
Well-Being, Physical Activity, and Social Support in Octogenarians with Heart Failure during COVID-19 Confinement: A Mixed-Methods Study

 ,
,  ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Setting
2.2. Design
2.3. Data Collection
- (1)
- Well-being was assessed using the Cantril Ladder of Life [19], a single-item indicator with a ladder of steps numbered from 0 to 10 (0 = the worst possible life, 10 = the best possible life). Participants answered on which step they stand at present. Cantril Ladder of Life validity and test-retest coefficients of 0.70 have been reported in previous studies in patients with acute coronary events. Several studies have previously used this scale in HF patients [24,25,26,27,28].
- (2)
- Physical activity was evaluated using the International Physical Activity Questionnaire (IPAQ). It contains seven items for identifying frequency and duration of low, moderate, and vigorous PA as well as inactivity during the past week. Frequency is measured in days and duration in hours and minutes. The answers to the questions were transformed into metabolic equivalent of task (MET-minutes). The total PA score is the sum of vigorous, moderate, and walking PA scores. Typical IPAQ correlations with an accelerometer were 0.80 for reliability [29]. Several studies have previously used this questionnaire in HF patients [30,31,32].
2.4. Sample Size Calculation
2.5. Data Analysis
- (1)
- Data reduction. Information was divided into grammatical content units (paragraphs and sentences). Inductive content analysis (elaborating categories from the reading and analysis of the collected material without taking into consideration the initial categories) and deductive content analysis (categories are established a priori whilst the researcher adapts each unit to an already existing category) were performed. The assessment of content belonging to the corresponding category/subcategory was performed based on two levels, intracoder and intercoder, until agreement was reached among the members of the research team [37].
- (2)
- Layout and grouping. Different graphic resources and information were obtained using CAQDAS as follows: relationships and deep structure of the text [38], graphic representations or visual images of the relationships between concepts [39], and matrices/double-entry tables in which verbal information was included according to the aspects specified by rows and columns [34]. For the calculation of the analysis of the frequency of concurrence of the categories and subcategories, the NVivo coding matrix tool was been used. A matrix was made for each category, taking into account that the subcategories were placed in the rows, whilst the classification of octogenarian/non-octogenarian was placed in the columns. The percentages of each row were calculated based on the total cell references of each subcategory.
- (3)
- Obtention of results and verification of conclusions. This phase involved the use of metaphors and analogies, as well as the inclusion of vignettes and narrative fragments, culminating with the aforementioned triangulation strategies. For textual data, description, interpretation, code counting, concurrence, comparison, and contextualization were performed. For data transformed into numerical values, statistical techniques, comparison, and contextualization were performed.
3. Results
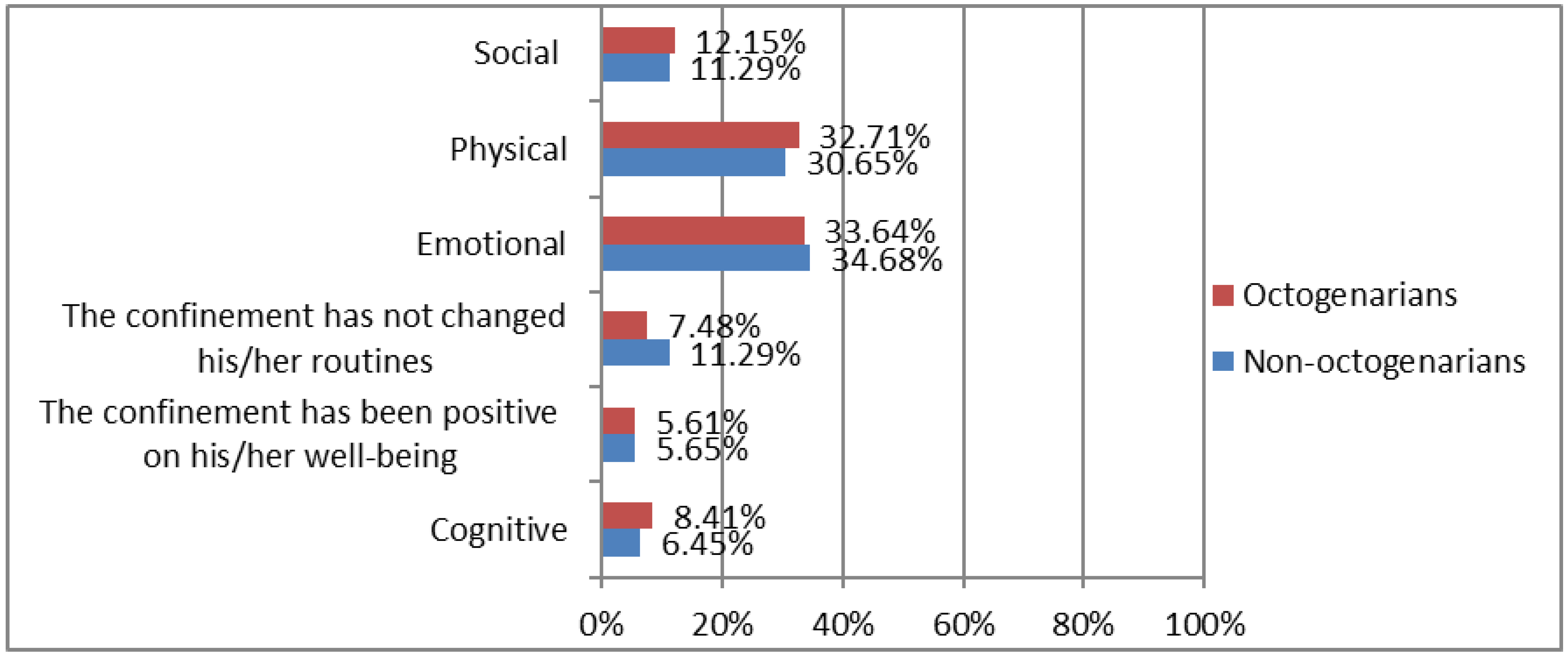
- (i)
- Alterations in well-being. This category defines the main areas of well-being affected by COVID-19. It is composed of the following six subcategories: (1) cognitive; (2) the confinement has been positive on his/her well-being; (3) the confinement has not changed his/her routines; (4) emotional; (5) physical; (6) social.
