

Identification of Early Knee Osteoarthritis Based on Knee Joint Trajectory during Stair Climbing

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Radiographic Severity of Osteoarthritis
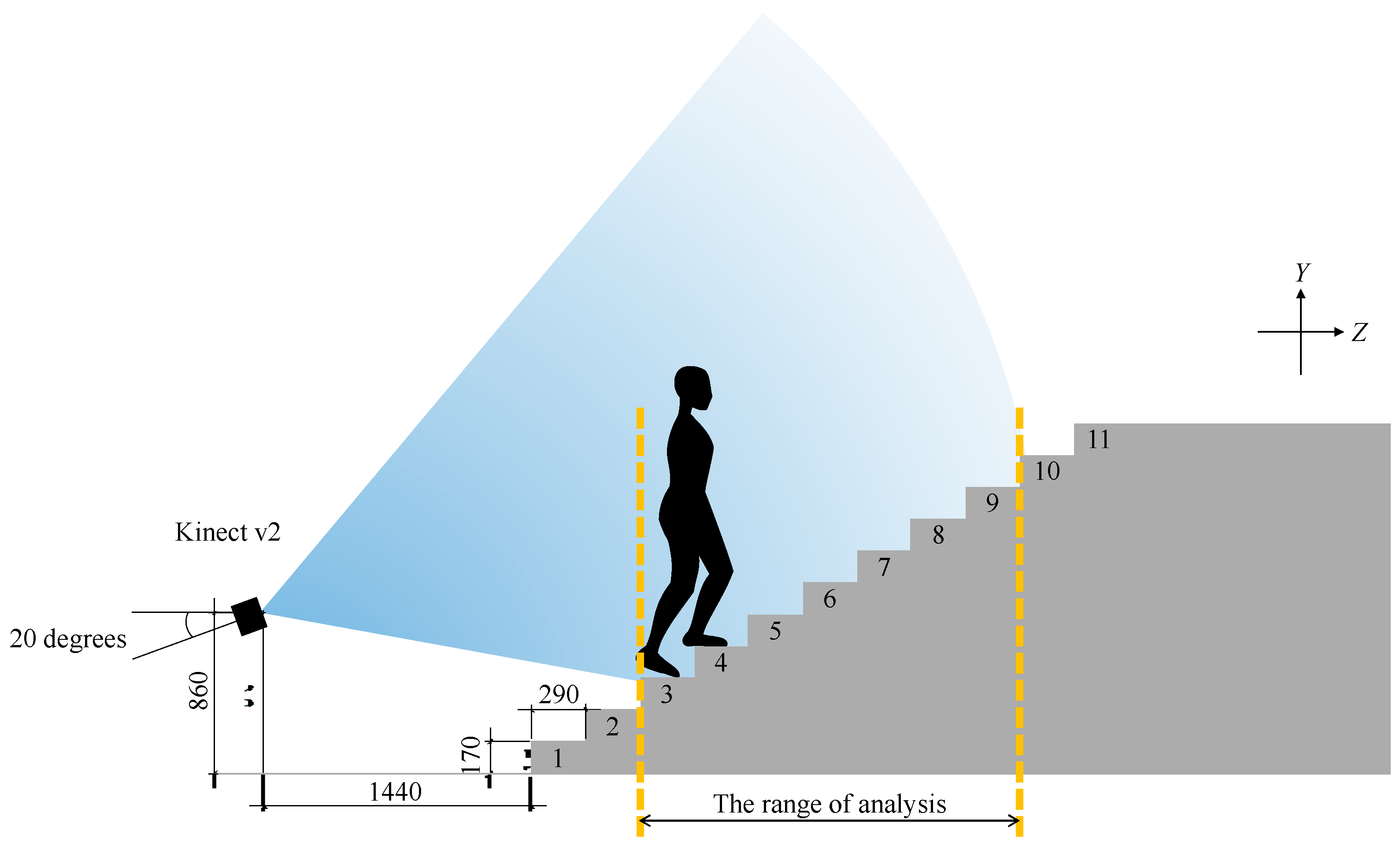
2.3. Instrumentation of Stair Climbing Test
2.4. Procedure for Eleven-Step Stair Climb Test (11-SCT)
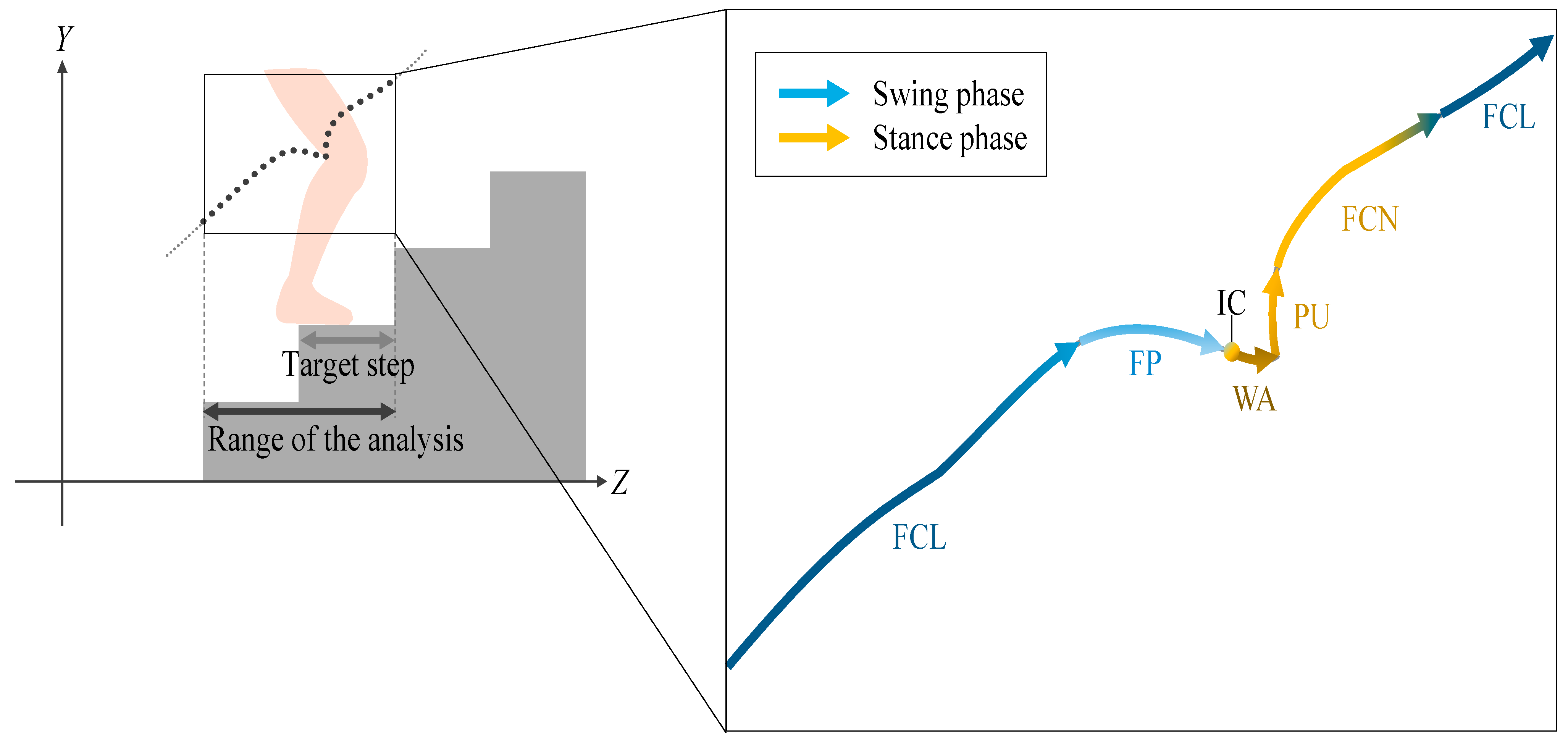
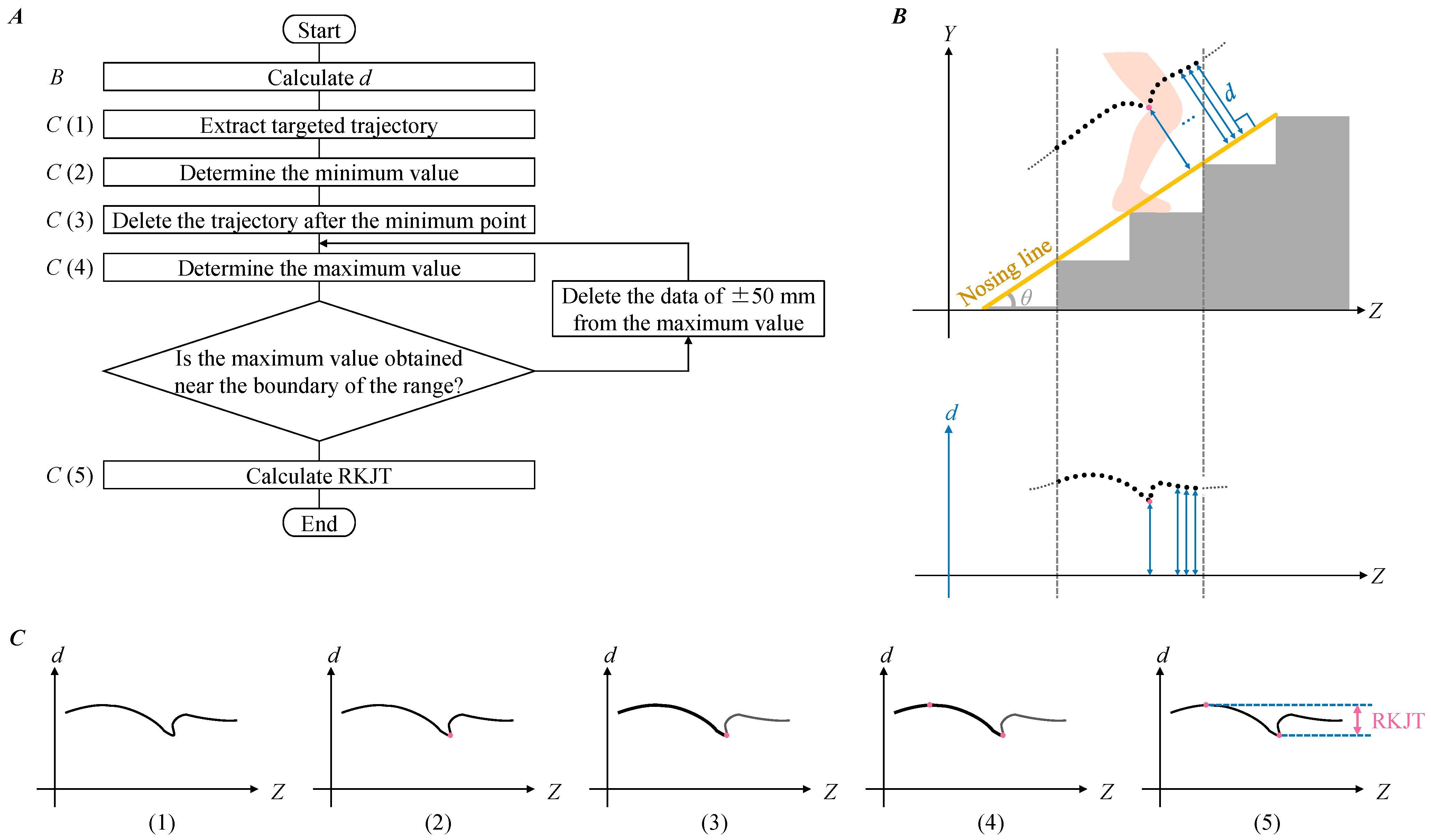
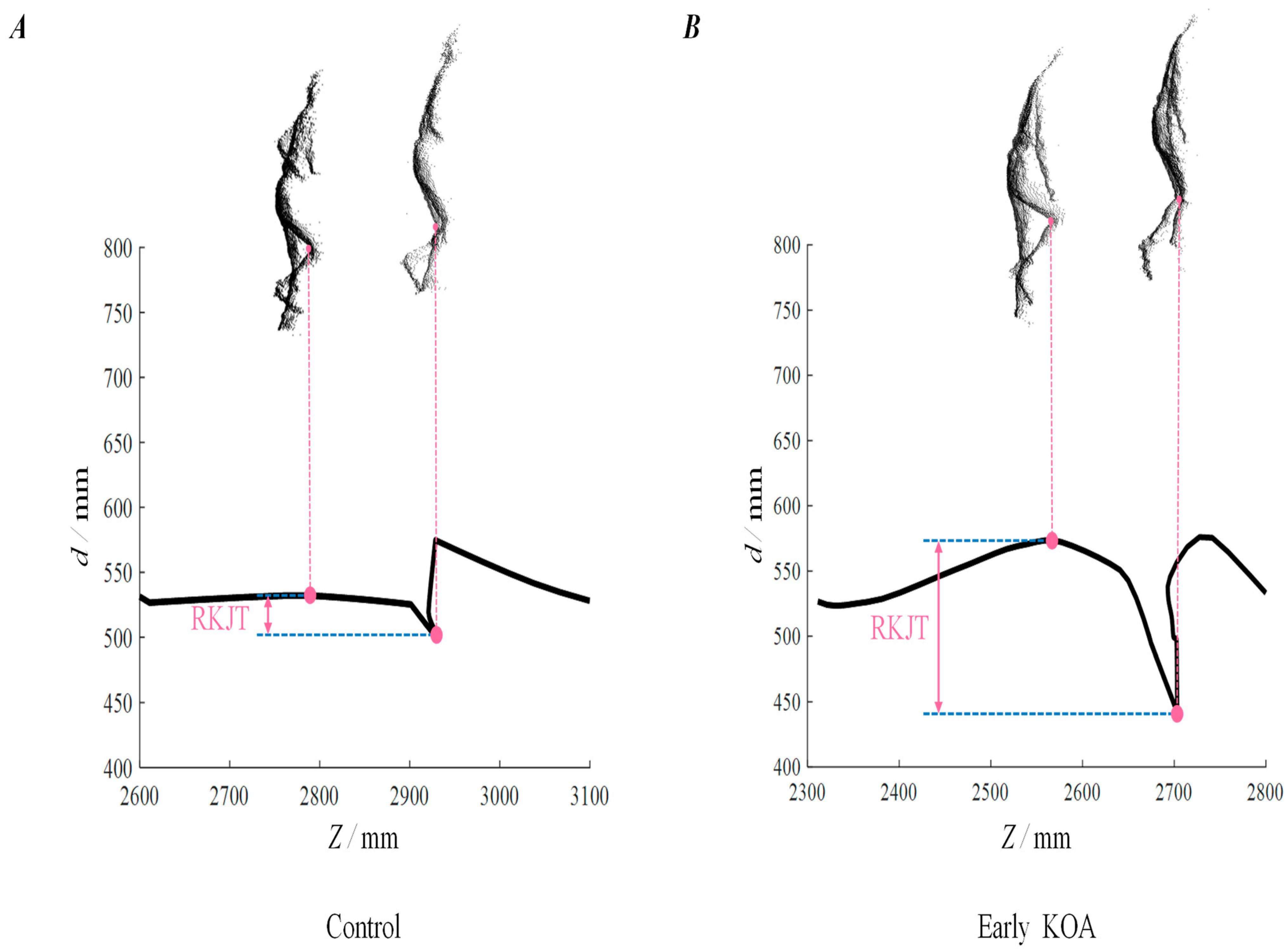
2.5. Range of Knee Joint Trajectory (RKJT)
2.6. Patients Characteristics and Covariates
2.7. Statistical Analyses
3. Results
4. Discussion
4.1. Interpretation of Larger RKJT in People at Early KOA
4.2. Significance and Clinical Impacts of Study
4.3. Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guccione, A.A.; Felson, D.T.; Anderson, J.J.; Anthony, J.M.; Zhang, Y.; Wilson, P.W.; Kelly-Hayes, M.; A Wolf, P.; E Kreger, B.; Kannel, W.B. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am. J. Public Health 1994, 84, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Guermazi, A.; Niu, J.; Hayashi, D.; Roemer, F.W.; Englund, M.; Neogi, T.; Aliabadi, P.; McLennan, C.E.; Felson, D. Prevalence of abnormalities in knees detected by MRI in adults without knee osteoarthritis: Population based observational study (Framingham Osteoarthritis Study). BMJ 2012, 345, e5339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruyere, O.; Cooper, C.; Arden, N.; Branco, J.; Brandi, M.L.; Herrero-Beaumont, G.; Berenbaum, F.; Dennison, E.; Devogelaer, J.