
The Effects of Wearing Facemasks during Vigorous Exercise in the Aspect of Cardiopulmonary Response, In-Mask Environment, and Subject Discomfort


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
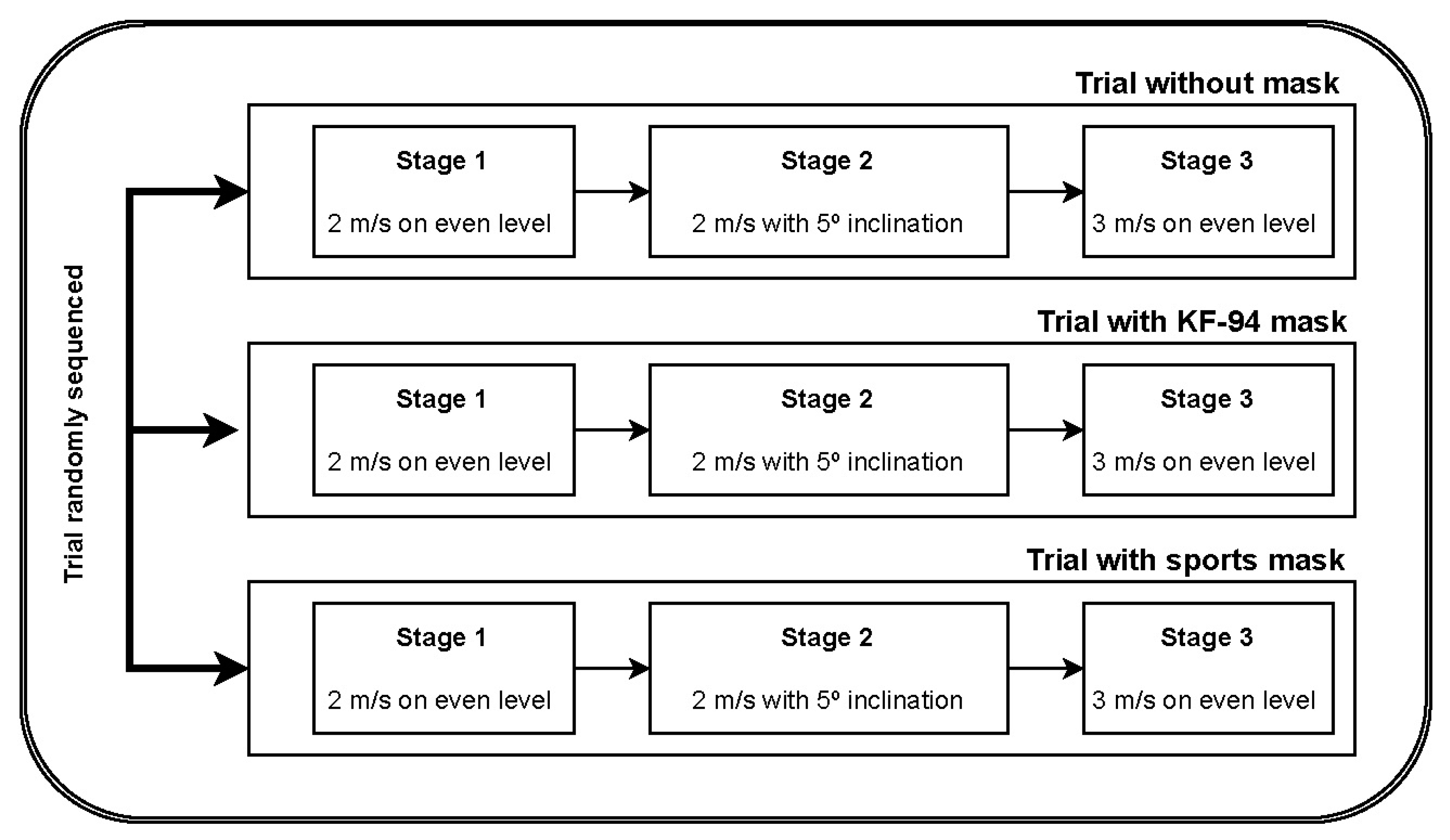
