K.; Al-Rawashdeh, S.; Ashour, A.; Al-Ghabeesh, S.; Al-Smadi, A. Spirituality, Anxiety and Depression Among People Receiving Hemodialysis Treatment in Jordan: A Cross-Sectional Study. J. Relig. Health 2020, 59, 2414–2429. [Google Scholar] [CrossRef] [PubMed]
- Braam, A.W.; Koenig, H.G. Religion, Spirituality and Depression in Prospective Studies: A Systematic Review. J. Affect. Disord. 2019, 257, 428–438. [Google Scholar] [CrossRef]
- Koenig, H.G. Research on Religion, Spirituality, and Mental Health: A Review. Can. J. Psychiatry 2009, 54, 283–291. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Berman, S.L. Spirituality and Adjustment: The Role of Identity. J. Spiritual. Ment. Health 2019, 22, 285–301. [Google Scholar] [CrossRef]
- Sherman, M.D.; Usset, T.; Voecks, C.; Irene Harris, J. Roles of Religion and Spirituality among Veterans Who Manage PTSD and Their Partners. Psychol. Relig. Spiritual. 2018, 10, 368–374. [Google Scholar] [CrossRef]
- Bartlett, S.J.; Piedmont, R.; Bilderback, A.; Matsumoto, A.K.; Bathon, J.M. Spirituality, Well-Being, and Quality of Life in People with Rheumatoid Arthritis. Arthritis Care Res. 2003, 49, 778–783. [Google Scholar] [CrossRef]
- Büssing, A.; Recchia, D.R.; Dienberg, T.; Surzykiewicz, J.; Baumann, K. Awe/Gratitude as an Experiential Aspect of Spirituality and Its Association to Perceived Positive Changes During the COVID-19 Pandemic. Front. Psychiatry 2021, 12, 642716. [Google Scholar] [CrossRef]
- Büssing, A.; Recchia, D.R.; Hübner, J.; Walter, S.; Büntzel, J.; Büntzel, J. Tumor Patients’ Fears and Worries and Perceived Changes of Specific Attitudes, Perceptions and Behaviors Due to the COVID-19 Pandemic Are Still Relevant. J. Cancer Res. Clin. Oncol. 2021, 147, 1673–1683. [Google Scholar] [CrossRef]
- McClain, C.S.; Rosenfeld, B.; Breitbart, W. Effect of Spiritual Well-Being on End-of-Life Despair in Terminally-Ill Cancer Patients. Lancet 2003, 361, 1603–1607. [Google Scholar] [CrossRef]
- Skalski, S.B.; Loichen, T.; Toussaint, L.; Patrycja, U.; Kwiatkowska, A.; Surzykiewicz, J. Relationships between Spirituality, Religious Fundamentalism and Ecology. Mediating Role of Right- Wing Authoritarianism. 2022; Manuscript Submitted. [Google Scholar]
- Kira, I.A.; Shuwiekh, H.A.M.; Alhuwailah, A.; Balaghi, D. Does COVID-19 Type III Continuous Existential Trauma Deplete the Traditional Coping, Diminish Health and Mental Health, and Kindle Spirituality?: An Exploratory Study on Arab Countries. J. Loss. Trauma 2021, 27, 297–317. [Google Scholar] [CrossRef]
- Puchalski, C.M. The Role of Spirituality in Health Care. Bayl. Univ. Med. Cent. Proc. 2017, 14, 352–357. [Google Scholar] [CrossRef]
- Antonovsky, H.; Sagy, S. The Development of a Sense of Coherence and Its Impact on Responses to Stress Situations. J. Soc. Psychol. 1986, 126, 213–225. [Google Scholar]
- Puchalski, C. Spirituality in Health: The Role of Spirituality in Critical Care. Crit. Care Clin. 2004, 20, 487–504. [Google Scholar] [CrossRef]
- de Blot, P. Religion and Spirituality. In Handbook of Spirituality and Business; Bouckaert, L., Zsolnai, L., Eds.; Palgrave Macmillan: London, UK, 2011; pp. 11–17. [Google Scholar] [CrossRef]
