
The Associations between 24-Hour Movement Behaviours and Quality of Life in Preschoolers: A Compositional Analysis of Cross-Sectional Data from 2018–2021

 , ,
, , 
Abstract
:
1. Introduction
- (1)
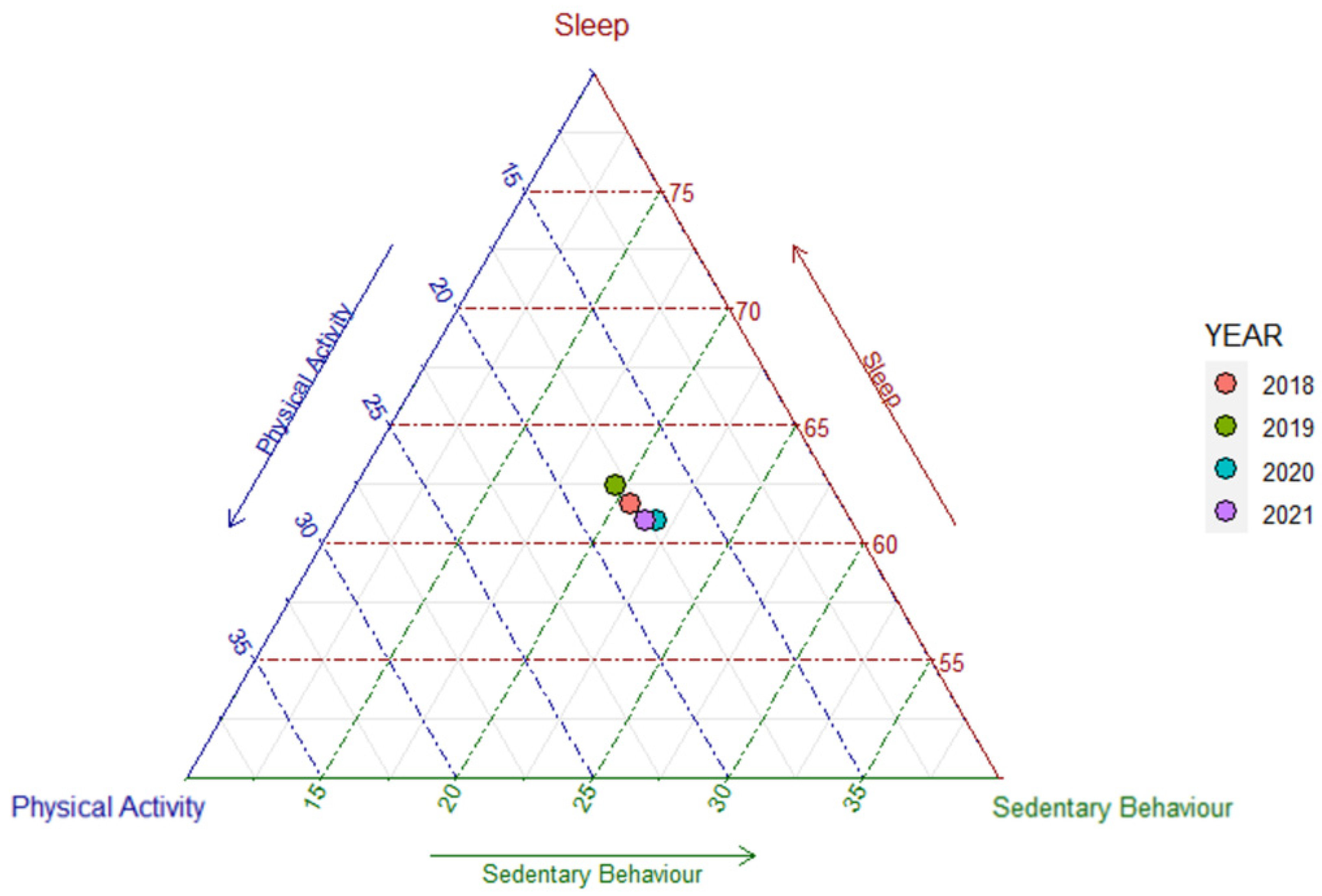
- To investigate the changes in 24-h behaviours (PA, SB, and SL) of preschoolers from 2018–2021 using CoDA;
- (2)
- To examine the trends of association between 24-h behaviours and QoL of preschoolers from 2018–2021 based on linear regression models;
- (3)
- To predict changes in QoL by re-allocating time between PA, SB, and SL behaviours using an isotemporal substitution analysis model with PA, SB, and SL behaviours from data collected in 2021.
