


Social Capital and Self-Rated Health: A Cross-Sectional Study among Rural Japanese Working Residents

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
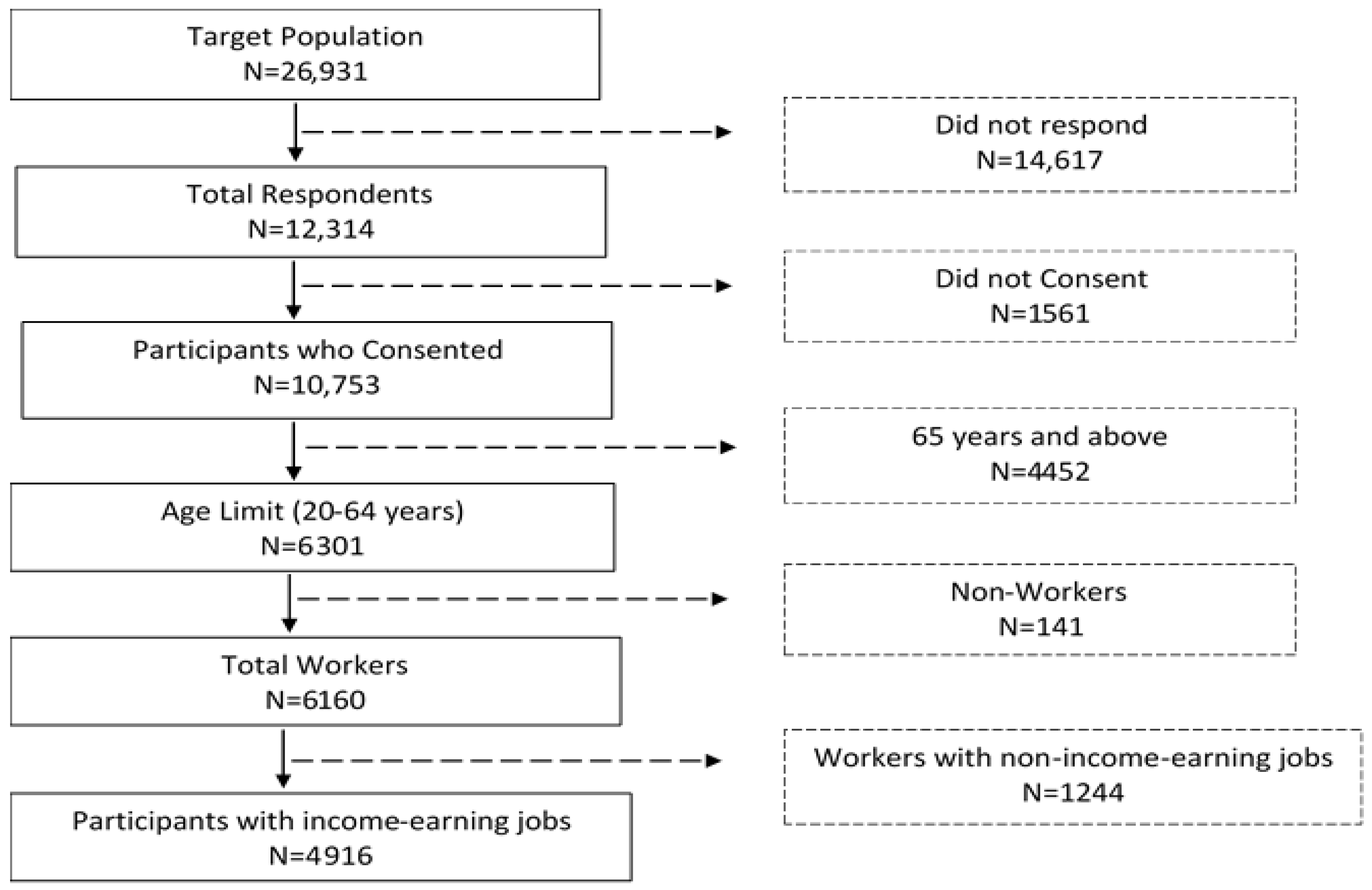
2.1. Data Collection
2.2. Measurement of Social Capital
2.3. Self-Rated Health
2.4. Covariates
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Demographic Characteristics of Respondents
3.2. Distribution of Respondents among the Social Capital Levels
3.3. Prevalence Ratios of Social Capital for Poor Self-Rated Health Respondents
3.4. Prevalence Ratios of Social Capital Dimensions for Poor Self-Rated Health Respondents
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Japan Institute for Labour Policy and Training. Labor Situation in Japan and Its Analysis: General Overview 2015/2016; Japan Institute for Labour Policy and Training: Tokyo, Japan, 2016; pp. 2–9. [Google Scholar]
- Bouchillon, B.C. Social networking for social capital: The declining value of presence for trusting with age. Behav. Inf. Technol. 2021, 41, 1425–1438. [Google Scholar] [CrossRef]
- Cortright, J. Less in Common. City Observatory. 2015. Available online: http://cityobservatory.org/wp-content/uploads/2015/06/CityObservatory_Less_In_Common.pdf (accessed on 25 August 2022).