- Principe, W.H. Toward Defining Spirituality. SAGE J. 1983, 12, 127–141. [Google Scholar] [CrossRef]
- Bergman, Y.S.; Cohen-Fridel, S.; Shrira, A.; Bodner, E.; Palgi, Y. COVID-19 Health Worries and Anxiety Symptoms among Older Adults: The Moderating Role of Ageism. Int. Psychogeriatr. 2020, 32, 1371–1375. [Google Scholar] [CrossRef]
- Culliford, L. Routledge International Handbook of Spirituality in Society and the Professions. J. Study Spiritual. 2020, 10, 104–107. [Google Scholar] [CrossRef]
- Emmons, R.A. Emotion and Religion. In Handbook of the Psychology of Religion and Spirituality; Park, C.L., Ed.; Guilford Press: New York, NY, USA, 2005; pp. 235–252. [Google Scholar]
- Murgia, C.; Notarnicola, I.; Rocco, G.; Stievano, A. Spirituality in Nursing: A Concept Analysis. Nurs. Ethics 2020, 27, 1327–1343. [Google Scholar] [CrossRef]
- Paley, J. Spirituality and Nursing: A Reductionist Approach. Nurs. Philos. 2008, 9, 3–18. [Google Scholar] [CrossRef]
- Paloutziana, R.F.; Parkb, C.L. Religiousness and Spirituality: The Psychology of Multilevel Meaning-Making Behavior. Relig. Brain Behav. 2014, 5, 166–178. [Google Scholar] [CrossRef]
- Socha, P.M. Spirituality: Explicit and Implicit. Hindrances to the Scientific Status of Research on Spirituality? Rocz. Psychol. 2013, 16, 391–413. [Google Scholar]
- Elkins, D.N. Beyond Religion: Toward a Humanistic Spirituality. In The Handbook of Humanistic Psychology: Leading Edges in Theory, Research, and Practice; Schneider, K.J., Bugental, J.T., Pierson, J.F., Eds.; Sage: Thousand Oaks, CA, USA, 2001; pp. 201–212. [Google Scholar]
- Emmons, R.A. Spirituality: Recent Progress. In A Life Worth Living: Contributions to Positive Psychology; Csikszentmihalyi, M., Csikszentmihalyi, I., Eds.; Oxford University Press: New York, NY, USA, 2006; pp. 62–84. [Google Scholar]
- Pargament, K.I. The Psychology of Religion and Coping; Guilford Press: New York, NY, USA, 1997. [Google Scholar]
- Park, C.L. Religiousness/Spirituality and Health: A Meaning Systems Perspective. J. Behav. Med. 2007, 30, 319–328. [Google Scholar] [CrossRef]
- Zinnbauer, B.J.; Pargament, K.I. Religiousness and Spirituality. In Handbook of the Psychology of Religion and Spirituality; Zinnbauer, B.J., Pargament, K.I., Eds.; Guilford Press: New York, NY, USA, 2005; pp. 21–42. [Google Scholar]
- Hill, P.C.; Pargament, K.I. Advances in the Conceptualization and Measurement of Religion and Spirituality: Implications for Physical and Mental Health Research. Am. Psychol. 2003, 58, 64–74. [Google Scholar] [CrossRef] [Green Version]
- Cloninger, C.R. Feeling Good: The Science of Well-Being; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Emmons, R.A.; Paloutzian, R.F. The Psychology of Religion. Annu. Rev. Psychol. 2003, 54, 377–402. [Google Scholar] [CrossRef] [Green Version]
- Piedmont, R.L. Cross-Cultural Generalizability of the Spiritual Transcendence Scale to the Philippines: Spirituality as a Human Universal. Ment. Health. Relig. Cult. 2007, 10, 89–107. [Google Scholar] [CrossRef]
