

The Use of Pb Isotope Ratios to Determine Environmental Sources of High Blood Pb Concentrations in Children: A Feasibility Study in Georgia

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Sample Collection, Transport, and Storage
2.3. Sample Preparation
2.4. Total Pb Concentration Determination
2.5. Pb Isotope Ratio Analysis
3. Results and Discussion
3.1. Interlaboratory Comparison
3.2. Pb Concentrations
3.3. Pb Isotope Ratios
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rees, N.; Fuller, R. The Toxic Truth: Children’s Exposure to Lead Pollution Undermines a Generation of Future Potential; UNICEF: New York, NY, USA, 2020. [Google Scholar]
- World Health Organization. Childhood Lead Poisoning; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Moya, J.; Bearer, C.F.; Etzel, R.A. Children’s Behavior and Physiology and How It Affects Exposure to Environmental Contaminants. Pediatrics 2004, 113, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, G.W. Neurologic concepts of lead poisoning in children. Pediatr. Ann. 1992, 21, 384–388. [Google Scholar] [CrossRef]
- Pervin, R.; Hossain, M.A.; Debnath, D.; Bhuiyan, M.A. Lead Toxicity: An Overview of Its Pathophysiology and Intervention Strategies. In Metal Toxicology Handbook; CRC Press: Boca Raton, FL, USA, 2020; pp. 353–372. [Google Scholar]
- U.S. Centers for Disease Control and Prevention. Childhood Lead Poisoning Prevention. Available online: https://www.cdc.gov/nceh/lead/data/blood-lead-reference-value.htm (accessed on 29 March 2022).
- UK Health Security Agency. Evaluation of Whether to Lower the Public Health Intervention Concentration for Lead Exposure in Children: A Report by the Lead Intervention Concentration Working Group; UK Health Security Agency: London, UK, 2021.
- European Food Safety Authority. Scientific Opinion on Lead in Food. EFSA J. 2010, 8, 1570.
- Lanphear, B.P.; Hornung, R.; Khoury, J.; Yolton, K.; Baghurst, P.; Bellinger, D.C.; Canfield, R.L.; Dietrich, K.N.; Bornschein, R.; Greene, T.; et al. Low-level environmental lead exposure and children’s intellectual function: An international pooled analysis. Env. Health Perspect 2005, 113, 894–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazzi, Z.; Gabelaia, L.; Shengelia, L.; Sturua, L.; Ericson, B.; Giorgobiani, A.; Nadiradze, A.; Gamkrelidze, A. Lessons Learned Through the Journey of a Medical Toxicologist While Characterizing Lead Hazards in the Republic of Georgia. J. Med. Toxicol. 2020, 16, 3–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Statistics Office of Georgia. Georgia Multiple Indicator Cluster Survey 2018, Survey Findings Report; National Statistics Office of Georgia: Tbilisi, Georgia, 2019. [Google Scholar]
