
Validity of the Baiobit Inertial Measurements Unit for the Assessment of Vertical Double- and Single-Leg Countermovement Jumps in Athletes

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
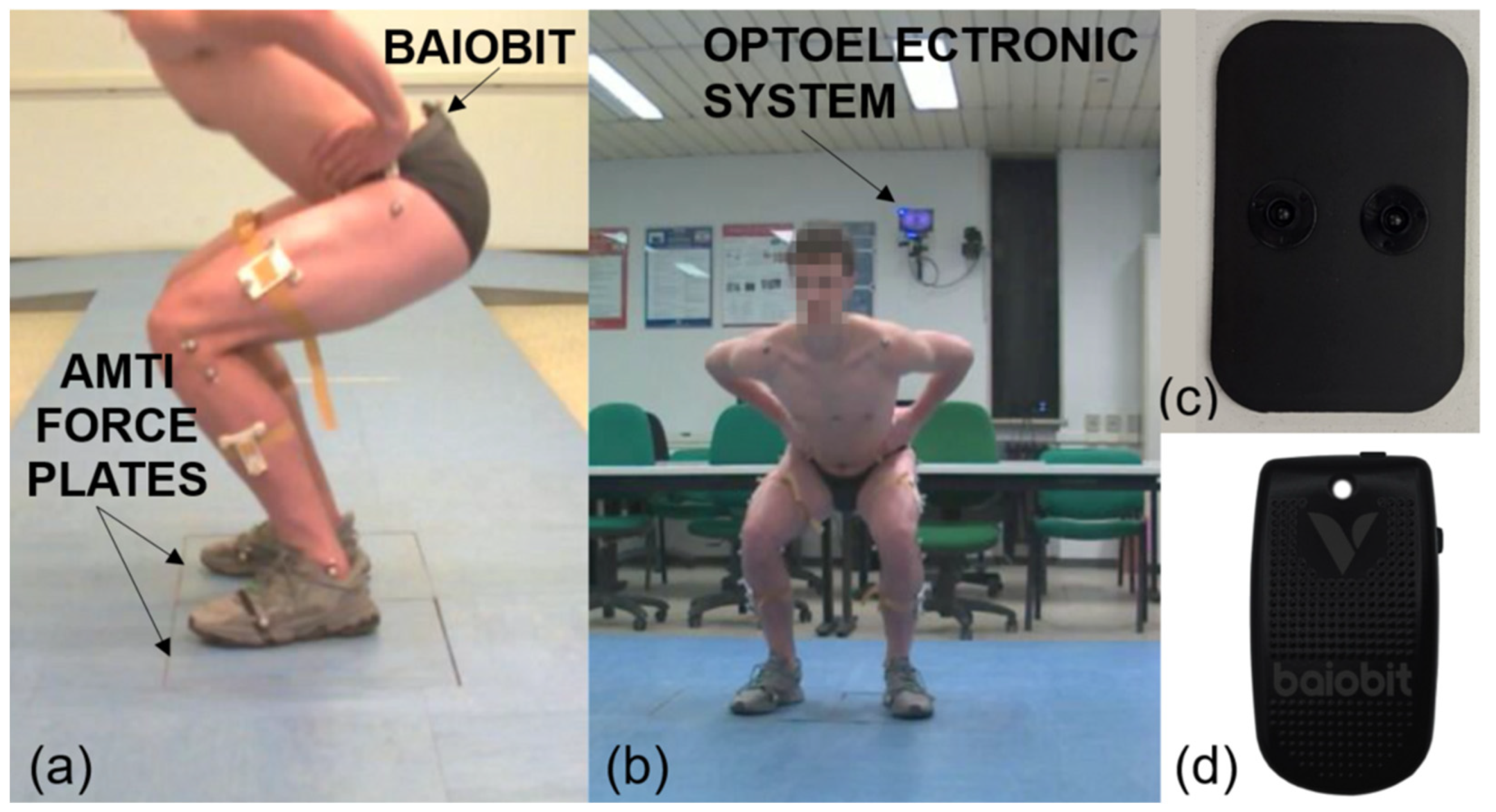
2.2. Devices
- A Baiobit sensor, comprising a triaxial accelerometer with multiple sensitivity levels (±2, ±4, ±8, and ±16 g); a 13-bit triaxial magnetometer (±1200 µT); and a triaxial gyroscope with multiple sensitivity levels (±250, ±500, ±1000, and ±2000°/s), manufactured by Rivelo Srl—BTS bioengineering Group, Milan, Italy. The Baiobit sensor works with an accelerometer frequency bandwidth ranging from 4 to 1000 Hz, a gyroscope bandwidth ranging from 4 to 8000 Hz, a magnetometer bandwidth up to 100 Hz, and sensor fusion up to 200 Hz. The Baiobit sensor has inter-instrument correlation coefficient ranging between 0.90 and 0.99, and an intra-instrument coefficient of variation of ≤2.5%, making it suitable for the assessment of physical activity with the same technical specifications of G-WALK (BTS Bioengineering, Garbagnate, Italy) [16,17,18].