2. Materials and Methods
2.1. Design and Participants
2.2. Measurements
2.2.1. Assessment of the PA, SL and SB
Surveillance of Digital Media in Early Childhood Questionnaire (SMALLQ®)
Development and Front-Loaded Validity of the SMALLQ®
Established Face and Content Validity of the SMALLQ®
Internal Consistency (Reliability) of the SMALLQ®
Classification of Activities into PA, SB, and SL
2.2.2. Assessment of the Quality of Life
2.2.3. Treatment of Data
2.2.4. Covariates
2.3. Statistical Analysis
2.3.1. Application of Compositional Data Analysis (CoDA)
2.3.2. Analysis Process
3. Results
3.1. Descriptive Statistics
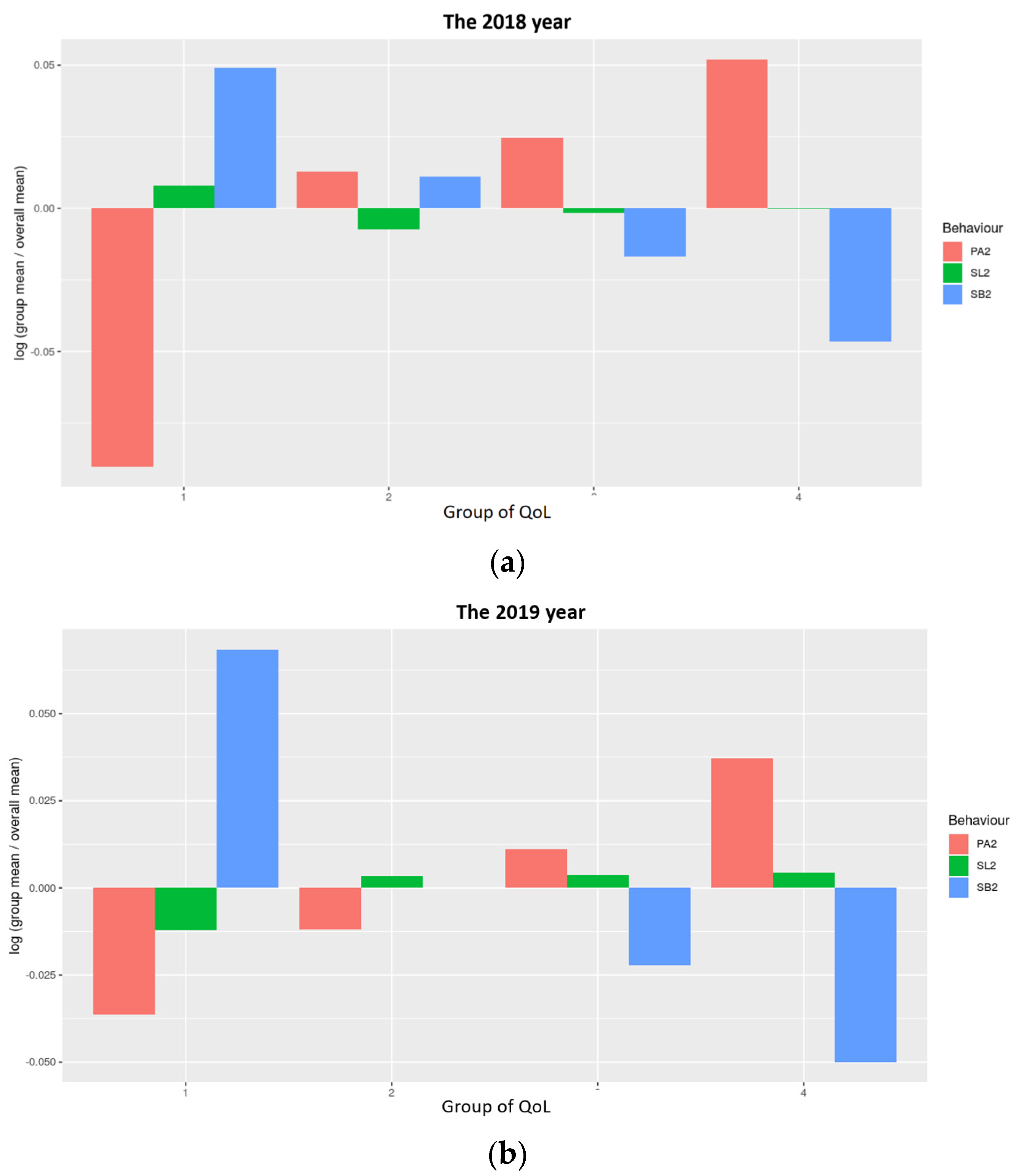
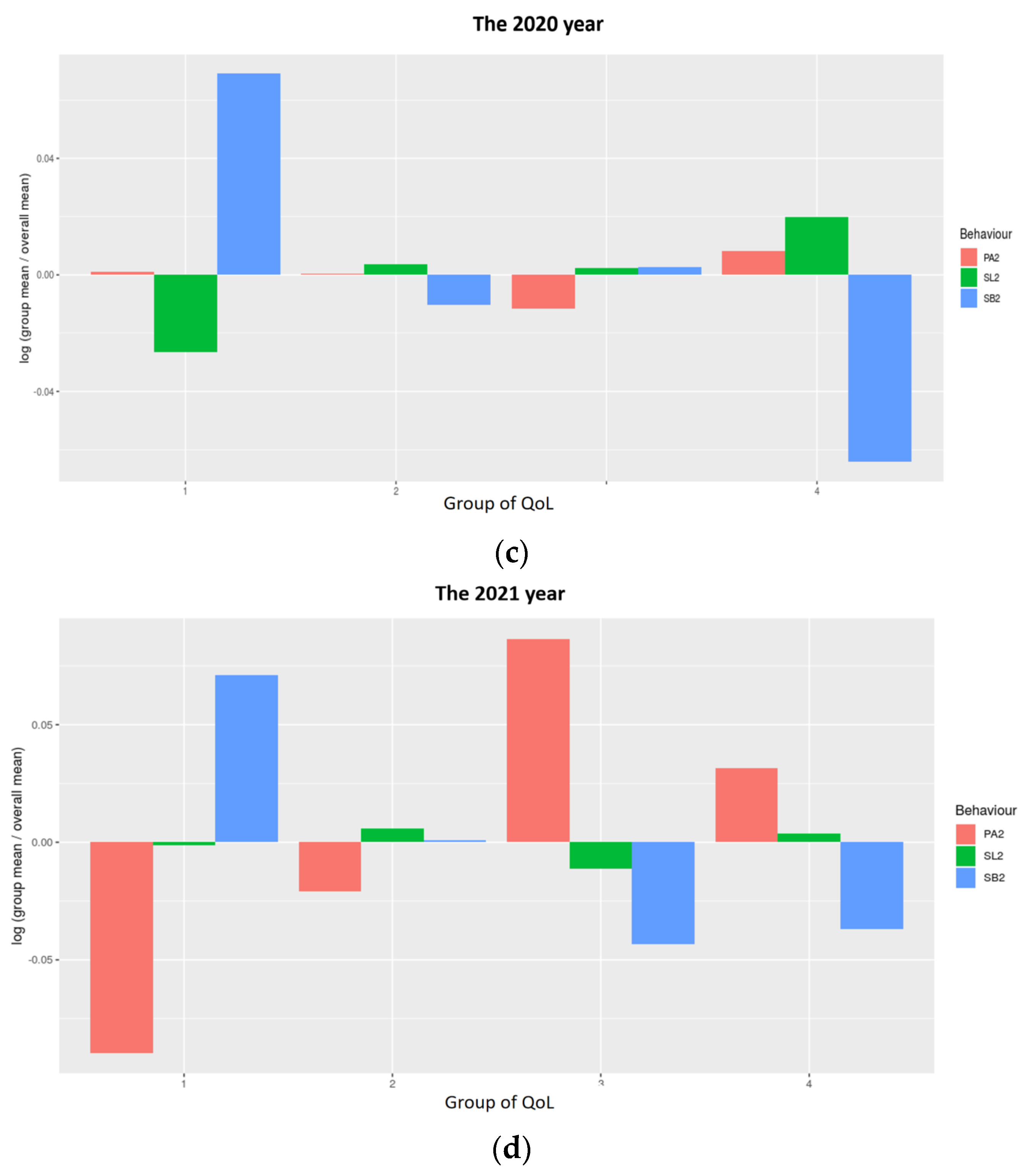
3.2. Composition of a 24-h Day in PA, SB, and SL by Different QoL Quantiles
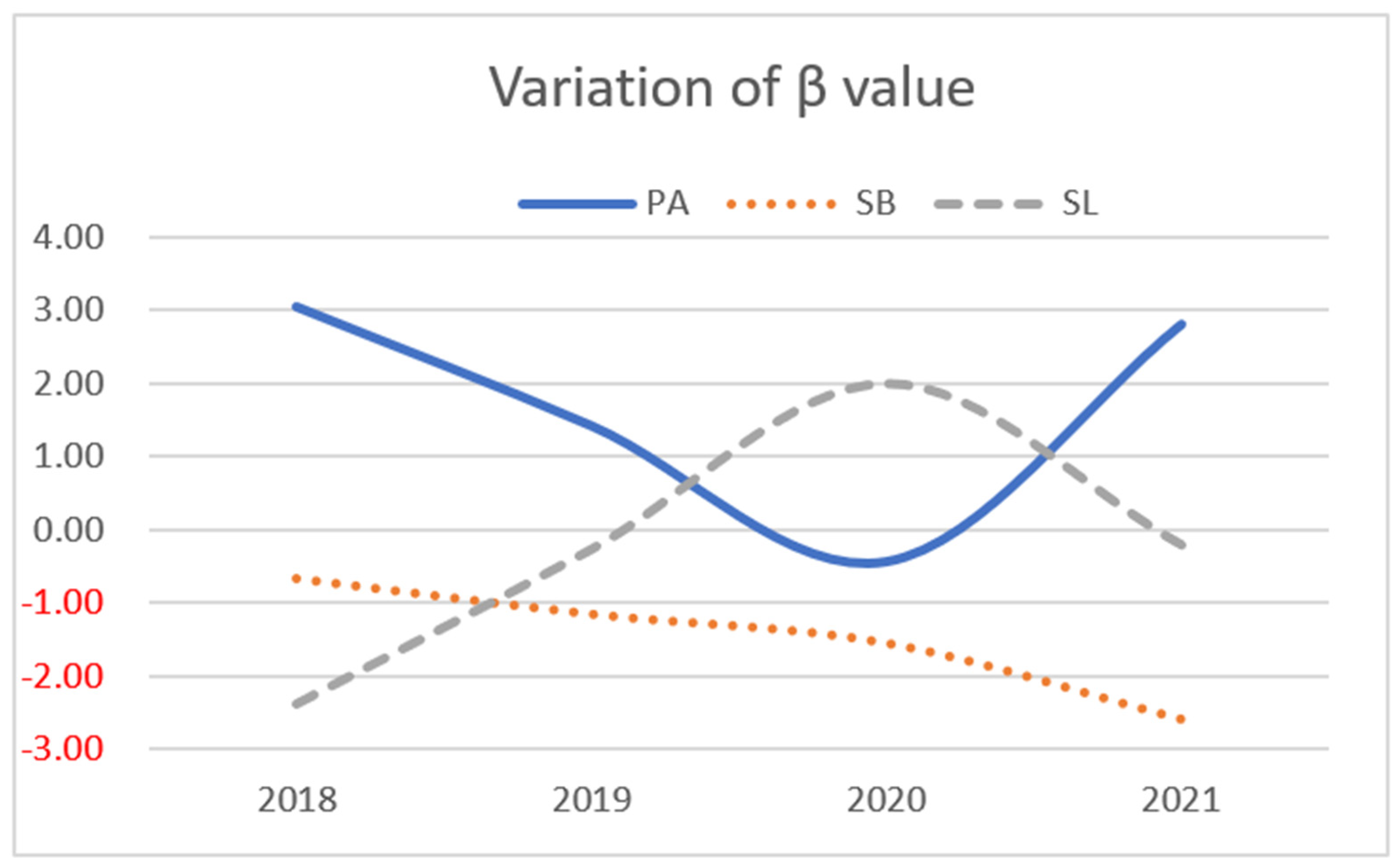
3.3. Compositional Linear Regression Models: Associations between 24-h Behaviors and QoL
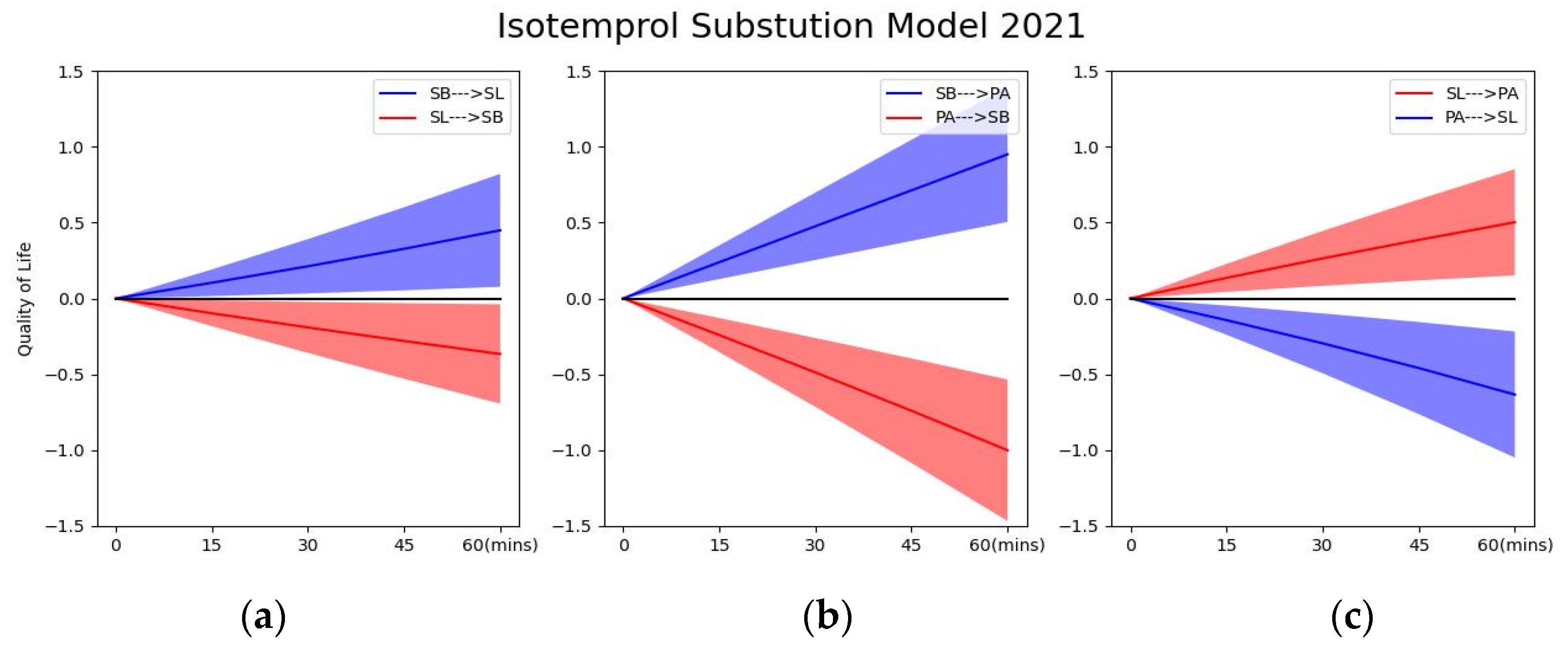
3.4. Isotemporal Substitution Analysis: Effect of Time Re-Allocation