- Gao, G. Americans Divided on How Much They Trust Their Neighbors|Pew Research Center. 2016. Available online: https://www.pewresearch.org/fact-tank/2016/04/13/americans-divided-on-how-much-they-trust-their-neighbors/ (accessed on 25 January 2022).
- Parker, K.; Menasce Horowitz, J.; Brown, A.; Fry, R.; Cohn, D.V.; Igielnik, R. How Urban, Suburban and Rural Residents Interact with Their Neighbors. 2018. Available online: http://www.pewsocialtrends.org/2018/05/22/how-urban-suburban-and-rural-residents-interact-with-their-neighbors/ (accessed on 25 January 2022).
- Tomono, M.; Yamauchi, T.; Suka, M.; Yanagisawa, H. Impact of overtime working and social interaction on the deterioration of mental well-being among full-time workers during the COVID-19 pandemic in Japan: Focusing on social isolation by household composition. J. Occup. Health 2021, 63, e12254. [Google Scholar] [CrossRef] [PubMed]
- Ferrie, J.E. Is job insecurity harmful to health? J. R. Soc. Med. 2001, 94, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Addae, E.A. The mediating role of social capital in the relationship between socioeconomic status and adolescent wellbeing: Evidence from Ghana. BMC Public Health 2020, 20, 20. [Google Scholar] [CrossRef]
- Kawachi, I.; Subramanian, I.V.; Kim, D. Social Capital and Health, 1st ed.; Springer: New York, NY, USA, 2008; Volume 3, pp. 1–291. [Google Scholar]
- Kawachi, I.; Berkman, L.F. Social Ties and Mental Health. J. Hered. 2001, 78, 458–467. [Google Scholar] [CrossRef] [Green Version]
- Putnam, R.D. What makes democracy work? Natl. Civ. Rev. 1993, 82, 101–107. [Google Scholar] [CrossRef]
- Szreter, S.; Woolcock, M. Health by association? Social capital, social theory, and the political economy of public health. Int. J. Epidemiol. 2004, 33, 650–667. [Google Scholar] [CrossRef]
- Yang, T.-C.; Jensen, L.; Haran, M. Social Capital and Human Mortality: Explaining the Rural Paradox with County-Level Mortality Data. Rural Sociol. 2011, 76, 347–374. [Google Scholar] [CrossRef] [Green Version]
- Schultz, J.; O’Brien, A.M.; Tadesse, B. Social capital and self-rated health: Results from the US 2006 social capital survey of one community. Soc. Sci. Med. 2008, 67, 606–617. [Google Scholar] [CrossRef]
- Ahmmad, Z.; Wen, M.; Li, K. Self-rated Health Disparities Among Asian Americans: Mediating Roles of Education Level and Household Income. J. Immigr. Minor. Health 2021, 23, 583–590. [Google Scholar] [CrossRef]
- Kim, B.J.; Harris, L.M. Social Capital and Self-Rated Health Among Older Korean Immigrants. J. Appl. Gerontol. 2013, 32, 997–1014. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wang, R.; Zhao, Y.; Ma, X.; Wu, M.; Yan, X.; He, J. The relationship between self-rated health and objective health status: A population-based study. BMC Public Health 2013, 13, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luckhaupt, S.E.; Alterman, T.; Li, J.; Calvert, G.M. Job Characteristics Associated With Self-Rated Fair or Poor Health Among U.S. Workers. Am. J. Prev. Med. 2017, 53, 216–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.-S.; Ju, Y.-S.; Paek, D.; Kim, H.; Jung-Choi, K. The Combined Effect of Long Working Hours and Low Job Control on Self-Rated Health. J. Occup. Environ. Med. 2018, 60, 475–480. [Google Scholar] [CrossRef]
