
Effect of Longitudinal Practice in Real and Virtual Environments on Motor Performance, Physical Activity and Enjoyment in People with Autism Spectrum Disorder: A Prospective Randomized Crossover Controlled Trial

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Characterization
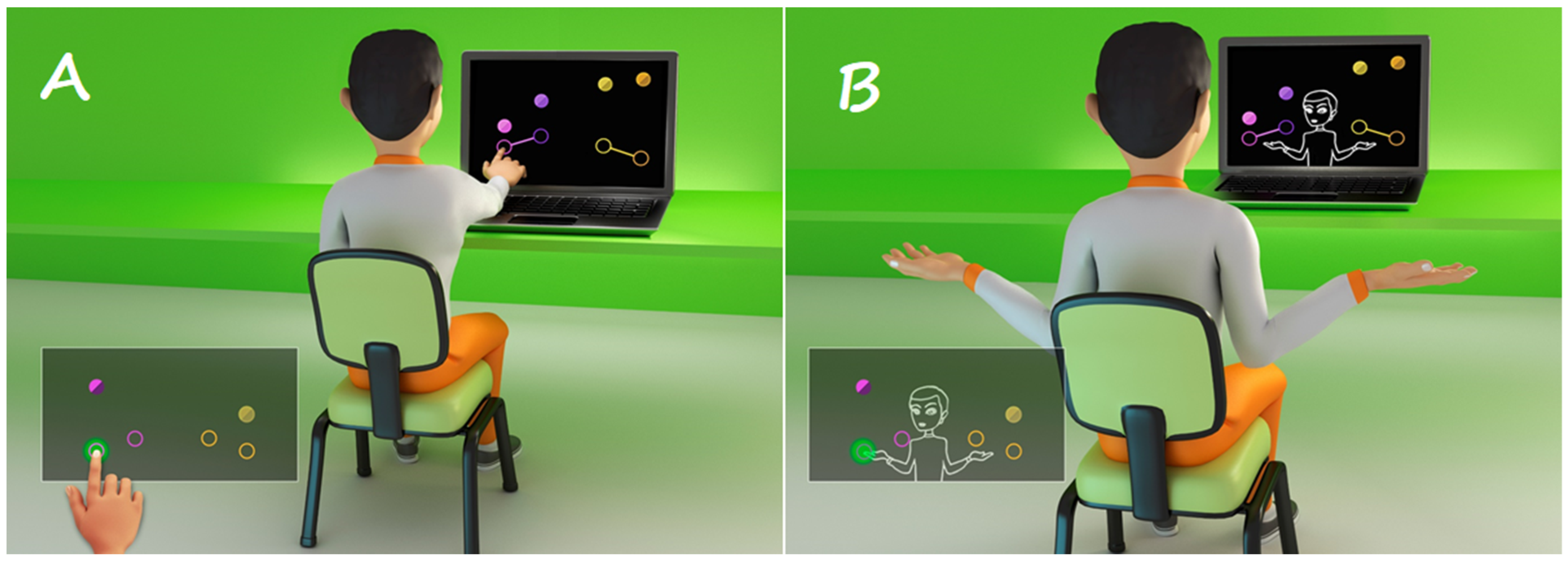
2.3. Virtual Reality (VR) Activity
2.4. Physical Activity by Percentage of Heart Rate Reserve (HRR)
2.5. Enjoyment Scale
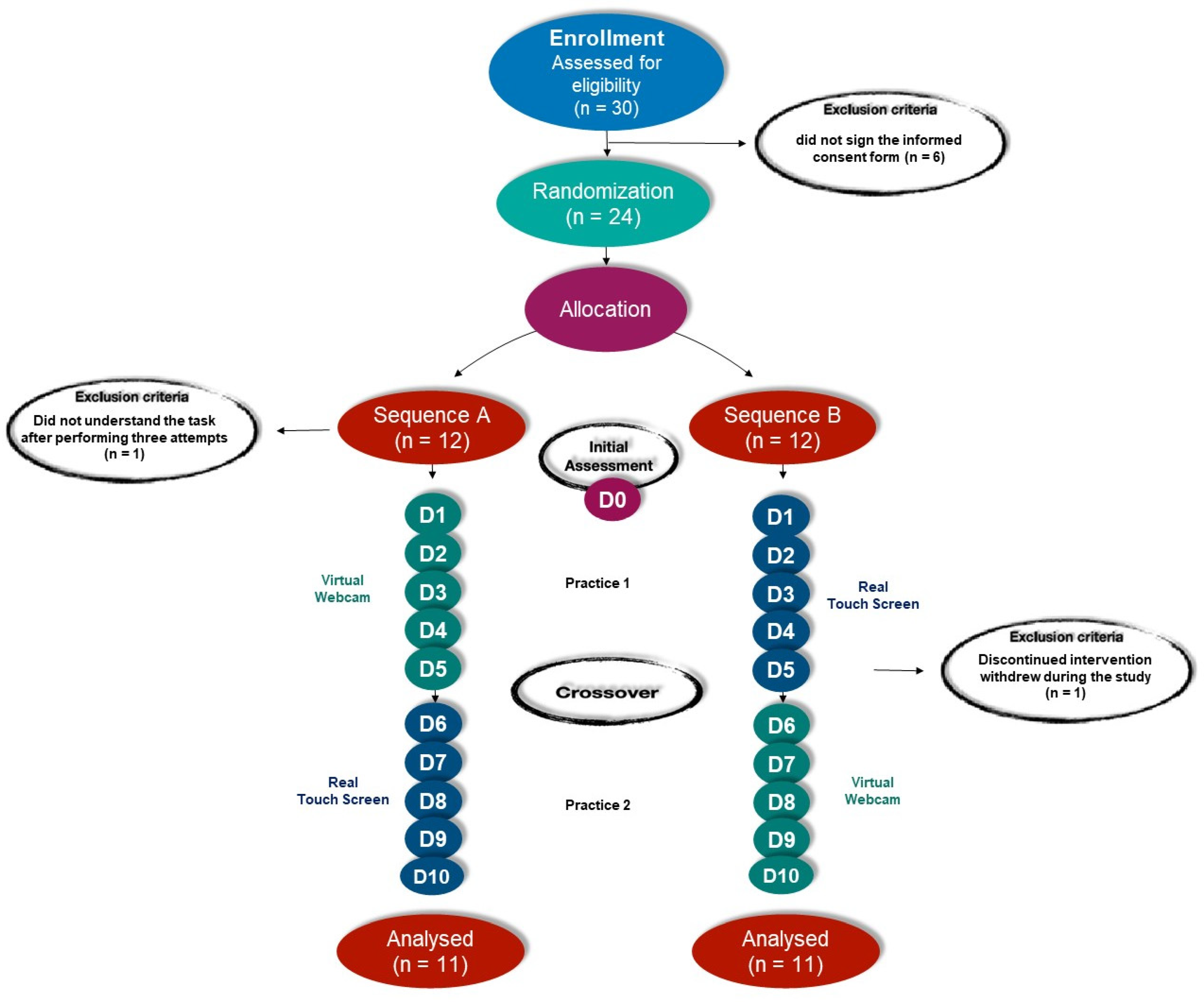
2.6. Randomization
- Sequence A: Beginning the intervention by performing a virtual task using the Webcam interface, followed by a real task, using the Touch Screen interface.
