
Evaluation of Synchronous and Asynchronous Telemedical Applications in Primary Care in Rural Regions of Northern Germany—Results and Lessons Learned from a Pilot Study


Abstract
:1. Introduction
1.1. Synchronous Video Liaison Consultations of GPs with Patient and Ophthalmologist
1.2. Asynchronous Teledermatological Consultations
1.3. Usage of Digital Vital Sensors by a Medical Assistant during Home Visits
2. Materials and Methods
2.1. Synchronous Video Liaison Consultations of GPs with Patient and Ophthalmologist
2.2. Asynchronous Teledermatological Consultations
2.3. Usage of Digital Vital Sensors by a Medical Assistant during Home Visits
2.4. Duration of the Study and Used Equipment
2.5. Evaluation
2.5.1. Shared Items in the Evaluation of TAs
- gender of patient;
- year of birth of patient;
- reason for the consultation;
- result of consultation;
- doctor’s/MFA’s assessment of the benefit for the patients.
2.5.2. Unique Items in the Evaluation of the Synchronous Video Liaison Consultations
2.5.3. Unique Items in the Evaluation of the Digital Vital Sensors by an MFA during Home Visits
2.5.4. Documentation of Asynchronous Teledermatological Consultations
3. Results
3.1. Video Liaison Consultations of GPs with Patient and Ophthalmologist
3.2. Asynchronous Teledermatological Consultations
- Local reaction after animal bite ×2.
- Atopic eczema ×2.
- Mycosis ×2.
- Stasis dermatitis.
- Scabies.
- Herpes-like infection.
- Skin lesion nose.
- Dermal scar.
- Urticaria.
- Rosacea or acne.
- Varicella zoster.
- Majorca callus.
- Alopecia areata.
- Itching, knee + left thigh.
- Eczema left wrist.
- Redness, swelling right wrist.
- Unclear ×5.
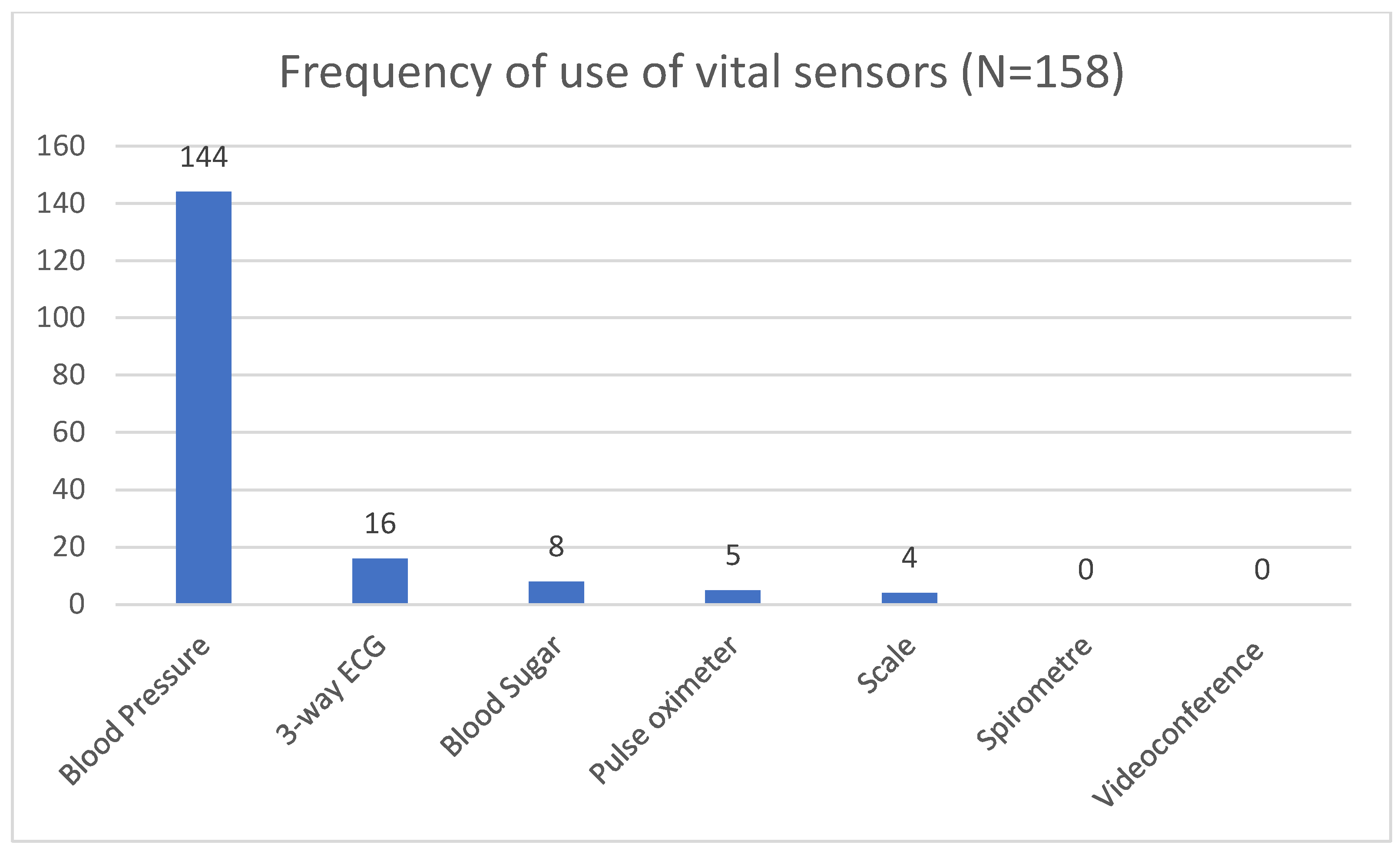
3.3. Usage of Digital Vital Sensors by an MFA during Home Visits
4. Discussion
4.1. Lessons Learned
- Checking the availability of broadband internet access, both mobile and stationary seems trivial today, but makes still sense especially in rural areas, in order to eliminate a frustration barrier.
