
Intervention of Physical Activity for University Students with Anxiety and Depression during the COVID-19 Pandemic Prevention and Control Period: A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
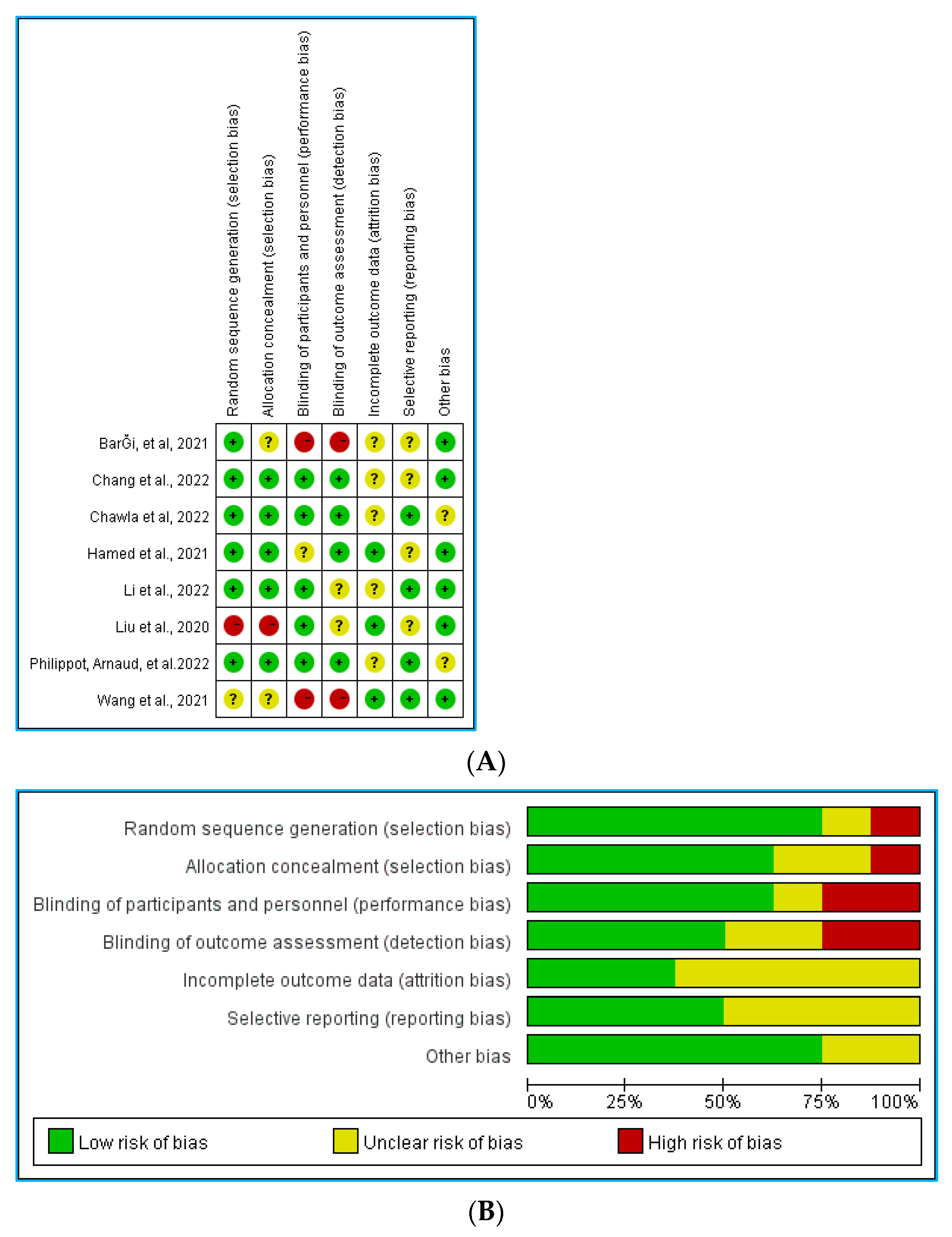
2.4. Quality Assessment of Eligible Study
2.5. Study Analysis Method
3. Results
3.1. Studies Selection
3.2. Characteristics of Eligible Studies
3.3. Interventions and Controls
3.4. Risk of Bias
3.5. Meta-Analysis of Outcome Indicators
3.5.1. Physical Activity Compared to No Intervention Control
3.5.2. Regression Analysis
3.5.3. Sub-Group Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baloch, S.; Baloch, M.A.; Zheng, T.; Pei, X. The Coronavirus Disease 2019 (COVID-19) Pandemic. Tohoku J. Exp. Med. 2020, 250, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 25 October 2022).