- Sequence B: Beginning the intervention by performing a real task using the Touch Screen interface, followed by a virtual task, using the Webcam interface.
2.7. Data Analysis
3. Results
3.1. Software MoveHero—VR Activity
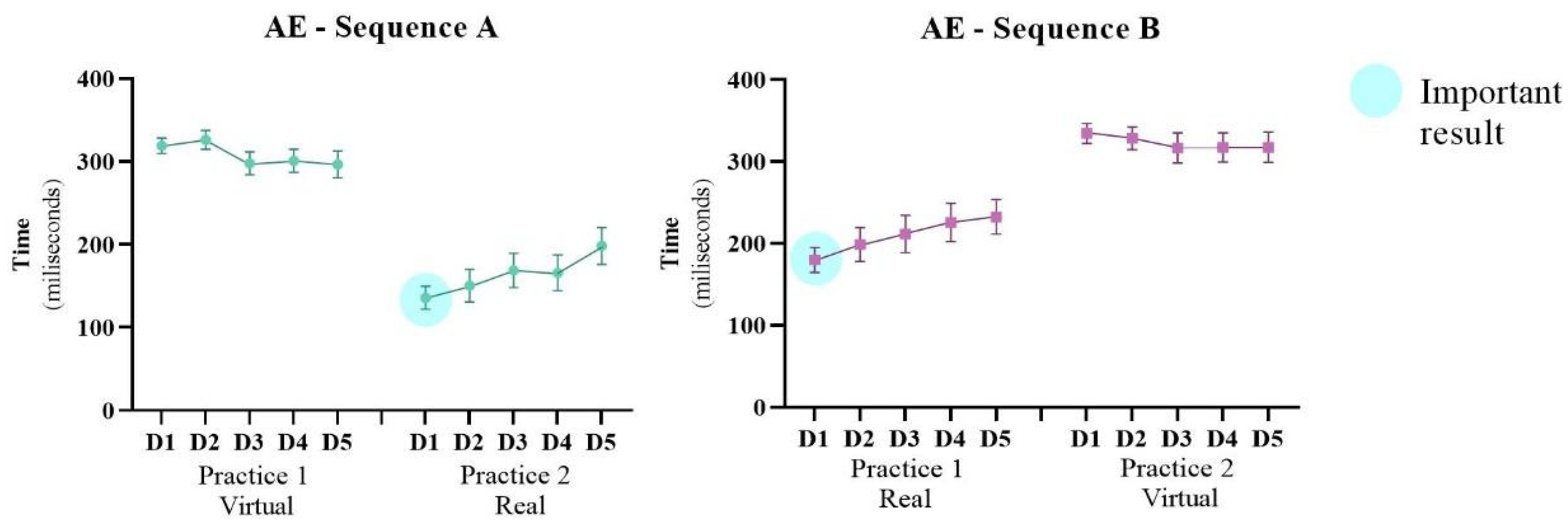
3.1.1. Absolute Error/Accuracy—AE
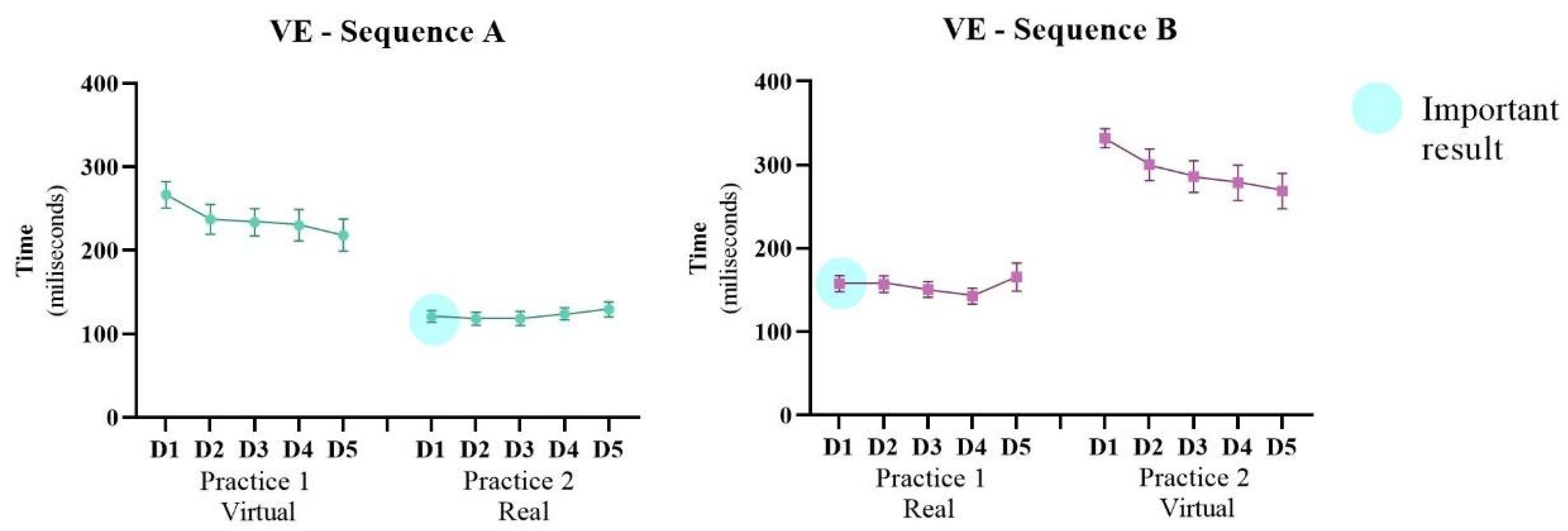
3.1.2. Variable Error/Precision—VE
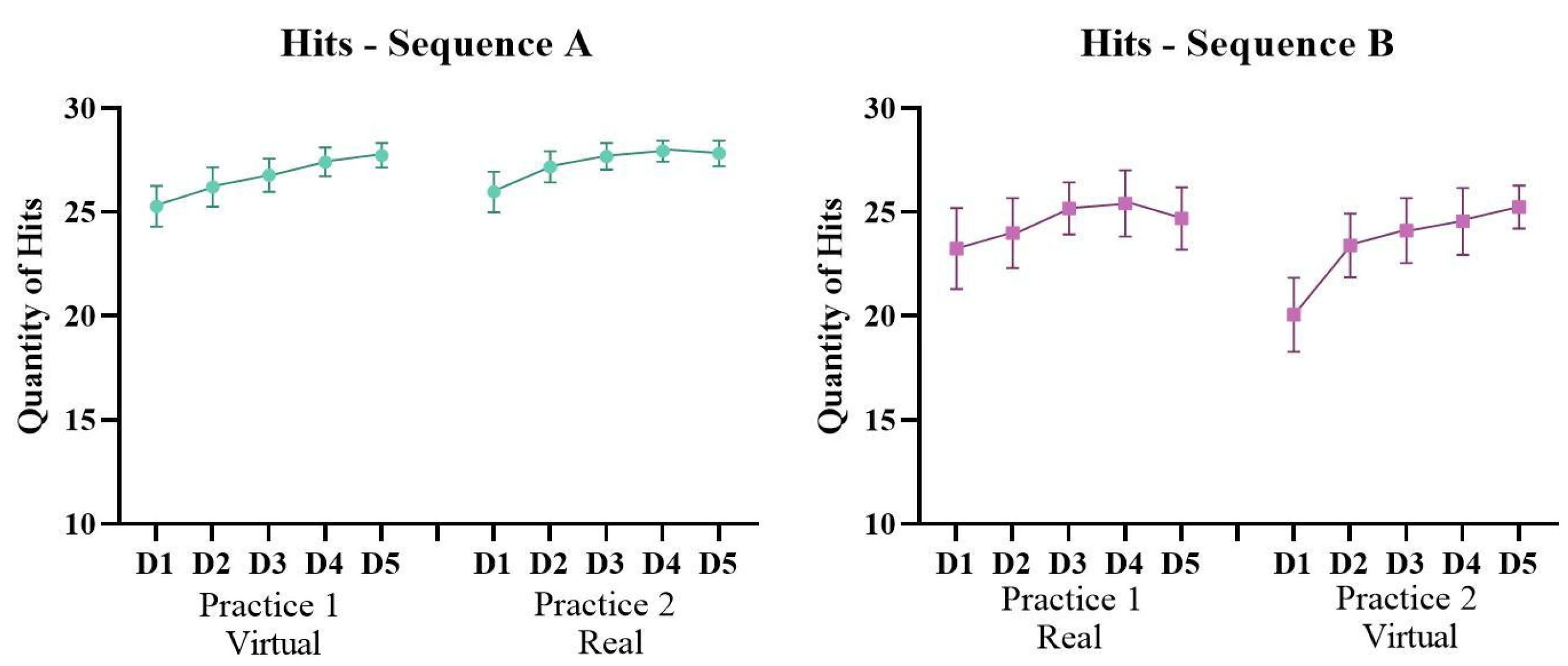
3.1.3. Quantity of Hits
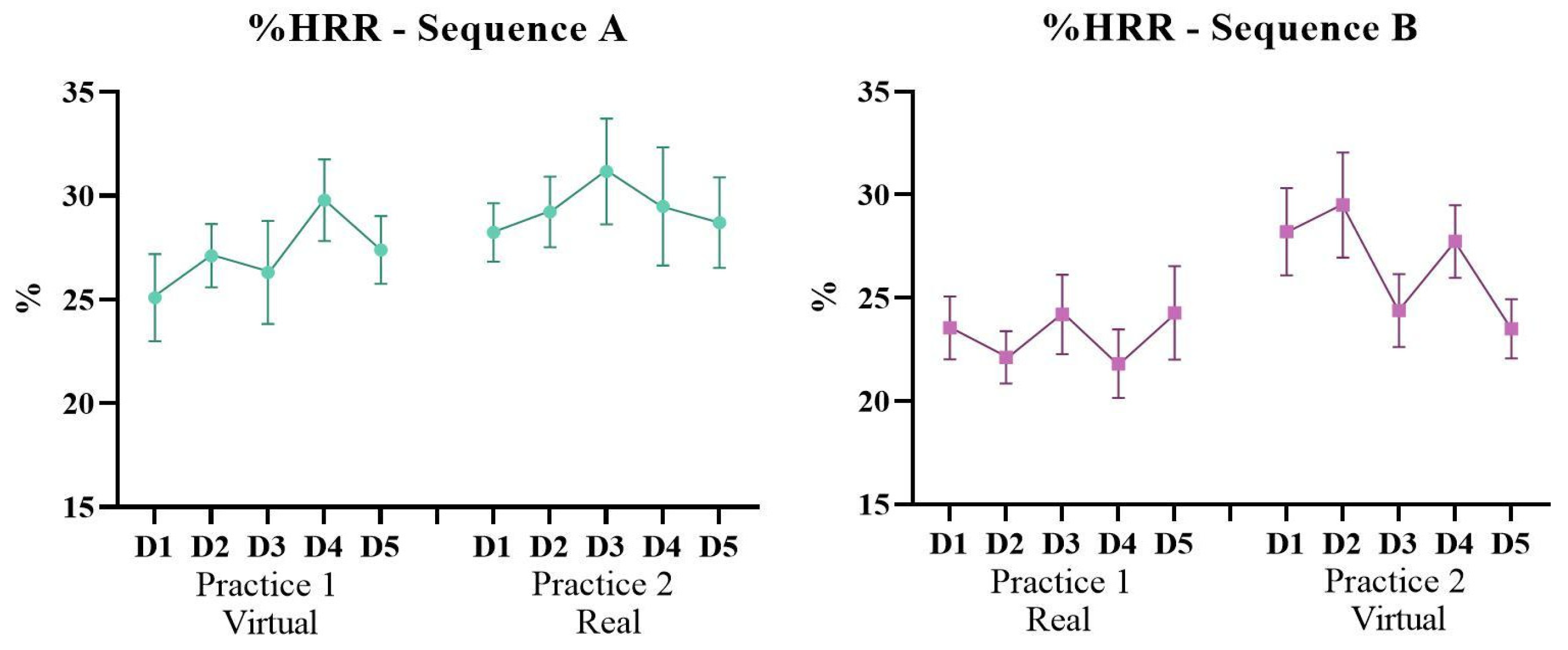
3.2. Percentage of Heart Rate Reserve (%HRR)
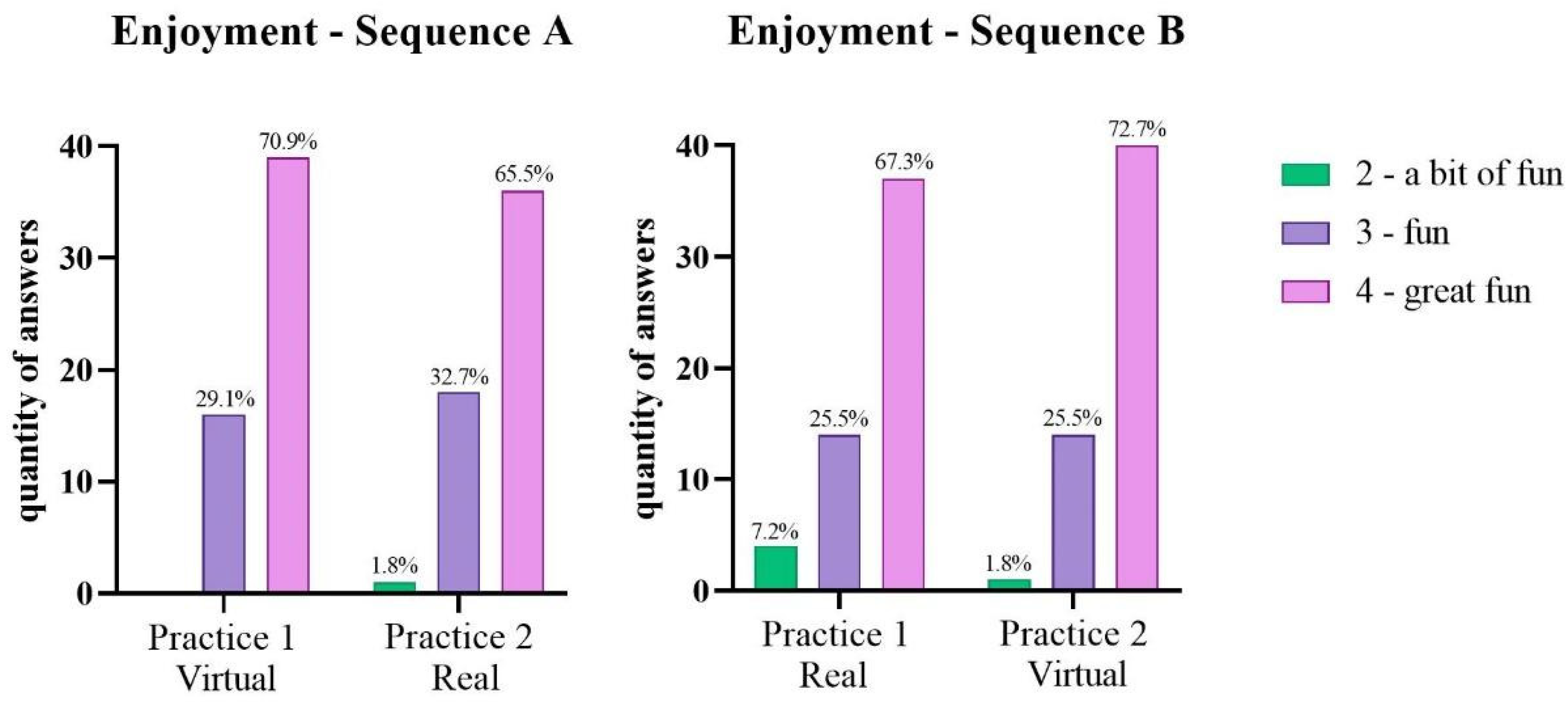
3.3. Enjoyment Scale
4. Discussion
4.1. Improvement in Motor Performance and Transfer to the Subsequent Practice When Changing the Environment
4.2. Promote Physical Activity by Altering the Heart Rate
4.3. Enjoyment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Luca, R.; Leonardi, S.; Portaro, S.; le Cause, M.; de Domenico, C.; Colucci, P.V.; Pranio, F.; Bramanti, P.; Calabrò, R.S. Innovative Use of Virtual Reality in Autism Spectrum Disorder: A Case-Study. Appl. Neuropsychol. Child. 2021, 10, 90–100. [Google Scholar] [CrossRef]
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Philadelphia, PA, USA, 2013. [Google Scholar]
- Rynkiewicz, A.; Schuller, B.; Marchi, E.; Piana, S.; Camurri, A.; Lassalle, A.; Baron-Cohen, S. An Investigation of the “female Camouflage Effect” in Autism Using a Computerized ADOS-2 and a Test of Sex/Gender Differences. Mol. Autism. 2016, 7, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ecker, C. The Neuroanatomy of Autism Spectrum Disorder: An Overview of Structural Neuroimaging Findings and Their Translatability to the Clinical Setting. Autism 2017, 21, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Volkmar, F.R.; Reichow, B. Autism in DSM-5: Progress and Challenges. Mol. Autism. 2013, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawakami, S.; Uono, S.; Otsuka, S.; Yoshimura, S.; Zhao, S.; Toichi, M. Atypical Multisensory Integration and the Temporal Binding Window in Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 3944–3956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siemann, J.K.; Veenstra-VanderWeele, J.; Wallace, M.T. Approaches to Understanding Multisensory Dysfunction in Autism Spectrum Disorder. Autism Res. 2020, 13, 1430–1449. [Google Scholar] [CrossRef]