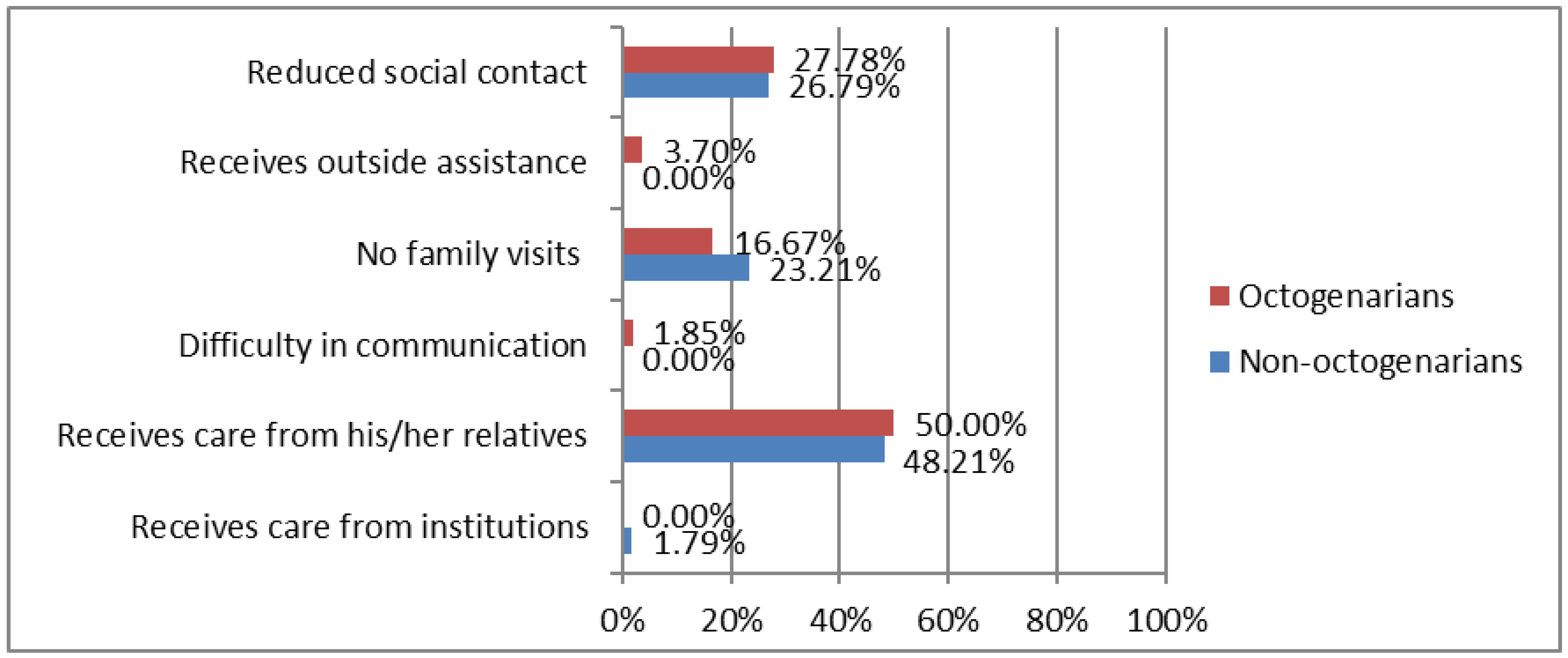
- (ii)
- Changes in social support. This category shows the main changes in social support for people with HF during COVID-19. It is composed of six subcategories: (1) receives care from institutions; (2) receives care from his/her relatives; (3) difficulty in communication; (4) no family visits; (5) receives outside assistance; (6) reduced social contact.