4. Discussion
4.1. Trends in 24-h Movement Behaviors of Preschoolers over 2018–2021
4.2. PA, SB and SL in Relation to QoL and Impact of the COVID-19 Epidemic
4.3. Effect of Time Re-Allocation in PA, SB and SL on QoL
4.4. Strengths and Limitations
4.5. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haraldstad, K.; Wahl, A.; Andenaes, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A Systematic Review of Quality of Life Research in Medicine and Health Sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.; Dixit, S. Health-Related Quality of Life and Health Management. J. Health Manag. 2010, 12, 153–172. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Measuring Healthy Days: Population Assessment of Health-Related Quality of Life; Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2001. [Google Scholar]
- Hennessy, C.H.; Moriarty, D.G.; Zack, M.M.; Scherr, P.A.; Brackbill, R. Measuring Health-Related Quality of Life for Public Health Surveillance. Public Health Rep. 1994, 109, 665. [Google Scholar] [PubMed]
- Hays, R.D.; Reeve, B.B. Measurement and Modeling of Health-Related Quality of Life. Int. Encycl. Public Health 2008, 4, 241–252. [Google Scholar]
- Eiser, C.; Morse, R. The Measurement of Quality of Life in Children: Past and Future Perspectives. J. Dev. Behav. Pediatr. 2001, 22, 248–256. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-001512-8.
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2019; ISBN 978-92-4-155053-6. [Google Scholar]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Altenburg, T.M.; et al. Sedentary Behavior Research Network (SBRN)–Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Regional Office for the Eastern Mediterranean–2022. East. Mediterr. Health J. 2022, 28, 319–391. [Google Scholar]
- 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Available online: https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf (accessed on 1 November 2022).