- Posar, A.; Visconti, P. Sensory Abnormalities in Children with Autism Spectrum Disorder. J. Pediatr. 2018, 94, 342–350. [Google Scholar] [CrossRef]
- Gidley Larson, J.C.; Mostofsky, S.H. Evidence That the Pattern of Visuomotor Sequence Learning Is Altered in Children with Autism. Autism Res. 2008, 1, 341–353. [Google Scholar] [CrossRef] [Green Version]
- Marko, M.K.; Crocetti, D.; Hulst, T.; Donchin, O.; Shadmehr, R.; Mostofsky, S.H. Behavioural and Neural Basis of Anomalous Motor Learning in Children with Autism. Brain 2015, 138, 784–797. [Google Scholar] [CrossRef]
- Mostofsky, S.H.; Ewen, J.B. Altered Connectivity and Action Model Formation in Autism Is Autism. Neuroscientist 2011, 17, 437–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moraes, Í.A.P.; Massetti, T.; Crocetta, T.B.; Silva, T.D.; Menezes, L.D.C.; Monteiro, C.B.D.M.; Magalhães, F.H. Motor Learning Characterization in People with Autism Spectrum Disorder: A Systematic Review. Dement. Neuropsychol. 2017, 11, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, A.; Dancel, A.; Johnson, R.; Sargent, B. The Effect of Motor and Physical Activity Intervention on Motor Outcomes of Children with Autism Spectrum Disorder: A Systematic Review. Autism 2020, 24, 544–568. [Google Scholar] [CrossRef] [PubMed]
- Dowell, L.R.; Mahone, E.M.; Mostofsky, S.H. Associations of Postural Knowledge and Basic Motor Skill With Dyspraxia in Autism: Implication for Abnormalities in Distributed Connectivity and Motor Learning. Neuropsychology 2009, 23, 563–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gidley Larson, J.C.; Bastian, A.J.; Donchin, O.; Shadmehr, R.; Mostofsky, S.H. Acquisition of Internal Models of Motor Tasks in Children with Autism. Brain 2008, 131, 2894–2903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ketcheson, L.; Hauck, J.; Ulrich, D. The