


Effects of 12-Week Progressive Sandbag Exercise Training on Glycemic Control and Muscle Strength in Patients with Type 2 Diabetes Mellitus Combined with Possible Sarcopenia

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Patients
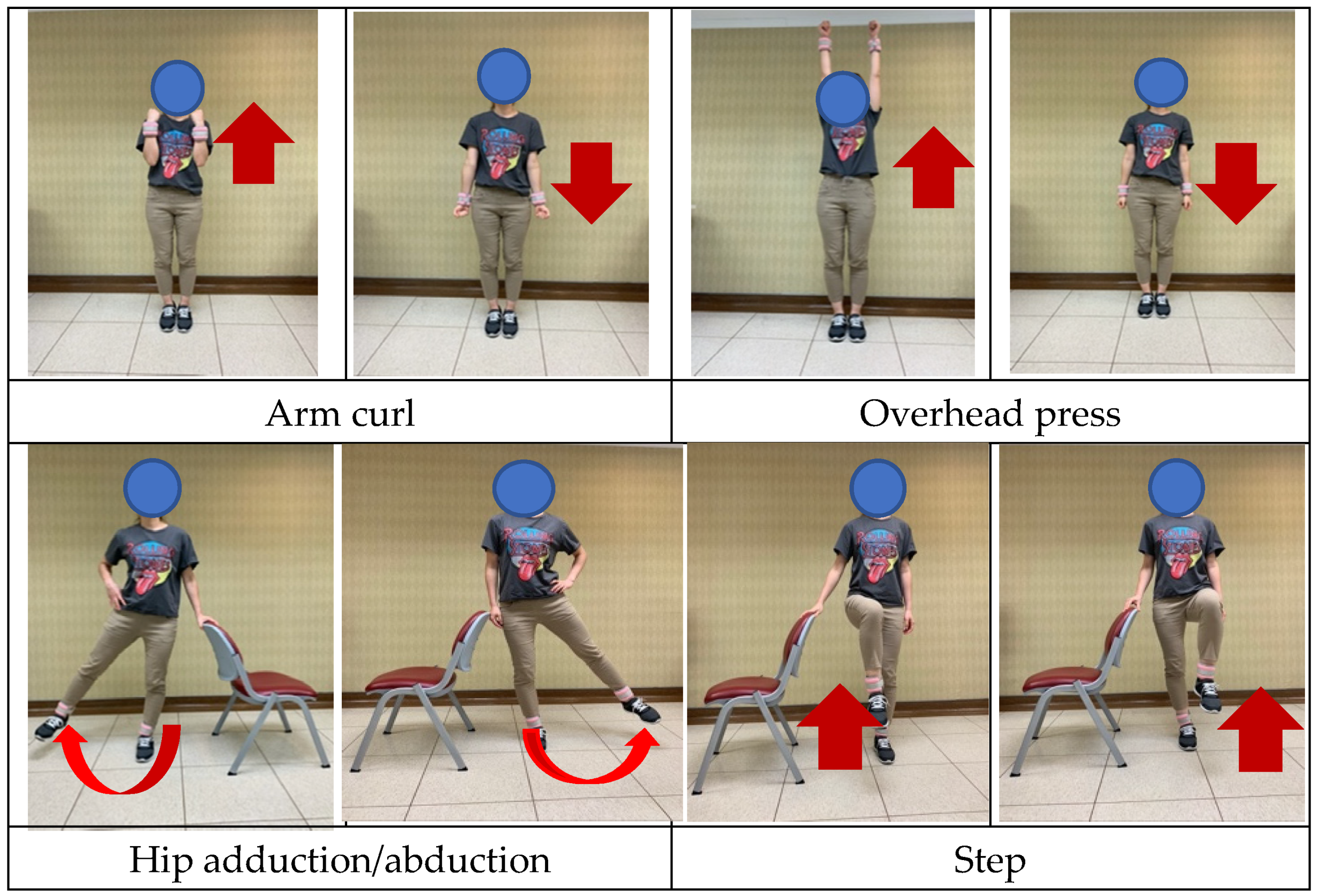
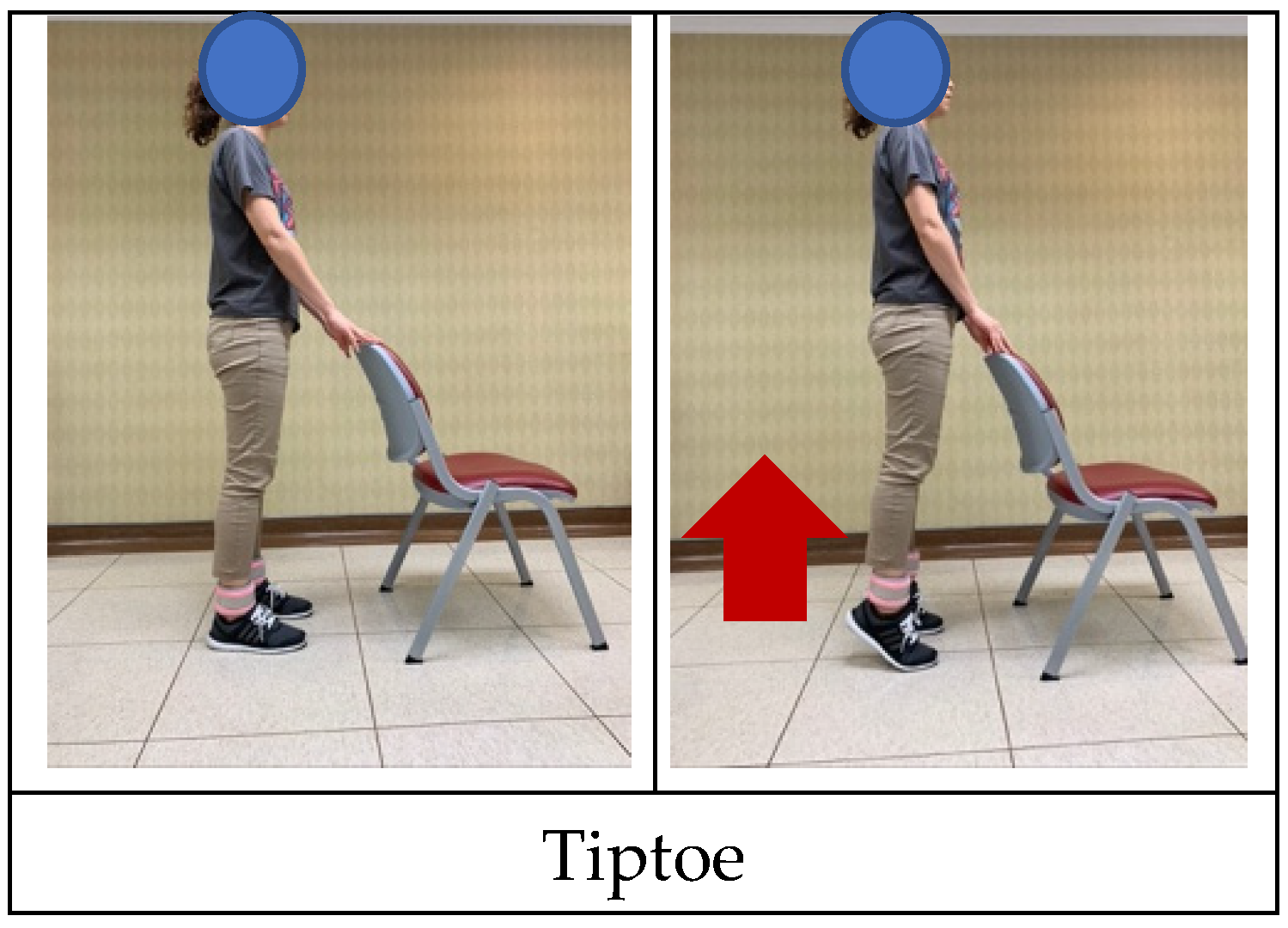
2.3. Intervention
2.3.1. Resistance Training Group
2.3.2. Control Group
2.4. Outcome Measures
2.4.1. Biochemical Analysis
2.4.2. Grip Strength
2.4.3. Five Times Sit-to-Stand Test
2.4.4. Muscle Mass
2.4.5. Calf Circumference
2.4.6. WHOQOL-BREF Taiwan Version
2.5. Statistical Analysis
3. Results
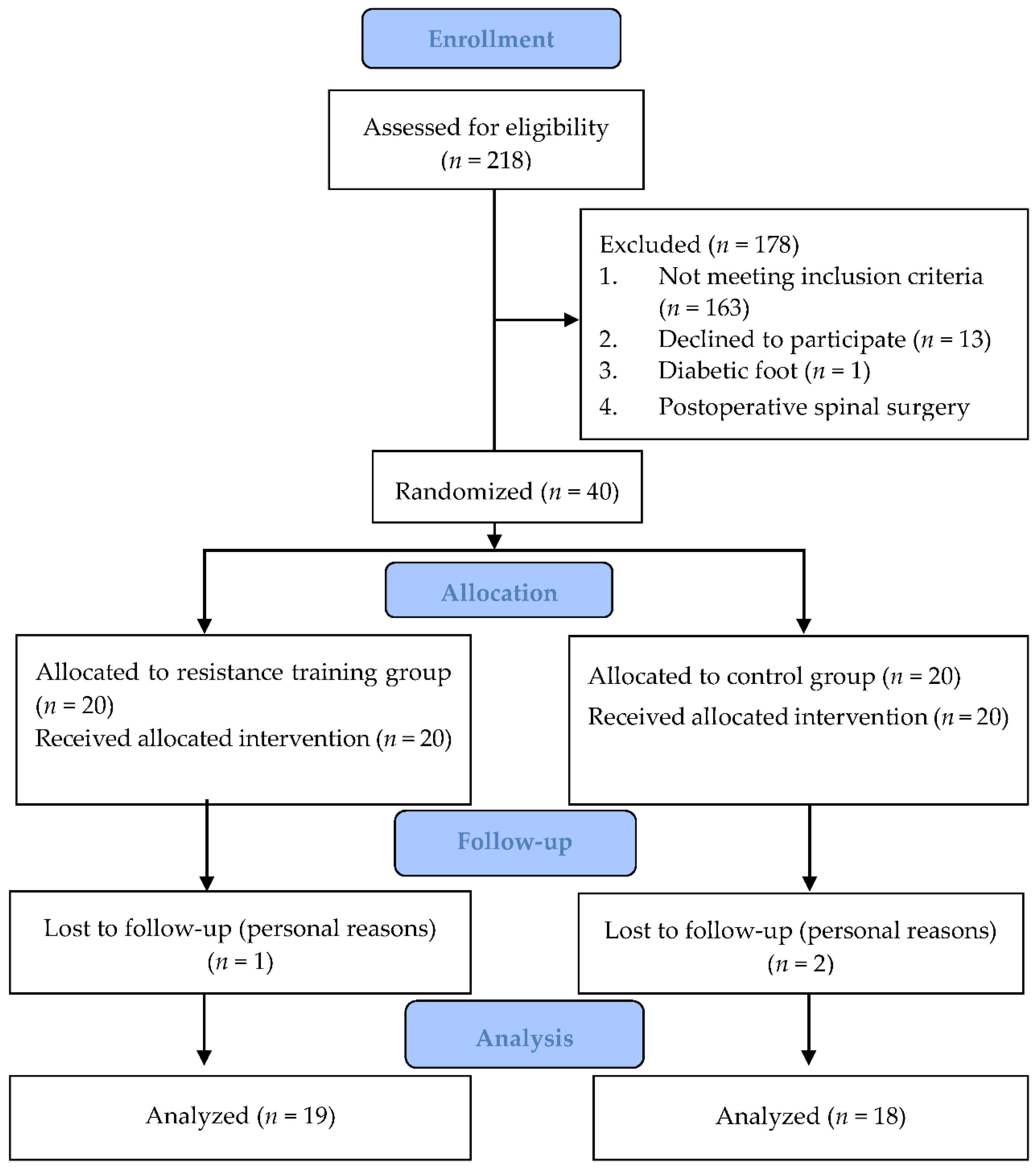
3.1. Flow of Participants
3.2. Effect of Intervention on HbA1c
3.3. Effect of Intervention on the Lipid Profile
3.4. Effect of Intervention on Grip Strength
3.5. Effect of Intervention on the Five Times Sit-to-Stand Test
3.6. Effect of Intervention on ASM and ASMI
3.7. Effect of Intervention on Calf Circumference
3.8. Effect of Intervention on the WHOQOL Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation. Annual Report 2021; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Baron, A.D.; Brechtel, G.; Wallace, P.; Edelman, S.V. Rates and tissue sites of non-insulin- and insulin-mediated glucose uptake in humans. Am. J. Physiol. 1988, 255, E769–E774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umegaki, H. Sarcopenia and frailty in older patients with diabetes mellitus. Geriatr. Gerontol. Int. 2016, 16, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; Kuller, L.H.; Broudeau, R.; Kammerer, C.; De Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A. Accelerated loss of skeletal muscle strength in older adults with type 2 diabetes: The health, aging, and body composition study. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesinovic, J.; Zengin, A.; De Courten, B.; Ebeling, P.R.; Scott, D. Sarcopenia and type 2 diabetes mellitus: A bidirectional relationship. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1057–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B. Exercise and type 2 diabetes: The american college of sports medicine and the american diabetes association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigal, R.J.; Kenny, G.P.; Boulé, N.G.; Wells, G.A.; Prud’homme, D.; Fortier, M.; Reid, R.D.; Tulloch, H.; Coyle, D.; Phillips, P.; et al. Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: A randomized trial. Ann. Intern. Med. 2007, 147, 357–369. [Google Scholar] [CrossRef]
- Boulé, N.G.; Haddad, E.; Kenny, G.P.; Wells, G.A.; Sigal, R.J. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitusa meta-analysis of controlled clinical trials. JAMA 2001, 286, 1218–1227. [Google Scholar] [CrossRef]
- Lee, J.; Kim, D.; Kim, C. Resistance training for glycemic control, muscular strength, and lean body mass in old type 2 diabetic patients: A meta-analysis. Diabetes Ther. 2017, 8, 459–473. [Google Scholar] [CrossRef] [Green Version]
- Takenami, E.; Iwamoto, S.; Shiraishi, N.; Kato, A.; Watanabe, Y.; Yamada, Y.; Yamada, S.; Ishii, N. Effects of low-intensity resistance training on muscular function and glycemic control in older adults with type 2 diabetes. J. Diabetes Investig. 2019, 10, 331–338. [Google Scholar] [CrossRef]
- Myers, V.H.; McVay, M.A.; Brashear, M.M.; Johannsen, N.M.; Swift, D.L.; Kramer, K.; Harris, M.N.; Johnson, W.D.; Earnest, C.P.; Church, T.S. Exercise training and quality of life in individuals with type 2 diabetes: A randomized controlled trial. Diabetes Care 2013, 36, 1884–1890. [Google Scholar] [CrossRef]
- Sun, S.; Lee, H.; Yim, H.W.; Won, H.S.; Ko, Y.H. The impact of sarcopenia on health-related quality of life in elderly people: Korean national health and nutrition examination survey. Korean J. Intern. Med. 2019, 34, 877–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigal, R.J.; Kenny, G.P.; Wasserman, D.H.; Castaneda-Sceppa, C. Physical activity/exercise and type 2 diabetes. Diabetes Care 2004, 27, 2518–2539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaneda, C.; Layne, J.E.; Munoz-Orians, L.; Gordon, P.L.; Walsmith, J.; Foldvari, M.; Roubenoff, R.; Tucker, K.L.; Nelson, M.E. A