- The State Program for Disease Early Diagnosis and Screening. Available online: https://matsne.gov.ge/ka/document/view/4569980?publication=0 (accessed on 29 March 2022).
- Smith, K.E.; Shafer, M.M.; Weiss, D.; Anderson, H.A.; Gorski, P.R. High-Precision (MC-ICPMS) Isotope Ratio Analysis Reveals Contrasting Sources of Elevated Blood Lead Levels of an Adult with Retained Bullet Fragments, and of His Child, in Milwaukee, Wisconsin. Biol. Trace Elem. Res. 2017, 177, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Cheema, A.I.; Liu, G.; Yousaf, B.; Abbas, Q.; Zhou, H. A comprehensive review of biogeochemical distribution and fractionation of lead isotopes for source tracing in distinct interactive environmental compartments. Sci. Total Environ. 2020, 719, 135658. [Google Scholar] [CrossRef]
- Gulson, B. Stable lead isotopes in environmental health with emphasis on human investigations. Sci. Total Environ. 2008, 400, 75–92. [Google Scholar] [CrossRef]
- Komarek, M.; Ettler, V.; Chrastny, V.; Mihaljevic, M. Lead isotopes in environmental sciences: A review. Environ. Int. 2008, 34, 562–577. [Google Scholar] [CrossRef]
- Glorennec, P.; Peyr, C.; Poupon, J.; Oulhote, Y.; Le Bot, B. Identifying sources of lead exposure for children, with lead concentrations and isotope ratios. J. Occup. Environ. Hyg. 2010, 7, 253–260. [Google Scholar] [CrossRef]
- Oulhote, Y.; Le Bot, B.; Poupon, J.; Lucas, J.P.; Mandin, C.; Etchevers, A.; Zmirou-Navier, D.; Glorennec, P. Identification of sources of lead exposure in French children by lead isotope analysis: A cross-sectional study. Environ. Health 2011, 10, 75. [Google Scholar] [CrossRef] [PubMed]
- Becker, F.; Marcantonio, F.; Datta, S.; Wichterich, C.; Cizmas, L.; Surber, J.; Kennedy, K.; Bowles, E. Tracking the source of contaminant lead in children’s blood. Environ. Res. 2022, 212, 113307. [Google Scholar] [CrossRef] [PubMed]
- Gulson, B.; Anderson, P.; Taylor, A. Surface dust wipes are the best predictors of blood leads in young children with elevated blood lead levels. Environ. Res. 2013, 126, 171–178. [Google Scholar] [CrossRef]
- Takagi, M.; Tanaka, A.; Seyama, H.; Uematsu, A.; Kaji, M.; Yoshinaga, J. Source Identification Analysis of Lead in the Blood of Japanese Children by Stable Isotope Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7784. [Google Scholar] [CrossRef]