Effects of an Early Motor Skill Intervention on Motor Skills, Levels of Physical Activity, and Socialization in Young Children with Autism Spectrum Disorder: A Pilot Study. Autism 2017, 21, 481–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Du, C.; Liu, J.; Tan, G. Meta-Analysis on Intervention Effects of Physical Activities on Children and Adolescents with Autism. Int. J. Environ. Res. Public Health 2020, 17, 1950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanish, H.; Curtin, C.; Must, A.; Phillips, S.; Maslin, M.; Bandini, L. Enjoyment, Barriers, and Beliefs about Physical Activity in Adolescents with and without Autism Spectrum Disorder. Adapt. Phys. Act. Q. 2015, 32, 302–317. [Google Scholar] [CrossRef]
- Obrusnikova, I.; Cavalier, A.R. Perceived Barriers and Facilitators of Participation in After-School Physical Activity by Children with Autism Spectrum Disorders. J. Dev. Phys. Disabil. 2011, 23, 195–211. [Google Scholar] [CrossRef]
- Arnell, S.; Jerlinder, K.; Lundqvist, L.O. Perceptions of Physical Activity Participation Among Adolescents with Autism Spectrum Disorders: A Conceptual Model of Conditional Participation. J. Autism Dev. Disord. 2018, 48, 1792–1802. [Google Scholar] [CrossRef]
- Eversole, M.; Collins, D.M.; Karmarkar, A.; Colton, L.; Quinn, J.P.; Karsbaek, R.; Johnson, J.R.; Callier, N.P.; Hilton, C.L. Leisure Activity Enjoyment of Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2016, 46, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Dębska, M.; Polechoński, J.; Mynarski, A.; Polechoński, P. Enjoyment and Intensity of Physical Activity in Immersive Virtual Reality Performed on Innovative Training Devices in Compliance with Recommendations for Health. Int. J. Environ. Res. Public Health 2019, 16, 3673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gough, C. Distribution of Video Gamers Worldwide in 2017, by Age Group and Gender. Available online: https://www.statista.com/statistics/722259/world-gamers-by-age-and-gender/ (accessed on 10 August 2022).
