

Contextual Variables with an Impact on the Educational Inclusion of Students with Rare Diseases

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- School type: public (501 or 87.28%) or private–independent (73 or 12.72%). Public schools are fully funded by the regional education authority, but private–independent schools receive no public funding (private) or partial public funding (concertados) but are educationally independent.
- Location/setting: urban (347 or 60.45%) or rural (227 or 39.55%). Urban means towns or cities with more than 10,000 inhabitants, rural means towns with fewer than 10,000 inhabitants.
2.2. Instruments
2.3. Procedure and Data Analysis
3. Results
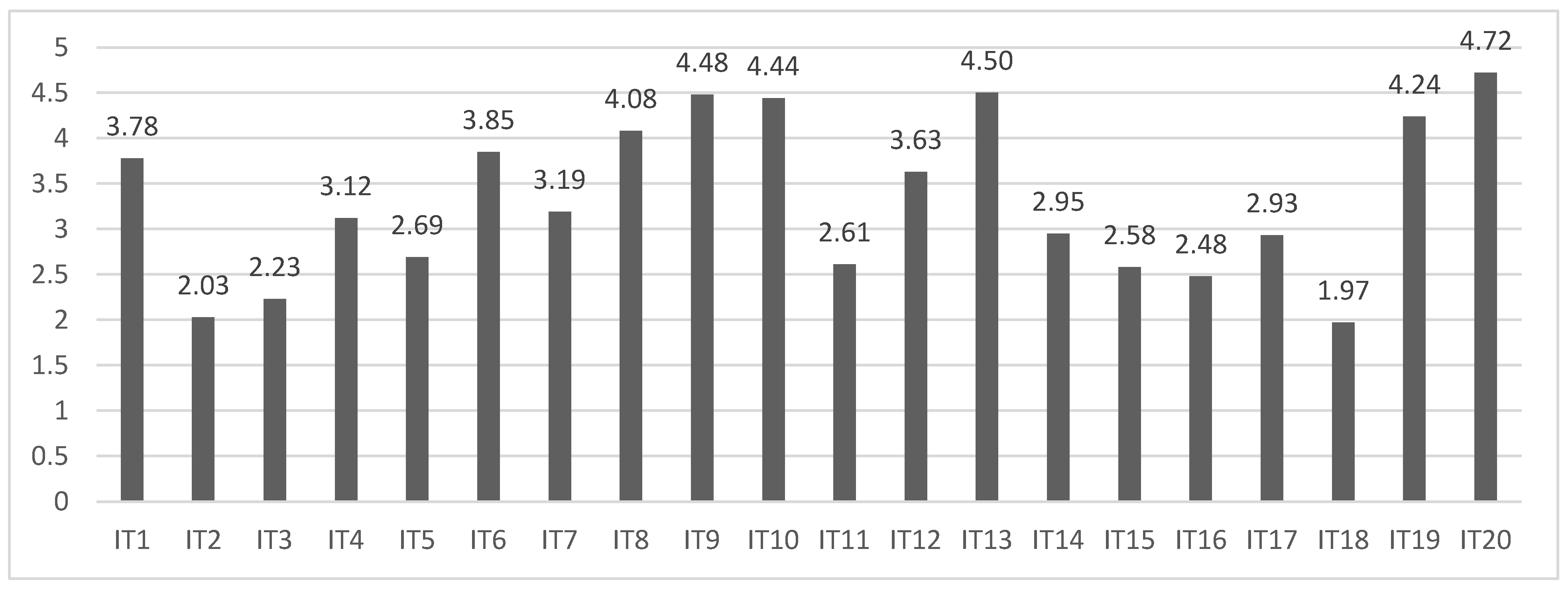
3.1. Teachers’ Knowledge and Perceptions According to School Type and Location/Setting
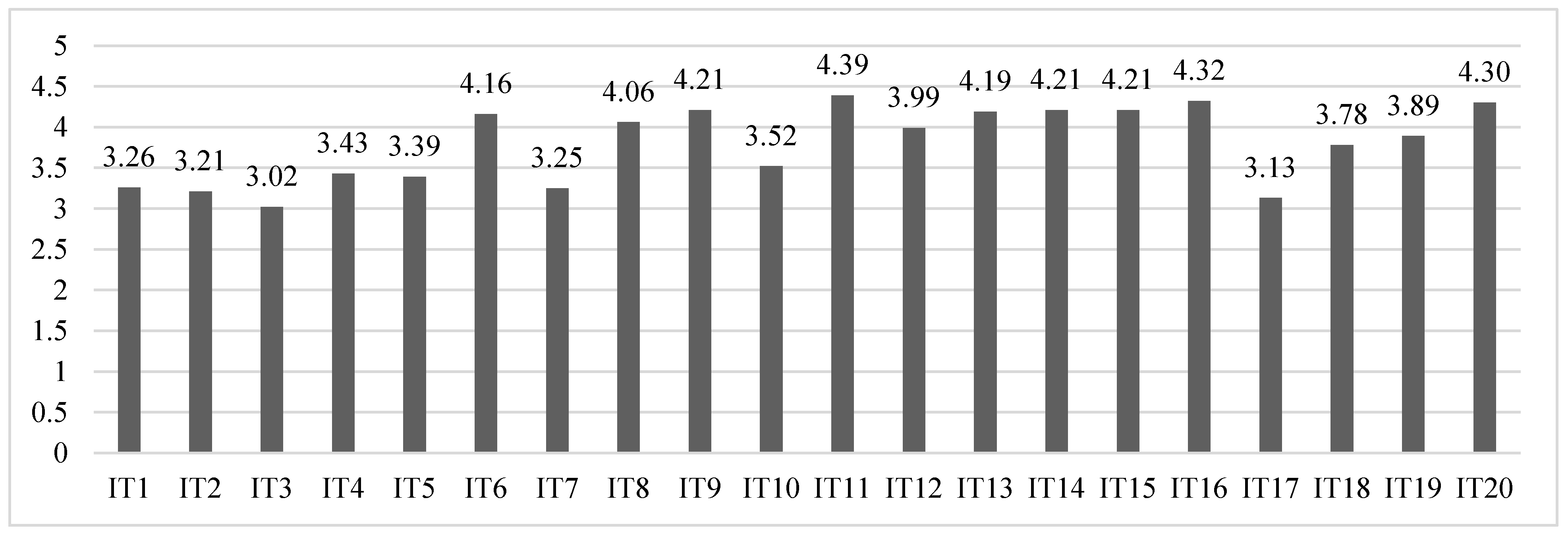
3.2. Results According to the Patient Advocacy Group Location/Setting
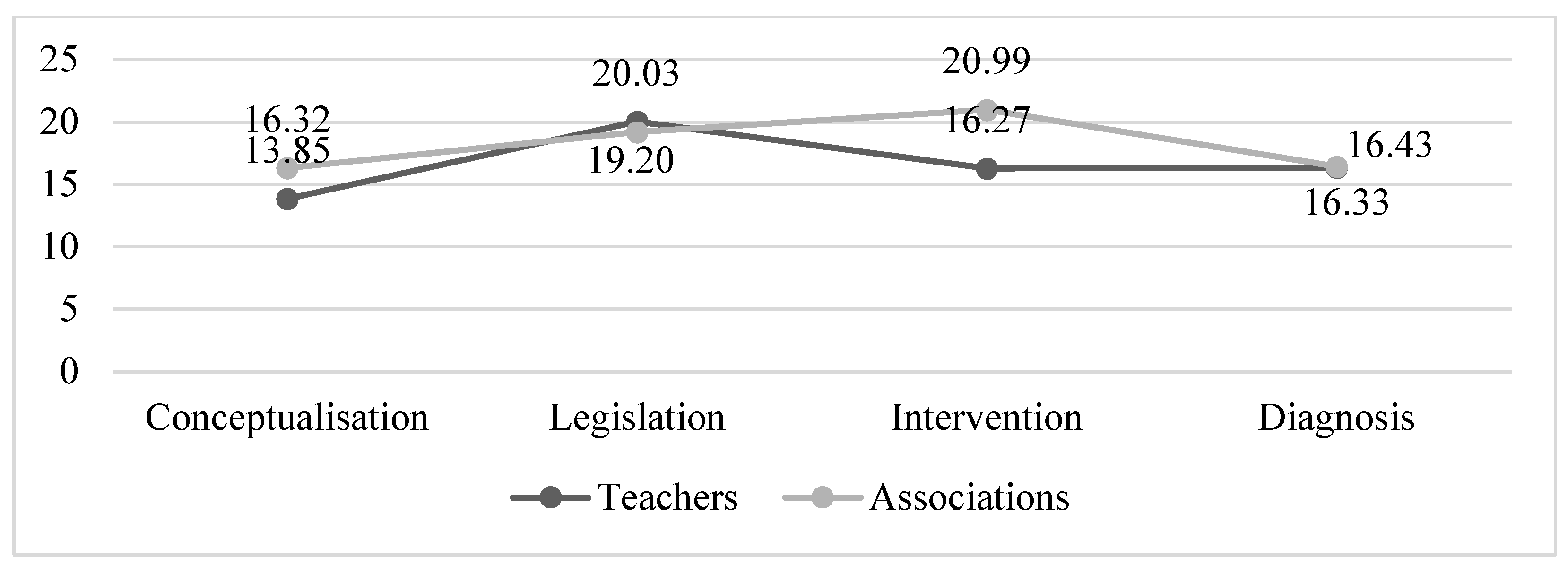
3.3. Comparison of Results between the Two Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chavarria, R.M.E.; Condoy, M.B.G.; Montesino, R.H.G. Diseño Universal del Aprendizaje e Inclusión en la Educación Básica en Ecuador. Alteridad 2019, 14, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Esteban-Guitart, M.; Rivas, M.J.; Pérez, R. Empathy and tolerance of diversity in an intercultural educative setting. Univ. Psychol. 2012, 11, 415–426. [Google Scholar] [CrossRef]
- Arnaiz, P. La educación inclusiva: Mejora escolar y retos para el siglo XXI. Part. Educ. 2019, 6, 41–54. [Google Scholar]
- Nilsen, S. Special education and general education—coordinated or separated? A study of curriculum planning for pupils with special educational needs. Int. J. Incl. Educ. 2016, 21, 205–217. [Google Scholar] [CrossRef]
- Gallegos, M. La Inclusión de las TIC en la Educación de Personas con Discapacidad: Relatos de Experiencias; Editorial Universitaria Abya-Yala: Quito, Ecuador, 2018; pp. 29–163. [Google Scholar]