- Examining the regional situation helps to avoid investing effort in the implementation of unnecessary TAs. Not every application is suitable for every practice due to regional circumstances [33].
- Allow enough time for testing and training the use of the applications. A well-developed training concept right at the beginning of the implementation helps immensely.
- Think about a technical support plan. If the TA does not work in a used case and no immediate support is available, the willingness to use it will drop sharply.
- Regular contact with the practices, ideally using the very same technology helps to further deepen the know-how initially gained in the training sessions and generates confidence in the use of the technology [35].
- Does it work asynchronously? Our pilot study suggests that asynchronous TAs are easier to implement in the workflow of practices. The fact that two doctors do not have to be available online at the same and the lesser demand of broadband internet time makes implementation much easier.
4.2. Limitation
5. Conclusions
6. Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steinhäuser, J.; Scheidt, L.; Szecsenyi, J.; Goetz, K.; Joos, S. Perceptions of the local government about the primary care physicians shortage - A survey among mayors in the federal state of Baden-Wuerttemberg. Gesundheitswesen 2012, 74, 612–617. (In German) [Google Scholar] [PubMed]
- Popert, U.; Egidi, G.; Eras, J.; Kühlein, T.; Baum, E. Why we need a primary care system. Z. Allgemeinmed 2018, 94, 250–254. (In German) [Google Scholar]
- Scheidt, L.R.S.; Joos, S.; Szecsenyi, J.; Steinhäuser, J. Oversupplied? Undersupplied? —The perspective of local governments of the federal state of Baden-Württemberg: A contribution to the discussion of close-to-home health care. Gesundheitswesen 2015, 77, e179–e183. (In German) [Google Scholar] [CrossRef]
- Schröder, L.; Flägel, K.; Goetz, K.; Steinhäuser, J. Mobility concepts and access to health care in a rural district in Germany: A mixed methods approach. BMC Fam. Pract. 2018, 19, 47. [Google Scholar] [CrossRef] [Green Version]
- Bardsley, M.; Steventon, A.; Doll, H. Impact of telehealth on general practice contacts: Findings from the whole systems demonstrator cluster randomised trial. BMC Health Serv. Res. 2013, 13, 395. [Google Scholar] [CrossRef] [Green Version]
- Piette, E.; Nougairède, M.; Vuong, V.; Crickx, B.; Tran, V.-T. Impact of a store-and-forward teledermatology intervention versus usual care on delay before beginning treatment: A pragmatic cluster-randomized trial in ambulatory care. J. Telemed. Telecare 2017, 23, 725–732. [Google Scholar] [CrossRef]
- Ardielli, E. Implementation of eHealth applications by primary care physicians in the European Union member states. Int. J. Electron. Healthc. 2021, 11, 378–398. [Google Scholar] [CrossRef]
- Haserück, A. The majority of German doctors see opportunities above all else. Dtsch. Arztebl. 2022, 119, A–1778/B–1486. (In German) [Google Scholar]
- National Association of Statutory Health Insurance Physicians (KBV). Schlussfolgerungen Praxisbarometer Digitalisierung 2021. Available online: https://www.kbv.de/media/sp/Schlussfolgerungen_Praxisbarometer_2021.pdf (accessed on 28 October 2022).
- Waschkau, A.; Zwierlein, R.; Steinhäuser, J. Barriers and enablers for telemedical applications in family physicians’ practices—Qualitative results of a pilot study. Z. Allg. Med. 2019, 95, 405–412. (In German) [Google Scholar]
- Advisory Council on the Assessment of Developments in the Health Care System. Coordination and Integration—Health Care in an Ageing Society. Available online: https://www.svr-gesundheit.de/fileadmin/Gutachten/Sondergutachten_2009/Kurzfassung_engl_2009.pdf (accessed on 14 September 2022).