- Agrawal, A. Sustainability of airlines in India with Covid-19: Challenges ahead and possible way-outs. J. Revenue Pricing Manag. 2020, 20, 457–472. [Google Scholar] [CrossRef]
- Alsharef, A.; Banerjee, S.; Uddin, S.M.J.; Albert, A.; Jaselskis, E. Early Impacts of the COVID-19 Pandemic on the United States Construction Industry. Int. J. Environ. Res. Public Health 2021, 18, 1559. [Google Scholar] [CrossRef] [PubMed]
- Beh, L.-S.; Lin, W.L. Impact of COVID-19 on ASEAN tourism industry. J. Asian Public Policy 2021, 15, 300–320. [Google Scholar] [CrossRef]
- Kolahchi, Z.; De Domenico, M.; Uddin, L.Q.; Cauda, V.; Grossmann, I.; Lacasa, L.; Grancini, G.; Mahmoudi, M.; Rezaei, N. COVID-19 and Its Global Economic Impact. Adv. Exp. Med. Biol. 2021, 1318, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Pinilla, J.; Barber, P.; Vallejo-Torres, L.; Rodriguez-Mireles, S.; Lopez-Valcarcel, B.G.; Serra-Majem, L. The Economic Impact of the SARS-COV-2 (COVID-19) Pandemic in Spain. Int. J. Environ. Res. Public Health 2021, 18, 4708. [Google Scholar] [CrossRef]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14, 20. [Google Scholar] [CrossRef]
- Guessoum, S.B.; Lachal, J.; Radjack, R.; Carretier, E.; Minassian, S.; Benoit, L.; Moro, M.R. Adolescent psychiatric disorders during the COVID-19 pandemic and lockdown. Psychiatry Res. 2020, 291, 113264. [Google Scholar] [CrossRef]
- Kourti, A.; Stavridou, A.; Panagouli, E.; Psaltopoulou, T.; Spiliopoulou, C.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Domestic Violence during the COVID-19 Pandemic: A Systematic Review. Trauma Violence Abus. 2021. [Google Scholar] [CrossRef]
- Griffith, A.K. Parental Burnout and Child Maltreatment during the COVID-19 Pandemic. J. Fam. Violence 2022, 37, 725–731. [Google Scholar] [CrossRef]
- Haider, I.I.; Tiwana, F.; Tahir, S.M. Impact of the COVID-19 Pandemic on Adult Mental Health. Pak. J. Med. Sci. 2020, 36, S90–S94. [Google Scholar] [CrossRef] [PubMed]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghazawy, E.R.; Ewis, A.A.; Mahfouz, E.M.; Khalil, D.M.; Arafa, A.; Mohammed, Z.; Mohammed, E.F.; Hassan, E.E.; Abdel Hamid, S.; Ewis, S.A.; et al. Psychological impacts of COVID-19 pandemic on the university students in Egypt. Health Promot. Int. 2021, 36, 1116–1125. [Google Scholar] [CrossRef] [PubMed]
- Pratomo, H. From Social Distancing to Physical Distancing: A Challenge for Evaluating Public Health Intervention against COVID-19. Kesmas-Natl. Public Health J. 2020, 15, 60–62. [Google Scholar] [CrossRef]
- Dergaa, I.; Abdelrahman, H.; Varma, A.; Yousfi, N.; Souissi, A.; Ghram, A.; Hammad, A.S.; Musa, E.R.; Taheri, M.; Irandoust, K.; et al. COVID-19 Vaccination, Herd Immunity and the Transition toward Normalcy: Challenges with the Upcoming Sports Events. Ann. Appl. Sport Sci. 2021, 9, 10. [Google Scholar] [CrossRef]
- Daly, Z.; Slemon, A.; Richardson, C.G.; Salway, T.; McAuliffe, C.; Gadermann, A.M.; Thomson, K.C.; Hirani, S.; Jenkins, E.K. Associations between periods of COVID-19 quarantine and mental health in Canada. Psychiatry Res. 2021, 295, 113631. [Google Scholar] [CrossRef] [PubMed]