- Two three-dimensional AMTI force platforms (dimensions: 464 × 508 × 82.5 mm; AMTI, Wetertown, MA, USA, sampling rate = 200 Hz).
- An optoelectronic system composed by an eight-infrared camera (BTS Bioengineering, Garbagnate, Italy).
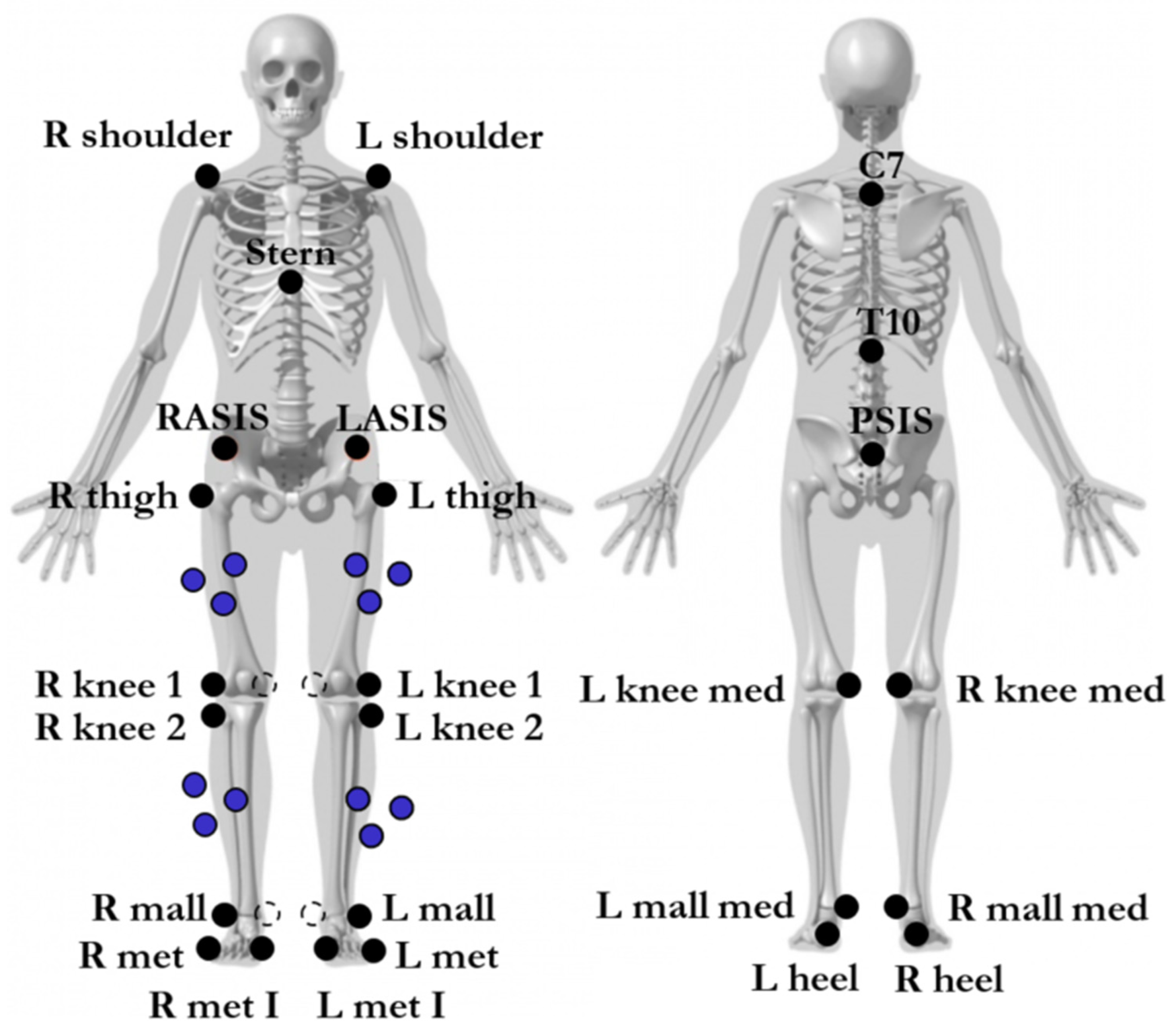
2.3. Procedures
2.4. Data Analysis
2.5. Statistica Analysis
3. Results
4. Discussion
4.1. Limitations and Possible Bias
4.2. Future Developments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fares, M.Y.; Khachfe, H.H.; Salhab, H.A.; Bdeir, A.; Fares, J.; Baydoun, H. Physical Testing in Sports Rehabilitation: Implications on a Potential Return to Sport. Arthrosc. Sport. Med. Rehabil. 2022, 4, e189–e198. [Google Scholar] [CrossRef]
- Kotsifaki, A.; Korakakis, V.; Graham-Smith, P.; Sideris, V.; Whiteley, R. Vertical and Horizontal Hop Performance: Contributions of the Hip, Knee, and Ankle. Sports Health 2021, 13, 128–135. [Google Scholar] [CrossRef]
- Lesinski, M.; Muehlbauer, T.; Granacher, U. Concurrent validity of the Gyko inertial sensor system for the assessment of vertical jump height in female sub-elite youth soccer players. BMC Sports Sci. Med. Rehabil. 2016, 8, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, J.B.; Ford, K.R.; Nguyen, A.D.; Shultz, S.J. Biomechanical Comparison of Single- and Double-Leg Jump Landings in the Sagittal and Frontal Plane. Orthop. J. Sport. Med. 2016, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whatman, C.; Hing, W.; Hume, P. Physiotherapist agreement when visually rating movement quality during lower extremity functional screening tests. Phys. Ther. Sport 2012, 13, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Bird, S.P.; Markwick, W.J. Musculoskeletal Screening and Functional Testing: Considerations for Basketball Athletes. Int. J. Sports Phys. Ther. 2016, 11, 784–802. [Google Scholar] [PubMed]