- García-González, C.; Herrera-Seda, C.; Vanegas-Ortega, C. Competencias Docentes para una Pedagogía Inclusiva. Consideraciones a partir de la Experiencia con Formadores de Profesores Chilenos. RINACE Rev. Iberoam. Inv. Cam. Efic. Escol. 2018, 12, 149–167. [Google Scholar] [CrossRef] [Green Version]
- García-Perales, R.; Almeida, L. Programa de enriquecimiento para alumnado con alta capacidad: Efectos positivos para el currículum. Comunicar 2019, 60, 39–48. [Google Scholar] [CrossRef]
- López-Fernández, O. Emerging Health and Education Issues Related to Internet Technologies and Addictive Problems. Int. J. Environ. Res. Public Health 2021, 18, 321. [Google Scholar] [CrossRef]
- Vázquez, E.; Portela, I.; Domínguez, V. Attention to Diversity in Compulsory Secondary Education. J. Investig. Psicología Salud Educ. 2020, 10, 1176–1185. [Google Scholar] [CrossRef]
- Verger, S.; De La Iglesia, B.; Paz, B.; Negre, F. Informe de situación sobre la escolarización del alumnado con enfermedades poco frecuentes en las Islas Baleares. In Alumnado con Enfermedades poco Frecuentes y Escuela Inclusiva; Monzón, J., Aróstegui, I., Ozerinjaugeri, N., Eds.; Octaedro Editorial: Barcelona, Spain, 2017; pp. 119–148. [Google Scholar]
- Federación Española de Enfermedades Raras. Estudio Sobre Situación de Necesidades Sociosanitarias de las Personas con Enfermedades Raras en España. Estudio ENSERio Datos 2016–2017; FEDER: Madrid, Spain; CREER: Burgos, Spain, 2018. [Google Scholar]
- Caso-González, A.; Núñez-Rodríguez, J.; Nebot-Villacampa, M.J.; González-Pérez, Y.; Marín-Gorricho, R.; Leralta-González, C.; Obaldía-Alaña, C. Experiencia clínica con medicamentos huérfanos para enfermedades raras metabólicas. An. Pediatr. 2020, 96, 8–16. [Google Scholar] [CrossRef]
- Charco, J.M.; Barrio, T.; Eraña, H. Enfermedades priónicas: Historia, diversidad e importancia socioeconómica como paradigma de las Enfermedades Raras. Araucaria 2021, 23, 429–451. [Google Scholar] [CrossRef]