-P.; Hochberg, M.; et al. Can we identify patients with high risk of osteoarthritis progression who will respond to treatment? A focus on epidemiology and phenotype of osteoarthritis. Drugs Aging 2015, 32, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Duffell, L.D.; Southgate, D.F.; Gulati, V.; McGregor, A.H. Balance and gait adaptations in patients with early knee osteoarthritis. Gait Posture 2014, 39, 1057–1061. [Google Scholar] [CrossRef] [Green Version]
- Mahmoudian, A.; van Dieёn, J.H.; Baert, I.A.; Bruijn, S.M.; Faber, G.S.; Luyten, F.P.; Verschueren, S.M. Changes in gait characteristics of women with early and established medial knee osteoarthritis: Results from a 2-years longitudinal study. Clin. Biomech. 2017, 50, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Meireles, S.; de Groote, F.; Reeves, N.; Verschueren, S.; Maganaris, C.; Luyten, F.; Jonkers, I. Knee contact forces are not altered in early knee osteoarthritis. Gait Posture 2016, 45, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Larsen, A.H.; Puggaard, L.; Hämäläinen, U.; Aagaard, P. Comparison of ground reaction forces and antagonist muscle coactivation during stair walking with ageing. J. Electromyogr. Kinesiol. 2008, 18, 568–580. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, G.; Deuretzbacher, G.; Heller, M.; Graichen, F.; Rohlmann, A.; Strauss, J.; Duda, G. Hip contact forces and gait patterns from routine activities. J. Biomech. 2001, 34, 859–871. [Google Scholar] [CrossRef]