randomized controlled trial of resistance exercise training to improve glycemic control in older adults with type 2 diabetes. Diabetes Care 2002, 25, 2335–2341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bemben, D.A.; Fetters, N.L.; Bemben, M.G.; Nabavi, N.; Koh, E.T. Musculoskeletal responses to high- and low-intensity resistance training in early postmenopausal women. Med. Sci. Sports Exerc. 2000, 32, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Pourtaghi, F.; Moghadam, Z.E.; Ramezani, M.; Vashani, H.B.; Mohajer, S. Effect of resistance training using thera-band on muscular strength and quality of life among the elderly. Evid. Based Care 2017, 7, 7–16. [Google Scholar]
- Liao, C.-D.; Tsauo, J.-Y.; Huang, S.-W.; Ku, J.-W.; Hsiao, D.-J.; Liou, T.-H. Effects of elastic band exercise on lean mass and physical capacity in older women with sarcopenic obesity: A randomized controlled trial. Sci. Rep. 2018, 8, 2317. [Google Scholar] [CrossRef] [Green Version]
- Higgins, T. Hba1c—An analyte of increasing importance. Clin. Biochem. 2012, 45, 1038–1045. [Google Scholar] [CrossRef]
- Vikberg, S.; Sörlén, N.; Brandén, L.; Johansson, J.; Nordström, A.; Hult, A.; Nordström, P. Effects of resistance training on functional strength and muscle mass in 70-year-old individuals with pre-sarcopenia: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2019, 20, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Picorelli, A.M.A.; Pereira, D.S.; Felício, D.C.; Dos Anjos, D.M.; Pereira, D.A.G.; Dias, R.C.; Assis, M.G.; Pereira, L.S.M. Adherence of older women with strength training and aerobic exercise. Clin. Interv. Aging 2014, 9, 323–331. [Google Scholar] [CrossRef] [Green Version]
- Misra, A.; Alappan, N.K.; Vikram, N.K.; Goel, K.; Gupta, N.; Mittal, K.; Bhatt, S.; Luthra, K. Effect of supervised progressive resistance-exercise training protocol on insulin sensitivity, glycemia, lipids, and body composition in asian indians with type 2 diabetes. Diabetes Care 2008, 31, 1282–1287. [Google Scholar] [CrossRef] [Green Version]