- Nguengang-Wakap, S.; Lambert, D.M.; Olry, A.; Rodwell, C.; Gueydan, C.; Lanneau, V.; Murphy, D.; Le Cam, Y.; Rath, A. Estimating cumulative point prevalence of rare diseases: Analysis of the Orphanet database. Eur. J. Hum. Genet. EJHG 2020, 28, 165–173. [Google Scholar] [CrossRef]
- Valdez, R.; Ouyang, L.; Bolen, J. Public Health and Rare Diseases: Oxymoron No More. Prev. Chronic Dis. 2016, 13, E05. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfaro, A.; Negre, F. Análisis de las necesidades de información que presentan los docentes respecto a la atención educativa del alumnado con enfermedades raras. REIFOP. Rev. Electron. Interuniv. Form. Prof. 2019, 22, 175–195. [Google Scholar] [CrossRef]
- García-Perales, R.; Palomares-Ruiz, A.; Ordóñez-García, L.; García-Toledano, E. Rare Diseases in the Educational Field: Knowledge and Perceptions of Spanish Teachers. Int. J. Environ. Res. Public Health 2022, 19, 6057. [Google Scholar] [CrossRef] [PubMed]
- Arnaiz-Sánchez, P.; García, S.A.; García, C.M.C. Estudio de la percepción de los profesionales de la orientación educativa sobre las aulas abiertas en centros regulares de la región de Murcia (España). RELIEVE 2022, 9, 4–26. [Google Scholar] [CrossRef]
- Perales, R.G.; Fernández, C.J.; Ruiz, A.P. Seguimiento de un grupo de alumnos y alumnas con alta capacidad matemática. RIE. Rev. Investig. Educ. 2020, 38, 415–434. [Google Scholar] [CrossRef]
- Pelentsov, L.J.; Fielder, A.L.; Laws, T.A.; Esterman, A.J. The supportive care needs of parents with a child with a rare disease: Results of an online survey. BMC Fam. Pract. 2016, 17, 88. [Google Scholar] [CrossRef] [Green Version]
- García-Toledano, E.; Palomares-Ruiz, A.; Serrano-Marugán, I. Enfermedades raras que precisan respuesta social y educativa. In Investigación y Respuestas Socioeducativas del Profesorado en el Siglo XXI; Síntesis: Madrid, Spain, 2020; pp. 145–154. [Google Scholar]
- Collado-Sanchís, A.; Tárraga-Mínguez, R.; Lacruz-Pérez, I.; Sanz-Cervera, P. Analysis of teachers’ attitudes and perceived self-efficacy towards inclusive education. Educar 2020, 56, 509–523. [Google Scholar] [CrossRef]