2.2. Experiment Protocol: Three Trial-Three Stage Protocol
2.3. Data Acquisition
2.4. Statistical Analysis
3. Results
3.1. Comparison with Baseline Data
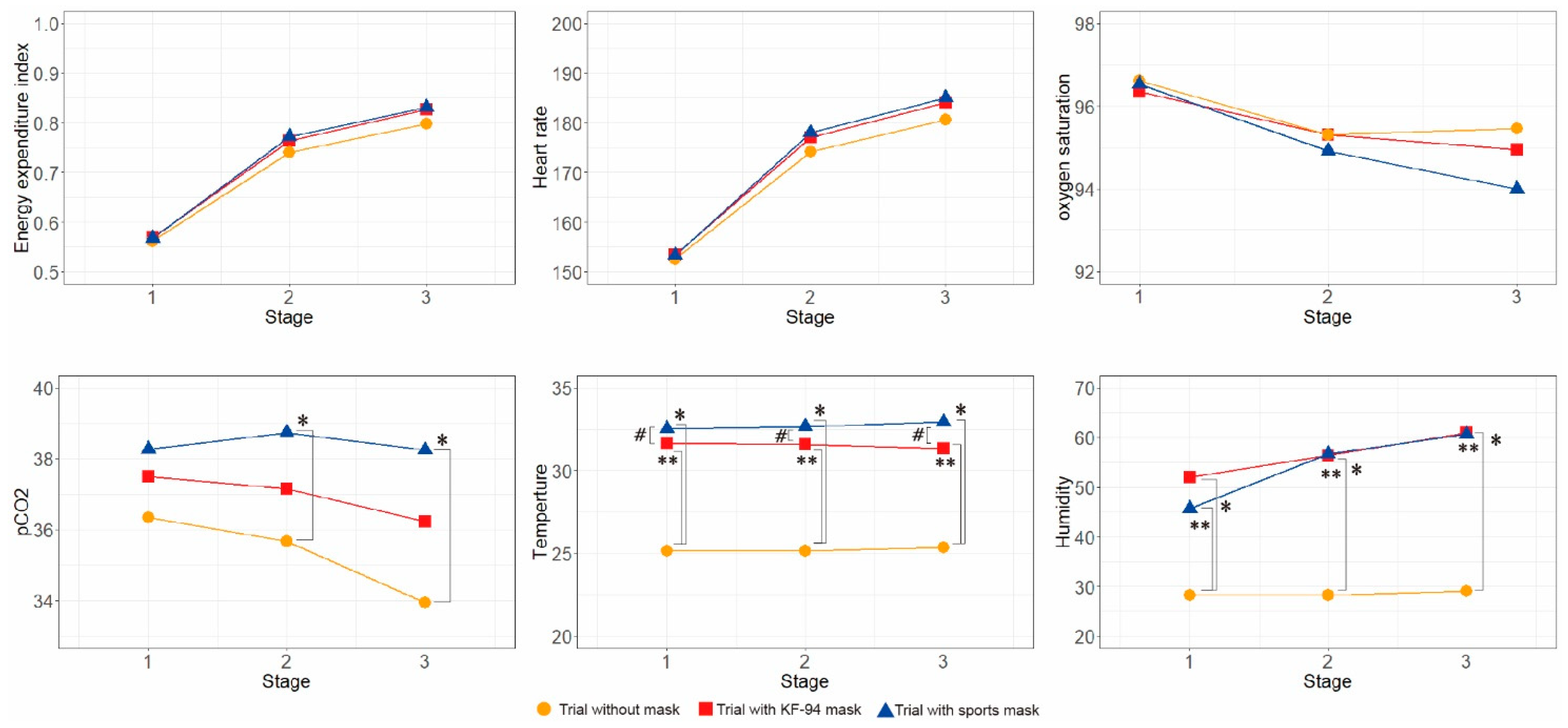
3.2. Comparison between Groups without Mask, with KF-94 Mask, and with Sports Mask