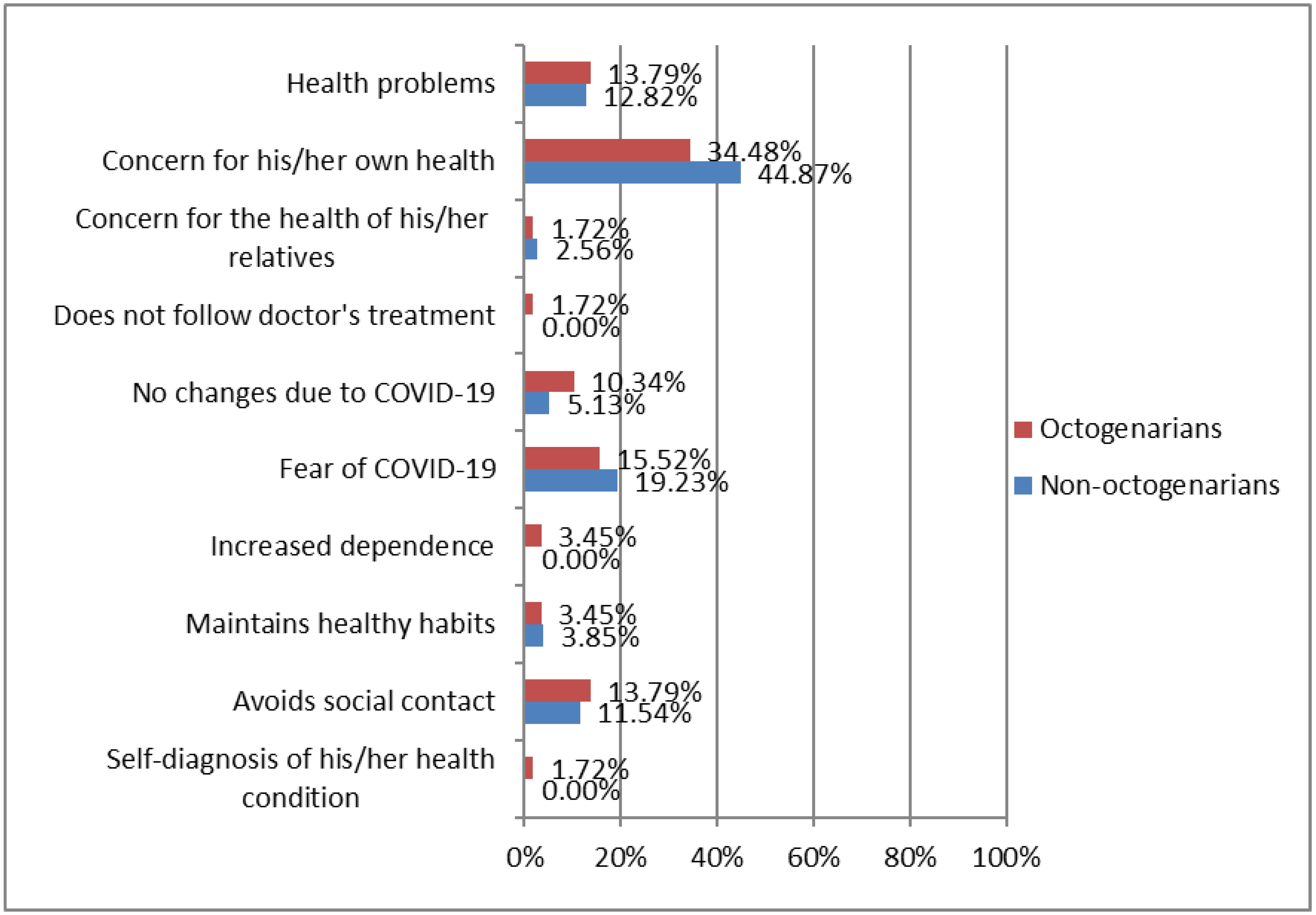
- (iii)
- Attention to HF symptoms. This category highlights the main characteristics related to the attention to HF symptoms during confinement. It is composed of ten subcategories: (1) self-diagnosis of his/her health condition; (2) avoids social contact; (3) maintains healthy habits; (4) increased dependence; (5) fear of COVID-19; (6) no changes due to COVID-19; (7) does not follow doctor’s treatment; (8) concern for the health of his/her relatives; (9) concern for his/her own health; (10) health problems.
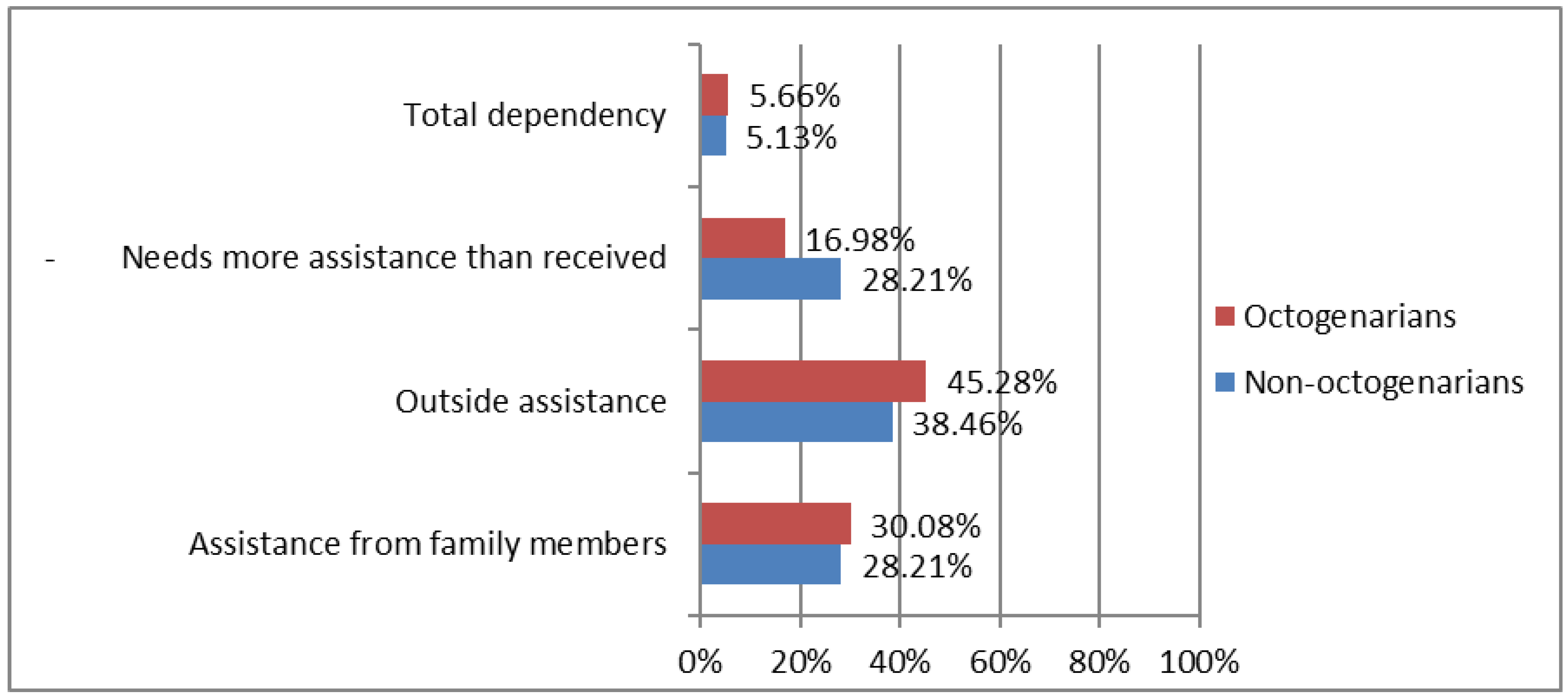
- (iv)
- Assistance needs. This category defines the needs of care and highlights the main needs or care requirements of HF patients during confinement. This category is composed of two subcategories and four contexts that define assistance needs: (1) no assistance needs; (2) if had assistance needs: (2a) assistance from family members; (2b) outside assistance (ambulance, telephone assistance, telecare button, caregiver, person for household chores and shopping, cardiac rehabilitation, neighbors); (2c) needs more assistance than received; (2d) total dependency.
- (v)
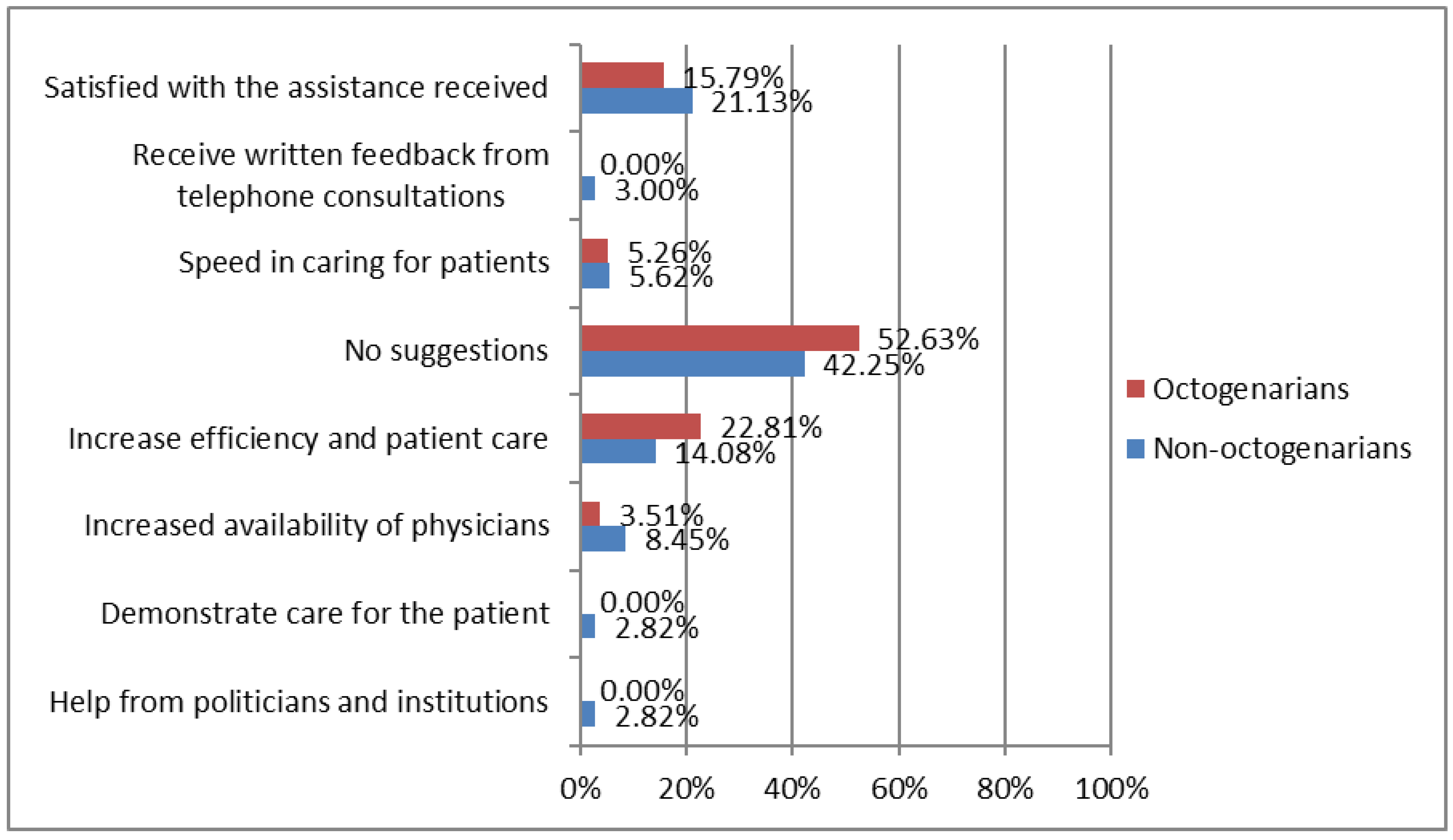
- Suggestions to improve care. This category highlights the suggestions of HF patients in order to improve their care during COVID-19 confinement. It is composed of the following eight subcategories: (1) help from politicians and from institutions; (2) demonstrate care to the patient; (3) increase the availability of physicians; (4) increase efficiency and patient care; (5) no suggestions; (6) speed in caring for patients; (7) receive written feedback from telephone consultations; (8) satisfied with the assistance received.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Daw, P.; Wood, G.E.R.; Harrison, A.; Doherty, P.J.; Veldhuijzen van Zanten, J.J.C.S.; Dalal, H.M.; Taylor, R.S.; van Beurden, S.M.; McDonagh, S.T.J.; Greaves, C.J. Barriers and facilitators to implementation of a home-based cardiac rehabilitation programme for patients with heart failure in the NHS: A mixed-methods study. BMJ Open 2022, 12, e060221. [Google Scholar] [CrossRef]
- Roger, V.L. Epidemiology of Heart Failure. Circ. Res. 2021, 128, 1421–1434. [Google Scholar] [CrossRef] [PubMed]
- McIlvennan, C.K.; Allen, L.A.; Devore, A.D.; Granger, C.B.; Kaltenbach, L.A.; Granger, B.B. Changes in Care Delivery for Patients with Heart Failure During the COVID-19 Pandemic: Results of a Multicenter Survey. J. Card Fail. 2020, 26, 635–636. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, A.N.; Tea, I.; Al-Mallah, M.H. Cardiovascular Implications of COVID-19 Infections. Methodist DeBakey Cardiovasc. J. 2020, 16, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Tersalvi, G.; Winterton, D.; Cioffi, G.M.; Ghidini, S.; Roberto, M.; Biasco, L.; Pedrazzini, G.; Dauw, J.; Ameri, P.; Vicenzi, M. Telemedicine in Heart Failure During COVID-19: A Step Into the Future. Front. Cardiovasc. Med. 2020, 7, 612818. [Google Scholar] [CrossRef] [PubMed]