- Pérez-Gutiérrez, R.; Casado-Muñoz, R.; Rodríguez-Conde, M. Evolución del profesorado de apoyo hacia la educación inclusiva: Una perspectiva autonómica en España. Rev. Complut. Educ. 2021, 32, 285–295. [Google Scholar] [CrossRef]
- Perlado, I.; Muñoz, Y.; Torrejo, J.C. Implicaciones de la formación del profesorado en aprendizaje cooperativo para la educación inclusiva. Prof. Rev. Curr. Form. Prof. 2019, 23, 128–151. [Google Scholar] [CrossRef] [Green Version]
- Quesada, M.I. Metodologías inclusivas y emergentes para la formación docente en inclusión educativa. Rev. Int. Apoyo Incl. Logop. Soc. Multicult. 2021, 7, 110–117. [Google Scholar] [CrossRef]
- Castañeda, L. Trazabilidad de los discursos sobre tecnología educativa: Los caminos de la influencia. RiiTE. Rev. Interuniv. Inv. Tecnol. Educ. 2021, 10, 1–8. [Google Scholar] [CrossRef]
- Cavus, N.; Sani, A.S.; Haruna, Y.; Lawan, A.A. Efficacy of Social Networking Sites for Sustainable Education in the Era of COVID-19: A Systematic Review. Sustainability 2021, 13, 808. [Google Scholar] [CrossRef]
- Alfaro, A. Creación de material de sensibilización sobre las enfermedades raras (ER) dirigido a la comunidad docente. Edutec. Rev. Electron. Tecnol. Educ. 2021, 77, 87–101. [Google Scholar] [CrossRef]
- Federación Española de Enfermedades Raras. Misión, Visión y Valores; FEDER: Madrid, Spain, 2022. [Google Scholar]
- United Nations. Plan of Action to Integrate Volunteering into the 2030 Agenda; United Nations: New York, NY, USA, 2022. [Google Scholar]
- European Union. European Solidarity Corps Guide; European Union: Brussels, Belgium, 2022. [Google Scholar]
- Linertová, R.; González-Guadarrama, J.; Serrano-Aguilar, P.; Posada-De-la-Paz, M.; Péntek, M.; Iskrov, G.; Ballester, M. Schooling of Children with Rare Diseases and Disability in Europe. Int. J. Disab. Develop. Educ. 2019, 66, 362–373. [Google Scholar] [CrossRef]
- Cortes Generales. Ley 45/2015, de 14 de Octubre, de Voluntariado. Available online: https://cutt.ly/hL0sOaB (accessed on 1 September 2022).