- Catlin, E.A.; Guillemin, J.H.; Thiel, M.M.; Hammond, S.; Wang, M.L.; O’Donnell, J. Spiritual and Religious Components of Patient Care in the Neonatal Intensive Care Unit: Sacred Themes in a Secular Setting. J. Perinatol. 2001, 21, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Grant, D.; O’Neil, K.; Stephens, L. Spirituality in the Workplace: New Empirical Directions in the Study of the Sacred. Sociol. Relig. 2004, 65, 265–283. [Google Scholar] [CrossRef]
- Harper, C.L.; Schulte-Murray, R.K. Religion and the Sociology of Culture: Exploring the Organizational Cultures of Two Midwestern Roman Catholic Dioceses. Rev. Relig. Res. 1998, 40, 101–119. [Google Scholar] [CrossRef]
- Howard, N.C.; Mcminn, M.R.; Bissell, L.D.; Faries, S.R.; Vanmeter, J.B. Spiritual Directors and Clinical Psychologists: A Comparison of Mental Health and Spiritual Values. J. Psychol. Theol. 2000, 28, 308–320. [Google Scholar] [CrossRef]
- Kira, I.; Shuwiekh, H.; Al-Huwailah, A.H.; Zidan, T.; Bujold-Bugeaud, M. Measuring Interfaith Spirituality: Initial Validation and Psychometrics. Psycholog. Relig. Spiritual. 2021, 13, 324–339. [Google Scholar] [CrossRef]
- Frankl, V.E. Self-Transcendence as a Human Phenomenon. J. Humanist Psychol. 2016, 6, 97–106. [Google Scholar] [CrossRef]
- Conn, W.E. The Desiring Self: Rooting Pastoral Counseling and Spiritual Direction in Self Transcendence; Paulist Press: Mahwah, NJ, USA, 1998. [Google Scholar]
- Sperry, L. Spirituality in Clinical Practice, 2nd ed.; Routledge: New York, NY, USA, 2012. [Google Scholar]
- Kira, I.; Özcan, N.A.; Kucharska, J.; Shuwiekh, H.; Kanaan, A.; Bujold-Bugeaud, M.; Kira, I.; Özcan, N.A.; Kucharska, J.; Shuwiekh, H.; et al. Measuring Interfaith Spirituality: Cross-Cultural Validation of Interfaith Spirituality Scale and Its Short Version. Psychology 2021, 12, 1960–1981. [Google Scholar] [CrossRef]
- Skowroński, B.; Bartoszewski, J. Scale of Spirituality–Design Description, and Psychometric Properties. Psychiatr. Psychoter. 2017, 13, 3–9. [Google Scholar]
- Sousa, V.D.; Rojjanasrirat, W. Translation, Adaptation and Validation of Instruments or Scales for Use in Cross-Cultural Health Care Research: A Clear and User-Friendly Guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Cichoń, E.; Kiejna, A.; Kokoszka, A.; Gondek, T.; Rajba, B.; Lloyd, C.E.; Sartorius, N. Validation of the Polish Version of WHO-5 as a Screening Instrument for Depression in Adults with Diabetes. Diabetes Res. Clin. Pract. 2020, 159, 107970. [Google Scholar] [CrossRef]
- Skalski, S. New Perspective Questionnaire to Measure Positive and Negative Trauma Effects. Polish Adaptation of the Short Form of the Changes in Outlook Questionnaire. Ann. Univ. Mariae Curie-Skłodowska Sect. J. Paedagog. 2019, 32, 307–317. [Google Scholar] [CrossRef]
- Preisendörfer, P. Umweltbewusstsein in Deutschland 1998. Ergebnisse Einer Repräsentativen Bevölkerungsumfrage Bundesministerium Für Umwelt; Naturschutz und Reaktorsicherheit: Bonn, Germany, 1998. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kokoszka, A.; Jastrzębski, A.; Obrębski, M. Psychometric Properties of the Polish Version of Patient Health Questionnaire-9. Psychiatria 2016, 13, 187–193. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling With AMOS: Basic Concepts, Applications, and Programming; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Lawshe, C. A Quantitative Approach to Content Validity. Pers. Psychol. 1975, 28, 563–575. [Google Scholar] [CrossRef]