- Matsangidou, M.; Ang, C.S.; Mauger, A.R.; Intarasirisawat, J.; Otkhmezuri, B.; Avraamides, M.N. Is your virtual self as sensational as your real? Virtual Reality: The effect of body consciousness on the experience of exercise sensations. Psychol. Sport Exerc. 2019, 41, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Baños, R.M.; Escobar, P.; Cebolla, A.; Guixeres, J.; Alvarez Pitti, J.; Lisón, J.F.; Botella, C. Using Virtual Reality to Distract Overweight Children from Bodily Sensations during Exercise. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Lyons, E.J.; Tate, D.F.; Ward, D.S.; Ribisl, K.M.; Bowling, J.M.; Kalyanaraman, S. Engagement, Enjoyment, and Energy Expenditure during Active Video Game Play. Health Psychol. 2014, 33, 174–181. [Google Scholar] [CrossRef] [Green Version]
- Lewis, B.A.; Williams, D.M.; Frayeh, A.; Marcus, B.H. Self-Efficacy versus Perceived Enjoyment as Predictors of Physical Activity Behaviour. Psychol. Health 2016, 31, 456–469. [Google Scholar] [CrossRef] [Green Version]
- Newbutt, N.; Sung, C.; Kuo, H.J.; Leahy, M.J.; Lin, C.C.; Tong, B. Brief Report: A Pilot Study of the Use of a Virtual Reality Headset in Autism Populations. J. Autism Dev. Disord. 2016, 46, 3166–3176. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Reid, D. Virtual Reality in Pediatric Neurorehabilitation: Attention Deficit Hyperactivity Disorder, Autism and Cerebral Palsy. Neuroepidemiology 2011, 36, 2–18. [Google Scholar] [CrossRef]
- de Mello Monteiro, C.B.; Massetti, T.; da Silva, T.D.; van der Kamp, J.; de Abreu, L.C.; Leone, C.; Savelsbergh, G.J.P. Transfer of Motor Learning from Virtual to Natural Environments in Individuals with Cerebral Palsy. Res. Dev. Disabil. 2014, 35, 2430–2437. [Google Scholar] [CrossRef]
- Sveistrup, H. Motor Rehabilitation Using Virtual Reality. J. NeuroEng. Rehabil. 2004, 1, 10. [Google Scholar] [CrossRef]
- de Moraes, Í.A.P.; Monteiro, C.B.D.M.; da Silva, T.D.; Massetti, T.; Crocetta, T.B.; de Menezes, L.D.C.; Andrade, G.P.D.R.; Alessandro Hervaldo Nicolai, R.E.; Dawes, H.; Coe, S.; et al. Motor Learning and Transfer between Real and Virtual Environments in Young People with Autism Spectrum Disorder: A Prospective Randomized Cross over Controlled Trial. Autism Res. 2020, 13, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.; Shamseer, L.; Altman, D.G.; Weeks, L.; Peters, J.; Kober, T.; Dias, S.; Schulz, K.F.; Plint, A.C.; Moher, D. Consolidated Standards of Reporting Trials (CONSORT) and the Completeness of Reporting of Randomised Controlled Trials (RCTs) Published in Medical Journals. Cochrane Database Syst. Rev. 2012, 2013, MR000030. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, J.M. Internal and External Validity of Seven Wechsler Intelligence Scale for Children-Third Edition Short Forms in a Sample of Psychiatric Inpatients. Psychol. Assess 1998, 10, 431–434. [Google Scholar] [CrossRef]
- Rao, V.; Raman, V.; Mysore, A.V. Issues Related to Obtaining Intelligence Quotient-Matched Controls in Autism Research. Indian J. Psychol. Med. 2015, 37, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.Y.; Chou, W.; Chow, J.C.; Lin, C.H.; Tung, L.C.; Chen, K.L. IQ Discrepancy Differentiates Levels of Fine Motor Skills and Their Relationship in Children with Autism Spectrum Disorders. Neuropsychiatr. Dis. Treat. 2018, 14, 597–605. [Google Scholar] [CrossRef] [Green Version]
- al Backer, N.B. Correlation between Autism Treatment Evaluation Checklist (ATEC) and Childhood Autism Rating Scale (CARS) in the Evaluation of Autism Spectrum Disorder. Sudan J. Paediatr. 2016, 16, 17. [Google Scholar]
- Pereira, A.M.; Riesgo, R.S.; Wagner, M.B. Childhood Autism: Translation and Validation of the Childhood Autism Rating Scale for Use in Brazil. J. Pediatr. 2008, 84, 487–494. [Google Scholar] [CrossRef]
- Berg, M.; Jahnsen, R.; Frøslie, K.F.; Hussain, A. Reliability of the Pediatric Evaluation of Disability Inventory (PEDI). Phys Occup Ther. Pediatr. 2004, 24, 61–77. [Google Scholar] [CrossRef]
- Mancini, M.C. Inventário de Avaliação Pediátrica de Incapacidade (PEDI)—Manual Da Versão Brasileira Adaptada; Editora UFMG: Belo Horizonte, Brazil, 2005. [Google Scholar]
- Martins, F.P.A.; Massetti, T.; Crocetta, T.B.; Lopes, P.B.; da Silva, A.A.; Figueiredo, E.F.; de Abreu, L.C.; da Silva, T.D.; Monteiro, C.B.d.M. Analysis of Motor Performance in Individuals with Cerebral Palsy Using a Non-Immersive Virtual Reality Task—A Pilot Study. Neuropsychiatr. Dis. Treat. 2019, 15, 417–428. [Google Scholar] [CrossRef] [Green Version]
- da Silva, T.D.; de Oliveira, P.M.; Dionizio, J.B.; de Santana, A.P.; Bahadori, S.; Dias, E.D.; Ribeiro, C.M.; Gomes, R.D.A.; Ferreira, M.; Ferreira, C.; et al. Comparison Between Conventional Intervention and Non-Immersive Virtual Reality in the Rehabilitation of Individuals in an Inpatient Unit for the Treatment of COVID-19: A Study Protocol for a Randomized Controlled Crossover Trial. Front Psychol. 2021, 12, 622618. [Google Scholar] [CrossRef] [PubMed]