- Bambra, C.; Lunau, T.; van der Wel, K.A.; Eikemo, T.A.; Dragano, N. Work, Health, and Welfare: The Association between Working Conditions, Welfare States, and Self-Reported General Health in Europe. Int. J. Health Serv. 2014, 44, 113–136. [Google Scholar] [CrossRef] [Green Version]
- Kwon, K.; Park, J.B.; Lee, K.-J.; Cho, Y.-S. Association between employment status and self-rated health: Korean working conditions survey. Ann. Occup. Environ. Med. 2016, 28, 43. [Google Scholar] [CrossRef] [Green Version]
- Honjo, K.; Iso, H.; Ikeda, A.; Yamagishi, K.; Saito, I.; Kato, T.; Yasuda, N.; Aoyagi, K.; Arima, K.; Sakata, K.; et al. Cross-Sectional Association Between Employment Status and Self-Rated Health Among Middle-Aged Japanese Women: The Influence of Socioeconomic Conditions and Work-Life Conflict. J. Epidemiol. 2020, 30, 396–403. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.; Bernell, S.L. The effect of self-employment on health, access to care, and health behavior. Health 2013, 05, 2116–2127. [Google Scholar] [CrossRef] [Green Version]
- Sverke, M.; Hellgren, J.; Näswall, K. No security: A meta-analysis and review of job insecurity and its consequences. J. Occup. Health Psychol. 2002, 7, 242–264. [Google Scholar] [CrossRef]
- Nishide, Y.; Yamauchi, N. Social Capital and Civic Activities in Japan. Nonprofit Rev. 2005, 5, 13–28. [Google Scholar] [CrossRef]
- De Silva, M.J.; Mckenzie, K.; Harpham, T.; Huttly, S.R.A. Social capital and mental illness: A systematic review. J. Epidemiol. Community Health 2005, 59, 619–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamano, T.; Fujisawa, Y.; Ishida, Y.; Subramanian, S.V.; Kawachi, I.; Shiwaku, K. Social Capital and Mental Health in Japan: A Multilevel Analysis. PLoS ONE 2010, 5, e13214. [Google Scholar] [CrossRef] [PubMed]
- Win, T.; Yamazaki, T.; Kanda, K.; Tajima, K.; Sokejima, S. Neighborhood social capital and sleep duration: A population based cross-sectional study in a rural Japanese town. BMC Public Health 2018, 18, 343. [Google Scholar] [CrossRef] [PubMed]
- Nishi, A.; Kawachi, I.; Shirai, K.; Hirai, H.; Jeong, S.; Kondo, K. Sex/Gender and Socioeconomic Differences in the Predictive Ability of Self-Rated Health for Mortality. PLoS ONE 2012, 7, e30179. [Google Scholar] [CrossRef] [PubMed]
- Osera, T.; Awai, M.; Kobayashi, M.; Tsutie, S.; Kurihara, N. Relationship between Self-Rated Health and Lifestyle and Food Habits in Japanese High School Students. Behav. Sci. 2017, 7, 71. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Guidelines on physical activity and sedentary behaviour. In Routledge Handbook of Youth Sport; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, T.; Nagata, S. Relationship between job stress and self-rated health among Japanese full-time occupational physicians. Environ. Health Prev. Med. 2005, 10, 227–232. [Google Scholar] [CrossRef]
- Yoo, K.-B.; Park, E.-C.; Jang, S.-Y.; Kwon, J.A.; Kim, S.J.; Cho, K.-H.; Choi, J.-W.; Kim, J.-H.; Park, S. Association between employment status change and depression in Korean adults. BMJ Open 2016, 6, e008570. [Google Scholar] [CrossRef] [Green Version]
- Bosmans, K.; Hardonk, S.; De Cuyper, N.; Vanroelen, C. Explaining the relation between precarious employment and mental well-being. A qualitative study among temporary agency workers. Work 2015, 53, 249–264. [Google Scholar] [CrossRef]