- Brown, I. Exploring the Spiritual Dimension of School Health Education. Eta Sigma Gam. 1978, 10, 12–16. [Google Scholar]
- Adams, F. The Genuine Works of Hippocrates, [Trans. from the Greek, p. 299 (Aphorisms, I.1)]; Tindall & Cox: London, UK, 1939. [Google Scholar]
- Coward, D.D.; Reed, P.G. Self-Transcendence: A Resource for Healing at the End of Life. Issues Ment. Health Nurs. 2009, 17, 275–288. [Google Scholar] [CrossRef]
- Hodge, D.R. Spiritually Modified Cognitive Therapy: A Review of the Literature. Soc. Work 2006, 51, 157–166. [Google Scholar] [CrossRef] [Green Version]
- Jim, H.S.L.; Pustejovsky, J.E.; Park, C.L.; Danhauer, S.C.; Sherman, A.C.; Fitchett, G.; Merluzzi, T.V.; Munoz, A.R.; George, L.; Snyder, M.A.; et al. Religion, Spirituality, and Physical Health in Cancer Patients: A Meta-Analysis. Cancer 2015, 121, 3760–3768. [Google Scholar] [CrossRef] [Green Version]
- Sawatzky, R.; Ratner, P.A.; Chiu, L. A Meta-Analysis of the Relationship between Spirituality and Quality of Life. Soc. Indic. Res. 2005, 72, 153–188. [Google Scholar] [CrossRef]
- Aldwin, C.M.; Park, C.L.; Jeong, Y.J.; Nath, R. Differing Pathways between Religiousness, Spirituality, and Health: A Self-Regulation Perspective. Psychol. Relig. Spiritual. 2014, 6, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Seeman, T.E.; Dubin, L.F.; Seeman, M. Religiosity/Spirituality and Health: A Critical Review of the Evidence for Biological Pathways. Am. Psychol. 2003, 58, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Currier, J.M.; Drescher, K.D.; Holland, J.M.; Lisman, R.; Foy, D.W. Spirituality, Forgiveness, and Quality of Life: Testing a Mediational Model with Military Veterans with PTSD. Int. J. Psychol. Relig. 2016, 26, 167–179. [Google Scholar] [CrossRef]
- Dadfar, M.; Lester, D.; Turan, Y.; Beshai, J.A.; Unterrainer, H.F. Religious Spiritual Well-Being: Results from Muslim Iranian Clinical and Non-Clinical Samples by Age, Sex and Group. J. Relig. Spirit. Aging 2020, 33, 16–37. [Google Scholar] [CrossRef]
- Bosworth, H.B.; Park, K.S.; McQuoid, D.R.; Hays, J.C.; Steffens, D.C. The Impact of Religious Practice and Religious Coping on Geriatric Depression. Int. J. Geriatr. Psychiatry 2003, 18, 905–914. [Google Scholar] [CrossRef]
- Kendler, K.S.; Gardner, C.O.; Prescott, C.A. Religion, Psychopathology, and Substance Use and Abuse: A Multimeasure, Genetic-Epidemiologic Study. Am. J. Psychiatry 1997, 154, 322–329. [Google Scholar] [CrossRef]
- Krause, N. Religiosity and Self-Esteem among Older Adults. J. Gerontol. 1995, 50, 236–246. [Google Scholar] [CrossRef]
- Piedmont, R.L. Spiritual Transcendence and the Scientific Study of Spirituality-Document-Gale OneFile: Health and Medicine. J. Rehabil. 2001, 67, 4–11. [Google Scholar]
- Fisher, J. The Four Domains Model: Connecting Spirituality, Health and Well-Being. Religions 2011, 2, 17–28. [Google Scholar] [CrossRef]