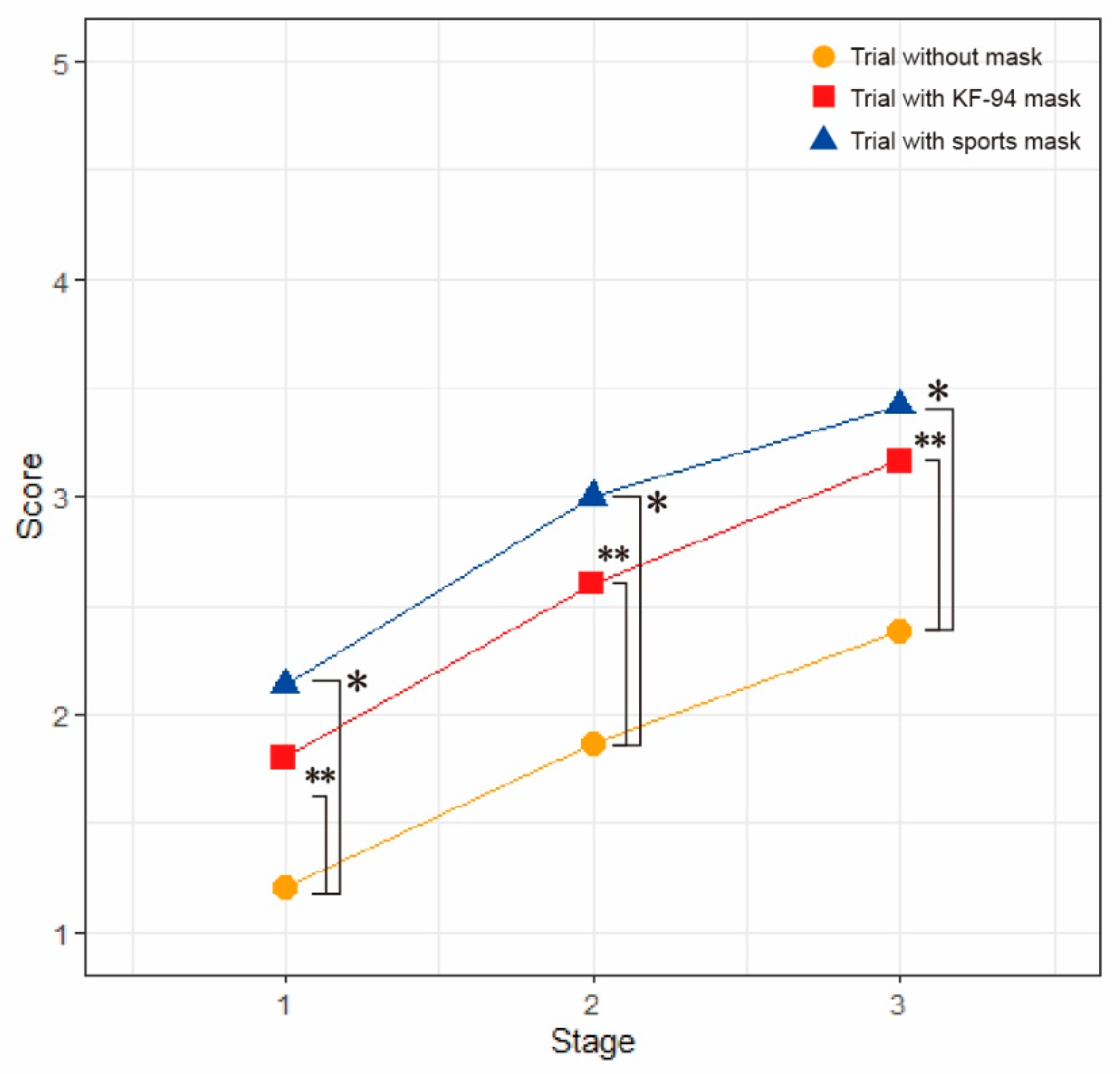
3.3. Subjective Ratings of Discomfort
3.4. Correlation between Physiologic Parameter and Subjective Discomfort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 23 June 2022).