- Friendlander, L.; Vincent, M.; Berdal, A.; Cormier-Daire, V.; Lyonnet, S.; Garcelon, N. Consideration of oral health in rare disease expertise centres: A retrospective study on 39 rare diseases using text mining extraction method. Inf. Period. Orphanet. Ser. Enferm. Raras 2022, 17, 317. [Google Scholar] [CrossRef]
- Ministerio de Educación y Formación Profesional. Estadísticas no Universitarias. Available online: https://cutt.ly/bGGRbeB (accessed on 15 September 2022).
- Esteban, G.; Ruano, M.; Motero, I. The quality of life in the relatives of Wolfram’s syndrome patients. Eur. J. Investig. Health Psychol. Educ. 2015, 5, 89–97. [Google Scholar] [CrossRef]
- Shamionov, R.; Grigoryeva, M.; Grinina, E.; Sozonnik, A. Characteristics of Academic Adaptation and Subjective Well-Being in University Students with Chronic Diseases. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 816–831. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NY, USA, 1988. [Google Scholar]
- Pélissier, A.; Wallut, L.; Giot, G.; Domenighetti, L.; Demougeot, L.; Faivre, L. Access to social services for undiagnosed rare disease patients in France: A pilot study. Eur. J. Med. Genet. 2022, 65, 104494. [Google Scholar] [CrossRef]
- Reinhard, C.; Bachoud-Lévi, A.-C.; Bäumer, T.; Bertini, E.; Brunelle, A.; Buizer, A.I.; Federico, A.; Gasser, T.; Groeschel, S.; Hermanns, S.; et al. The European Reference Network for Rare Neurological Diseases. Front. Neurol. 2021, 11, 616569. [Google Scholar] [CrossRef]
- Heuyer, T.; Pavan, S.; Vicard, C. The health and life path of rare disease patients: Results of the 2015 French barometer. PROMs. Patient Relat. Outcome Meas. 2017, 8, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Dugas, E.; Rollin, Z.; Sivilotti, L.; Dugas, K. Action Research with People Being Treated for Cancer of a Rare Disease: Health Mediation Central to Their Experiences and Their Inclusion. In Global Handbook of Health Promotion Research; Potvin, L., Jourdan, D., Eds.; Springer: New York, NY, USA, 2022; p. 1. [Google Scholar]
- Ahedo, Y.; Cabrejas, M.; Santamaría, A. Enfermedades Raras en la Escuela: Guía de Apoyo; Centro de Referencia Estatal de Atención a Personas con Enfermedades Raras y sus Familias: Burgos, Spain, 2021; Available online: https://cutt.ly/3AqfSa5 (accessed on 22 September 2022).