- Lu, T.W.; Chang, C.F. Biomechanics of human movement and its clinical applications. Kaohsiung J. Med. Sci. 2012, 28, S13–S25. [Google Scholar] [CrossRef]
- Ancillao, A. An experimental analysis of the sources of inaccuracy occurring in hip strength measurements conducted by hand held dynamometry. Eur. J. Physiother. 2021, 23, 110–115. [Google Scholar] [CrossRef]
- Ancillao, A. A New Method for the Quality Assurance of Strength Measurements. In Modern Functional Evaluation Methods for Muscle Strength and Gait Analysis; Springer: Cham, Switzerland, 2018; pp. 31–88. [Google Scholar] [CrossRef]
- Vastola, R.; Medved, V.; Albano, D.; Coppola, S.; Sibilio, M. Use of Optoelectronic Systems for the Analysis of Technique in Trials. J. Sport. Sci. 2016, 4, 293–299. [Google Scholar] [CrossRef]
- Nielsen, E.T.; Jørgensen, P.B.; Mechlenburg, I.; Sørensen, H. Validation of an inertial measurement unit to determine countermovement jump height. Asia-Pacific J. Sport. Med. Arthrosc. Rehabil. Technol. 2019, 16, 8–13. [Google Scholar] [CrossRef]
- Gadev, M.; Peev, P.; Hristov, O. Agreeement Between Measurement of Jump Height in Different Vertical Jump Tests Executed By Young Football Players. J. Appl. Sport. Sci. 2020, 2, 51–63. [Google Scholar] [CrossRef]
- Picerno, P.; Camomilla, V.; Capranica, L. Countermovement jump performance assessment using a wearable 3D inertial measurement unit. J. Sports Sci. 2011, 29, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Yazici, G.; Yazici, M.V.; Çobanoğlu, G.; Küpeli, B.; Özkul, Ç.; Oskay, D.; Güzel, N.A. The reliability of a wearable movement analysis system (G-walk) on gait and jump assessment in healthy adults. J. Exerc. Ther. Rehabil. 2020, 7, 159–167. [Google Scholar]
- Requena, B.; Requena, F.; García, I.; de Villarreal, E.S.S.; Pääsuke, M. Reliability and validity of a wireless microelectromechanicals based system (Keimove TM) for measuring vertical jumping performance. J. Sport. Sci. Med. 2012, 11, 115–122. [Google Scholar]