- Raffaello, W.M.; Huang, I.; Budi Siswanto, B.; Pranata, R. In-depth review of cardiopulmonary support in COVID-19 patients with heart failure. World J. Cardiol. 2021, 13, 298–308. [Google Scholar] [CrossRef]
- McArthur, C.; Turcotte, L.A.; Sinn, C.L.J.; Berg, K.; Morris, J.N.; Hirdes, J.P. Social Engagement and Distress Among Home Care Recipients During the COVID-19 Pandemic in Ontario, Canada: A Retrospective Cohort Study. J. Am. Med. Dir. Assoc. 2022, 23, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- De Simone, V.; Guarise, P.; Guardalben, S.; Padovani, N.; Tondelli, S.; Sandrini, D.; Visentin, E.; Zanotto, G. Telecardiology during the COVID-19 pandemic: Past mistakes and future hopes. Am. J. Cardiovasc. Dis. 2020, 10, 34–47. [Google Scholar] [PubMed]
- Gorodeski, E.Z.; Goyal, P.; Cox, Z.L.; Thibodeau, J.T.; Reay, R.E.; Rasmusson, K.; Rogers, J.G.; Starling, R.C. Virtual Visits for Care of Patients with Heart Failure in the Era of COVID-19: A Statement from the Heart Failure Society of America. J. Card. Fail. 2020, 26, 448–456. [Google Scholar] [CrossRef]
- Raman, K.S.; Vyselaar, J.R. Patient-Reported Experiences in Outpatient Telehealth Heart Failure Management. Cardiol. Res. 2021, 12, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Vetrovsky, T.; Frybova, T.; Gant, I.; Semerad, M.; Cimler, R.; Bunc, V.; Siranec, M.; Miklikova, M.; Vesely, J.; Griva, M.; et al. The detrimental effect of COVID-19 nationwide quarantine on accelerometer-assessed physical activity of heart failure patients. ESC Hear. Fail. 2020, 7, 2093–2097. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, C.; McCullough, M.; Fuery, M.A.; Chouairi, F.; Keating, C.; Ravindra, N.G.; Miller, P.E.; Malinis, M.; Kashyap, N.; Hsiao, A.; et al. COVID-19 infections and outcomes in a live registry of heart failure patients across an integrated health care system. PLoS ONE 2020, 15, e0238829. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Quintana, E.; Vega-Acedo, L.d.C.; Santana-Herrera, D.; Pérez-Acosta, C.; Medina-Gil, J.M.; Muñoz-Díaz, E.; Rodríguez-González, F. Mental well-being among patients with congenital heart disease and heart failure during the COVID-19 pandemic. Am. J. Cardiovasc. Dis. 2021, 11, 618–623. [Google Scholar] [PubMed]
- Sammour, Y.; Spertus, J.A.; Austin, B.A.; Magalski, A.; Gupta, S.K.; Shatla, I.; Dean, E.; Kennedy, K.F.; Jones, P.G.; Nassif, M.E.; et al. Outpatient Management of Heart Failure During the COVID-19 Pandemic After Adoption of a Telehealth Model. JACC Heart Fail. 2021, 9, 916–924. [Google Scholar] [CrossRef] [PubMed]
- El-Dassouki, N.; Pfisterer, K.; Benmessaoud, C.; Young, K.; Ge, K.; Lohani, R.; Saragadam, A.; Pham, Q. The value of technology to support dyadic caregiving for individuals living with heart failure: A qualitative descriptive study (Preprint). J. Med. Internet Res. 2022, 24, e40108. [Google Scholar] [CrossRef] [PubMed]