- Baker, R.E.; Mahmud, A.S.; Miller, I.F.; Rajeev, M.; Rasambainarivo, F.; Rice, B.L.; Takahashi, S.; Tatem, A.J.; Wagner, C.E.; Wang, L.-F.; et al. Infectious disease in an era of global change. Nat. Rev. Microbiol. 2022, 20, 193–205. [Google Scholar] [CrossRef]
- Johnson, D.F.; Druce, J.D.; Birch, C.; Grayson, M.L. A quantitative assessment of the efficacy of surgical and N95 masks to filter influenza virus in patients with acute influenza infection. Clin. Infect. Dis. 2009, 49, 275–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, Y.; Willeke, K.; Grinshpun, S.A.; Donnelly, J.; Coffey, C.C. Performance of N95 respirators: Filtration efficiency for airborne microbial and inert particles. Am. Ind. Hyg. Assoc. J. 1998, 59, 128–132. [Google Scholar] [CrossRef]
- Kim, M.C.; Bae, S.; Kim, J.Y.; Park, S.Y.; Lim, J.S.; Sung, M.; Kim, S.H. Effectiveness of surgical, KF94, and N95 respirator masks in blocking SARS-CoV-2: A controlled comparison in 7 patients. Infect. Dis. 2020, 52, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Asadi, S.; Cappa, C.D.; Barreda, S.; Wexler, A.S.; Bouvier, N.M.; Ristenpart, W.D. Efficacy of masks and face coverings in controlling outward aerosol particle emission from expiratory activities. Sci. Rep. 2020, 10, 15665. [Google Scholar] [CrossRef] [PubMed]
- Why It Feels Like You Can’t Breathe Inside Your Face Mask—and What to Do About It. Available online: https://www.discovermagazine.com/health/why-it-feels-like-you-cant-breathe-inside-your-face-mask-and-what-to-do (accessed on 3 June 2021).
- Coronavirus Global Impact. Available online: https://datastudio.google.com/u/0/reporting/1RX1twzFniNjjOqd_HzuSqS_05rYD0zYH/page/i58TB (accessed on 20 June 2022).
- Kim, J.H.; Benson, S.M.; Roberge, R.J. Pulmonary and heart rate responses to wearing N95 filtering facepiece respirators. Am. J. Infect. Control 2013, 41, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Shein, S.L.; Whitticar, S.; Mascho, K.K.; Pace, E.; Speicher, R.; Deakins, K. The effects of wearing facemasks on oxygenation and ventilation at rest and during physical activity. PLoS ONE 2021, 16, e0247414. [Google Scholar] [CrossRef]
- Rhee, M.S.M.; Lindquist, C.D.; Silvestrini, M.T.; Chan, A.C.; Ong, J.J.Y.; Sharma, V.K. Carbon dioxide increases with face masks but remains below short-term NIOSH limits. BMC Infect. Dis. 2021, 21, 354. [Google Scholar] [CrossRef]
- Salati, H.; Khamooshi, M.; Vahaji, S.; Christo, F.C.; Fletcher, D.F.; Inthavong, K. N95 respirator mask breathing leads to excessive carbon dioxide inhalation and reduced heat transfer in a human nasal cavity. Phys. Fluids 2021, 33, 081913. [Google Scholar] [CrossRef]
- Ahmadian, M.; Ghasemi, M.; Nasrollahi Borujeni, N.; Afshan, S.; Fallah, M.; Ayaseh, H.; Pahlavan, M.; Nabavi Chashmi, S.M.; Haeri, T.; Imani, F.; et al. Does wearing a mask while exercising amid COVID-19 pandemic affect hemodynamic and hematologic function among healthy individuals? Implications of mask modality, sex, and exercise intensity. Phys. Sportsmed. 2022, 50, 257–268. [Google Scholar] [CrossRef]