- Sigler, T.; Mahmuda, S.; Kimpton, A.; Loginova, J.; Wohland, P.; Charles-Edwards, E.; Corcoran, J. The socio-spatial determinants of COVID-19 diffusion: The impact of globalisation, settlement characteristics and population. Glob. Health 2021, 17, 56. [Google Scholar] [CrossRef]
- Woodruff, S.J.; Coyne, P.; St-Pierre, E. Stress, physical activity, and screen-related sedentary behaviour within the first month of the COVID-19 pandemic. Appl. Psychol. Health Well Being 2021, 13, 454–468. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Kaparounaki, C.K.; Patsali, M.E.; Mousa, D.V.; Papadopoulou, E.V.K.; Papadopoulou, K.K.K.; Fountoulakis, K.N. University students’ mental health amidst the COVID-19 quarantine in Greece. Psychiatry Res. 2020, 290, 113111. [Google Scholar] [CrossRef]
- Wu, L.; Guo, X.; Shang, Z.; Sun, Z.; Jia, Y.; Sun, L.; Liu, W. China experience from COVID-19: Mental health in mandatory quarantine zones urgently requires intervention. Psychol. Trauma 2020, 12, S3–S5. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, B.; Al-Jumaily, A.; Fong, K.N.K.; Prasad, P.; Meena, S.K.; Tong, R.K. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak Quarantine, Isolation, and Lockdown Policies on Mental Health and Suicide. Front. Psychiatry 2021, 12, 565190. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, J.; Seto, S.; Fukuda, Y.; Funakoshi, S.; Amae, S.; Onobe, J.; Izumi, S.; Ito, K.; Imamura, F. Mental Health and Physical Activity among Children and Adolescents during the COVID-19 Pandemic. Tohoku J. Exp. Med. 2021, 253, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Zivin, K.; Eisenberg, D.; Gollust, S.E.; Golberstein, E. Persistence of mental health problems and needs in a college student population. J. Affect. Disord. 2009, 117, 180–185. [Google Scholar] [CrossRef]
- Karaman, M.A.; Lerma, E.; Vela, J.C.; Watson, J.C. Predictors of Academic Stress among College Students. J. Coll. Couns. 2019, 22, 41–55. [Google Scholar] [CrossRef] [Green Version]
- Kite, C.; Lagojda, L.; Clark, C.C.T.; Uthman, O.; Denton, F.; McGregor, G.; Harwood, A.E.; Atkinson, L.; Broom, D.R.; Kyrou, I.; et al. Changes in Physical Activity and Sedentary Behaviour Due to Enforced COVID-19-Related Lockdown and Movement Restrictions: A Protocol for a Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 5251. [Google Scholar] [CrossRef]
- Abdul Rahim, N.; Zainol Abidin, M.Z.A.; Shalan, N.A.A.M.; Bin Karim, Z.; Abdul Aziz, N.U.; Avin, F.A. COVID-19 Lockdown: Physical Activity, Sedentary Behaviour, and Academic Motivation among Undergraduates University Students in Malaysia. Ann. Appl. Sport Sci. 2022, 9. [Google Scholar] [CrossRef]
- Faisal, R.A.; Jobe, M.C.; Ahmed, O.; Sharker, T. Mental Health Status, Anxiety, and Depression Levels of Bangladeshi University Students during the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2022, 20, 1500–1515. [Google Scholar] [CrossRef]
- Zhai, Y.; Du, X. Addressing collegiate mental health amid COVID-19 pandemic. Psychiatry Res. 2020, 288, 113003. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br. J. Psychiatry 2021, 218, 326–333. [Google Scholar] [CrossRef]