- Baik, D.; Coats, H.; Baker, M.C. Experiences of Older Family Care Partners of Persons with Heart Failure 1 Year after the Onset of the COVID-19 Pandemic: A Qualitative Study. J. Gerontol. Nurs. 2022, 48, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Forsyth, F.; Sowden, E.; Hossain, M.Z.; Tuffnell, R.; Chew-Graham, C.; Blakeman, T.; Deaton, C. Clinicians’ and patients’ experiences of managing heart failure during the COVID-19 pandemic: A qualitative study. BJGP Open 2021, 5. [Google Scholar] [CrossRef]
- Smith, J. Well-being and health from age 70 to 100: Findings from the Berlin Aging Study. Eur. Rev. 2001, 9, 461–477. [Google Scholar] [CrossRef]
- Radhakrishnan, K.; Allen, C.; DeMain, A.S.; Park, L. Impact of COVID-19 on Heart Failure Self-Care: A Qualitative Study. J. Cardiovasc. Nurs. 2021, 36, 609–617. [Google Scholar] [CrossRef]
- Creswell, J.; Guetterman, T. Educational Research: Planning, Conducting, and Evaluating Quantitative and Qualitative Research, 6th ed.; Pearson: New York, NY, USA, 2018. [Google Scholar]
- Hernández Sampieri, R.; Fernández Collado, C.; Baptista Lucio, P. Metodología de la Investigación—Sexta Edición; McGraw-Hill Education: Mexico City, Mexico, 2014. [Google Scholar]
- García-Peñalvo, F.J.; López, L.M.; Sánchez-Gómez, M.C. Empirical evaluation of educational interactive systems. Qual. Quant. 2018, 52, 2427–2434. [Google Scholar] [CrossRef]
- Sarrado, J.J.; Clèries, X.; Ferrer, M.; Kronfly, E. Evidencia científica en medicina: ¿única alternativa? Gac. Sanitaria 2004, 18, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Ståhle, A.; Mattsson, E.; Rydén, L.; Unden, A.; Nordlander, R. Improved physical fitness and quality of life following training of elderly patients after acute coronary events. A 1 year follow-up randomized controlled study. Eur. Heart J. 1999, 20, 1475–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoekstra, T.; Lesman-Leegte, I.; van Veldhuisen, D.J.; Sanderman, R.; Jaarsma, T. Quality of life is impaired similarly in heart failure patients with preserved and reduced ejection fraction. Eur. J. Heart Fail. 2011, 13, 1013–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luttik, M.L.; Lesman-Leegte, I.; Jaarsma, T. Quality of Life and Depressive Symptoms in Heart Failure Patients and Their Partners: The Impact of Role and Gender. J. Card. Fail. 2009, 15, 580–585. [Google Scholar] [CrossRef]
- Luttik, M.L.; Jaarsma, T.; Veeger, N.; van Veldhuisen, D.J. Marital status, quality of life, and clinical outcome in patients with heart failure. Heart Lung. 2006, 35, 3–8. [Google Scholar] [CrossRef]
- Lesman-Leegte, I.; Jaarsma, T.; Coyne, J.C.; Hillege, H.L.; Van Veldhuisen, D.J.; Sanderman, R. Quality of Life and Depressive Symptoms in the Elderly: A Comparison Between Patients with Heart Failure and Age- and Gender-Matched Community Controls. J. Card. Fail. 2009, 15, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Klompstra, L.; Deka, P.; Almenar, L.; Pathak, D.; Muñoz-Gómez, E.; López-Vilella, R.; Marques-Sule, E. Physical activity enjoyment, exercise motivation, and physical activity in patients with heart failure: A mediation analysis. Clin. Rehabil. 2022, 36. [Google Scholar] [CrossRef]