- Takagi, M.; Yoshinaga, J.; Tanaka, A.; Seyama, H. Isotope ratio analysis of lead in blood and environmental samples by multi-collector inductively coupled plasma mass spectrometry. Anal. Sci. 2011, 27, 29–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsyth, J.E.; Weaver, K.L.; Maher, K.; Islam, M.S.; Raqib, R.; Rahman, M.; Fendorf, S.; Luby, S.P. Sources of Blood Lead Exposure in Rural Bangladesh. Environ. Sci. Technol. 2019, 53, 11429–11436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fillion, M.; Blais, J.M.; Yumvihoze, E.; Nakajima, M.; Workman, P.; Osborne, G.; Chan, H.M. Identification of environmental sources of lead exposure in Nunavut (Canada) using stable isotope analyses. Environ. Int. 2014, 71, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Gulson, B.; Kamenov, G.D.; Manton, W.; Rabinowitz, M. Concerns about Quadrupole ICP-MS Lead Isotopic Data and Interpretations in the Environment and Health Fields. Int. J. Environ. Res. Public Health 2018, 15, 723. [Google Scholar] [CrossRef] [Green Version]
- Health and Social Affairs of Georgia. Order No 38/N of 24th of February 2003 of Minister of Labor, on Norms of Environmental Quality; Health and Social Affairs of Georgia: Tbilisi, Georgia, 2003. [Google Scholar]
- Ericson, B.; Gabelaia, L.; Keith, J.; Kashibadze, T.; Beraia, N.; Sturua, L.; Kazzi, Z. Elevated Levels of Lead (Pb) Identified in Georgian Spices. Ann. Glob. Health 2020, 86, 124. [Google Scholar] [CrossRef]
- Hore, P.; Alex-Oni, K.; Sedlar, S.; Nagin, D. A Spoonful of Lead: A 10-Year Look at Spices as a Potential Source of Lead Exposure. J. Public Health Manag. Pract. 2019, 25 (Suppl. S1), S63–S70. [Google Scholar] [CrossRef]
- International Pollutants Elimination Network. Global Lead Paint Elimination Report; International Pollutants Elimination Network: Stockholm, Sweden, 2020. [Google Scholar]
- Middleton, D.; Watts, M.; Hamilton, E.; Coe, J.; Fletcher, T.; Crabbe, H.; Close, R.; Leonardi, G.; Polya, D. Surface wipe and bulk sampling of household dust: Arsenic exposure in Cornwall, UK. Environ. Sci. Process. Impacts 2018, 20, 505–512. [Google Scholar] [CrossRef] [PubMed]
- BS Publications. BS EN 71-3: 2019 Safety of toys—Part 3: Migration of Certain Elements; BS Publications: Hyderabad, India, 2019. [Google Scholar]