- Kwon, H.R.; Han, K.A.; Ku, Y.H.; Ahn, H.J.; Koo, B.-K.; Kim, H.C.; Min, K.W. The effects of resistance training on muscle and body fat mass and muscle strength in type 2 diabetic women. Korean Diabetes J. 2010, 34, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Holten, M.K.; Zacho, M.; Gaster, M.; Juel, C.; Wojtaszewski, J.F.; Dela, F. Strength training increases insulin-mediated glucose uptake, glut4 content, and insulin signaling in skeletal muscle in patients with type 2 diabetes. Diabetes 2004, 53, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Durstine, J.L.; Grandjean, P.W.; Cox, C.A.; Thompson, P.D. Lipids, lipoproteins, and exercise. J. Cardiopulm. Rehabil. 2002, 22, 385–398. [Google Scholar] [CrossRef] [PubMed]
- Durstine, J.L.; Grandjean, P.W.; Davis, P.G.; Ferguson, M.A.; Alderson, N.L.; DuBose, K.D. Blood lipid and lipoprotein adaptations to exercise. Sports Med. 2001, 31, 1033–1062. [Google Scholar] [CrossRef] [PubMed]
- Nery, C.; Moraes, S.R.A.; Novaes, K.A.; Bezerra, M.A.; Silveira, P.V.C.; Lemos, A. Effectiveness of resistance exercise compared to aerobic exercise without insulin therapy in patients with type 2 diabetes mellitus: A meta-analysis. Braz. J. Phys. Ther. 2017, 21, 400–415. [Google Scholar] [CrossRef]
- Häkkinen, K.; Kallinen, M.; Izquierdo, M.; Jokelainen, K.; Lassila, H.; Mälkiä, E.; Kraemer, W.J.; Newton, R.U.; Alen, M. Changes in agonist-antagonist emg, muscle csa, and force during strength training in middle-aged and older people. J. Appl. Physiol. 1998, 84, 1341–1349. [Google Scholar] [CrossRef]
- Aagaard, P.; Suetta, C.; Caserotti, P.; Magnusson, S.P.; Kjær, M. Role of the nervous system in sarcopenia and muscle atrophy with aging: Strength training as a countermeasure. Scand. J. Med. Sci. Sports 2010, 20, 49–64. [Google Scholar] [CrossRef]
- Bao, W.; Sun, Y.; Zhang, T.; Zou, L.; Wu, X.; Wang, D.; Chen, Z. Exercise programs for muscle mass, muscle strength and physical performance in older adults with sarcopenia: A systematic review and meta-analysis. Aging Dis. 2020, 11, 863–873. [Google Scholar] [CrossRef]