- Kutzner, I.; Heinlein, B.; Graichen, F.; Bender, A.; Rohlmann, A.; Halder, A.; Beier, A.; Bergmann, G. Loading of the knee joint during activities of daily living measured in vivo in five subjects. J. Biomech. 2010, 43, 2164–2173. [Google Scholar] [CrossRef] [PubMed]
- Liikavainio, T.; Isolehto, J.; Helminen, H.J.; Perttunen, J.; Lepola, V.; Kiviranta, I.; Arokoski, J.P.; Komi, P.V. Loading and gait symmetry during level and stair walking in asymptomatic subjects with knee osteoarthritis: Importance of quadriceps femoris in reducing impact force during heel strike? Knee 2007, 14, 231–238. [Google Scholar] [CrossRef]
- Iijima, H.; Eguchi, R.; Shimoura, K.; Aoyama, T.; Takahashi, M. Stair climbing ability in patients with early knee osteoarthritis: Defining the clinical hallmarks of early disease. Gait Posture 2019, 72, 148–153. [Google Scholar] [CrossRef]
- Emery, C.A.; Whittaker, J.L.; Mahmoudian, A.; Lohmander, L.S.; Roos, E.M.; Bennell, K.L.; Toomey, C.M.; Reimer, R.A.; Thompson, D.; Ronsky, J.L.; et al. Establishing outcome measures in early knee osteoarthritis. Nat. Rev. Rheumatol. 2019, 15, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, A.; Mita, A.; Yorozu, A.; Takahashi, M. Markerless knee joint position measurement using depth data during stair walking. Sensors 2017, 17, 2698. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, A.; Iijima, H.; Takahashi, M. Staircase design for health monitoring in elderly people. J. Build. Eng. 2021, 37, 102152. [Google Scholar] [CrossRef]