- Usman, A.; Ander, E.L.; Bailey, E.H.; Nelms, S.; Pashley, V.; Young, S.D.; Chenery, S.R. Optimisation of a current generation ICP-QMS and benchmarking against MC-ICP-MS spectrometry for the determination of lead isotope ratios in environmental samples. J. Anal. At. Spectrom. 2018, 33, 2184–2194. [Google Scholar] [CrossRef]
- Nelms, S.M.; Quétel, C.R.; Prohaska, T.; Vogl, J.; Taylor, P.D.P. Evaluation of detector dead time calculation models for ICP-MS. J. Anal. At. Spectrom. 2001, 16, 333–338. [Google Scholar] [CrossRef]
- Ruadze, E.; Leonardi, G.S.; Saei, A.; Khonelidze, I.; Sturua, L.; Getia, V.; Crabbe, H.; Marczylo, T.; Lauriola, P.; Gamkrelidze, A. Reduction in Blood Lead Concentration in Children across the Republic of Georgia following Interventions to Address Widespread Exceedance of Reference Value in 2019. Int. J. Environ. Res. Public Health 2021, 18, 11903. [Google Scholar] [CrossRef] [PubMed]
- Woolf, A.D.; Woolf, N.T. Childhood lead poisoning in 2 families associated with spices used in food preparation. Pediatrics 2005, 116, e314–e318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erasmus, S.W.; van Hasselt, L.; Ebbinge, L.M.; van Ruth, S.M. Real or fake yellow in the vibrant colour craze: Rapid detection of lead chromate in turmeric. Food Control 2021, 121, 107714. [Google Scholar] [CrossRef]
- Reimann, C.; Flem, B.; Fabian, K.; Birke, M.; Ladenberger, A.; Négrel, P.; Demetriades, A.; Hoogewerff, J. Lead and lead isotopes in agricultural soils of Europe—The continental perspective. Appl. Geochem. 2012, 27, 532–542. [Google Scholar] [CrossRef]
- Toth, G.; Hermann, T.; Da Silva, M.R.; Montanarella, L. Heavy metals in agricultural soils of the European Union with implications for food safety. Environ. Int. 2016, 88, 299–309. [Google Scholar] [CrossRef]
- Ander, E.L.; Johnson, C.C.; Cave, M.R.; Palumbo-Roe, B.; Nathanail, C.P.; Lark, R.M. Methodology for the determination of normal background concentrations of contaminants in English soil. Sci. Total Environ. 2013, 454–455, 604–618. [Google Scholar] [CrossRef] [Green Version]
- Department for Environment Food and Rural Affairs (DEFRA). Technical Guidance Sheet on Normal Levels of Contaminants in English Soils: Lead. Technical Guidance Sheet No. TGS02; Soils R&D Project SP1008; Department for Environment Food and Rural Affairs (DEFRA): London, UK, 2012.
- US EPA. Lead in Soil. Available online: https://www.epa.gov/sites/default/files/2020-10/documents/lead-in-soil-aug2020.pdf (accessed on 29 March 2022).