- Carrión, J.; Pino-Ramírez, G.; Males, A. Perfil Organizacional del Movimiento Asociativo de las Enfermedades Raras en Iberoamérica. Intr. Persp. Rev. Trabajo Soc. 2019, 9, 72–94. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Dimension | Items |
|---|---|
| Conceptualisation |
|
| |
| |
| |
| |
| Legislation |
|
| |
| |
| |
| |
| Intervention |
|
| |
| |
| |
| |
| Diagnosis |
|
| |
| |
| |
|
| Dimension | Items |
|---|---|
| Conceptualisation |
|
| |
| |
| |
| |
| Legislation |
|
| |
| Legislation |
|
| |
| |
| Intervention |
|
| |
| |
| |
| |
| Diagnosis |
|
| |
| |
| |
|
| Statistics | Indexes | |
|---|---|---|
| Teachers | Associations | |
| Cronbach’s Alpha | Between 0.79 and 0.94 | Between 0.77 and 0.88 |
| Content validity | Between 0.77 and 0.94 | Between 0.79 and 0.86 |
| Kappa Index | 0.88 | 0.86 |
| Exploratory factor analysis (EFA): | ||
| KMO | 0.94 | 0.82 |
| Bartlett’s sphericity test | 7699.08 | 1838.05 |
| Significance | p < 0.001 | p < 0.001 |
| Percentage of total variance explained | 68.49% | 65.04% |
| Factorial structure | 4 factors | 4 factors |
| Confirmatory factor analysis (CFA): | ||
| CMIN | 32.48 | 38.23 |
| p | 0.09 | 0.08 |
| RMSEA | 0.05 | 0.04 |
| CFI | 0.95 | 0.93 |
| TLI | 0.94 | 0.92 |
| Factorial structure | 4 factors | 4 factors |
| IT/D | Ownership | t | df | p | d | |||
|---|---|---|---|---|---|---|---|---|
| Public | Private–Independent | |||||||
| M | SD | M | SD | |||||
| IT1 | 3.86 | 1.07 | 3.23 | 1.21 | 4.56 | 572 | <0.001 *** | 0.57 |
| IT2 | 2.05 | 1.12 | 1.88 | 1.03 | 1.27 | 572 | 0.203 | 0.16 |
| IT3 | 2.28 | 1.29 | 1.92 | 1.13 | 2.24 | 572 | 0.025 * | 0.28 |
| IT4 | 3.15 | 1.26 | 2.90 | 1.17 | 1.57 | 572 | 0.117 | 0.20 |
| IT5 | 2.70 | 1.34 | 2.63 | 1.38 | 0.43 | 572 | 0.667 | 0.05 |
| D1 | 14.04 | 4.69 | 12.56 | 4.93 | 2.50 | 572 | 0.013 * | 0.31 |
| IT6 | 3.90 | 1.17 | 3.56 | 1.24 | 2.26 | 572 | 0.024 * | 0.28 |
| IT7 | 3.27 | 1.44 | 2.60 | 1.57 | 3.67 | 572 | <0.001 *** | 0.46 |
| IT8 | 4.12 | 1.08 | 3.79 | 1.10 | 2.39 | 572 | 0.017 * | 0.30 |
| IT9 | 4.55 | 0.74 | 3.99 | 1.10 | 5.64 | 572 | <0.001 *** | 0.71 |
| IT10 | 4.49 | 0.81 | 4.05 | 1.09 | 4.13 | 572 | <0.001 *** | 0.52 |
| D2 | 20.33 | 3.93 | 18.00 | 4.66 | 4.62 | 572 | <0.001 *** | 0.58 |
| IT11 | 2.59 | 1.53 | 2.75 | 1.41 | 0.84 | 572 | 0.398 | 0.11 |
| IT12 | 3.71 | 1.44 | 3.07 | 1.53 | 3.53 | 572 | <0.001 *** | 0.44 |
| IT13 | 4.58 | 0.79 | 3.93 | 1.28 | 6.01 | 572 | <0.001 *** | 0.75 |
| IT14 | 2.99 | 1.33 | 2.67 | 1.41 | 1.91 | 572 | 0.056 | 0.24 |
| IT15 | 2.63 | 1.42 | 2.26 | 1.48 | 2.05 | 572 | 0.041 * | 0.26 |
| D3 | 16.50 | 5.22 | 14.68 | 6.31 | 2.70 | 572 | 0.007 ** | 0.34 |