- Hicks-Little, C.A.; Peindl, R.D.; Hubbard, T.J.; Scannell, B.P.; Springer, B.D.; Odum, S.M.; Fehring, T.K.; Cordova, M.L. Lower extremity joint kinematics during stair climbing in knee osteoarthritis. Med. Sci. Sport. Exerc. 2011, 43, 516–524. [Google Scholar] [CrossRef]
- Iijima, H.; Shimoura, K.; Aoyama, T.; Takahashi, M. Biomechanical characteristics of stair ambulation in patients with knee OA: A systematic review with meta-analysis toward a better definition of clinical hallmarks. Gait Posture 2018, 62, 191–201. [Google Scholar] [CrossRef]
- Shimoura, K.; Iijima, H.; Suzuki, Y.; Aoyama, T. Immediate effects of transcutaneous electrical nerve stimulation on pain and physical performance in individuals with preradiographic knee osteoarthritis: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2019, 100, 300–306.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellgren, J.; Lawrence, J. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494. [Google Scholar] [CrossRef] [Green Version]
- Iijima, H.; Suzuki, Y.; Aoyama, T.; Takahashi, M. Interaction between low back pain and knee pain contributes to disability level in individuals with knee osteoarthritis: A cross-sectional study. Osteoarthr. Cartil. 2018, 26, 1319–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, A.; Mita, A.; Georgoulas, C.; Bock, T. A Face Recognition System for Automated Door Opening with parallel Health Status Validation Using the Kinect v2, ISARC. In Proceedings of the International Symposium on Automation and Robotics in Construction, Auburn, AL, USA, 18–21 July 2016; pp. 132–140. [Google Scholar]