- Taaffe, D.R. Sarcopenia—Exercise as a treatment strategy. Aust. Fam. Physician 2006, 35, 130–134. [Google Scholar]
- Watanabe, Y.; Tanimoto, M.; Ohgane, A.; Sanada, K.; Miyachi, M.; Ishii, N. Increased muscle size and strength from slow-movement, low-intensity resistance exercise and tonic force generation. J. Aging Phys. Act. 2013, 21, 71–84. [Google Scholar] [CrossRef] [Green Version]
- Schoenfeld, B.J. Is there a minimum intensity threshold for resistance training-induced hypertrophic adaptations? Sports Med. 2013, 43, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J.; Latham, N.K. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst. Rev. 2009, 2009, Cd002759. [Google Scholar] [CrossRef] [PubMed]
- Tsekoura, M.; Billis, E.; Tsepis, E.; Dimitriadis, Z.; Matzaroglou, C.; Tyllianakis, M.; Panagiotopoulos, E.; Gliatis, J. The effects of group and home-based exercise programs in elderly with sarcopenia: A randomized controlled trial. J. Clin. Med. 2018, 7, 480. [Google Scholar] [CrossRef] [Green Version]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.-J.; Wu, G.-H.; Yang, Y.-L.; Wu, Y.-H.; Zhang, L.; Wang, M.-H.; Mo, L.-Y.; Xue, G.; Wang, C.-Z.; Weng, X.-F. Nutrition, physical exercise, and the prevalence of sarcopenia in elderly residents in nursing homes in china. Med. Sci. Monit. 2019, 25, 4390–4399. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, M.; Lee, Y.; Kim, B.; Yoon, T.Y.; Won, C.W. Calf circumference as a simple screening marker for diagnosing sarcopenia in older korean adults: The korean frailty and aging cohort study (kfacs). J. Korean Med. Sci. 2018, 33, e151. [Google Scholar] [CrossRef]
- Kawakami, R.; Murakami, H.; Sanada, K.; Tanaka, N.; Sawada, S.S.; Tabata, I.; Higuchi, M.; Miyachi, M. Calf circumference as a surrogate marker of muscle mass for diagnosing sarcopenia in japanese men and women. Geriatr. Gerontol. Int. 2015, 15, 969–976. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Training Group (n = 20) | Control Group (n = 20) | p-Value | |
|---|---|---|---|
| Gender b | |||