- Xu, Y.; Su, S.; Jiang, Z.; Guo, S.; Lu, Q.; Liu, L.; Zhao, Y.; Wu, P.; Que, J.; Shi, L.; et al. Prevalence and Risk Factors of Mental Health Symptoms and Suicidal Behavior among University Students in Wuhan, China during the COVID-19 Pandemic. Front. Psychiatry 2021, 12, 695017. [Google Scholar] [CrossRef] [PubMed]
- Goldrick-Rab, S.; Coca, V.; Gill, J.; Peele, M.; Clark, K.; Looker, E. Self-reported COVID-19 infection and implications for mental health and food insecurity among American college students. Proc. Natl. Acad. Sci. USA 2022, 119, e2111787119. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.T.; Tan, S.S.; Tan, C.X. Screen time-based sedentary behaviour, eating regulation and weight status of university students during the COVID-19 lockdown. Nutr. Food Sci. 2022, 52, 281–291. [Google Scholar] [CrossRef]
- Castaneda-Babarro, A.; Arbillaga-Etxarri, A.; Gutierrez-Santamaria, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Zhang, L.; Yu, W.; Yu, B.; Liu, M.; Zhang, D.; Yang, S. Impact of COVID-19 lockdown on activity patterns and weight status among youths in China: The COVID-19 Impact on Lifestyle Change Survey (COINLICS). Int. J. Obes. 2021, 45, 695–699. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Drawve, G.; Harris, C. Facing new fears during the COVID-19 pandemic: The State of America’s mental health. J. Anxiety Disord. 2020, 75, 102291. [Google Scholar] [CrossRef]
- Bosselmann, V.; Amatriain-Fernandez, S.; Gronwald, T.; Murillo-Rodriguez, E.; Machado, S.; Budde, H. Physical Activity, Boredom and Fear of COVID-19 among Adolescents in Germany. Front. Psychol. 2021, 12, 624206. [Google Scholar] [CrossRef]
- Ishikawa, J.; Nishimura, R.; Ishikawa, A. Early-life stress induces anxiety-like behaviors and activity imbalances in the medial prefrontal cortex and amygdala in adult rats. Eur. J. Neurosci. 2015, 41, 442–453. [Google Scholar] [CrossRef]
- Suzuki, Y.; Tanaka, S.C. Functions of the ventromedial prefrontal cortex in emotion regulation under stress. Sci. Rep. 2021, 11, 18225. [Google Scholar] [CrossRef]
- Mladenović, M.; Stojanović, N.; Stojanović, D.; Živković, M.; Aleksić, D.; Tešanović, G.; Momčilović, V. Emotional Reactivity and Emotion Regulation among Young Adults during COVID-19 Lockdown: The Moderating Role of Gender and Engagement in Sports. Front. Psychol. 2021, 12, 774732. [Google Scholar] [CrossRef]
- San Román-Mata, S.; Puertas-Molero, P.; Ubago-Jiménez, J.L.; González-Valero, G. Benefits of Physical Activity and Its Associations with Resilience, Emotional Intelligence, and Psychological Distress in University Students from Southern Spain. Int. J. Environ. Res. Public Health 2020, 17, 4474. [Google Scholar] [CrossRef]
- Shahrokhian, N.; Hassanzadeh, S.; Hashemi Razini, H.; Ramshini, M. The Effects of Cognitive-Behavioral Therapy (CBT) in Well-Being and Perceived Stress in Adolescents with Low Academic Performance during the COVID-19 Pandemic. Int. J. Sport Stud. Health 2021, 4, e122504. [Google Scholar] [CrossRef]
- WHO. Guidelines Approved by the Guidelines Review Committee. Available online: https://www.who.int/zh/news-room/campaigns/connecting-the-world-to-combat-coronavirus/healthyathome/healthyathome---physical-activity (accessed on 25 October 2022).