- Sapp, A.L.; Kawachi, I.; Sorensen, G.; LaMontagne, A.D.; Subramanian, S. Does Workplace Social Capital Buffer the Effects of Job Stress? A Cross-Sectional, Multilevel Analysis of Cigarette Smoking Among U.S. Manufacturing Workers. J. Occup. Environ. Med. 2010, 52, 740–750. [Google Scholar] [CrossRef]
- Thoits, P.A. Mechanisms Linking Social Ties and Support to Physical and Mental Health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [Green Version]
- Verhaeghe, P.-P.; Pattyn, E.; Bracke, P.; Verhaeghe, M.; Van De Putte, B. The association between network social capital and self-rated health: Pouring old wine in new bottles? Health Place 2011, 18, 358–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asao, Y.; Slater, G.; Seifer, H.; Valenzuela, A.; Michon, F.; Keizer, A. Non-Regular Employment-Issues and Challenges Common to the Major Developed Countries. JILPT Report; The Japan Institute for Labour Policy and Training: Tokyo, Japan, 2011. [Google Scholar]
- Tsurugano, S.; Inoue, M.; Yano, E. Precarious Employment and Health: Analysis of the Comprehensive National Survey in Japan. Ind. Health 2012, 50, 223–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, D.; Emeljanovas, A.; Mieziene, B.; Štefan, L.; Kawachi, I. How different contexts of social capital are associated with self-rated health among Lithuanian high-school students. Glob. Health Action 2018, 11, 1477470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azagba, S.; Sharaf, M.F. The effect of job stress on smoking and alcohol consumption. Health Econ. Rev. 2011, 1, 15. [Google Scholar] [CrossRef] [Green Version]
- Giordano, G.N.; Björk, J.; Lindström, M. Social capital and self-rated health—A study of temporal (causal) relationships. Soc. Sci. Med. 2012, 75, 340–348. [Google Scholar] [CrossRef]
- Granovetter, M.S. The Strength of Weak Ties. Am. J. Soc. 1973, 78, 1360–1380. [Google Scholar] [CrossRef] [Green Version]
- Viitala, R.; Kantola, J. Temporary agency workers shake a work community: A social capital perspective. Empl. Relat. 2016, 38, 147–162. [Google Scholar] [CrossRef]


{kind=link}
| Regular Employees | Non-Regular Employees | Self-Employed | |||
|---|---|---|---|---|---|
| (n = 2574) | (n = 1641) | (n = 701) | |||
| Characteristics | n (%) | n (%) | n (%) | p-Value | |
| Social capital | |||||
| Low | 132 (5.2) | 96 (5.9) | 32 (4.6) | <0.001 | |
| Medium | 1071 (42.0) | 615 (37.8) | 202 (29.1) | ||
| High | 1346 (52.8) | 914 (56.2) | 461 (66.3) | ||
| Gender | |||||
| Men | 1689 (66.8) | 411 (25.4) | 406 (58.7) | <0.001 | |
| Women | 840 (33.2) | 1208 (74.6) | 286 (41.3) | ||
| Age (Years) | |||||
| 20–24 | 133 (5.2) | 84 (5.1) | 1 (0.1) | <0.001 | |
| 25–34 | 492 (19.1) | 220 (13.4) | 34 (4.9) | ||
| 35–44 | 697 (27.1) | 376 (22.9) | 136 (19.4) | ||
| 45–54 | 744 (28.9) | 407 (24.8) | 197 (28.1) | ||
| 55–64 | 508 (19.7) | 554 (33.8) | 333 (47.5) | ||
| Educational level | |||||
| Low | 1402 (55.0) | 1021 (62.8) | 415 (59.6) | <0.001 | |
| Medium | 544 (21.3) | 397 (24.4) | 148 (21.3) | ||
| High | 605 (23.7) | 209 (12.8) | 133 (19.1) | ||
| Occupation | |||||
| Blue-collar | 1083 (42.5) | 493 (31.2) | 319 (46.6) | <0.001 | |
| White-collar | 948 (37.2) | 688 (43.6) | 231 (33.7) | ||
| Others | 519 (20.4) | 397 (25.2) | 135 (19.7) | ||
| Annual Household Income (Million Yen) | |||||