- Saucier, G.; Skrzypińska, K. Spiritual But Not Religious? Evidence for Two Independent Dispositions. J. Pers. 2006, 74, 1257–1292. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| M (SD) | IFS | DRC | ASCT | DL | MED | IFS-4 | |
|---|---|---|---|---|---|---|---|
| Religious spirituality a | 21.80 (10.33) | 0.80 *** | 0.86 *** | 0.52 *** | 0.58 *** | 0.78 *** | 0.73 *** |
| Spirituality as expanding consciousness a | 13.75 (2.08) | 0.36 *** | 0.21 *** | 0.38 *** | 0.44 *** | 0.23 *** | 0.35 *** |
| Spirituality as searching for meaning a | 13.71 (3.87) | 0.40 *** | 0.28 *** | 0.38 *** | 0.59 *** | 0.26 *** | 0.46 *** |
| Spirituality as sensitivity to art a | 10.47 (3.18) | 0.37 *** | 0.18 *** | 0.45 *** | 0.48 *** | 0.22 *** | 0.36 *** |
| Spirituality as doing good a | 15.89 (2.83) | 0.39 *** | 0.28 *** | 0.38 *** | 0.39 *** | 0.33 *** | 0.36 *** |
| Sensitivity to inner beauty a | 20.34 (2.72) | 0.32 *** | 0.21 *** | 0.32 *** | 0.41 *** | 0.19 *** | 0.31 *** |
| Mental well-being | 13.95 (5.24) | 0.25 *** | 0.28 *** | 0.26 *** | 0.24 *** | 0.27 *** | 0.24 *** |
| PTG | 14. 64 (4.33) | 0.17 *** | 0.19 *** | 0.22 *** | 0.18 *** | 0.22 *** | 0.18 *** |
| Ecological behaviour | 56.38 (10.69) | 0.08 * | 0.08 * | 0.16 *** | 0.15 *** | 0.09 * | 0.08 * |
| PTSD | 11.59 (5.62) | –0.20 *** | –0.27 *** | –0.22 *** | –0.24 *** | –0.20 *** | –0.21 *** |
| Depressiveness | 9.98 (5.79) | –0.23 *** | –0.23 *** | –0.23 *** | –0.22 *** | –0.20 *** | –0.23 *** |
| Interfaith spirituality (IFS) | 41.00 (15.27) | - | |||||
| Direct connection with the creator (DRC) | 12.54 (6.49) | 0.89 *** | - | ||||
| Asceticism (ASCT) | 10.77 (4.31) | 0.82 *** | 0.55 *** | - | |||
| Divine love (DL) | 4.89 (2.36) | 0.89 *** | 0.86 *** | 0.62 *** | - | ||
| Meditation (MED) | 12.81 (4.35) | 0.88 *** | 0.65 *** | 0.74 *** | 0.69 *** | - | |
| Short form of the IFS (IFS-4) | 7.77 (2.92) | 0.94 *** | 0.79 *** | 0.81 *** | 0.87 *** | 0.83 *** | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surzykiewicz, J.; Skalski, S.B.; Niesiobędzka, M.; Toussaint, L.L.; Konaszewski, K. Polish Adaptation and Psychometric Properties of the Long- and Short-Form Interfaith Spirituality Scale. Int. J. Environ. Res. Public Health 2022, 19, 13274. https://doi.org/10.3390/ijerph192013274
Surzykiewicz J, Skalski SB, Niesiobędzka M, Toussaint LL, Konaszewski K. Polish Adaptation and Psychometric Properties of the Long- and Short-Form Interfaith Spirituality Scale. International Journal of Environmental Research and Public Health. 2022; 19(20):13274. https://doi.org/10.3390/ijerph192013274
Chicago/Turabian StyleSurzykiewicz, Janusz, Sebastian Binyamin Skalski, Małgorzata Niesiobędzka, Loren L. Toussaint, and Karol Konaszewski. 2022. "Polish Adaptation and Psychometric Properties of the Long- and Short-Form Interfaith Spirituality Scale" International Journal of Environmental Research and Public Health 19, no. 20: 13274. https://doi.org/10.3390/ijerph192013274
APA StyleSurzykiewicz, J., Skalski, S. B., Niesiobędzka, M., Toussaint, L. L., & Konaszewski, K. (2022). Polish Adaptation and Psychometric Properties of the Long- and Short-Form Interfaith Spirituality Scale. International Journal of Environmental Research and Public Health, 19(20), 13274. https://doi.org/10.3390/ijerph192013274