- Deka, P.; Almenar, L.; Pathak, D.; Klompstra, L.; López-Vilella, R.; Marques-Sule, E. Depression mediates physical activity readiness and physical activity in patients with heart failure. ESC Heart Fail. 2021, 8, 5259–5265. [Google Scholar] [CrossRef]
- Guimarães, G.V.; Carvalho, V.O.; Torlai, V.; Bocchi, E.A. Physical activity profile in heart failure patients from a Brazilian tertiary cardiology hospital. Cardiol. J. 2010, 17, 143–145. [Google Scholar]
- García, J.L.C.; Martín-Sevillano, R.; Sánchez-Gómez, M.C.; Martín-Cilleros, M.V.; Verdugo-Castro, S.; Mena, J.; Pinto-Llorente, A.M.; Álvarez, V.I. A Qualitative Study and Analysis on the Use, Utility, and Emotions of Technology by the Elderly in Spain. Comput. Support. Qual. Res. 2022, 466, 248–263. [Google Scholar] [CrossRef]
- Miles, M.B.; Huberman, A.M. Qualitative Data Analysis: An Expanded Sourcebook; SAGE: London, UK, 1994; p. 358. [Google Scholar]
- Cilleros, M.V.M.; Gómez, M.C.S. Análisis cualitativo de tópicos vinculados a la calidad de vida en personas con discapacidad. Ciênc. Saúde Colet. 2016, 21, 2365–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Sabiote, C.; Lorenzo-Quiles, O. Teoría y Práctica del Análisis de Datos Cualitativo. Proceso General y Criterios de Calidad; Revista Internacional de Ciencias Sociales y Humanidades: Ciudad Victoria, Mexico, 2005; Volume 15, pp. 133–154. [Google Scholar]
- Rodríguez-Jiménez, C.J.; Corrales-Vázquez, J.M.; Sánchez-Gómez, M.C.; Losada-Vázquez, Á.; Cabanillas-García, J.L.; Losada-Moncada, M. Reflexiones del profesorado de secundaria sobre la utilidad y viabilidad de las técnicas participativas en el sistema educativo formal. New Trends Qual. Res. 2022, 12, e636. [Google Scholar]
- Wainer, H. Understanding Graphs and Tables. Educ. Res. 1992, 21, 14–23. [Google Scholar] [CrossRef]
- Strauss, A.; Corbin, J. Basics of Qualitative Research. Grounded Theory Procedures and Techniques; SAGE Publications Ltd.: London, UK, 2022. [Google Scholar]
- Rantanen, T.; Eronen, J.; Kauppinen, M.; Kokko, K.; Sanaslahti, S.; Kajan, N.; Portegijs, E. Life-Space Mobility and Active Aging as Factors Underlying Quality of Life among Older People before and during COVID-19 Lock-down in Finland–a Longitudinal Study. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 76, e60–e67. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.M.; Page, D.; Okely, J.A.; Corley, J.; Welstead, M.; Skarabela, B.; Redmond, P.; Russ, T.C.; Cox, S.R. Impact of COVID-19 lockdown on psychosocial factors, health, and lifestyle in Scottish octogenarians: The Lothian Birth Cohort 1936 study. PLoS ONE 2021, 16, e0253153. [Google Scholar] [CrossRef]
- Brasca, F.M.A.; Casale, M.C.; Canevese, F.L.; Tortora, G.; Pagano, G.; Botto, G.L. Physical Activity in Patients with Heart Failure During and After COVID-19 Lockdown: Single-Center Observational Retrospective Study. JMIR Cardio. 2022, 6, e30661. [Google Scholar] [CrossRef]