- Vancini, R.L.; Borges Viana, R.; dos Santos Andrade, M.; Andre Barbosa de Lira, C.; Theodoros Nikolaidis, P.; Aparecido de Almeida, A.; Knechtle, B. YouTube as a Source of Information about Physical Exercise during COVID-19 Outbreak. Int. J. Sport Stud. Health 2021, 4, e123312. [Google Scholar] [CrossRef]
- O’Brien, K.; Nixon, S.; Tynan, A.M.; Glazier, R. Aerobic exercise interventions for adults living with HIV/AIDS. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Howe, T.E.; Rochester, L.; Neil, F.; Skelton, D.A.; Ballinger, C. Exercise for improving balance in older people. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.; Slavet, J.; Miller, D.P.; Haneuse, S.; Beardslee, W.; Davison, K. Dose-response effects of exercise on behavioral health in children and adolescents. Ment. Health Phys. Act. 2017, 12, 110–115. [Google Scholar] [CrossRef]
- McMahon, E.M.; Corcoran, P.; O’Regan, G.; Keeley, H.; Cannon, M.; Carli, V.; Wasserman, C.; Hadlaczky, G.; Sarchiapone, M.; Apter, A.; et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur. Child Adolesc. Psychiatry 2017, 26, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1, CD012424. [Google Scholar] [CrossRef] [PubMed]
- Irandoust, K.; Taheri, M.; Chtourou, H.; Nikolaidis, P.T.; Rosemann, T.; Knechtle, B. Effect of Time-of-Day-Exercise in Group Settings on Level of Mood and Depression of Former Elite Male Athletes. Int. J. Environ. Res. Public Health 2019, 16, 3541. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.W.; Barnes, S.; Barnes, C.; Defina, L.F.; Nakonezny, P.; Emslie, G.J. Depressed Adolescents Treated with Exercise (DATE): A pilot randomized controlled trial to test feasibility and establish preliminary effect sizes. Ment. Health Phys. Act. 2013, 6, 119–131. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Rosenbaum, S.; Richards, J.; Ward, P.B.; Stubbs, B. Exercise improves physical and psychological quality of life in people with depression: A meta-analysis including the evaluation of control group response. Psychiatry Res. 2016, 241, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helgadottir, B.; Forsell, Y.; Hallgren, M.; Moller, J.; Ekblom, O. Long-term effects of exercise at different intensity levels on depression: A randomized controlled trial. Prev. Med. 2017, 105, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M.; Minghetti, A.; Beck, J.; Zahner, L.; Donath, L. Sprint Interval Training and Continuous Aerobic Exercise Training Have Similar Effects on Exercise Motivation and Affective Responses to Exercise in Patients with Major Depressive Disorders: A Randomized Controlled Trial. Front. Psychiatry 2018, 9, 694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, D.J.; Sirard, J.R.; Neumark-Sztainer, D. Adolescents’ attitudes toward sports, exercise, and fitness predict physical activity 5 and 10 years later. Prev. Med. 2011, 52, 130–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, S.B.; Overland, S.; Hatch, S.L.; Wessely, S.; Mykletun, A.; Hotopf, M. Exercise and the Prevention of Depression: Results of the HUNT Cohort Study. Am. J. Psychiatry 2018, 175, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wang, A.; Wu, Y.; Han, N.; Huang, H. Research on the impact of online Baduanjin on the mental health of college freshmen under the new crown pneumonia epidemic. Health Prof. Educ. 2021, 39, 155–159. [Google Scholar]
- Liu, Y.; LI, X.; WANG, X.; YANG, N.; WAN, B.; SHI, B. Mediating Effect of Exercise Intervention on Self-Efficacy of Negative Emotion Regulation of Home Schooled Students during the COVID-19 Pandemic. J. Beijing Sport Univ. 2020, 43, 76–83. [Google Scholar] [CrossRef]
- Chang, T.F.H.; Ley, B.L.; Ramburn, T.T.; Srinivasan, S.; Hariri, S.; Purandare, P.; Subramaniam, B. Online Isha Upa Yoga for student mental health and well-being during COVID-19: A randomized control trial. Appl. Psychol. Health Well-Being 2022, 14, 1408–1428. [Google Scholar] [CrossRef]