- da Silva, T.D.; Fontes, A.M.G.G.; de Oliveira-Furlan, B.S.; Roque, T.T.; Lima, A.I.I.; de Souza, B.M.M.; Alberissi, C.A.D.O.; Silveira, A.C.; de Moraes, Í.A.P.; Collett, J.; et al. Effect of Combined Therapy of Virtual Reality and Transcranial Direct Current Stimulation in Children and Adolescents With Cerebral Palsy: A Study Protocol for a Triple-Blinded Randomized Controlled Crossover Trial. Front Neurol. 2020, 11, 953. [Google Scholar] [CrossRef] [PubMed]
- Leal, A.F.; da Silva, T.D.; Lopes, P.B.; Bahadori, S.; de Araújo, L.V.; da Costa, M.V.B.; de Moraes, Í.A.P.; Marques, R.H.; Crocetta, T.B.; de Abreu, L.C.; et al. The Use of a Task through Virtual Reality in Cerebral Palsy Using Two Different Interaction Devices (Concrete and Abstract)—A Cross-Sectional Randomized Study. J. Neuroeng. Rehabil. 2020, 17, 59. [Google Scholar] [CrossRef] [PubMed]
- Crocetta, T.B.; de Araújo, L.V.; Guarnieri, R.; Massetti, T.; Ferreira, F.H.I.B.; de Abreu, L.C.; de Mello Monteiro, C.B. Virtual Reality Software Package for Implementing Motor Learning and Rehabilitation Experiments. Virtual Real. 2018, 22, 199–209. [Google Scholar] [CrossRef]
- de Mello Monteiro, C.B.; da Silva, T.D.; de Abreu, L.C.; Fregni, F.; de Araujo, L.V.; Ferreira, F.H.I.B.; Leone, C. Short-Term Motor Learning through Non-Immersive Virtual Reality Task in Individuals with down Syndrome. BMC Neurol. 2017, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Roos, L.; Taube, W.; Beeler, N.; Wyss, T. Validity of Sports Watches When Estimating Energy Expenditure during Running. BMC Sport Sci. Med. Rehabil. 2017, 9, 22. [Google Scholar] [CrossRef] [Green Version]
- Karvonen, M.J.; Kentala, E.; Mustala, O. The Effects of Training on Heart Rate; a Longitudinal Study. Ann. Med. Exp. Biol. Fenn. 1957, 35, 307–315. [Google Scholar]
- She, J.; Nakamura, H.; Makino, K.; Ohyama, Y.; Hashimoto, H. Selection of Suitable Maximum-Heart-Rate Formulas for Use with Karvonen Formula to Calculate Exercise Intensity. Int. J. Autom. Comput. 2015, 12, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Evans, E.; Naugle, K.E.; Kaleth, A.S.; Arnold, B.; Naugle, K.M. Physical Activity Intensity, Perceived Exertion, and Enjoyment during Head-Mounted Display Virtual Reality Games. Games Health J. 2021, 10, 314–320. [Google Scholar] [CrossRef]
- Naugle, K.E.; Naugle, K.M.; Wikstrom, E.A. Cardiovascular and Affective Outcomes of Active Gaming: Using the Nintendo Wii as a Cardiovascular Training Tool. J. Strength Cond. Res. 2014, 28, 443–451. [Google Scholar] [CrossRef] [Green Version]
- Jelsma, D.; Geuze, R.H.; Mombarg, R.; Smits-Engelsman, B.C.M. The Impact of Wii Fit Intervention on Dynamic Balance Control in Children with Probable Developmental Coordination Disorder and Balance Problems. Hum. Mov. Sci. 2014, 33, 404–418. [Google Scholar] [CrossRef] [PubMed]
- Smits-Engelsman, B.C.M.; Jelsma, L.D.; Ferguson, G.D. The Effect of Exergames on Functional Strength, Anaerobic Fitness, Balance and Agility in Children with and without Motor Coordination Difficulties Living in Low-Income Communities. Hum. Mov. Sci. 2017, 55, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Farhat, F.; Hsairi, I.; Baati, H.; Smits-Engelsman, B.C.M.; Masmoudi, K.; Mchirgui, R.; Triki, C.; Moalla, W. The Effect of a Motor Skills Training Program in the Improvement of Practiced and Non-Practiced Tasks Performance in Children with Developmental Coordination Disorder (DCD). Hum. Mov. Sci. 2016, 46, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Guth, D. Space Saving Statistics: An Introduction to Constant Error, Variable Error, and Absolute Error. Peabody J. Educ. 1990, 67, 110–120. [Google Scholar] [CrossRef]
- Kim, J.; Chung, S.; Tennant, L.K.; Singer, R.N.; Janelle, C.M. Minimizing Error in Measurement of Error: A Proposed Method for Calculation of Error in a Two-Dimensional Motor Task. Percept. Mot. Ski. 2000, 90, 253–261. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and Reporting Effect Sizes to Facilitate Cumulative Science: A Practical Primer for t-Tests and ANOVAs. Front Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sport Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Mineo, B.A.; Ziegler, W.; Gill, S.; Salkin, D. Engagement with Electronic Screen Media among Students with Autism Spectrum Disorders. J. Autism Dev. Disord. 2009, 39, 172–187. [Google Scholar] [CrossRef]
- Cox, D.J.; Brown, T.; Ross, V.; Moncrief, M.; Schmitt, R.; Gaffney, G.; Reeve, R. Can Youth with Autism Spectrum Disorder Use Virtual Reality Driving Simulation Training to Evaluate and Improve Driving Performance? An Exploratory Study. J. Autism Dev. Disord. 2017, 47, 2544–2555. [Google Scholar] [CrossRef]
- Ross, V.; Cox, D.J.; Reeve, R.; Brown, T.; Moncrief, M.; Schmitt, R.; Gaffney, G. Measuring the Attitudes of Novice Drivers with Autism Spectrum Disorder as an Indication of Apprehensive Driving: Going beyond Basic Abilities. Autism 2018, 22, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Patrick, K.E.; Hurewitz, F.; McCurdy, M.D.; Agate, F.T.; Daly, B.P.; Tarazi, R.A.; Chute, D.L.; Schultheis, M.T. Driving Comparisons between Young Adults with Autism Spectrum Disorder and Typical Development. J. Dev. Behav. Pediatr. 2018, 39, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Saiano, M.; Garbarino, E.; Lumachi, S.; Solari, S.; Sanguineti, V. Effect of Interface Type in the VR-Based Acquisition of Pedestrian Skills in Persons with ASD. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Milan, Italy, 25–29 August 2015; Volume 2015. [Google Scholar] [CrossRef]