- Shaw, K.; Butcher, S.; Ko, J.; Zello, G.A.; Chilibeck, P.D. Wearing of Cloth or Disposable Surgical Face Masks has no Effect on Vigorous Exercise Performance in Healthy Individuals. Int. J. Environ. Res. Public Health 2020, 17, 8110. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, S.R.; Dominelli, P.B.; Davis, C.K.; Guenette, J.A.; Luks, A.M.; Molgat-Seon, Y.; Sá, R.C.; Sheel, A.W.; Swenson, E.R.; Stickland, M.K. Face Masks and the Cardiorespiratory Response to Physical Activity in Health and Disease. Ann. Am. Thorac. Soc. 2021, 18, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.A.; Zello, G.A.; Butcher, S.J.; Ko, J.B.; Bertrand, L.; Chilibeck, P.D. The impact of face masks on performance and physiological outcomes during exercise: A systematic review and meta-analysis. Appl. Physiol. Nutr. Metab. 2021, 46, 693–703. [Google Scholar] [CrossRef]
- Asín-Izquierdo, I.; Ruiz-Ranz, E.; Arévalo-Baeza, M. The Physiological Effects of Face Masks During Exercise Worn Due to COVID-19: A Systematic Review. Sport. Health 2022, 14, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, R.; Gwosdow, A.R.; Berglund, L.G.; DuBois, A.B. The effect of temperature and humidity levels in a protective mask on user acceptability during exercise. Am. Ind. Hyg. Assoc. J. 1987, 48, 639–645. [Google Scholar] [CrossRef]
- Chhajed, P.N.; Chaudhari, P.; Tulasigeri, C.; Kate, A.; Kesarwani, R.; Miedinger, D.; Leuppi, J.; Baty, F. Infraclavicular sensor site: A new promising site for transcutaneous capnography. Scand. J. Clin. Lab. Investig. 2012, 72, 340–342. [Google Scholar] [CrossRef]
- Nene, A.V. Physiological cost index of walking in able-bodied adolescents and adults. Clin. Rehabil. 1993, 7, 319–326. [Google Scholar] [CrossRef]
- Rose, J.; Gamble, J.G.; Lee, J.; Lee, R.; Haskell, W.L. The energy expenditure index: A method to quantitate and compare walking energy expenditure for children and adolescents. J. Pediatr. Orthop. 1991, 11, 571–578. [Google Scholar] [CrossRef]
- Karami, H.; Karami, K.; Khafaie, M.; Zahednejad, S.; Arastoo, A. The Physiological Cost Index and Some Kinematic Parameters of Walking and Jogging in Blind and Sighted Students. Iran. J. Med. Sci. 2020, 45, 16–22. [Google Scholar] [CrossRef]
- Bailey, M.J.; Ratcliffe, C.M. Reliability of Physiological Cost Index Measurements in Walking Normal Subjects Using Steady-state, Non-steady-state and Post-exercise Heart Rate Recording. Physiotherapy 1995, 81, 618–623. [Google Scholar] [CrossRef]
- Lalonde, T.; Nguyen, A.; Yin, J.; Irimata, K.; Wilson, J. Modeling Correlated Binary Outcomes with Time-Dependent Covariates. J. Data Sci. 2021, 11, 715–738. [Google Scholar] [CrossRef]
- Eroğlu, H.A.; Okyaz, B.; Türkçapar, Ü. The Effect of Acute Aerobical Exercise on Arterial Blood Oxygen Saturation of Athletes. J. Educ. Train. Stud. 2018, 6, 74–79. [Google Scholar] [CrossRef]
- Balfour-Lynn, I.M.; Prasad, S.A.; Laverty, A.; Whitehead, B.F.; Dinwiddie, R. A step in the right direction: Assessing exercise tolerance in cystic fibrosis. Pediatr. Pulmonol. 1998, 25, 278–284. [Google Scholar] [CrossRef]