- Wong, C.K.H.; Wong, R.S.; Cheung, J.P.Y.; Tung, K.T.S.; Yam, J.C.S.; Rich, M.; Fu, K.-W.; Cheung, P.W.H.; Luo, N.; Au, C.H.; et al. Impact of Sleep Duration, Physical Activity, and Screen Time on Health-Related Quality of Life in Children and Adolescents. Health Qual. Life Outcomes 2021, 19, 145. [Google Scholar] [CrossRef]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Gorber, S.C.; et al. Systematic Review of Sedentary Behaviour and Health Indicators in School-Aged Children and Youth: An Update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef] [Green Version]
- Leung, M.M.; Agaronov, A.; Grytsenko, K.; Yeh, M.-C. Intervening to Reduce Sedentary Behaviors and Childhood Obesity among School-Age Youth: A Systematic Review of Randomized Trials. J. Obes. 2011, 2012, e685430. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.Y.; Han, L.H.; Zhang, J.H.; Luo, S.; Hu, J.W.; Sun, K. The Influence of Physical Activity, Sedentary Behavior on Health-Related Quality of Life among the General Population of Children and Adolescents: A Systematic Review. PLoS ONE 2017, 12, e0187668. [Google Scholar] [CrossRef] [Green Version]
- Paruthi, S.; Brooks, L.J.; D’Ambrosio, C.; Hall, W.A.; Kotagal, S.; Lloyd, R.M.; Malow, B.A.; Maski, K.; Nichols, C.; Quan, S.F.; et al. Consensus Statement of the American Academy of Sleep Medicine on the Recommended Amount of Sleep for Healthy Children: Methodology and Discussion. J. Clin. Sleep Med. 2016, 12, 1549–1561. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.A.; Zendarski, N.; Lange, K.; Quach, J.; Molloy, C.; Clifford, S.A.; Mulraney, M. Sleep Problems, Internalizing and Externalizing Symptoms, and Domains of Health-Related Quality of Life: Bidirectional Associations from Early Childhood to Early Adolescence. Sleep 2021, 44, zsaa139. [Google Scholar] [CrossRef] [PubMed]
- Stefelova, N.; Dygryn, J.; Hron, K.; Gaba, A.; Rubin, L.; Palarea-Albaladejo, J. Robust Compositional Analysis of Physical Activity and Sedentary Behaviour Data. Int. J. Environ. Res. Public Health 2018, 15, 2248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prentice-Dunn, H.; Prentice-Dunn, S. Physical Activity, Sedentary Behavior, and Childhood Obesity: A Review of Cross-Sectional Studies. Psychol. Health Med. 2012, 17, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.-P.; Carson, V.; Gray, C.E.; Tremblay, M.S. Importance of All Movement Behaviors in a 24 Hour Period for Overall Health. Int. J. Environ. Res. Public Health 2014, 11, 12575–12581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumuid, D.; Pedišić, Ž.; Palarea-Albaladejo, J.; Martín-Fernández, J.A.; Hron, K.; Olds, T. Compositional Data Analysis in Time-Use Epidemiology: What, Why, How. IJERPH 2020, 17, 2220. [Google Scholar] [CrossRef] [Green Version]
- Chastin, S.F.M.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined Effects of Time Spent in Physical Activity, Sedentary Behaviors and Sleep on Obesity and Cardio-Metabolic Health Markers: A Novel Compositional Data Analysis Approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Tremblay, M.S.; Chaput, J.-P.; Chastin, S.F.M. Associations between Sleep Duration, Sedentary Time, Physical Activity, and Health Indicators among Canadian Children and Youth Using Compositional Analyses. Appl. Physiol. Nutr. Metab. 2016, 41, S294–S302. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Tremblay, M.S.; Chastin, S.F.M. Cross-Sectional Associations between Sleep Duration, Sedentary Time, Physical Activity, and Adiposity Indicators among Canadian Preschool-Aged Children Using Compositional Analyses. BMC Public Health 2017, 17, 848. [Google Scholar] [CrossRef] [Green Version]
- Atkin, A.J.; Dainty, J.R.; Dumuid, D.; Kontostoli, E.; Shepstone, L.; Tyler, R.; Noonan, R.; Richardson, C.; Fairclough, S.J. Adolescent Time Use and Mental Health: A Cross-Sectional, Compositional Analysis in the Millennium Cohort Study. BMJ Open 2021, 11, e047189. [Google Scholar] [CrossRef] [PubMed]
- Bianchim, M.S.; McNarry, M.A.; Holland, A.; Cox, N.S.; Dreger, J.; Barker, A.R.; Williams, C.A.; Denford, S.; Mackintosh, K.A. A Compositional Analysis of Physical Activity, Sedentary Time, and Sleep and Associated Health Outcomes in Children and Adults with Cystic Fibrosis. Int. J. Environ. Res. Public Health 2022, 19, 5155. [Google Scholar] [CrossRef] [PubMed]
- Domingues, S.F.; Diniz da Silva, C.; Faria, F.R.; de Sá Souza, H.; Dos Santos Amorim, P.R. Sleep, Sedentary Behavior, and Physical Activity in Brazilian Adolescents: Achievement Recommendations and BMI Associations through Compositional Data Analysis. PLoS ONE 2022, 17, e0266926. [Google Scholar] [CrossRef] [PubMed]
- Kuzik, N.; Naylor, P.-J.; Spence, J.C.; Carson, V. Movement Behaviours and Physical, Cognitive, and Social-Emotional Development in Preschool-Aged Children: Cross-Sectional Associations Using Compositional Analyses. PLoS ONE 2020, 15, e0237945. [Google Scholar] [CrossRef]
- Giurgiu, M.; Ebner-Priemer, U.W.; Dumuid, D. Compositional Insights on the Association between Physical Activity and Sedentary Behavior on Momentary Mood in Daily Life. Psychol. Sport Exerc. 2022, 58, 102102. [Google Scholar] [CrossRef]
- Anchor Operator Scheme. Available online: https://www.ecda.gov.sg/Parents/Pages/AOP.aspx (accessed on 6 September 2022).