- Dobson, F.; Hinman, R.S.; Hall, M.; Terwee, C.; Roos, E.M.; Bennell, K. Measurement properties of performance-based measures to assess physical function in hip and knee osteoarthritis: A systematic review. Osteoarthr. Cartil. 2012, 20, 1548–1562. [Google Scholar] [CrossRef]
- McFadyen, B.J.; Winter, D.A. An integrated biomechanical analysis of normal stair ascent and descent. J. Biomech. 1988, 21, 733–744. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Akai, M.; Doi, T.; Fujino, K.; Iwaya, T.; Kurosawa, H.; Nasu, T. An outcome measure for Japanese people with knee osteoarthritis. J. Rheumatol. 2005, 32, 1524–1532. [Google Scholar]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- McConnell, S.; Kolopack, P.; Davis, A.M. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): A review of its utility and measurement properties. Arthritis Care Res. Off. J. Am. Coll. Rheumatol. 2001, 45, 453–461. [Google Scholar] [CrossRef]
- Stewart, S.; Pearson, J.; Rome, K.; Dalbeth, N.; Vandal, A.C. Analysis of data collected from right and left limbs: Accounting for dependence and improving statistical efficiency in musculoskeletal research. Gait Posture 2018, 59, 182–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannigan, J.; Chou, L.-S. Sex differences in lower extremity coordinative variability during running. Gait Posture 2019, 70, 317–322. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Person-Level Characteristics | All (n = 47 Participants) | Control (n = 27 Participants) | Early KOA (n = 20 Participants) |