- Brereton, N.; Baxter, M.; Wallis, M.; Wilderspin, M.; Simpson, E. Analyses of Lead Levels in Tea, Report for the UK Food Standards Agency (FS102115); UK Food Standards Agency: London, UK, 2015. [Google Scholar]
- European Commission. Regulation EC No 1881_2006—Setting Maximum Levels for Certain Contaminants in Foodstuffs; European Commission: Brussels, Belgium, 2006.
- Cao, S.; Duan, X.; Zhao, X.; Wang, B.; Ma, J.; Fan, D.; Sun, C.; He, B.; Wei, F.; Jiang, G. Isotopic ratio based source apportionment of children’s blood lead around coking plant area. Environ. Int. 2014, 73, 158–166. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Blood | Flour, Spice and Tea | Paint | Milk |
|---|---|---|---|---|
| Volume/Mass | 1 mL | 0.5 g | <0.25 g | 1.5 mL |
| Laboratory–Instrument | UKHSA–Anton Paar Multiwave Go | Multitest–Berghof Speedwave Two | ||
| Reagents | 1 mL HNO3 | 2 mL HNO3 | 6 mL HNO3 | 0.5 mL HNO3 |
| 1 mL UPW | 2 mL UPW | 3.0 mL UPW | ||
| 1 mL H2O2 | 1 mL H2O2 | |||
| Digestion protocol | Ramp to 180 °C over 10 min, hold for 20 min | Ramp to 175 °C over 15 min, hold for 15 min | Ramp to 180 °C over 10 min, hold for 20 min | |
| Sample | Units | n | Min | Max | Percentile | Geometric Mean | Arithmetic Mean | Median | Reference Value a | >Reference Value (n) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 25th | 75th | ||||||||||
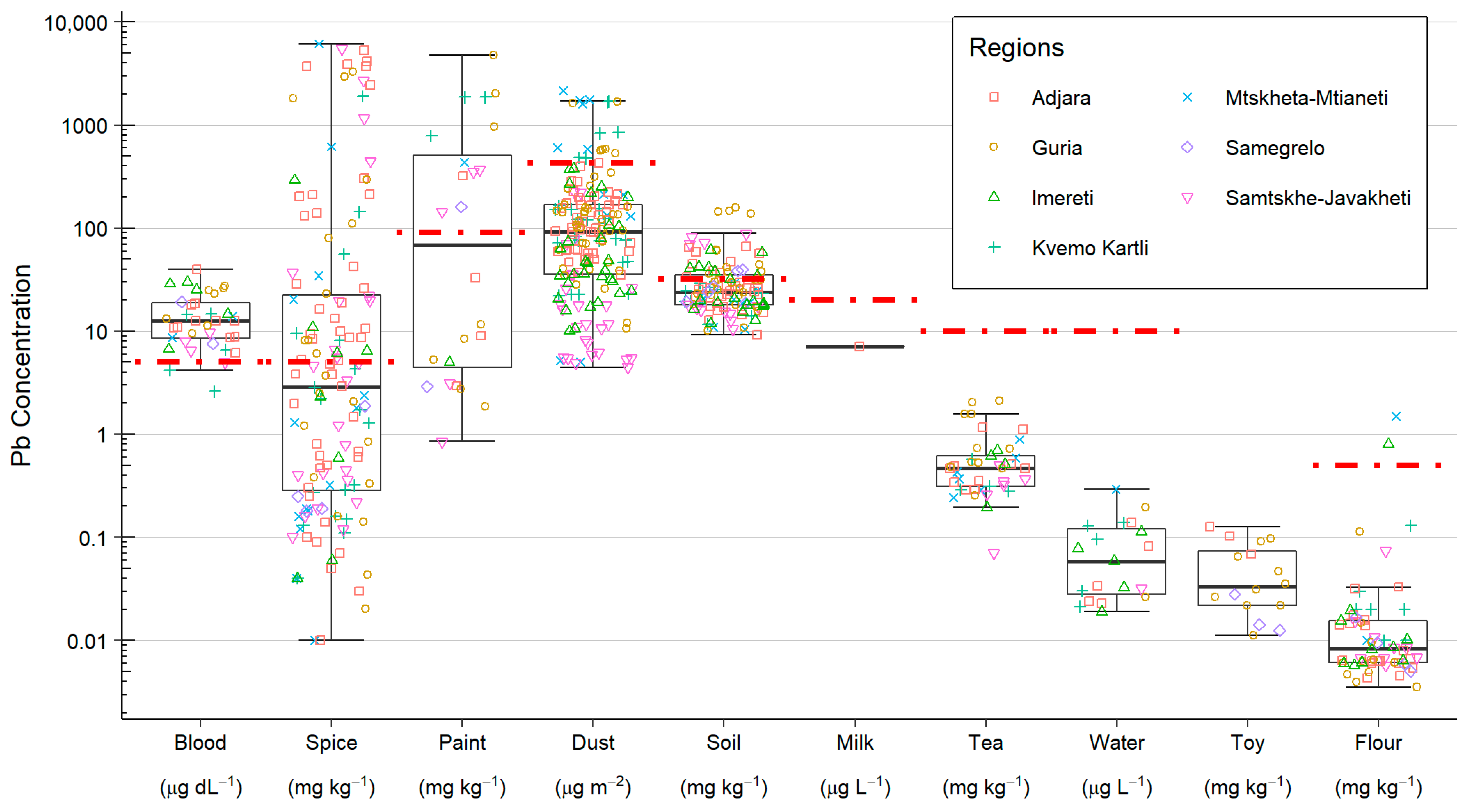
| Blood | µg dL−1 | 36 | 2.6 | 39.9 | 8.5 | 18.7 | 12.2 | 14.5 | 12.6 | 5 | 34 [94%] |
| Paint | mg kg−1 | 22 | 0.8 | 4802 | 4.1 | 699 | 73.0 | 644 | 153 | 90 | 12 [55%] |
| Spice | mg kg−1 | 136 | 0.01 | 6164 | 0.3 | 22.4 | 4.1 | 387 | 2.9 | 5 | 59 [43%] |
| Soil | mg kg−1 | 62 | 10.5 | 158.8 | 17.9 | 35 | 25.8 | 31.7 | 23.4 | 32 | 16 [26%] |
| Dust | µg m−2 | 92 | 34.9 | 2163 | 34.9 | 168 | 79.5 | 198 | 88.6 | 431 | 9 [10%] |
| Tea | mg kg−1 | 31 | 0.07 | 2.1 | 0.3 | 0.6 | 0.4 | 0.5 | 0.4 | 10 | 0 [0%] |
| Flour | mg kg−1 | 62 | <0.01 | 1.5 | 0.01 | 0.02 | 0.01 | 0.05 | 0.01 | 0.5 | 2 [3%] |
| Water | µg L−1 | 48 b | 0.02 | 0.3 | 0.03 | 0.12 | 0.1 | 0.1 | 0.1 | 10 | 0 [0%] |
| Milk | µg L−1 | 16 c | 7.1 | 7.1 | 7.1 | 7.1 | 7.1 | 7.1 | 7.1 | 20 | 0 [0%] |
| Toys | mg kg−1 | 16 | 11.2 | 126 | 21.8 | 74.3 | 37.8 | 49.9 | 33.1 | - | - |
| Spice Type | n | Lead Concentration mg kg−1 | >5 mg kg−1 (n [%]) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median | Percentile | Min | Max | Geometric Mean | Arithmetic Mean | ||||
| 25th | 75th | ||||||||
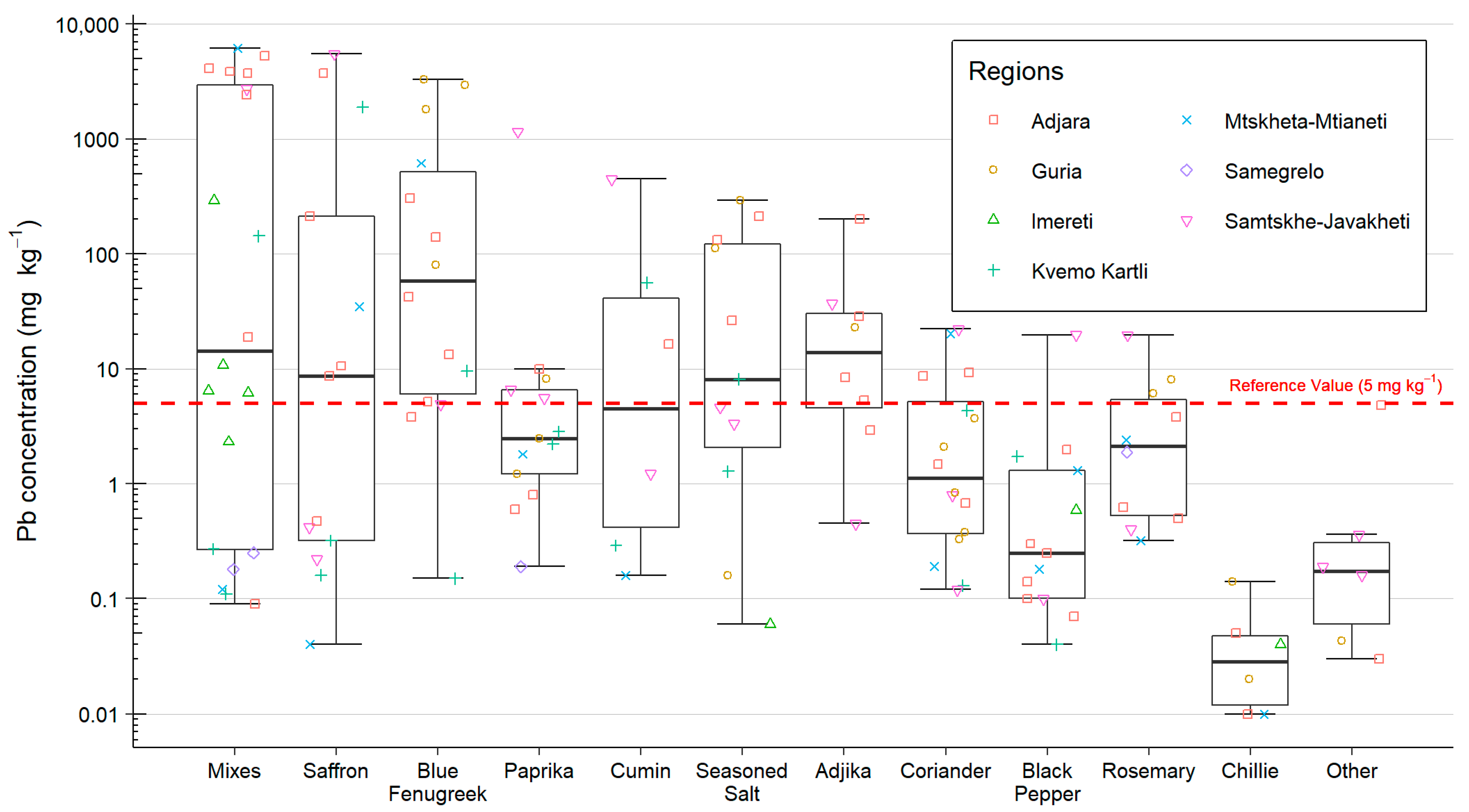
| Spice mixes | 20 | 14.9 | 0.3 | 2971 | 0.09 | 6165 | 28.7 | 1444 | 13 [65%] |