- Boynton, P.M.; Greenhalgh, T. Selecting, Designing, and Developing Your Questionnaire. BMJ 2004, 328, 1312–1315. [Google Scholar] [CrossRef] [Green Version]
- Artino, A.R.; La Rochelle, J.S.; Dezee, K.J.; Gehlbach, H. Developing Questionnaires for Educational Research: AMEE Guide No. 87. Med. Teach. 2014, 36, 463–474. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, T.M.; Hingle, M.; Chuang, R.-J.; Gorely, T.; Hinkley, T.; Jago, R.; Lanigan, J.; Pearson, N.; Thompson, D.A. Conceptual Understanding of Screen Media Parenting: Report of a Working Group. Child. Obes. 2013, 9, S110. [Google Scholar] [CrossRef] [Green Version]
- Lance, C.E.; Butts, M.M.; Michels, L.C. The Sources of Four Commonly Reported Cutoff Criteria: What Did They Really Say? Organ. Res. Methods 2006, 9, 202–220. [Google Scholar] [CrossRef]
- Paruthi, S.; Brooks, L.J.; D’Ambrosio, C.; Hall, W.A.; Kotagal, S.; Lloyd, R.M.; Malow, B.A.; Maski, K.; Nichols, C.; Quan, S.F.; et al. Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2016, 12, 785–786. [Google Scholar] [CrossRef]
- Reinfjell, T.; Diseth, T.H.; Veenstra, M.; Vikan, A. Measuring Health-Related Quality of Life in Young Adolescents: Reliability and Validity in the Norwegian Version of the Pediatric Quality of Life Inventory 4.0 (PedsQL) Generic Core Scales. Health Qual. Life Outcomes 2006, 4, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PedsQL TM (Pediatric Quality of Life Inventory TM). Available online: https://www.pedsql.org/pedsql2.html (accessed on 23 June 2022).
- Cheema, J.R. A Review of Missing Data Handling Methods in Education Research. Rev. Educ. Res. 2014, 84, 487–508. [Google Scholar] [CrossRef]
- Aitchison, J. The Statistical Analysis of Compositional Data; Springer: Dordrecht, The Netherlands, 1986; ISBN 978-94-009-4109-0. [Google Scholar]
- Alenazi, A. A Review of Compositional Data Analysis and Recent Advances. Commun. Stat.-Theory Methods 2021, 1–33. [Google Scholar] [CrossRef]
- Aitchison, J. Compositional data analysis: Where are we and where should we be heading? Math. Geology 2015, 37, 829–850. [Google Scholar] [CrossRef] [Green Version]
- Using the R Package “Compositions”.Pdf. Available online: https://cran.r-project.org/web/packages/compositions/compositions.pdf (accessed on 1 November 2022).
- Chastin, S.; Palarea-Albaladejo, J. Supplementary material s2: Concise guide to compositional data analysis for physical activity, sedentary behavior and sleep research. PLoS ONE 2015, 10, e0139984. [Google Scholar]
- Stephanie Beta Weight: Definition, Uses. Available online: https://www.statisticshowto.com/beta-weight/ (accessed on 10 August 2022).
- Luszczki, E.; Bartosiewicz, A.; Pezdan-Sliz, I.; Kuchciak, M.; Jagielski, P.; Oleksy, L.; Stolarczyk, A.; Deren, K. Children’s Eating Habits, Physical Activity, Sleep, and Media Usage before and during COVID-19 Pandemic in Poland. Nutrients 2021, 13, 2447. [Google Scholar] [CrossRef]
- Dunton, G.F.; Do, B.; Wang, S.D. Early Effects of the COVID-19 Pandemic on Physical Activity and Sedentary Behavior in Children Living in the US. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef]
- Clarke, J.; Kipping, R.; Chambers, S.; Willis, K.; Taylor, H.; Brophy, R.; Hannam, K.; Simpson, S.A.; Langford, R. Impact of COVID-19 Restrictions on Preschool Children’s Eating, Activity and Sleep Behaviours: A Qualitative Study. BMJ Open 2021, 11, e051497. [Google Scholar] [CrossRef]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 Virus Outbreak on Movement and Play Behaviours of Canadian Children and Youth: A National Survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef]
- Lim, M.T.C.; Ramamurthy, M.B.; Aishworiya, R.; Rajgor, D.D.; Tran, A.P.; Hiriyur, P.; Kunaseelan, S.; Jabri, M.; Goh, D.Y.T. School Closure during the Coronavirus Disease 2019 (COVID-19) Pandemic—Impact on Children’s Sleep. Sleep Med. 2021, 78, 108–114. [Google Scholar] [CrossRef]
- Carson, V.; Lee, E.-Y.; Hewitt, L.; Jennings, C.; Hunter, S.; Kuzik, N.; Stearns, J.A.; Unrau, S.P.; Poitras, V.J.; Gray, C.; et al. Systematic Review of the Relationships between Physical Activity and Health Indicators in the Early Years (0–4 Years). BMC Public Health 2017, 17, 854. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Hunter, S.; Kuzik, N.; Wiebe, S.A.; Spence, J.C.; Friedman, A.; Tremblay, M.S.; Slater, L.; Hinkley, T. Systematic Review of Physical Activity and Cognitive Development in Early Childhood. J. Sci. Med. Sport 2016, 19, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Effects of Physical Activity on Motor Skills and Cognitive Development in Early Childhood: A Systematic Review. Available online: https://www.hindawi.com/journals/bmri/2017/2760716/ (accessed on 4 July 2022).