- Herrero, D.; Crocetta, T.B.; Massetti, T.; Moraes, Í.A.P.; Trevizan, I.L.; Guarnieri, R.; de Rezende, G.P.; Villaça, K.P.; de Mello Monteiro, C.B. Total Reaction Time Performance of Individuals with Autism after a Virtual Reality Task. Int. J. Neurorehabil. 2015, 2, 1–5. [Google Scholar] [CrossRef]
- Bölte, S.; Golan, O.; Goodwin, M.S.; Zwaigenbaum, L. Editorial: What Can Innovative Technologies Do for Autism Spectrum Disorders? Autism 2010, 14, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Lejeune, C.; Wansard, M.; Geurten, M.; Meulemans, T. Procedural Learning, Consolidation, and Transfer of a New Skill in Developmental Coordination Disorder. Child Neuropsychol. 2016, 22, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Seidler, R.D. Aging Affects Motor Learning but Not Savings at Transfer of Learning. Learn. Mem. 2007, 14, 17–21. [Google Scholar] [CrossRef] [Green Version]
- Fernani, D.C.G.L.; Prado, M.T.A.; da Silva, T.D.; Massetti, T.; de Abreu, L.C.; Magalhães, F.H.; Dawes, H.; de Mello Monteiro, C.B. Evaluation of Speed-Accuracy Trade-off in a Computer Task in Individuals with Cerebral Palsy: A Cross-Sectional Study. BMC Neurol. 2017, 17, 143. [Google Scholar] [CrossRef] [Green Version]
- da Silva, T.D.; Ribeiro-Papa, D.C.; Coe, S.; Malheiros, S.R.P.; Massetti, T.; Meira Junior, C.D.M.; Nicolai Ré, A.H.; Collett, J.; Monteiro, C.B.D.M.; Dawes, H. Evaluation of Speed-Accuracy Trade-off in a Computer Task to Identify Motor Difficulties in Individuals with Duchenne Muscular Dystrophy—A Cross-Sectional Study. Res. Dev. Disabil. 2020, 96, 103541. [Google Scholar] [CrossRef]
- Heitz, R.P. The Speed-Accuracy Tradeoff: History, Physiology, Methodology, and Behavior. Front. Neurosci. 2014, 8, 150. [Google Scholar] [CrossRef] [Green Version]
- Heitz, R.P.; Schall, J.D. Neural Mechanisms of Speed-Accuracy Tradeoff. Neuron 2012, 76, 616–628. [Google Scholar] [CrossRef] [Green Version]
- Sharer, E.A.; Mostofsky, S.H.; Pascual-Leone, A.; Oberman, L.M. Isolating Visual and Proprioceptive Components of Motor Sequence Learning in ASD. Autism Res. 2016, 9, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Arnoni, J.L.B.; Pavão, S.L.; dos Santos Silva, F.P.; Rocha, N.A.C.F. Effects of Virtual Reality in Body Oscillation and Motor Performance of Children with Cerebral Palsy: A Preliminary Randomized Controlled Clinical Trial. Complement. Ther. Clin. Pract. 2019, 35, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Baum, S.H.; Stevenson, R.A.; Wallace, M.T. Behavioral, Perceptual, and Neural Alterations in Sensory and Multisensory Function in Autism Spectrum Disorder. Prog. Neurobiol. 2015, 134, 140–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haswell, C.C.; Izawa, J.; Dowell, L.R.; Mostofsky, S.H.; Shadmehr, R. Representation of Internal Models of Action in the Autistic Brain. Nat. Neurosci. 2009, 12, 970–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izawa, J.; Pekny, S.E.; Marko, M.K.; Haswell, C.C.; Shadmehr, R.; Mostofsky, S.H. Motor Learning Relies on Integrated Sensory Inputs in ADHD, but over-Selectively on Proprioception in Autism Spectrum Conditions. Autism Res. 2012, 5, 124–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ropar, D.; Greenfield, K.; Smith, A.D.; Carey, M.; Newport, R. Body Representation Difficulties in Children and Adolescents with Autism May Be Due to Delayed Development of Visuo-Tactile Temporal Binding. Dev. Cogn. Neurosci. 2018, 29, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heaton, P.; Hermelin, B.; Pring, L. Can Children with Autistic Spectrum Disorders Perceive Affect in Music? An Experimental Investigation. Psychol. Med. 1999, 29, 1405–1410. [Google Scholar] [CrossRef] [Green Version]
- Quintin, E.M. Music-Evoked Reward and Emotion: Relative Strengths and Response to Intervention of People With ASD. Front. Neural Circuits 2019, 13, 49. [Google Scholar] [CrossRef] [Green Version]
- Bharathi, G.; Jayaramayya, K.; Balasubramanian, V.; Vellingiri, B. The Potential Role of Rhythmic Entrainment and Music Therapy Intervention for Individuals with Autism Spectrum Disorders. J. Exerc. Rehabil. 2019, 15, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Sharda, M.; Tuerk, C.; Chowdhury, R.; Jamey, K.; Foster, N.; Custo-Blanch, M.; Tan, M.; Nadig, A.; Hyde, K. Music Improves Social Communication and Auditory–Motor Connectivity in Children with Autism. Transl. Psychiatry 2018, 8, 231. [Google Scholar] [CrossRef] [Green Version]
- Qian, J.; McDonough, D.J.; Gao, Z. The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4133. [Google Scholar] [CrossRef]
- Eichhorn, S.; Koller, V.; Schreiber, U.; Mendoza, A.; Krane, M.; Lange, R. Development of an Exergame for Individual Rehabilitation of Patients with Cardiovascular Diseases. Australas. Phys. Eng. Sci. Med. 2013, 36, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Naugle, K.E.; Carey, C.; Ohlman, T.; Godza, M.; Mikesky, A.; Naugle, K.M. Improving Active Gaming’s Energy Expenditure in Healthy Adults Using Structured Playing Instructions for the Nintendo Wii and Xbox Kinect. J. Strength Cond. Res. 2019, 33, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Shen, M.; Wang, Y.X.; He, Z.W.; Chi, S.Q.; Yang, Z.H. Effect of Virtual Reality on Balance and Gait Ability in Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis. Clin. Rehabil. 2019, 33, 1130–1138. [Google Scholar] [CrossRef] [PubMed]