| Male/female, n (%) | 5 (25%)/15 (75%) | 2 (10%)/18 (90%) | 0.212 |
| Age (years) a | 67.6 ± 7.7 | 67.3 ± 6.1 | 0.892 |
| Duration of T2DM (years) | 17.5 ± 16.3 | 13.6 ± 7.6 | 0.346 |
| Body height (cm) a | 154.4 ± 16.3 | 156.3 ± 6.0 | 0.349 |
| Body weight (kg) | 58.0 ± 9.0 | 62.4 ± 9.9 | 0.149 |
| Body index (kg/m2) | 24.3 ± 3.4 | 25.5 ± 3.7 | 0.311 |
| HbA1c (%) | 8.1 ± 1.1 | 7.6 ± 0.6 | 0.057 |
| LDL (mg/dL) a | 86.9 ± 36.5 | 77.7 ± 29.7 | 0.388 |
| HDL (mg/dL) a | 54.4 ± 13.6 | 47.5 ± 11.6 | 0.094 |
| Triglycerides (mg/dL) a | 117.4 ± 32.1 | 125.4 ± 61.2 | 0.608 |
| Outcomes | Group | Baseline | Post | Within Group p-Value | Between Groups p-Value | Time * Group p-Value |
|---|---|---|---|---|---|---|
| HbA1c (%) | Training | 8.1 ± 1.1 | 7.7 ± 0.9 | 0.037 * | 0.042 * | 0.004 * |
| Control | 7.6 ± 0.6 | 7.4 ± 0.7 | ||||
| HDL (mg/dL) | Training | 54.4 ± 13.6 | 53.7 ± 11.8 | 0.416 | 0.078 | 0.354 |
| Control | 47.5 ± 11.6 | 48.8 ± 12.6 | ||||
| LDL (mg/dL) | Training | 87.0 ± 36.5 | 76.6 ± 27.0 | 0.272 | 0.370 | 0.072 |
| Control | 77.8 ± 29.7 | 82.7 ± 31.2 | ||||
| TG (mg/dL) | Training | 117.4 ± 32.1 | 125.4 ± 61.2 | 0.669 | 0.595 | 0.172 |
| Control | 100.3 ± 36.2 | 130.9 ± 65.0 | ||||
| Hand grip (kg) | Training | 15.9 ± 5.0 | 19.1 ± 4.9 | 0.010 * | 0.520 | 0.097 |
| Control | 15.1 ± 3.8 | 16.5 ± 5.4 | ||||
| Five times sit-to-stand test (s) | Training | 16.6 ± 3.5 | 13.4 ± 3.2 | 0.061 | 0.499 | 0.001 * |
| Control | 15.9 ± 3.0 | 17.1 ± 4.7 | ||||
| ASM (kg) | Training | 16.7 ± 3.3 | 17.1 ± 3.5 | 0.009 * | 0.795 | 0.001 * |
| Control | 16.9 ± 2.1 | 16.6 ± 2.2 | ||||
| ASMI (kg/m2) | Training | 6.9 ± 0.9 | 7.1 ± 1.0 | 0.009 * | 0.795 | 0.001 * |
| Control | 6.9 ± 0.7 | 6.8 ± 0.1 | ||||
| Calf circumference (cm) | Training | 30.4 ± 2.3 | 31.2 ± 1.9 | 0.009 * | 0.795 | 0.001 * |
| Control | 31.3 ± 2.0 | 30.6 ± 2.8 |
| Domain | Group | Baseline | After 12 Weeks | Within Group p-Value | Between Groups p-Value | Time * Group p-Value |
|---|---|---|---|---|---|---|
| General health | Training | 2.8 ± 0.6 | 3.0 ± 0.6 | 0.953 | 0.703 | 0.304 |