- Hoffmann, C. Effect of a Facemask on Heart Rate, Oxygen Saturation, and Rate of Perceived Exertion. Dtsch. Z. Sportmed. 2021, 72, 359–364. [Google Scholar]
- Amput, P.; Wongphon, S. Effects of Wearing Face Masks on Cardiorespiratory Parameters at Rest and after Performing the Six-Minute Walk Test in Older Adults. Geriatrics 2022, 7, 62. [Google Scholar] [CrossRef] [PubMed]
- Fikenzer, S.; Uhe, T.; Lavall, D.; Rudolph, U.; Falz, R.; Busse, M.; Hepp, P.; Laufs, U. Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clin. Res. Cardiol. 2020, 109, 1522–1530. [Google Scholar] [CrossRef]
- Gholamreza, F.; Nadaraja, A.V.; Milani, A.S.; Golovin, K. Enhanced protection face masks do not adversely impact thermophysiological comfort. PLoS ONE 2022, 17, e0265126. [Google Scholar] [CrossRef]
- Gericke, A.; Militký, J.; Venkataraman, M.; Steyn, H.; Vermaas, J. The Effect of Mask Style and Fabric Selection on the Comfort Properties of Fabric Masks. Materials 2022, 15, 2559. [Google Scholar] [CrossRef] [PubMed]
- Person, E.; Lemercier, C.; Royer, A.; Reychler, G. Effect of a surgical mask on six minute walking distance. Rev. Mal. Respir. 2018, 35, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Wu, T.; Powell, J.B.; Roberge, R.J. Physiologic and fit factor profiles of N95 and P100 filtering facepiece respirators for use in hot, humid environments. Am. J. Infect. Control 2016, 44, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Martellucci, C.A.; Flacco, M.E.; Martellucci, M.; Violante, F.S.; Manzoli, L. Inhaled CO2 concentration while wearing face masks: A pilot study using capnography. medRxiv 2022, 16, 11786302221123573. [Google Scholar] [CrossRef]
- Geiss, O. Effect of wearing face masks on the carbon dioxide concentration in the breathing zone. Aerosol Air Qual. Res. 2021, 21, 200403. [Google Scholar] [CrossRef]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef]
- Bannister, R.G.; Cunningham, D.J.; Douglas, C.G. The carbon dioxide stimulus to breathing in severe exercise. J. Physiol. 1954, 125, 90–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, N.; Honda, Y.; Komura, K.; Tsuji, B.; Sugihara, A.; Watanabe, K.; Kondo, N.; Nishiyasu, T. Effect of voluntary hypocapnic hyperventilation on the relationship between core temperature and heat loss responses in exercising humans. J. Appl. Physiol. 2014, 117, 1317–1324. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SaO2 1 | pCO2 2 | Heart Rate | Temperature | Humidity | EEI 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | p-Value | Mean ± SD | p Value | Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | ||
| Baseline | 96.93 ± 1.03 | 38.61 ± 4.14 | 88.20 ± 12.72 | 25.14 ± 0.90 | 28.27 ± 9.88 | |||||||
| No mask | Stage 1 | 96.61 ± 1.69 | 0.640 | 36.35 ± 3.63 | 0.066 | 152.57 ± 11.41 | <0.001 *** | 0.56 ± 0.09 | ||||
| Stage 2 | 95.31. ± 2.53 | 0.016 ** | 35.67 ± 4.45 | 0.022 * | 175.03 ± 9.90 | <0.001 *** | 0.75 ± 0.10 | |||||
| Stage 3 | 95.46 ± 1.47 | 0.028 * | 33.94 ± 5.15 * | 0.003 * | 180.65 ± 12.51 | <0.001 *** | 0.80 ± 0.11 | |||||
| KF- 94 mask | Stage 1 | 96.34 ± 1.37 | 0.129 | 37.50 ± 2.55 | 0.679 | 153.45 ± 10.95 | <0.001 *** | 31.66 ± 0.92 | <0.001 *** | 51.97 ± 13.35 | <0.001 *** | 0.57 ± 0.09 |