- Román-Oyola, R.; Figueroa-Feliciano, V.; Torres-Martínez, Y.; Torres-Vélez, J.; Encarnación-Pizarro, K.; Fragoso-Pagán, S.; Torres-Colón, L. Play, Playfulness, and Self-Efficacy: Parental Experiences with Children on the Autism Spectrum. Occup. Ther. Int. 2018, 2018, 4636780. [Google Scholar] [CrossRef] [PubMed]
- Skard, G.; Bundy, A.C. Test of Playfulness. In Play in Occupational Therapy for Children; Mosby: Boston, MA, USA, 2008. [Google Scholar] [CrossRef]
- Jin, J.; Yun, J.; Agiovlasitis, S. Impact of Enjoyment on Physical Activity and Health among Children with Disabilities in Schools. Disabil. Health J. 2018, 11, 14–19. [Google Scholar] [CrossRef]
- Moraes, Í.A.P.; Silva, T.D.; Massetti, T.; Menezes, L.D.C.; Ribeiro, V.F.; Tropiano, L.M.C.C.; Barnabé, V.; Hoshi, R.A.; Monteiro, C.B.M.; Fernandes, M. Fractal Correlations and Linear Analyses of Heart Rate Variability in Healthy Young People with Different Levels of Physical Activity. Cardiol. Young 2019, 29, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Dias, R.M.; Moraes, Í.A.P.; Dantas, M.T.A.P.; Fernani, D.C.G.L.; Fontes, A.M.G.G.; Silveira, A.C.; Barnabé, V.; Fernandes, M.; Martinelli, P.M.; Monteiro, C.B.M.; et al. Influence of Chronic Exposure to Exercise on Heart Rate Variability in Children and Adolescents Affected by Obesity: A Systematic Review and Meta-Analysis. Int. J. Environ Res. Public Health 2021, 18, 11065. [Google Scholar] [CrossRef]
- Silveira, A.C.; Moraes, Í.A.P.; Vidigal, G.P.; Simcsik, A.O.; Rosa, R.M.; Favero, F.M.; Fernandes, S.M.S.; Garner, D.M.; Araújo, L.V.; Massa, M.; et al. Cardiac Autonomic Modulation in Subjects with Amyotrophic Lateral Sclerosis (ALS) during an Upper Limb Virtual Reality Task: A Prospective Control Trial. Biomed Res. Int. 2022, 2022, 4439681. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence A | Sequence B | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| CI (LL, UL) | CI (LL, UL) | ||
| Age—years | 14.1 ± 1.7 | 13.9 ± 1.9 | 0.822 |
| (12, 15) | (12, 15) | ||
| Height—meters | 1.65 ± 0.13 | 1.67 ± 0.11 | 0.693 |
| (1.57, 1.73) | (1.59, 1.75) | ||
| Weight—kilograms | 61.9 ± 14.8 | 63.0 ± 18.8 | 0.877 |
| (51, 72) | (52, 73) | ||
| BMI | 22.0 ± 4.0 | 22.0 ± 6.0 | 0.899 |
| (19, 25) | (19, 25) | ||
| IQ | 87.6 ± 11.3 | 83.13 ± 13.6 | 0.412 |
| (79, 95) | (75, 91) | ||
| CARS | 34.3 ± 1.3 | 33.7 ± 1.7 | 0.348 |
| (33, 35) | (32, 34) | ||
| PEDI—FS | 89.6 ± 11.3 | 91.8 ± 10.1 | 0.648 |
| Self-Care | (82, 96) | (85, 98) | |
| PEDI—FS | 66.3 ± 7.7 | 67.7 ± 1.6 | 0.586 |
| Mobility | (62, 69) | (64, 71) | |
| PEDI—FS | 77.5 ± 9.8 | 77.8 ± 9.9 | 0.947 |
| Social Function | (71, 83) | (71, 84) | |
| PEDI—CA | 94.2 ± 9.0 | 97.0 ± 6.7 | 0.419 |
| Self-Care | (89, 99) | (92, 102) | |
| PEDI—CA | 92.4 ± 15.0 | 96.8 ± 5.7 | 0.377 |
| Mobility | (85, 99) | (89, 103) | |
| PEDI—CA | 88.0 ± 11.5 | 87.1 ± 12.8 | 0.867 |
| Social Function | (80, 95) | (79, 94) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moraes, Í.A.P.; Lima, J.A.; Silva, N.M.; Simcsik, A.O.; Silveira, A.C.; Menezes, L.D.C.; Araújo, L.V.; Crocetta, T.B.; Voos, M.C.; Tonks, J.; et al. Effect of Longitudinal Practice in Real and Virtual Environments on Motor Performance, Physical Activity and Enjoyment in People with Autism Spectrum Disorder: A Prospective Randomized Crossover Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 14668. https://doi.org/10.3390/ijerph192214668
Moraes ÍAP, Lima JA, Silva NM, Simcsik AO, Silveira AC, Menezes LDC, Araújo LV, Crocetta TB, Voos MC, Tonks J, et al. Effect of Longitudinal Practice in Real and Virtual Environments on Motor Performance, Physical Activity and Enjoyment in People with Autism Spectrum Disorder: A Prospective Randomized Crossover Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(22):14668. https://doi.org/10.3390/ijerph192214668
Chicago/Turabian StyleMoraes, Íbis A. P., Joyce A. Lima, Nadja M. Silva, Amanda O. Simcsik, Ana C. Silveira, Lilian D. C. Menezes, Luciano V. Araújo, Tânia B. Crocetta, Mariana C. Voos, James Tonks, and et al. 2022. "Effect of Longitudinal Practice in Real and Virtual Environments on Motor Performance, Physical Activity and Enjoyment in People with Autism Spectrum Disorder: A Prospective Randomized Crossover Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 22: 14668. https://doi.org/10.3390/ijerph192214668
APA StyleMoraes, Í. A. P., Lima, J. A., Silva, N. M., Simcsik, A. O., Silveira, A. C., Menezes, L. D. C., Araújo, L. V., Crocetta, T. B., Voos, M. C., Tonks, J., Silva, T. D., Dawes, H., & Monteiro, C. B. M. (2022). Effect of Longitudinal Practice in Real and Virtual Environments on Motor Performance, Physical Activity and Enjoyment in People with Autism Spectrum Disorder: A Prospective Randomized Crossover Controlled Trial. International Journal of Environmental Research and Public Health, 19(22), 14668. https://doi.org/10.3390/ijerph192214668