| IT16 | 2.52 | 1.22 | 2.22 | 1.23 | 1.97 | 572 | 0.050 | 0.25 |
| IT17 | 2.98 | 1.31 | 2.56 | 1.34 | 2.53 | 572 | 0.012 * | 0.32 |
| IT18 | 1.98 | 1.16 | 1.85 | 1.08 | 0.93 | 572 | 0.350 | 0.12 |
| IT19 | 4.35 | 1.03 | 3.48 | 1.50 | 6.28 | 572 | <0.001 *** | 0.79 |
| IT20 | 4.81 | 0.56 | 4.11 | 1.20 | 8.36 | 572 | <0.001 *** | 1.05 |
| D4 | 16.64 | 3.93 | 14.22 | 5.40 | 4.67 | 572 | <0.001 *** | 0.58 |
| Total | 67.52 | 15.63 | 59.47 | 19.70 | 3.97 | 572 | <0.001 *** | 0.50 |
| IT/D | Location/Setting | t | df | p | d | |||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | |||||||
| M | SD | M | SD | |||||
| IT1 | 3.75 | 1.14 | 3.81 | 1.06 | −0.66 | 572 | 0.508 | 0.06 |
| IT2 | 2.11 | 1.17 | 1.91 | 1.01 | 2.09 | 572 | 0.037 * | 0.18 |
| IT3 | 2.23 | 1.28 | 2.22 | 1.27 | 0.08 | 572 | 0.936 | 0.01 |
| IT4 | 3.14 | 1.23 | 3.08 | 1.27 | 0.54 | 572 | 0.590 | 0.05 |
| IT5 | 2.72 | 1.33 | 2.66 | 1.36 | 0.53 | 572 | 0.593 | 0.05 |
| D1 | 13.95 | 4.88 | 13.69 | 4.53 | 0.65 | 572 | 0.517 | 0.05 |
| IT6 | 3.76 | 1.24 | 4.00 | 1.08 | −2.33 | 572 | 0.020 * | 0.20 |
| IT7 | 3.14 | 1.49 | 3.26 | 1.45 | −0.88 | 572 | 0.377 | 0.08 |
| IT8 | 4.08 | 1.12 | 4.08 | 1.05 | −0.02 | 572 | 0.987 | 0.00 |
| IT9 | 4.42 | 0.88 | 4.56 | 0.71 | −1.95 | 572 | 0.052 | 0.17 |
| IT10 | 4.40 | 0.89 | 4.49 | 0.81 | −1.27 | 572 | 0.206 | 0.11 |
| D2 | 19.81 | 4.22 | 20.38 | 3.89 | −1.65 | 572 | 0.099 | 0.14 |
| IT11 | 2.79 | 1.52 | 2.34 | 1.47 | 3.54 | 572 | <0.001 *** | 0.30 |
| IT12 | 3.66 | 1.43 | 3.58 | 1.52 | 0.63 | 572 | 0.531 | 0.05 |
| IT13 | 4.48 | 0.93 | 4.53 | 0.84 | −0.72 | 572 | 0.473 | 0.06 |
| IT14 | 2.95 | 1.35 | 2.96 | 1.32 | −0.07 | 572 | 0.946 | 0.01 |
| IT15 | 2.59 | 1.45 | 2.56 | 1.41 | 0.28 | 572 | 0.780 | 0.02 |
| D3 | 16.47 | 5.52 | 15.97 | 5.22 | 1.09 | 572 | 0.275 | 0.09 |
| IT16 | 2.50 | 1.24 | 2.45 | 1.20 | 0.52 | 572 | 0.600 | 0.04 |
| IT17 | 2.91 | 1.30 | 2.94 | 1.34 | −0.26 | 572 | 0.796 | 0.02 |
| IT18 | 2.04 | 1.17 | 1.86 | 1.12 | 1.82 | 572 | 0.069 | 0.15 |
| IT19 | 4.19 | 1.17 | 4.30 | 1.10 | −1.14 | 572 | 0.255 | 0.10 |
| IT20 | 4.65 | 0.79 | 4.84 | 0.54 | −3.13 | 572 | 0.002 ** | 0.27 |
| D4 | 16.30 | 4.36 | 16.39 | 4.00 | −0.26 | 572 | 0.792 | 0.02 |
| Total | 66.53 | 17.07 | 66.44 | 15.37 | 0.07 | 572 | 0.946 | 0.01 |
| IT/D | Setting | t | df | p | d | |||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | |||||||
| M | SD | M | SD | |||||
| IT1 | 3.26 | 1.50 | 3.38 | 0.74 | −0.22 | 150 | 0.826 | 0.08 |
| IT2 | 3.19 | 1.43 | 3.50 | 0.93 | −0.59 | 150 | 0.553 | 0.22 |
| IT3 | 2.96 | 1.42 | 4.13 | 0.83 | −2.29 | 150 | 0.023 * | 0.83 |
| IT4 | 3.40 | 1.43 | 4.00 | 1.07 | −1.17 | 150 | 0.242 | 0.43 |