- Sankarpandi, S.K.; Baldwin, A.J.; Ray, J.; Mazzà, C. Reliability of inertial sensors in the assessment of patients with vestibular disorders: A feasibility study. BMC Ear Nose Throat Disord. 2017, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an Accelerometer to Quantify a Comprehensive Battery of Gait Characteristics in Healthy Older Adults and Parkinson’s Disease: Toward Clinical and at Home Use. IEEE J. Biomed. Health Inform. 2016, 20, 838–847. [Google Scholar] [CrossRef] [Green Version]
- Gieysztor, E.; Kowal, M.; Paprocka-Borowicz, M. Gait parameters in healthy preschool and school children assessed using wireless inertial sensor. Sensors 2021, 21, 6423. [Google Scholar] [CrossRef]
- Rivelo. User Manual Baiobit; Rivelo: Garbagnate Milanese, Italy, 2021; pp. 99–109, 174–178. [Google Scholar]
- Lloyd, R.S.; Oliver, J.L.; Hughes, M.G.; Williams, C.A. Reliability and validity of field-based measures of leg stiffness and reactive strength index in youths. J. Sports Sci. 2009, 27, 1565–1573. [Google Scholar] [CrossRef]
- Flanagan, E.P.; Comyns, T.M. The use of contact time and the reactive strength index to optimize fast stretch-shortening cycle training. Strength Cond. J. 2008, 30, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Struzik, A.; Pietraszewski, B.; Zawadzki, J. Biomechanical analysis of the jump shot in basketball. J. Hum. Kinet. 2014, 42, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Mannocci, A.; Di Thiene, D.; Del Cimmuto, A.; Masala, D.; Boccia, A.; De Vito, E.; La Torre, G. International Physical Activity Questionnaire: Validation and assessment in an Italian sample. Ital. J. Public Health 2010, 7, 369–376. [Google Scholar]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A study of concurrent and construct validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Rantalainen, T.; Finni, T.; Walker, S. Jump height from inertial recordings: A tutorial for a sports scientist. Scand. J. Med. Sci. Sport. 2020, 30, 38–45. [Google Scholar] [CrossRef]