| <2 | 32 (1.6) | 148 (12.1) | 49 (9.4) | <0.001 | |
| 2–3.99 | 281 (14.0) | 311 (25.5) | 129 (24.6) | ||
| 4–5.99 | 534 (26.5) | 346 (28.3) | 143 (27.3) | ||
| 6–7.99 | 501 (24.9) | 208 (17.0) | 82 (15.6) | ||
| >7.99 | 666 (33.1) | 209 (17.1) | 121 (23.1) | ||
| Marital Status | |||||
| Never married | 589 (23.0) | 267 (16.4) | 74 (10.6) | <0.001 | |
| Currently married | 1805 (70.4) | 1214 (74.5) | 581 (83.1) | ||
| Previously married | 170 (6.6) | 149 (9.1) | 44 (6.3) | ||
| Physical Activity | |||||
| Inactive | 2325 (91.3) | 1469 (90.6) | 612 (89.0) | 0.169 | |
| Active | 222 (8.7) | 153 (9.4) | 76 (11.0) | ||
| Smoking status | |||||
| Currently smokes | 770 (30.0) | 293 (17.9) | 180 (25.9) | <0.001 | |
| Smoked before | 702 (27.3) | 372 (22.8) | 248 (35.7) | ||
| Never smoked | 1096 (42.7) | 970 (59.3) | 267 (38.4) | ||
| Non-communicable disease | |||||
| Absent | 1263 (52.9) | 779 (51.7) | 308 (47.4) | 0.046 | |
| Present | 1126 (47.1) | 728 (48.3) | 342 (52.6) | ||
| BMI (kg/m2) | |||||
| Underweight | 173 (6.9) | 204 (12.9) | 39 (5.6) | <0.001 | |
| Normal | 1714 (68.6) | 1136 (71.6) | 465 (67.3) | ||
| Overweight | 513 (20.5) | 210 (13.2) | 160 (23.2) | ||
| Obese | 97 (3.9) | 37 (2.3) | 27 (3.9) | ||
| Self-rated health | |||||
| Poor | 559 (21.8) | 368 (22.5) | 144 (20.5) | 0.579 | |
| Good | 2010 (78.2) | 1269 (77.5) | 557 (79.5) | ||
| Regular Employees | Non-Regular Employees | Self-Employed | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Social Capital | ||||||||||
| Low | Medium | High | Low | Medium | High | Low | Medium | High | ||
| (n = 132) | (n = 1071) | (n = 1346) | (n = 96) | (n = 615) | (n = 914) | (n = 32) | (n = 202) | (n = 461) | ||
| Characteristics | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Self-rated health | ||||||||||
| Poor | 46 (34.8) | 255 (23.9) | 251 (18.7) | 39 (40.6) | 147 (24.0) | 174 (19.1) | 10 (31.2) | 47 (23.3) | 86 (18.7) | |
| Good | 86 (65.2) | 813 (76.1) | 1093 (81.3) | 57 (59.4) | 465 (76.0) | 739 (80.9) | 22 (68.8) | 155 (76.7) | 375 (81.3) | |
| Gender | ||||||||||
| Men | 79 (61.2) | 670 (63.7) | 922 (69.6) | 24 (25.0) | 161 (26.6) | 219 (24.3) | 20 (62.5) | 125 (63.1) | 255 (55.9) | |
| Women | 50 (38.8) | 381 (36.3) | 402 (30.4) | 72 (75.0) | 445 (73.4) | 682 (75.7) | 12 (37.5) | 73 (36.9) | 201 (44.1) | |
| Age (Years) | ||||||||||
| 20–24 | 15 (11.4) | 79 (7.4) | 34 (2.5) | 17 (17.7) | 45 (7.3) | 21 (2.3) | 0 (0.0) | 1 (0.5) | 0 (0.0) | |
| 25–34 | 40 (30.3) | 272 (25.4) | 175 (13.0) | 21 (21.9) | 118 (19.2) | 80 (8.8) | 0 (0.0) | 15 (7.4) | 18 (3.9) | |
| 35–44 | 36 (27.3) | 323 (30.2) | 333 (24.7) | 21 (21.9) | 143 (23.3) | 211 (23.1) | 7 (21.9) | 56 (27.7) | 73 (15.8) | |
| 45–54 | 21 (15.9) | 275 (25.7) | 442 (32.8) | 22 (22.9) | 141 (22.9) | 241 (26.4) | 9 (28.1) | 53 (26.2) | 133 (28.9) | |
| 55–64 | 20 (15.2) | 122 (11.4) | 362 (26.9) | 15 (15.6) | 168 (27.3) | 361 (39.5) | 16 (50.0) | 77 (38.1) | 237 (51.4) | |
| Educational level | ||||||||||
| Low | 69 (52.7) | 557 (52.7) | 760 (56.8) | 58 (61.1) | 366 (60.0) | 588 (64.8) | 22 (68.8) | 118 (59.3) | 271 (59.0) | |
| Medium | 36 (27.5) | 238 (22.5) | 265 (19.8) | 19 (20.0) | 157 (25.7) | 218 (24.0) | 3 (9.4) | 42 (21.1) | 103 (22.4) | |
| High | 26 (19.8) | 261 (24.7) | 314 (23.5) | 18 (18.9) | 87 (14.3) | 101 (11.1) | 7 (21.9) | 39 (19.6) | 85 (18.5) | |