| Stage 2 | 95.31. ± 1.48 | 0.002 * | 37.15 ± 3.57 | 0.547 | 177.37 ± 10.56 | <0.001 *** | 31.57 ± 0.77 | <0.001 *** | 56.38 ± 11.77 | <0.001 *** | 0.77 ± 0.11 | |
| Stage 3 | 94.95 ± 1.61 | 0.001 ** | 36.23 ± 4.29 | 0.082 | 184.05 ± 7.39 | <0.001 *** | 31.34 ± 0.72 | <0.001 *** | 60.89 ± 11.80 | <0.001 *** | 0.83 ± 0.09 | |
| Sports mask | Stage 1 | 96.49 ± 1.26 | 0.169 | 38.26 ± 3.96 | 0.810 | 153.31 ± 10.81 | <0.001 *** | 32.53 ± 1.34 | <0.001 *** | 45.62 ± 8.94 | <0.001 *** | 0.57 ± 0.10 |
| Stage 2 | 95.11. ± 1.88 | 0.015 * | 38.73 ± 4.82 | 0.974 | 178.13 ± 10.59 | <0.001 *** | 32.66 ± 0.69 | <0.001 *** | 56.72 ± 12.10 | <0.001 *** | 0.77 ± 0.11 | |
| Stage 3 | 94.00 ± 2.85 | 0.004 ** | 38.25 ± 6.04 | 0.684 | 185.05 ± 8.05 | <0.001 *** | 32.75 ± 1.76 | <0.001 *** | 60.68 ± 11.41 | <0.001 *** | 0.83 ± 0.11 | |
| Stage 1 | Stage II | Stage III | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |
| Trial no mask | 1.20 ± 0.41 | 1.87 ± 0.74 | 2.38 ± 1.04 |
| Trial with KF-94 mask | 1.80 ± 0.41 | 2.60 ± 0.74 | 3.17 ± 1.03 |
| Trial with sports mask | 2.13 ± 0.74 | 3.00 ± 0.65 | 3.42 ± 1.00 |
| Subject Rating of Degree of Discomfort during Stage | ||||
|---|---|---|---|---|
| Between Effect | Within Effect | |||
| Beta Coefficient (SE) | p-Value | Beta Coefficient (SE) | p-Value | |
| SaO2 1 | −0.018(0.116) | 0.8812 | −0.0015(0.039) | 0.6989 |
| pCO2 2 | 0.046(0.054) | 0.4098 | 0.045(0.019) | 0.0167 * |
| Heart rate | 0.003(0.011) | 0.814 | −0.002(0.009) | 0.7813 |
| EEI 3 | 0.014(0.011) | 0.1803 | −0.007(0.009) | 0.4315 |
| Temperature in mask | 0.104(0.151) | 0.5036 | −0.07(0.055) | 0.2058 |
| Humidity in mask | −0.013(0.029) | 0.657 | −0.002(0.007) | 0.8218 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.; Byun, J.; Choi, J.-o.; Shim, D.; Rha, D.-w. The Effects of Wearing Facemasks during Vigorous Exercise in the Aspect of Cardiopulmonary Response, In-Mask Environment, and Subject Discomfort. Int. J. Environ. Res. Public Health 2022, 19, 14106. https://doi.org/10.3390/ijerph192114106
Hong J, Byun J, Choi J-o, Shim D, Rha D-w. The Effects of Wearing Facemasks during Vigorous Exercise in the Aspect of Cardiopulmonary Response, In-Mask Environment, and Subject Discomfort. International Journal of Environmental Research and Public Health. 2022; 19(21):14106. https://doi.org/10.3390/ijerph192114106
Chicago/Turabian StyleHong, Juntaek, Juahn Byun, Joong-on Choi, Dain Shim, and Dong-wook Rha. 2022. "The Effects of Wearing Facemasks during Vigorous Exercise in the Aspect of Cardiopulmonary Response, In-Mask Environment, and Subject Discomfort" International Journal of Environmental Research and Public Health 19, no. 21: 14106. https://doi.org/10.3390/ijerph192114106
APA StyleHong, J., Byun, J., Choi, J. -o., Shim, D., & Rha, D. -w. (2022). The Effects of Wearing Facemasks during Vigorous Exercise in the Aspect of Cardiopulmonary Response, In-Mask Environment, and Subject Discomfort. International Journal of Environmental Research and Public Health, 19(21), 14106. https://doi.org/10.3390/ijerph192114106