- Van Stralen, K.J.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Measuring agreement, more complicated than it seems. Nephron Clin. Pract. 2012, 120, c162–c167. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.P.; Clifford, T.; Abbott, W.; Kwiecien, S.Y.; Kremenic, I.J.; DeVita, J.J.; Howatson, G. Countermovement Jump Recovery in Professional Soccer Players Using an Inertial Sensor. Hum. Kinet. 2019, 14, 9–15. [Google Scholar] [CrossRef]
- Brooks, E.R.; Benson, A.C.; Bruce, L.M. Novel technologies found to be valid and reliable for the measurement of vertical jump height with jump-and-reach testing. J. Strength Cond. Res. 2018, 32, 2838–2845. [Google Scholar] [CrossRef]
- Glatthorn, J.F.; Gouge, S.; Nussbaumer, S.; Stauffacher, S.; Impellizzeri, F.M.; Maffiuletti, N.A. Validity and reliability of the Optojump Photoelectic cells for estimating vertical jump height. J. Strength Cond. Res. 2011, 25, 556–560. [Google Scholar] [CrossRef]
- Nalbant, Ö. Comparison of Physical and Motoric Features of Children Continuous the Sport School. J. Educ. Train. Stud. 2017, 5, 1. [Google Scholar] [CrossRef] [Green Version]
- Ancillao, A.; Aertbeliën, E.; De Schutter, J. Effect of the soft tissue artifact on marker measurements and on the calculation of the helical axis of the knee during a gait cycle: A study on the CAMS-Knee data set. Hum. Mov. Sci. 2021, 80, 102866. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject (ID) | Sex | Age (Years) | Weight (kg) | Height (m) | Sport | IPAQ |
|---|---|---|---|---|---|---|
| 1 | F | 36 | 73 | 1.85 | beach volley | VA |
| 2 | M | 26 | 77 | 1.82 | triathlon | SA |
| 3 | M | 27 | 86 | 1.91 | volleyball | VA |
| 4 | M | 22 | 81 | 1.92 | basket | VA |
| 5 | M | 27 | 85 | 1.92 | basket | VA |
| 6 | M | 23 | 80 | 1.91 | swimming | SA |