- Toraman, N.F.; Ayceman, N. Effects of six weeks of detraining on retention of functional fitness of old people after nine weeks of multicomponent training. Br. J. Sport. Med. 2005, 39, 565–568. [Google Scholar] [CrossRef]
- Bittner, V.; Weiner, D.H.; Yusuf, S.; Rogers, W.J.; McIntyre, K.M.; Bangdiwala, S.I.; Kronenberg, M.W.; Kostis, J.B.; Kohn, R.M.; Guillotte, M.; et al. Prediction of mortality and morbidity with a 6-minute walk test in patients with left ventricular dysfunction. SOLVD Investigators. JAMA 1993, 270, 1702–1707. [Google Scholar] [CrossRef]
- Ferrer, A.; Octabaix Study Group; Formiga, F.; Cunillera, O.; Megido, M.J.; Corbella, X.; Almeda, J. Predicting factors of health-related quality of life in octogenarians: A 3-year follow-up longitudinal study. Qual. Life Res. 2015, 24, 2701–2711. [Google Scholar] [CrossRef]
- Golden, J.; Conroy, R.M.; Bruce, I.; Denihan, A.; Greene, E.; Kirby, M.; Lawlor, B.A. Loneliness, social support networks, mood and wellbeing in community-dwelling elderly. Int. J. Geriatr. Psychiatry 2009, 24, 694–700. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Has your well-being been altered during COVID-19 confinement? Please explain. 2. How has the social support (family, friends, neighbors) you receive changed during the COVID-19 confinement? Please explain. 3. How has your attention to heart failure symptoms changed due to the COVID-19 confinement? Please explain. 4. What assistance needs do you have now during the COVID-19 confinement? Please explain. 5. Do you have any suggestions or advice on how health and healthcare services can assist you in your self-managed care for your heart failure? Please explain. |
| Variable | Mean ± SD/Frequency (Percentage) |
|---|---|
| Age (years) | 74.16 ± 12.90 |
| Non-octogenarians (<80 years) | 67 (55.83%) |
| Octogenarians (≥80 years) | 53 (44.16%) |
| Sex | |
| Male | 73 (60.83%) |
| Female | 47 (39.17%) |
| Time since diagnosis (months) | 78.73 ± 94.21 |
| Education | |
| Primary | 79 (65.83%) |
| Secondary | 17 (14.17%) |
| University | 24 (20.00%) |
| Marital status | |
| Single | 5 (4.17%) |
| Married | 81 (67.50%) |
| Divorced | 2 (1.67%) |
| Widow | 32 (26.67%) |
| Variable | Before COVID-19 Confinement (n = 120) | During COVID-19 Confinement (n = 120) | p-Value |
|---|---|---|---|
| Well-being | 7.5 ± 1.57 | 5.98 ± 2.14 | p < 0.001 * |
| Physical activity (METS-minute) | |||
| Light PA | 764.71 ± 826.08 | 103.59 ± 376.77 | p < 0.001 * |
| Moderate PA | 6.19 ± 13.59 | 1.49 ± 3.39 | p < 0.001 * |
| Vigorous PA | 1.68 ± 14.81 | 0.00 ± 0.00 | p = 0.26 |
| Sedentary time | 7.03 ± 2.41 | 9.39 ± 2.77 | p < 0.001 * |
| Total PA | 772.57 ± 828.96 | 105.08 ± 376.90 | p < 0.001 * |
| Variable | Non-Octogenarians (<80 Years) (n = 67) | Octogenarians (≥80 Years) (n = 53) | p-Value between Groups |
|---|---|---|---|
| Well-being | |||
| Before COVID-19 confinement | 7.46 ± 1.65 | 7.55 ± 1.47 | p = 0.77 |
| During COVID-19 confinement | 6.37 ± 2.12 | 5.49 ± 2.09 | p = 0.02 * |