| Occupation | ||||||||||
| Blue-collar | 46 (35.1) | 454 (42.8) | 570 (42.7) | 30 (34.5) | 197 (33.4) | 261 (29.3) | 13 (41.9) | 88 (44.4) | 216 (48.0) | |
| White-collar | 61 (46.6) | 411 (38.7) | 473 (35.4) | 39 (44.8) | 244 (41.4) | 404 (45.4) | 10 (32.3) | 65 (32.8) | 153 (34.0) | |
| Others | 24 (18.3) | 196 (18.5) | 293 (21.9) | 18 (20.7) | 149 (25.3) | 225 (25.3) | 8 (25.8) | 45 (22.7) | 81 (18.0) | |
| Annual Household Income (Million Yen) | ||||||||||
| <2 | 2 (2.3) | 13 (1.6) | 17 (1.5) | 20 (30.3) | 57 (13.0) | 67 (9.5) | 4 (18.2) | 14 (9.1) | 30 (8.7) | |
| 2–3.99 | 18 (20.5) | 138 (17.2) | 122 (10.9) | 19 (28.8) | 123 (28.0) | 166 (23.4) | 5 (22.7) | 38 (24.7) | 86 (24.9) | |
| 4–5.99 | 25 (28.4) | 216 (26.9) | 293 (26.3) | 6 (9.1) | 129 (29.4) | 210 (29.7) | 2 (9.1) | 43 (27.9) | 97 (28.0) | |
| 6–7.99 | 19 (21.6) | 193 (24.1) | 286 (25.6) | 13 (19.7) | 64 (14.6) | 130 (18.4) | 2 (9.1) | 22 (14.3) | 58 (16.8) | |
| >7.99 | 24 (27.3) | 242 (30.2) | 398 (35.7) | 8 (12.1) | 66 (15.0) | 135 (19.1) | 9 (40.9) | 37 (24.0) | 75 (21.7) | |
| Marital Status | ||||||||||
| Never married | 56 (42.4) | 320 (30.0) | 202 (15.1) | 35 (36.5) | 151 (24.7) | 77 (8.5) | 6 (18.8) | 23 (11.5) | 45 (9.8) | |
| Currently married | 62 (47.0) | 668 (62.7) | 1062 (79.1) | 47 (49.0) | 392 (64.1) | 768 (84.8) | 25 (78.1) | 161 (80.5) | 393 (85.2) | |
| Previously married | 14 (10.6) | 78 (7.3) | 78 (5.8) | 14 (14.6) | 69 (11.3) | 61 (6.7) | 1 (3.1) | 16 (8.0) | 23 (5.0) | |
| Physical Activity | ||||||||||
| Inactive | 123 (96.1) | 979 (92.2) | 1201 (90.0) | 91 (95.8) | 548 (90.3) | 820 (90.5) | 27 (87.1) | 184 (91.5) | 397 (87.8) | |
| Active | 5 (3.9) | 83 (7.8) | 134 (10.0) | 4 (4.2) | 59 (9.7) | 86 (9.5) | 4 (12.9) | 17 (8.5) | 55 (12.2) | |
| Smoking status | ||||||||||
| Currently smokes | 38 (29.0) | 350 (32.8) | 374 (27.8) | 28 (29.5) | 119 (19.4) | 141 (15.5) | 9 (28.1) | 59 (29.4) | 110 (24.1) | |
| Smoked before | 33 (25.2) | 230 (21.6) | 429 (31.9) | 17 (17.9) | 138 (22.5) | 212 (23.3) | 11 (34.4) | 80 (39.8) | 153 (33.6) | |
| Never smoked | 60 (45.8) | 487 (45.6) | 542 (40.3) | 50 (52.6) | 357 (58.1) | 558 (61.3) | 12 (37.5) | 62 (30.8) | 193 (42.3) | |
| Non-communicable disease | ||||||||||
| Absent | 63 (51.6) | 576 (58.1) | 608 (48.5) | 47 (52.2) | 302 (53.1) | 425 (50.8) | 16 (51.6) | 102 (55.7) | 189 (43.9) | |
| Present | 59 (48.4) | 416 (41.9) | 646 (51.5) | 43 (47.8) | 267 (46.9) | 411 (49.2) | 15 (48.4) | 81 (44.3) | 242 (56.1) | |
| BMI (kg/m2) | ||||||||||
| Underweight | 13 (10.1) | 92 (8.9) | 66 (5.0) | 19 (20.2) | 91 (15.3) | 94 (10.6) | 4 (12.5) | 7 (3.5) | 28 (6.2) | |
| Normal | 80 (62.0) | 707 (68.5) | 913 (69.4) | 57 (60.6) | 406 (68.5) | 664 (74.9) | 16 (50.0) | 146 (73.0) | 299 (66.0) | |
| Overweight | 28 (21.7) | 196 (19.0) | 285 (21.7) | 16 (17.0) | 76 (12.8) | 115 (13.0) | 12 (37.5) | 37 (18.5) | 110 (24.3) | |
| Obese | 8 (6.2) | 37 (3.6) | 51 (3.9) | 2 (2.1) | 20 (3.4) | 14 (1.6) | 0 (0.0) | 10 (5.0) | 16 (3.5) | |
| Crude Model | Model 1 a | Model 2 b | Model 3 c | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% C.I. for OR | OR | 95% C.I. for OR | OR | 95% C.I. for OR | OR | 95% C.I. for OR | |||||
| Lower | Upper | Lower | Upper | Lower | Upper | Lower | Upper | |||||
| Social capital | ||||||||||||
| Regular Employees | ||||||||||||