| IT5 | 3.43 | 1.17 | 2.75 | 0.89 | 1.62 | 150 | 0.107 | 0.59 |
| D1 | 16.24 | 5.86 | 17.75 | 3.01 | −0.72 | 150 | 0.470 | 0.26 |
| IT6 | 4.14 | 0.93 | 4.63 | 0.52 | −1.46 | 150 | 0.145 | 0.53 |
| IT7 | 3.25 | 1.21 | 3.25 | 1.39 | 0.00 | 150 | 1.000 | 0.00 |
| IT8 | 4.07 | 1.09 | 3.88 | 0.99 | 0.49 | 150 | 0.622 | 0.18 |
| IT9 | 4.19 | 0.85 | 4.63 | 0.52 | −1.43 | 150 | 0.154 | 0.52 |
| IT10 | 3.53 | 1.35 | 3.25 | 1.16 | 0.58 | 150 | 0.561 | 0.21 |
| D2 | 19.18 | 4.20 | 19.63 | 2.77 | −0.29 | 150 | 0.768 | 0.11 |
| IT11 | 4.37 | 0.75 | 4.75 | 0.46 | −1.41 | 150 | 0.160 | 0.51 |
| IT12 | 4.01 | 1.10 | 3.75 | 1.28 | 0.64 | 150 | 0.525 | 0.23 |
| IT13 | 4.21 | 0.91 | 3.88 | 0.83 | 1.01 | 150 | 0.316 | 0.37 |
| IT14 | 4.23 | 0.94 | 3.88 | 0.83 | 1.04 | 150 | 0.301 | 0.38 |
| IT15 | 4.22 | 1.02 | 4.00 | 1.07 | 0.60 | 150 | 0.551 | 0.22 |
| D3 | 21.03 | 3.46 | 20.25 | 1.67 | 0.63 | 150 | 0.526 | 0.23 |
| IT16 | 4.33 | 0.95 | 4.13 | 1.36 | 0.59 | 150 | 0.558 | 0.21 |
| IT17 | 3.17 | 1.31 | 2.50 | 0.53 | 1.43 | 150 | 0.156 | 0.52 |
| IT18 | 3.80 | 1.10 | 3.50 | 1.07 | 0.75 | 150 | 0.456 | 0.27 |
| IT19 | 3.87 | 1.08 | 4.38 | 1.19 | −1.28 | 150 | 0.203 | 0.46 |
| IT20 | 4.31 | 0.93 | 4.00 | 1.31 | 0.91 | 150 | 0.366 | 0.33 |
| D4 | 19.48 | 3.81 | 18.50 | 1.77 | 0.72 | 150 | 0.473 | 0.26 |
| Total | 72.60 | 13.30 | 71.00 | 5.85 | 0.34 | 150 | 0.736 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Perales, R.; Palomares-Ruiz, A.; Gracia-Zomeño, A.; García-Toledano, E. Contextual Variables with an Impact on the Educational Inclusion of Students with Rare Diseases. Int. J. Environ. Res. Public Health 2022, 19, 14103. https://doi.org/10.3390/ijerph192114103
García-Perales R, Palomares-Ruiz A, Gracia-Zomeño A, García-Toledano E. Contextual Variables with an Impact on the Educational Inclusion of Students with Rare Diseases. International Journal of Environmental Research and Public Health. 2022; 19(21):14103. https://doi.org/10.3390/ijerph192114103
Chicago/Turabian StyleGarcía-Perales, Ramón, Ascensión Palomares-Ruiz, Andrea Gracia-Zomeño, and Eduardo García-Toledano. 2022. "Contextual Variables with an Impact on the Educational Inclusion of Students with Rare Diseases" International Journal of Environmental Research and Public Health 19, no. 21: 14103. https://doi.org/10.3390/ijerph192114103
APA StyleGarcía-Perales, R., Palomares-Ruiz, A., Gracia-Zomeño, A., & García-Toledano, E. (2022). Contextual Variables with an Impact on the Educational Inclusion of Students with Rare Diseases. International Journal of Environmental Research and Public Health, 19(21), 14103. https://doi.org/10.3390/ijerph192114103