| Control | 2.7 ± 0.6 | 2.7 ± 0.8 | ||||
| Physical domain | Training | 10.6 ± 1.8 | 12.1 ± 1.8 | 0.921 | 0.371 | 0.009 * |
| Control | 11.1 ± 1.7 | 11.1 ± 2.3 | ||||
| Psychology domain | Training | 10.8 ± 1.8 | 11.4 ± 1.8 | 0.509 | 0.957 | 0.354 |
| Control | 10.8 ± 1.8 | 10.4 ± 2.4 | ||||
| Social relationship domain | Training | 11.7 ± 1.4 | 11.9 ± 1.4 | 0.787 | 0.582 | 0.540 |
| Control | 11.4 ± 2.0 | 11.4 ± 2.1 | ||||
| Environmental domain | Training | 14.0 ± 2.0 | 14.5 ± 1.7 | 0.927 | 0.631 | 0.167 |
| Control | 14.3 ± 1.7 | 14.3 ± 1.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, Y.-H.; Tsai, C.-J.; Wang, D.-C.; Chuang, P.-H.; Lin, H.-T. Effects of 12-Week Progressive Sandbag Exercise Training on Glycemic Control and Muscle Strength in Patients with Type 2 Diabetes Mellitus Combined with Possible Sarcopenia. Int. J. Environ. Res. Public Health 2022, 19, 15009. https://doi.org/10.3390/ijerph192215009
Chien Y-H, Tsai C-J, Wang D-C, Chuang P-H, Lin H-T. Effects of 12-Week Progressive Sandbag Exercise Training on Glycemic Control and Muscle Strength in Patients with Type 2 Diabetes Mellitus Combined with Possible Sarcopenia. International Journal of Environmental Research and Public Health. 2022; 19(22):15009. https://doi.org/10.3390/ijerph192215009
Chicago/Turabian StyleChien, Yu-Hsuan, Chia-Jen Tsai, Dean-Chuan Wang, Pin-Hung Chuang, and Hwai-Ting Lin. 2022. "Effects of 12-Week Progressive Sandbag Exercise Training on Glycemic Control and Muscle Strength in Patients with Type 2 Diabetes Mellitus Combined with Possible Sarcopenia" International Journal of Environmental Research and Public Health 19, no. 22: 15009. https://doi.org/10.3390/ijerph192215009
APA StyleChien, Y. -H., Tsai, C. -J., Wang, D. -C., Chuang, P. -H., & Lin, H. -T. (2022). Effects of 12-Week Progressive Sandbag Exercise Training on Glycemic Control and Muscle Strength in Patients with Type 2 Diabetes Mellitus Combined with Possible Sarcopenia. International Journal of Environmental Research and Public Health, 19(22), 15009. https://doi.org/10.3390/ijerph192215009