| 7 | M | 28 | 97 | 1.91 | jiu jitsu | SA |
| 8 | M | 28 | 65 | 1.78 | triathlon | SA |
| 9 | F | 24 | 47 | 1.64 | athletics | VA |
| 10 | M | 23 | 92 | 2.02 | volleyball | SA |
| 11 | M | 21 | 62 | 1.85 | volleyball | VA |
| 12 | M | 21 | 69 | 1.81 | tennis | VA |
| 13 | M | 20 | 83 | 1.94 | basket | VA |
| 14 | M | 37 | 93 | 1.95 | beach volley | VA |
| 15 | M | 24 | 71 | 1.76 | tennis | VA |
| 16 | M | 36 | 76 | 1.89 | volleyball | VA |
| 17 | F | 19 | 69 | 1.86 | volleyball | VA |
| 18 | F | 31 | 76 | 1.90 | volleyball | SA |
| 19 | M | 41 | 80 | 1.83 | triathlon | VA |
| 20 | M | 38 | 75 | 1.83 | beach volley | VA |
| 21 | F | 22 | 59 | 1.74 | volleyball | SA |
| 22 | F | 19 | 68 | 1.82 | volleyball | VA |
| 23 | M | 24 | 87 | 1.97 | volleyball | SA |
| 24 | M | 39 | 72 | 1.82 | beach volley | VA |
| 25 | M | 21 | 70 | 1.86 | volleyball | VA |
| 26 | F | 21 | 54 | 1.68 | volleyball | SA |
| 27 | M | 23 | 85 | 1.92 | basket | VA |
| MEAN ± SD | 20 M—7 F | 27 ± 7 | 75 ± 12 | 186 ± 0.09 | 18 VA—9 SA |
| Parameter | Definition | References |
|---|---|---|
| Flight time (s) | Time between take-off and landing | [20] |
| Contact time (s) | Time elapsing between the start of the jump and the take-off | [20] |
| Jump height (m) | 1.266 × flight time2 | [20,21] |
| Reactivity index (-) | Flight time/contact time | |
| Force take-off (KN) | Maximum value of the force during take-off Expressed in % of body mass | [22] |
| Impact ratio (-) | Force landing/force take-off | [22] |
| Double-Leg CMJ | Single-Leg CMJ | |
|---|---|---|
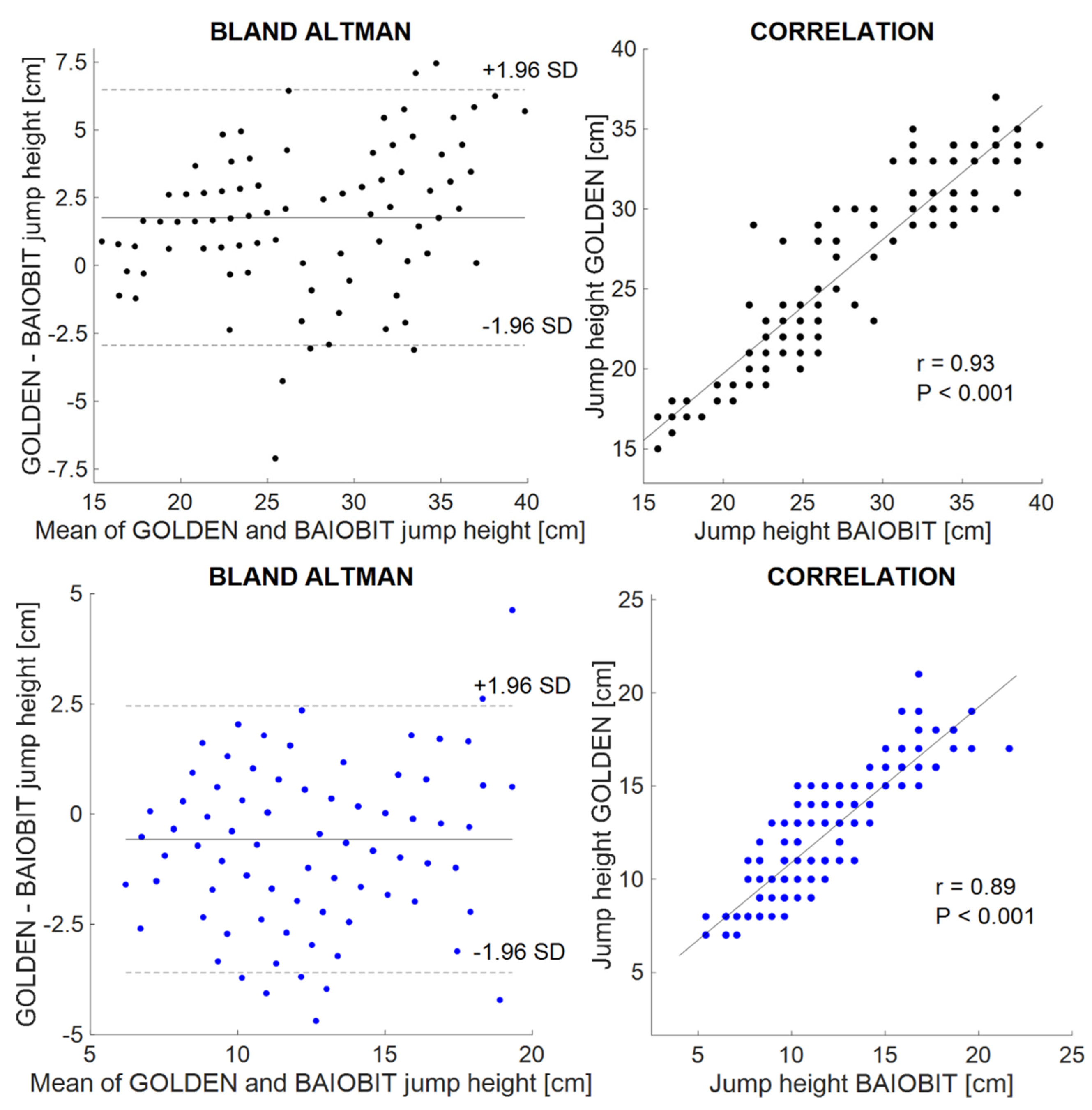
| AMTI force plates [cm] | 29.1 ± 6.3 | 12.0 ± 3.3 |
| Baiobit sensor [cm] | 27.4 ± 5.7 | 12.6 ± 3.1 |
| Systematic bias [cm] | 1.8 | −0.6 |
| Random error [cm] | ±4.7 | ±3.0 |
| Lower LoA | −2.9 | −3.6 |
| Upper LoA | 6.5 | 2.5 |
| ICC (95% CI) | 0.92 (0.89–0.94) | 0.89 (0.85–0.91) |
| Double-Leg CMJ | Single-Leg CMJ | |
|---|---|---|