- Waschkau, A.; Steinhäuser, J. Change in needs for video consultations in times of a pandemic—A qualitative observation. Z. Allg. Med. 2020, 9, 317–324. (In German) [Google Scholar]
- Steinhäuser, J. Inhaltliche Verbesserung weiterbildungsbegleitender Lerngruppen durch Daten des CONTENT-Projekts. In Versorgungsforschung in der Hausarztpraxis. Ergebnisse aus dem CONTENT-Projekt 2006-2009; Laux, G., Kühlein, T., Gutscher, A., Szecsenyi, J., Eds.; Springer Medizin: Munich, Germany, 2010; pp. 48–55. (In German) [Google Scholar]
- Rosenbaum, B.E.; Campion, C.H.; Cohen, J.M.; Latkowski, J.A. The Department of Defense: Pioneers of early teledermatology. Dermatol. Online J. 2017, 23. [Google Scholar] [CrossRef]
- Lee, J.J.; English, J.C., III. Teledermatology: A review and update. Am. J. Clin. Dermatol. 2018, 19, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Lozzi, G.P.; Soyer, H.P.; Massone, C.; Micantonio, T.; Kraenke, B.; Fargnoli, M.C.; Fink-Puches, R.; Binder, B.; Di Stefani, A.; Hofmann-Wellenhof, R.; et al. The additive value of second opinion teleconsulting in the management of patients with challenging inflammatory, neoplastic skin diseases: A best practice model in dermatology? J. Eur. Acad. Dermatol. Venereol. 2007, 21, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Whited, J.D.; Hall, R.P.; Simel, D.L.; Foy, M.E.; Stechuchak, K.M.; Drugge, R.J.; Grichnik, J.M.; Myers, S.A.; Horner, R.D. Reliability and accuracy of dermatologists’ clinic-based and digital image consultations. J. Am. Acad. Dermatol. 1999, 41, 693–702. [Google Scholar] [CrossRef]
- van der Heijden, J.P.; de Keizer, N.F.; Bos, J.D.; Spuls, P.I.; Witkamp, L. Teledermatology applied following patient selection by general practitioners in daily practice improves efficiency and quality of care at lower cost. Br. J. Dermatol. 2011, 165, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Goetz, K.; Kornitzky, A.; Mahnkopf, J.; Steinhäuser, J. At the dawn of delegation? Experiences and attitudes of general practitioners in Germany—A questionnaire survey. BMC Fam. Pract. 2017, 18, 102. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, N.; Heymann, R.; Meinke, C.; Baumeister, S.E.; Flea, S.; Hoffmann, W. Effect of the delegation of GP-home visits on the development of the number of patients in an ambulatory healthcare centre in Germany. BMC Health Serv. Res. 2012, 12, 355. [Google Scholar] [CrossRef] [Green Version]
- Waschkau, A.; Uebel, T.; Steinhäuser, J. Diabetes treatment 2.0: Telemedicine. Internist 2019, 60. [Google Scholar] [CrossRef] [Green Version]
- Abbott-Garner, P.; Richardson, J.; Jones, R.B. The impact of superfast broadband, tailored booklets for households, and discussions with general practitioners on personal electronic health readiness: Cluster factorial quasi-randomized control trial. J. Med. Internet. Res. 2019, 21, e11386. [Google Scholar] [CrossRef] [Green Version]
- Boyland, P. The state of mobile network experience. Open Signal. May 2019. Available online: https://cdn.opensignal.com/public/data/reports/global/data-2019-05/the_state_of_mobile_experience_may_2019_0.pdf. (accessed on 22 September 2022).
- Steventon, A.; Bardsley, M.; Doll, H.; Tuckey, E.; Newmann, S.P. Effect of telehealth on glycaemic control: Analysis of patients with type 2 diabetes in the whole systems demonstrator cluster randomised trial. BMC Health Serv. Res. 2014, 14, 334. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann-Petersen, N.; Lauritzen, T.; Bech, J.N.; Pedersen, E.B. Short-term telemedical home blood pressure monitoring does not improve blood pressure in uncomplicated hypertensive patients. J. Hum. Hypertens. 2017, 31, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Nicolucci, A.; Cercone, S.; Chiriatti, A.; Muscas, F.; Gensini, G. A randomized trial on home telemonitoring for the management of metabolic and cardiovascular risk in patients with Type 2 Diabetes. Diabetes Technol. The. 2015, 17, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Strumann, C.; von Meißner, W.C.G.; Blickle, P.G.; Held, L.; Steinhäuser, J. Experiences made by family physicians managing patients with SARS-CoV-2 infection during spring 2020—A cross-sectional analysis. Z. Evid. Fortbild. Qual. Gesundhwes. 2021, 165, 35–42. [Google Scholar] [CrossRef]
- National Association of Statutory Health Insurance Physicians (KBV). Fee Report 2nd Quarter 2020. Available online: https://www.kbv.de/media/sp/Honorarbericht_Quartal_2_2020.pdf (accessed on 28 October 2022).