| Low | Reference | Reference | Reference | Reference | ||||||||
| Medium | 0.589 | 0.401 | 0.865 | 0.554 | 0.376 | 0.816 | 0.551 | 0.372 | 0.815 | 0.583 | 0.391 | 0.870 |
| High | 0.433 | 0.295 | 0.635 | 0.372 | 0.251 | 0.551 | 0.369 | 0.248 | 0.550 | 0.393 | 0.262 | 0.590 |
| Non-Regular Employees | ||||||||||||
| Low | Reference | Reference | Reference | Reference | ||||||||
| Medium | 0.481 | 0.308 | 0.751 | 0.433 | 0.274 | 0.686 | 0.471 | 0.296 | 0.752 | 0.466 | 0.289 | 0.751 |
| High | 0.346 | 0.223 | 0.537 | 0.306 | 0.193 | 0.484 | 0.341 | 0.213 | 0.546 | 0.339 | 0.209 | 0.550 |
| Self-Employed | ||||||||||||
| Low | Reference | Reference | Reference | Reference | ||||||||
| Medium | 0.659 | 0.291 | 1.489 | 0.699 | 0.307 | 1.593 | 0.838 | 0.361 | 1.949 | 0.727 | 0.301 | 1.756 |
| High | 0.506 | 0.231 | 1.108 | 0.507 | 0.230 | 1.116 | 0.598 | 0.266 | 1.344 | 0.490 | 0.211 | 1.137 |
| Crude Model | Model 1 a | Model 2 b | Model 3 c | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% C.I. for OR | OR | 95% C.I. for OR | OR | 95% C.I. for OR | OR | 95% C.I. for OR | ||||||
| Lower | Upper | Lower | Upper | Lower | Upper | Lower | Upper | ||||||
| Feeling of Fellowship | |||||||||||||
| Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.753 | 0.559 | 1.015 | 0.717 | 0.530 | 0.968 | 0.705 | 0.520 | 0.954 | 0.728 | 0.535 | 0.991 | |
| High | 0.650 | 0.496 | 0.851 | 0.569 | 0.430 | 0.753 | 0.567 | 0.427 | 0.754 | 0.590 | 0.441 | 0.788 | |
| Non-Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.687 | 0.471 | 1.002 | 0.655 | 0.447 | 0.959 | 0.705 | 0.478 | 1.040 | 0.718 | 0.482 | 1.069 | |
| High | 0.503 | 0.360 | 0.703 | 0.476 | 0.337 | 0.672 | 0.513 | 0.360 | 0.731 | 0.525 | 0.366 | 0.755 | |
| Self-Employed | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.671 | 0.528 | 0.853 | 0.657 | 0.516 | 0.836 | 0.660 | 0.518 | 0.841 | 0.667 | 0.522 | 0.853 | |
| High | 0.616 | 0.496 | 0.766 | 0.563 | 0.450 | 0.704 | 0.559 | 0.446 | 0.701 | 0.567 | 0.451 | 0.714 | |
| Social support | |||||||||||||
| Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.671 | 0.528 | 0.853 | 0.657 | 0.516 | 0.836 | 0.660 | 0.518 | 0.841 | 0.667 | 0.522 | 0.853 | |
| High | 0.616 | 0.496 | 0.766 | 0.563 | 0.450 | 0.704 | 0.559 | 0.446 | 0.701 | 0.567 | 0.451 | 0.714 | |
| Non-Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.694 | 0.507 | 0.950 | 0.679 | 0.495 | 0.933 | 0.716 | 0.519 | 0.986 | 0.727 | 0.525 | 1.007 | |
| High | 0.609 | 0.468 | 0.794 | 0.604 | 0.460 | 0.792 | 0.630 | 0.476 | 0.833 | 0.636 | 0.478 | 0.846 | |
| Self-Employed | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.487 | 0.285 | 0.833 | 0.485 | 0.282 | 0.832 | 0.453 | 0.261 | 0.787 | 0.450 | 0.253 | 0.799 | |
| High | 0.533 | 0.347 | 0.818 | 0.531 | 0.343 | 0.821 | 0.530 | 0.341 | 0.826 | 0.485 | 0.306 | 0.768 | |
| Cooperation | |||||||||||||
| Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.858 | 0.679 | 1.084 | 0.790 | 0.622 | 1.003 | 0.782 | 0.614 | 0.995 | 0.802 | 0.628 | 1.024 | |
| High | 0.659 | 0.524 | 0.828 | 0.566 | 0.444 | 0.721 | 0.558 | 0.436 | 0.715 | 0.568 | 0.442 | 0.730 | |
| Non-Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 1.068 | 0.799 | 1.427 | 1.033 | 0.770 | 1.386 | 1.079 | 0.800 | 1.455 | 1.081 | 0.797 | 1.467 | |