| p-value between time measurements | p < 0.001 * | p < 0.001 * | |
| Physical activity (METS-minute) | |||
| Light PA | |||
| Before COVID-19 confinement | 844.93 ± 967.35 | 663.29 ± 595.96 | p = 0.23 |
| During COVID-19 confinement | 104.02 ± 285.64 | 103.05 ± 470.43 | p = 0.99 |
| p-value between time measurements | p < 0.001 * | p < 0.001 * | |
| Moderate PA | |||
| Before COVID-19 confinement | 7.09 ± 14.44 | 5.05 ± 12.47 | p = 0.42 |
| During COVID-19 confinement | 2.05 ± 3.93 | 0.80 ± 2.40 | p = 0.04 * |
| p-value between time measurements | p = 0.001 * | p = 0.02 * | |
| Vigorous PA | |||
| Before COVID-19 confinement | 2.75 ± 19.72 | 0.33 ± 2.20 | p = 0.38 |
| During COVID-19 confinement | 0.00 ± 0.00 | 0.00 ± 0.00 | p = 1.00 |
| p-value between time measurements | p = 0.13 | p = 0.87 | |
| Sedentary time | |||
| Before COVID-19 confinement | 6.58 ± 2.20 | 7.58 ± 2.56 | p = 0.06 |
| During COVID-19 confinement | 8.91 ± 2.261 | 10.00 ± 3.22 | p = 0.03 * |
| p-value between time measurements | p < 0.001 * | p < 0.001 * | |
| Total PA | |||
| Before COVID-19 confinement | 854.77 ± 971.31 | 668.66 ± 596.16 | p = 0.39 |
| During COVID-19 confinement | 106.06 ± 286.01 | 103.84 ± 470.37 | p = 0.15 |
| p-value between time measurements | p < 0.001 * | p < 0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques-Sule, E.; Muñoz-Gómez, E.; Almenar-Bonet, L.; Moreno-Segura, N.; Sánchez-Gómez, M.-C.; Deka, P.; López-Vilella, R.; Klompstra, L.; Cabanillas-García, J.L. Well-Being, Physical Activity, and Social Support in Octogenarians with Heart Failure during COVID-19 Confinement: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2022, 19, 15316. https://doi.org/10.3390/ijerph192215316
Marques-Sule E, Muñoz-Gómez E, Almenar-Bonet L, Moreno-Segura N, Sánchez-Gómez M-C, Deka P, López-Vilella R, Klompstra L, Cabanillas-García JL. Well-Being, Physical Activity, and Social Support in Octogenarians with Heart Failure during COVID-19 Confinement: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2022; 19(22):15316. https://doi.org/10.3390/ijerph192215316
Chicago/Turabian StyleMarques-Sule, Elena, Elena Muñoz-Gómez, Luis Almenar-Bonet, Noemi Moreno-Segura, María-Cruz Sánchez-Gómez, Pallav Deka, Raquel López-Vilella, Leonie Klompstra, and Juan Luis Cabanillas-García. 2022. "Well-Being, Physical Activity, and Social Support in Octogenarians with Heart Failure during COVID-19 Confinement: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 19, no. 22: 15316. https://doi.org/10.3390/ijerph192215316
APA StyleMarques-Sule, E., Muñoz-Gómez, E., Almenar-Bonet, L., Moreno-Segura, N., Sánchez-Gómez, M. -C., Deka, P., López-Vilella, R., Klompstra, L., & Cabanillas-García, J. L. (2022). Well-Being, Physical Activity, and Social Support in Octogenarians with Heart Failure during COVID-19 Confinement: A Mixed-Methods Study. International Journal of Environmental Research and Public Health, 19(22), 15316. https://doi.org/10.3390/ijerph192215316