- Krüger-Brand, H. Telemedizin: Kräftiger Schub für Videosprechstunden. Dtsch. Arztebl. 2020. Available online: https://www.aerzteblatt.de/nachrichten/110997/Telemedizin-Kraeftiger-Schub-fuer-Videosprechstunden (accessed on 28 October 2022).
- López-Liria, R.; Valverde-Martínez, M.Á.; López-Villegas, A.; Bautista-Mesa, R.J.; Vega-Ramirez, F.A.; Peiró, S.; Leal-Costa, C. Teledermatology versus face-to-face dermatology: An analysis of cost-effectiveness from eight studies from Europe and the United States. Int. J. Environ. Res. Public Health 2022, 22, 2534. [Google Scholar] [CrossRef]
- Strumann, C.; Steinhäuser, J. Evaluation of a direct-to-patient telehealth service in Germany (docdirekt) based on routine data. Dtsch. Arztebl. Int. 2021, 118, 872–873. [Google Scholar] [CrossRef] [PubMed]
- Miralles, J.G.; Heintze, C.; Dini, L. Delegation modalities for general practitioners in North Rhine-Westphalia: Results of a survey among general practitioners on the assignment of defined tasks to EVA, VERAH and VERAH Plus. Germany. Z. Evid. Fortbild. Qual. Gesundhwes. 2020, 156, 50–58. [Google Scholar]
- Kuhn, B.; Kleij, K.S.; Liersch, S.; Steinhäuser, J.; Amelung, V.E. Which strategies might improve local primary healthcare in Germany? An explorative study from a local government point of view. BMC Fam. Pract. 2017, 18, 105. [Google Scholar] [CrossRef] [Green Version]
- Held, L.A.; Wewetzer, L.; Steinhäuser, J. Determinants of the implementation of an artificial intelligence-supported device for the screening of diabetic retinopathy in primary care—A qualitative study. Health Inform. J. 2022, 28, 14604582221112816. [Google Scholar] [CrossRef]
- Hötker, D.; Ring, M.; Steinhäuser, J. Determinants of the implementation of telemedicine in the German Navy—A mixed methods study. Mil. Med. 2021, 187. [Google Scholar] [CrossRef]
- Hellfritz, M.; Waschkau, A.; Steinhäuser, J. Quality indicators of telemedical care offshore—A scoping review. BMC Health Serv. Res. 2021, 21, 1290. [Google Scholar] [CrossRef]
- Traulsen, P.; Steinhäuser, J.; Waschkau, A. Quality indicators for video consultations in primary care—A scoping review. Das Gesundheitswesen 2022. (In German) [Google Scholar] [CrossRef]


{kind=link}
| TA | Gender | Age (Min–Max) | Age (Average) |
|---|---|---|---|
| Video liaison consultations (N = 17) | ♀ 75% ♂ 25% | 5–81 | 51 |
| Teledermatological Consultations (N = 24) | ♀ 62% ♂ 38% | 5–90 | 42 |
| Digital vital sensors (N = 158) | ♀ 56% ♂ 44% | 81–101 | 87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waschkau, A.; Traulsen, P.; Steinhäuser, J. Evaluation of Synchronous and Asynchronous Telemedical Applications in Primary Care in Rural Regions of Northern Germany—Results and Lessons Learned from a Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 14860. https://doi.org/10.3390/ijerph192214860
Waschkau A, Traulsen P, Steinhäuser J. Evaluation of Synchronous and Asynchronous Telemedical Applications in Primary Care in Rural Regions of Northern Germany—Results and Lessons Learned from a Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(22):14860. https://doi.org/10.3390/ijerph192214860
Chicago/Turabian StyleWaschkau, Alexander, Pia Traulsen, and Jost Steinhäuser. 2022. "Evaluation of Synchronous and Asynchronous Telemedical Applications in Primary Care in Rural Regions of Northern Germany—Results and Lessons Learned from a Pilot Study" International Journal of Environmental Research and Public Health 19, no. 22: 14860. https://doi.org/10.3390/ijerph192214860
APA StyleWaschkau, A., Traulsen, P., & Steinhäuser, J. (2022). Evaluation of Synchronous and Asynchronous Telemedical Applications in Primary Care in Rural Regions of Northern Germany—Results and Lessons Learned from a Pilot Study. International Journal of Environmental Research and Public Health, 19(22), 14860. https://doi.org/10.3390/ijerph192214860