|---|---|---|---|
| Age, years | 59.2 ± 5.98 | 58.7 ± 6.18 | 60.0 ± 5.79 |
| Female, no. (%) | 32 (68.1) | 17 (63.0) | 15 (75.0) |
| Height, m | 1.61 ± 0.0817 | 1.62 ± 0.0853 | 1.61 ± 0.0782 |
| Mass, kg | 59.2 ± 10.1 | 57.3 ± 8.75 | 61.8 ± 11.5 |
| BMI, kg/m2 | 22.7 ± 3.04 | 21.8 ± 2.61 | 23.9 ± 3.26 |
| Bilateral disease, no. (%) † | 16 (34.0) | 0 (0.0) | 16 (80.0) |
| VAS pain score during 11-SCT, mm | 14.3 ± 16.5; 8 [0, 63] * | 10.7 ± 11.3; 4 [0, 34] * | 19.2 ± 21.0; 10 [0, 63] * |
| JKOM, points | |||
| Pain and stiffness | 6.70 ± 4.14; 6 [0, 22] * | 5.59 ± 3.48; 5 [1, 16] * | 8.20 ± 4.56; 7 [0, 22] * |
| Activities of daily living | 2.89 ± 3.30; 2 [0, 14] * | 2.00 ± 2.47; 1 [0, 8] * | 4.10 ± 3.92; 3 [0, 14] * |
| Participation in social activities | 2.66 ± 2.05; 2 [0, 9] * | 2.15 ± 1.68; 2 [0, 7] * | 3.35 ± 2.32; 3 [0, 9] * |
| General health conditions | 1.96 ± 1.02; 2 [0, 4] * | 1.78 ± 1.05; 2 [0, 3] * | 2.20 ± 0.95; 2 [0, 4] * |
| Total score | 14.2 ± 8.22; 12 [3, 49] * | 11.5 ± 5.79; 10 [3, 25] * | 17.9 ± 9.68; 16 [6, 49] * |
| Knee-level characteristics | All (n = 90 knees) | Control (n = 55 knees) | Early KOA (n = 35 knees) |
| K&L grade, no. (%) | |||
| Grade 0 | 55 (61.1) | 55 (100.0) | 0 (0.0) |
| Grade 1 | 35 (38.9) | 0 (0.0) | 35 (100.0) |