| Saffron/yellow flower | 13 | 8.7 | 0.3 | 211 | 0.04 | 5510 | 8.9 | 879 | 7 [54%] |
| Blue fenugreek | 14 | 61.3 | 6.3 | 540 | 0.15 | 3292 | 55.9 | 664 | 11 [79%] |
| Paprika | 13 | 2.5 | 1.2 | 6.6 | 0.19 | 1160 | 3.5 | 92.5 | 5 [38%] |
| Cumin | 6 | 8.8 | 0.5 | 46.1 | 0.16 | 449 | 5.3 | 87.1 | 3 [50%] |
| Seasoned salt | 11 | 8.1 | 2.3 | 122.1 | 0.06 | 295 | 9.1 | 72.4 | 6 [55%] |
| Adjika | 8 | 15.7 | 4.7 | 30.7 | 0.45 | 202 | 11.4 | 39 | 6 [75%] |
| Coriander | 16 | 1.2 | 0.4 | 5.4 | 0.12 | 22.2 | 1.4 | 4.7 | 4 [25%] |
| Black pepper | 13 | 0.3 | 0.1 | 1.3 | 0.04 | 19.8 | 0.4 | 2.0 | 1 [8%] |
| Rosemary | 10 | 2.1 | 0.5 | 5.5 | 0.32 | 19.6 | 1.9 | 4.4 | 3 [30%] |
| Chillies | 6 | 0.0 | 0.0 | 0.0 | 0.01 | 0.1 | 0.0 | 0.0 | 0 [0%] |
| Other | 6 | 0.2 | 0.1 | 0.3 | 0.03 | 4.8 | 0.2 | 0.9 | 0 [0%] |
| All | 135 | 2.9 | 22.6 | 943 | 0.01 | 6165 | 4.2 | 389 | 59 [44%] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laycock, A.; Chenery, S.; Marchant, E.; Crabbe, H.; Saei, A.; Ruadze, E.; Watts, M.; Leonardi, G.S.; Marczylo, T. The Use of Pb Isotope Ratios to Determine Environmental Sources of High Blood Pb Concentrations in Children: A Feasibility Study in Georgia. Int. J. Environ. Res. Public Health 2022, 19, 15007. https://doi.org/10.3390/ijerph192215007
Laycock A, Chenery S, Marchant E, Crabbe H, Saei A, Ruadze E, Watts M, Leonardi GS, Marczylo T. The Use of Pb Isotope Ratios to Determine Environmental Sources of High Blood Pb Concentrations in Children: A Feasibility Study in Georgia. International Journal of Environmental Research and Public Health. 2022; 19(22):15007. https://doi.org/10.3390/ijerph192215007
Chicago/Turabian StyleLaycock, Adam, Simon Chenery, Elizabeth Marchant, Helen Crabbe, Ayoub Saei, Ekaterine Ruadze, Michael Watts, Giovanni S. Leonardi, and Tim Marczylo. 2022. "The Use of Pb Isotope Ratios to Determine Environmental Sources of High Blood Pb Concentrations in Children: A Feasibility Study in Georgia" International Journal of Environmental Research and Public Health 19, no. 22: 15007. https://doi.org/10.3390/ijerph192215007
APA StyleLaycock, A., Chenery, S., Marchant, E., Crabbe, H., Saei, A., Ruadze, E., Watts, M., Leonardi, G. S., & Marczylo, T. (2022). The Use of Pb Isotope Ratios to Determine Environmental Sources of High Blood Pb Concentrations in Children: A Feasibility Study in Georgia. International Journal of Environmental Research and Public Health, 19(22), 15007. https://doi.org/10.3390/ijerph192215007