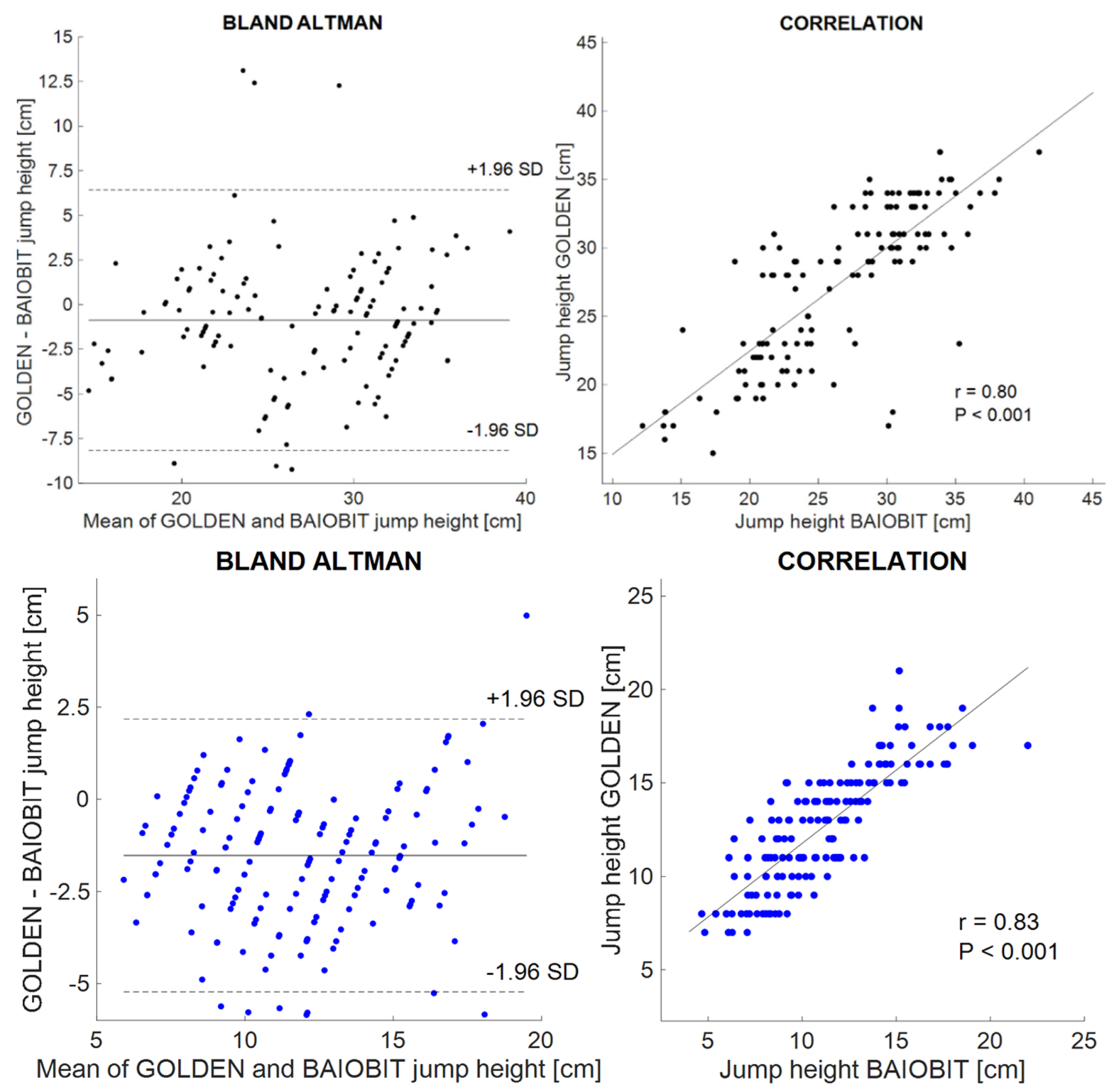
| Optoelectronic system + AMTI force plates [cm] | 26.5 ± 6.1 | 11.6 ± 3.3 |
| Baiobit sensor [cm] | 27.4 ± 5.7 | 12.6 ± 3.1 |
| Systematic bias [cm] | −0.9 | −1.2 |
| Random error [cm] | ±7.3 | ±3.5 |
| Lower LoA | −8.2 | −4.6 |
| Upper LoA | 6.4 | 2.3 |
| ICC (95% CI) | 0.80 (0.73–0.85) | 0.86 (0.80–0.89) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camuncoli, F.; Barni, L.; Nutarelli, S.; Rocchi, J.E.; Barcillesi, M.; Di Dio, I.; Sambruni, A.; Galli, M. Validity of the Baiobit Inertial Measurements Unit for the Assessment of Vertical Double- and Single-Leg Countermovement Jumps in Athletes. Int. J. Environ. Res. Public Health 2022, 19, 14720. https://doi.org/10.3390/ijerph192214720
Camuncoli F, Barni L, Nutarelli S, Rocchi JE, Barcillesi M, Di Dio I, Sambruni A, Galli M. Validity of the Baiobit Inertial Measurements Unit for the Assessment of Vertical Double- and Single-Leg Countermovement Jumps in Athletes. International Journal of Environmental Research and Public Health. 2022; 19(22):14720. https://doi.org/10.3390/ijerph192214720
Chicago/Turabian StyleCamuncoli, Federica, Luca Barni, Sebastiano Nutarelli, Jacopo Emanuele Rocchi, Matteo Barcillesi, Irene Di Dio, Andrea Sambruni, and Manuela Galli. 2022. "Validity of the Baiobit Inertial Measurements Unit for the Assessment of Vertical Double- and Single-Leg Countermovement Jumps in Athletes" International Journal of Environmental Research and Public Health 19, no. 22: 14720. https://doi.org/10.3390/ijerph192214720
APA StyleCamuncoli, F., Barni, L., Nutarelli, S., Rocchi, J. E., Barcillesi, M., Di Dio, I., Sambruni, A., & Galli, M. (2022). Validity of the Baiobit Inertial Measurements Unit for the Assessment of Vertical Double- and Single-Leg Countermovement Jumps in Athletes. International Journal of Environmental Research and Public Health, 19(22), 14720. https://doi.org/10.3390/ijerph192214720