- Spreafico, F.; Barretta, F.; Murelli, M.; Chisari, M.; Gattuso, G.; Terenziani, M.; Ferrari, A.; Veneroni, L.; Meazza, C.; Massimino, M. Positive Impact of Organized Physical Exercise on Quality of Life and Fatigue in Children and Adolescents with Cancer. Front. Pediatr. 2021, 9, 627876. [Google Scholar] [CrossRef]
- Khodashenas, E.; Badiee, Z.; Sohrabi, M.; Ghassemi, A.; Hosseinzade, V. The Effect of an Aerobic Exercise Program on the Quality of Life in Children with Cancer. Turk. J. Pediatr. 2017, 59, 678–683. [Google Scholar] [CrossRef]
- Thorsteinsdottir, H.; Diseth, T.H.; Lie, A.; Tangeraas, T.; Matthews, I.; Asberg, A.; Bjerre, A. Small Effort, High Impact: Focus on Physical Activity Improves Oxygen Uptake (VO2peak), Quality of Life, and Mental Health after Pediatric Renal Transplantation. Pediatr. Transplant. 2018, 22, e13242. [Google Scholar] [CrossRef] [Green Version]
- Shoup, J.A.; Gattshall, M.; Dandamudi, P.; Estabrooks, P. Physical Activity, Quality of Life, and Weight Status in Overweight Children. Qual. Life Res. 2008, 17, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Adibelli, D.; Suemen, A. The Effect of the Coronavirus (COVID-19) Pandemic on Health-Related Quality of Life in Children. Child. Youth Serv. Rev. 2020, 119, 105595. [Google Scholar] [CrossRef]
- Li, X.; Vanderloo, L.M.; Maguire, J.L.; Keown-Stoneman, C.D.G.; Aglipay, M.; Anderson, L.N.; Cost, K.T.; Charach, A.; Vanderhout, S.M.; Birken, C.S. Public Health Preventive Measures and Child Health Behaviours during COVID-19: A Cohort Study. Can. J. Public Health-Rev. Can. Sante Publ. 2021, 112, 831–842. [Google Scholar] [CrossRef]
- Williams, K.E.; Berthelsen, D.; Walker, S.; Nicholson, J.M. A Developmental Cascade Model of Behavioral Sleep Problems and Emotional and Attentional Self-Regulation Across Early Childhood. Behav. Sleep Med. 2017, 15, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Matricciani, L.; Paquet, C.; Galland, B.; Short, M.; Olds, T. Children’s Sleep and Health: A Meta-Review. Sleep Med. Rev. 2019, 46, 136–150. [Google Scholar] [CrossRef]
- Kurth, S.; Achermann, P.; Rusterholz, T.; LeBourgeois, M.K. Development of Brain EEG Connectivity across Early Childhood: Does Sleep Play a Role? Brain Sci. 2013, 3, 1445–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandner, M.A.; Drummond, S.P.A. Who Are the Long Sleepers? Towards an Understanding of the Mortality Relationship. Sleep Med. Rev. 2007, 11, 341–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knutson, K.L.; Turek, F.W. The U-Shaped Association Between Sleep and Health: The 2 Peaks Do Not Mean the Same Thing. Sleep 2006, 29, 878–879. [Google Scholar] [CrossRef] [PubMed]
- Kripke, D.F.; Garfinkel, L.; Wingard, D.L.; Klauber, M.R.; Marler, M.R. Mortality Associated With Sleep Duration and Insomnia. Arch. Gen. Psychiatry 2002, 59, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Lai, J.-S.; Blackwell, C.K.; Tucker, C.A.; Jensen, S.E.; Cella, D. Measuring PROMIS (R) Physical Activity and Sleep Problems in Early Childhood. J. Pediatr. Psychol. 2022, 47, 534–546. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Chaput, J.-P.; Adamo, K.B.; Aubert, S.; Barnes, J.D.; Choquette, L.; Duggan, M.; Faulkner, G.; Goldfield, G.S.; Gray, C.E.; et al. Canadian 24-Hour Movement Guidelines for the Early Years (0–4 Years): An Integration of Physical Activity, Sedentary Behaviour, and Sleep. BMC Public Health 2017, 17, 874. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef]
- Singapore Integrated 24-Hour Activity Guidelines for Children Under Seven Years Launched. Available online: http://www.kkh.com.sg:80/news/announcements/singapore-integrated-24-hour-activity-guidelines-for-children-under-seven-years-launched (accessed on 4 July 2022).
- Magee, C.A.; Robinson, L.; Keane, C. Sleep Quality Subtypes Predict Health-Related Quality of Life in Children. Sleep Med. 2017, 35, 67–73. [Google Scholar] [CrossRef]
- Saunders, T.J.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T.; Gorber, S.C.; Kho, M.E.; Sampson, M.; et al. Combinations of Physical Activity, Sedentary Behaviour and Sleep: Relationships with Health Indicators in School-Aged Children and Youth. Appl. Physiol. Nutr. Metab. 2016, 41, S283–S293. [Google Scholar] [CrossRef] [Green Version]
- Janurek, J.; Abdel Hadi, S.; Mojzisch, A.; Häusser, J. The Association of the 24 Hour Distribution of Time Spent in Physical Activity, Work, and Sleep with Emotional Exhaustion. IJERPH 2018, 15, 1927. [Google Scholar] [CrossRef] [Green Version]