| High | 0.687 | 0.515 | 0.917 | 0.657 | 0.487 | 0.886 | 0.701 | 0.516 | 0.953 | 0.688 | 0.504 | 0.941 | |
| Self-Employed | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.554 | 0.324 | 0.945 | 0.523 | 0.304 | 0.899 | 0.524 | 0.301 | 0.914 | 0.506 | 0.283 | 0.906 | |
| High | 0.615 | 0.389 | 0.971 | 0.537 | 0.335 | 0.861 | 0.523 | 0.320 | 0.853 | 0.479 | 0.287 | 0.799 | |
| Reciprocity Norm | |||||||||||||
| Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.749 | 0.550 | 1.021 | 0.724 | 0.530 | 0.988 | 0.693 | 0.506 | 0.950 | 0.686 | 0.498 | 0.944 | |
| High | 0.631 | 0.468 | 0.849 | 0.602 | 0.446 | 0.813 | 0.594 | 0.439 | 0.804 | 0.600 | 0.441 | 0.816 | |
| Non-Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.829 | 0.581 | 1.184 | 0.811 | 0.565 | 1.162 | 0.850 | 0.590 | 1.225 | 0.877 | 0.605 | 1.272 | |
| High | 0.528 | 0.375 | 0.743 | 0.518 | 0.367 | 0.733 | 0.545 | 0.383 | 0.775 | 0.562 | 0.393 | 0.805 | |
| Self-Employed | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.876 | 0.483 | 1.586 | 0.879 | 0.483 | 1.602 | 0.850 | 0.460 | 1.572 | 0.774 | 0.409 | 1.464 | |
| High | 0.613 | 0.351 | 1.069 | 0.613 | 0.349 | 1.076 | 0.602 | 0.339 | 1.069 | 0.560 | 0.309 | 1.017 | |
| Perceived Neighbourhood Trust | |||||||||||||
| Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.657 | 0.511 | 0.845 | 0.639 | 0.496 | 0.823 | 0.639 | 0.495 | 0.824 | 0.653 | 0.504 | 0.846 | |
| High | 0.470 | 0.362 | 0.609 | 0.437 | 0.336 | 0.570 | 0.440 | 0.337 | 0.575 | 0.454 | 0.346 | 0.596 | |
| Non-Regular Employees | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.597 | 0.444 | 0.802 | 0.581 | 0.431 | 0.783 | 0.620 | 0.458 | 0.840 | 0.647 | 0.475 | 0.881 | |
| High | 0.446 | 0.328 | 0.606 | 0.435 | 0.319 | 0.595 | 0.459 | 0.333 | 0.631 | 0.468 | 0.339 | 0.648 | |
| Self-Employed | |||||||||||||
| Low | Reference | Reference | Reference | Reference | |||||||||
| Medium | 0.889 | 0.530 | 1.492 | 0.844 | 0.500 | 1.424 | 0.826 | 0.484 | 1.412 | 0.887 | 0.505 | 1.559 | |
| High | 0.559 | 0.333 | 0.939 | 0.526 | 0.311 | 0.890 | 0.534 | 0.313 | 0.910 | 0.577 | 0.330 | 1.009 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuurdor, E.D.-M.; Tanaka, H.; Kitajima, T.; Amexo, J.X.; Sokejima, S. Social Capital and Self-Rated Health: A Cross-Sectional Study among Rural Japanese Working Residents. Int. J. Environ. Res. Public Health 2022, 19, 14018. https://doi.org/10.3390/ijerph192114018
Kuurdor ED-M, Tanaka H, Kitajima T, Amexo JX, Sokejima S. Social Capital and Self-Rated Health: A Cross-Sectional Study among Rural Japanese Working Residents. International Journal of Environmental Research and Public Health. 2022; 19(21):14018. https://doi.org/10.3390/ijerph192114018
Chicago/Turabian StyleKuurdor, Elijah Deku-Mwin, Hirokazu Tanaka, Takumi Kitajima, Jennifer Xolali Amexo, and Shigeru Sokejima. 2022. "Social Capital and Self-Rated Health: A Cross-Sectional Study among Rural Japanese Working Residents" International Journal of Environmental Research and Public Health 19, no. 21: 14018. https://doi.org/10.3390/ijerph192114018
APA StyleKuurdor, E. D. -M., Tanaka, H., Kitajima, T., Amexo, J. X., & Sokejima, S. (2022). Social Capital and Self-Rated Health: A Cross-Sectional Study among Rural Japanese Working Residents. International Journal of Environmental Research and Public Health, 19(21), 14018. https://doi.org/10.3390/ijerph192114018