| Independent Variable | Control (n = 55 Knees) | Early KOA (n = 35 Knees) | Difference between Control and Early KOA | Model 1 † Control vs. Early KOA | Model 2 †† Control vs. Early KOA | ||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean (95% CI) | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| RKJT, mm | 61.7 ± 18.4 | 71.7 ± 16.5 | 10.0 (−17.6, −2.39) | 1.04 (1.01, 1.08) | 0.018 | 1.04 (1.00, 1.07) | 0.044 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogawa, A.; Iijima, H.; Takahashi, M. Identification of Early Knee Osteoarthritis Based on Knee Joint Trajectory during Stair Climbing. Int. J. Environ. Res. Public Health 2022, 19, 15023. https://doi.org/10.3390/ijerph192215023
Ogawa A, Iijima H, Takahashi M. Identification of Early Knee Osteoarthritis Based on Knee Joint Trajectory during Stair Climbing. International Journal of Environmental Research and Public Health. 2022; 19(22):15023. https://doi.org/10.3390/ijerph192215023
Chicago/Turabian StyleOgawa, Ami, Hirotaka Iijima, and Masaki Takahashi. 2022. "Identification of Early Knee Osteoarthritis Based on Knee Joint Trajectory during Stair Climbing" International Journal of Environmental Research and Public Health 19, no. 22: 15023. https://doi.org/10.3390/ijerph192215023
APA StyleOgawa, A., Iijima, H., & Takahashi, M. (2022). Identification of Early Knee Osteoarthritis Based on Knee Joint Trajectory during Stair Climbing. International Journal of Environmental Research and Public Health, 19(22), 15023. https://doi.org/10.3390/ijerph192215023