- De Craemer, M.; Decraene, M.; Willems, I.; Buysse, F.; Van Driessche, E.; Verbestel, V. Objective Measurement of 24-Hour Movement Behaviors in Preschool Children Using Wrist-Worn and Thigh-Worn Accelerometers. Int. J. Environ. Res. Public Health 2021, 18, 9482. [Google Scholar] [CrossRef] [PubMed]
- Kastelic, K.; Sarabon, N.; Burnard, M.D.; Pedisic, Z. Validity and Reliability of the Daily Activity Behaviours Questionnaire (DABQ) for Assessment of Time Spent in Sleep, Sedentary Behaviour, and Physical Activity. Int. J. Environ. Res. Public Health 2022, 19, 5362. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Years | p | |||
|---|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | 2021 | |||
| n | 2677 | 1961 | 2403 | 1004 | ||
| Age (yr) | 3.77 (1.25) | 3.79 (1.27) | 3.9 (1.32) | 3.79 (1.29) | <0.001 | |
| Gender, n (%) | Girl | 1374 (51.33) | 953 (48.60) | 1201 (49.98) | 513 (51.10) | 0.29 |
| Boy | 1303 (48.67) | 1008 (51.40) | 1202 (50.02) | 491 (48.90) | ||
| PA (h) | 3.79 (2.11) | 3.81 (2.21) | 3.68 (2.16) | 3.83 (2.26) | 0.15 | |
| SB (h) | 4.45 (2.71) | 4.20 (2.60) | 4.23 (2.68) | 4.59 (2.60) | <0.001 | |
| SL (h) | 11.15 (1.52) | 11.18 (1.53) | 10.96 (1.50) | 11.17 (1.51) | <0.001 | |
| PedsQL (%) | 76.80 (15.56) | 76.79 (14.89) | 78.40 (14.40) | 77.57 (14.65) | <0.001 | |
| Year | Behaviour | PA | SB | SL |
|---|---|---|---|---|
| 2018 | PA | 0.00 | 0.49 | 0.33 |
| SB | 0.49 | 0.00 | 0.40 | |
| SL | 0.33 | 0.40 | 0.00 | |
| 2019 | PA | 0.00 | 0.43 | 0.38 |
| SB | 0.43 | 0.00 | 0.41 | |
| SL | 0.38 | 0.41 | 0.00 | |
| 2020 | PA | 0.00 | 0.45 | 0.37 |
| SB | 0.45 | 0.00 | 0.40 | |
| SL | 0.37 | 0.40 | 0.00 | |
| 2021 | PA | 0.00 | 0.50 | 0.36 |
| SB | 0.50 | 0.00 | 0.41 | |
| SL | 0.36 | 0.41 | 0.00 | |
| 2018–2021 | PA | 0.00 | 0.49 | 0.36 |
| SB | 0.49 | 0.00 | 0.41 | |
| SL | 0.36 | 0.41 | 0.00 |
| QoL of Years | Overall Composition | PA | SB | SL | ||||
|---|---|---|---|---|---|---|---|---|
| R2 | p | βilr | p | βilr | p | βilr | p | |
| 2018 | 0.07 | <0.001 *** | 3.06 | <0.001 *** | 0.67 | 0.25 | −2.39 | <0.001 *** |
| 2019 | 0.04 | <0.001 *** | 1.43 | 0.03 * | −1.16 | 0.09 | −0.27 | 0.73 |
| 2020 | 0.03 | <0.001 *** | −0.43 | 0.43 | −1.56 | 0.008 ** | 2.00 | 0.004 ** |
| 2021 | 0.03 | <0.001 *** | 2.82 | <0.001 *** | −2.61 | 0.002 ** | −0.21 | 0.84 |
| Reallocated Time | Delta of QoL (BS:79.1) | |||
|---|---|---|---|---|
| From PA | From SB | From SL | ||
| 15 min | to PA | 0.24 (0.13,0.35) * | 0.14 (0.04,0.23) * | |
| to SB | −0.24 (−0.35, −0.13) * | −0.10 (−0.18, −0.01) * | ||
| to SL | −0.14 (−0.24, −0.05) * | 0.10 (0.02, 0.19) * | ||
| 30 min | to PA | 0.48 (0.26, 0.70) * | 0.26 (0.08, 0.44) * | |
| to SB | −0.49 (−0.71, −0.26) * | 0.19 (−0.36, −0.03) * | ||
| to SL | −0.30 (−0.49, −0.10) * | 0.21 (0.03, 0.39) | ||
| 45 min | to PA | 0.71 (0.38, 1.05) * | 0.39 (0.12, 0.65) * | |
| to SB | −0.74 (−1.08, −0.40) * | −0.28 (−0.53, −0.03) * | ||
| to SL | −0.46 (−0.76, −0.16) * | 0.33 (0.05,0.60) * | ||
| 60 min | to PA | 0.95 (0.50,1.19) * | 0.50 (0.15, 0.85) * | |
| to SB | −1.00 (−1.47, −0.53) * | −0.37 (−0.70, −0.04) * | ||
| to SL | −0.63 (−1.05, −0.22) * | 0.45 (0.08,0.82) * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.; Chua, T.; Shen, Z.; Tay, L.Y.; Wang, X.; Chia, M. The Associations between 24-Hour Movement Behaviours and Quality of Life in Preschoolers: A Compositional Analysis of Cross-Sectional Data from 2018–2021. Int. J. Environ. Res. Public Health 2022, 19, 14969. https://doi.org/10.3390/ijerph192214969
Chen M, Chua T, Shen Z, Tay LY, Wang X, Chia M. The Associations between 24-Hour Movement Behaviours and Quality of Life in Preschoolers: A Compositional Analysis of Cross-Sectional Data from 2018–2021. International Journal of Environmental Research and Public Health. 2022; 19(22):14969. https://doi.org/10.3390/ijerph192214969
Chicago/Turabian StyleChen, Meiyuan, Terence Chua, Zhi Shen, Lee Yong Tay, Xiaozan Wang, and Michael Chia. 2022. "The Associations between 24-Hour Movement Behaviours and Quality of Life in Preschoolers: A Compositional Analysis of Cross-Sectional Data from 2018–2021" International Journal of Environmental Research and Public Health 19, no. 22: 14969. https://doi.org/10.3390/ijerph192214969
APA StyleChen, M., Chua, T., Shen, Z., Tay, L. Y., Wang, X., & Chia, M. (2022). The Associations between 24-Hour Movement Behaviours and Quality of Life in Preschoolers: A Compositional Analysis of Cross-Sectional Data from 2018–2021. International Journal of Environmental Research and Public Health, 19(22), 14969. https://doi.org/10.3390/ijerph192214969