- Li, K.; Walczak-Kozłowska, T.; Lipowski, M.; Li, J.; Krokosz, D.; Su, Y.; Yu, H.; Fan, H. The effect of the Baduanjin exercise on COVID-19-related anxiety, psychological well-being and lower back pain of college students during the pandemic. BMC Sports Sci. Med. Rehabil. 2022, 14, 102. [Google Scholar] [CrossRef]
- Hamed, N.; Abdel-aziem, A.; Muhsen, B.; Eid, M.; Allam, H.; El-Gendy, A.; El Sayyad, L. The effect of aerobic training versus cognitive behavioral therapy in management of anxiety, depression and stress related to COVID 19 pandemic among university students: A randomized controlled trial. Med. Sci. 2021, 25, 2233–2246. [Google Scholar]
- Chawla, G.; Azharuddin, M.; Ahmad, I.; Hussain, D.m. Effect Of Whole Body Vibration on Depression, Anxiety, Stress and Quality of Life in Collegiate Students: A Randomized Controlled Trial. Oman Med. J. 2022, 37. [Google Scholar] [CrossRef] [PubMed]
- Bargi, G. Effectiveness of physical activity counseling in university students educated by distance learning during COVID-19 pandemic: A randomized-controlled trial. J. Basic Clin. Health Sci. 2022, 6, 40–50. [Google Scholar] [CrossRef]
- Philippot, A.; Moulin, P.; Charon, M.H.; Balestra, C.; Dubois, V.; de Timary, P.; De Volder, A.; Bleyenheuft, Y.; Lambrechts, K. Feasibility of Online High-Intensity Interval Training (HIIT) on Psychological Symptoms in Students in Lockdown during the COVID-19 Pandemic: A Randomized Controlled Trial. Front. Psychiatry 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Caputo, E.L.; Reichert, F.F. Studies of Physical Activity and COVID-19 during the Pandemic: A Scoping Review. J. Phys. Act. Health 2020, 17, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Gallo, L.A.; Gallo, T.F.; Young, S.L.; Moritz, K.M.; Akison, L.K. The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students. Nutrients 2020, 12, 1865. [Google Scholar] [CrossRef]
- Li, M.; Wang, Q.; Shen, J. The Impact of Physical Activity on Mental Health during COVID-19 Pandemic in China: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6584. [Google Scholar] [CrossRef]
- Savage, M.J.; Hennis, P.J.; Magistro, D.; Donaldson, J.; Healy, L.C.; James, R.M. Nine Months into the COVID-19 Pandemic: A Longitudinal Study Showing Mental Health and Movement Behaviours Are Impaired in UK Students. Int. J. Environ. Res. Public Health 2021, 18, 2930. [Google Scholar] [CrossRef]
- Talapko, J.; Perić, I.; Vulić, P.; Pustijanac, E.; Jukić, M.; Bekić, S.; Meštrović, T.; Škrlec, I. Mental Health and Physical Activity in Health-Related University Students during the COVID-19 Pandemic. Healthcare 2021, 9, 801. [Google Scholar] [CrossRef]
- Ernstsen, L.; Havnen, A. Mental health and sleep disturbances in physically active adults during the COVID-19 lockdown in Norway: Does change in physical activity level matter? Sleep. Med. 2021, 77, 309–312. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P.; American College of Sports, M. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Schober, P.; Mascha, E.J.; Vetter, T.R. Statistics From A (Agreement) to Z (z Score): A Guide to Interpreting Common Measures of Association, Agreement, Diagnostic Accuracy, Effect Size, Heterogeneity, and Reliability in Medical Research. Anesth. Analg. 2021, 133, 1633–1641. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Kiliç, S. Cronbach’s alpha reliability coefficient. Psychiatry Behav. Sci. 2016, 6, 47. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [Green Version]
- Norton, K.; Norton, L.; Sadgrove, D. Position statement on physical activity and exercise intensity terminology. J. Sci. Med. Sport 2010, 13, 496–502. [Google Scholar] [CrossRef]
- Ng, S.W.; Popkin, B.M. Time use and physical activity: A shift away from movement across the globe. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2012, 13, 659–680. [Google Scholar] [CrossRef] [Green Version]
- Bailey, A.P.; Hetrick, S.E.; Rosenbaum, S.; Purcell, R.; Parker, A.G. Treating depression with physical activity in adolescents and young adults: A systematic review and meta-analysis of randomised controlled trials. Psychol. Med. 2018, 48, 1068–1083. [Google Scholar] [CrossRef]
- Wolf, S.; Seiffer, B.; Zeibig, J.M.; Welkerling, J.; Brokmeier, L.; Atrott, B.; Ehring, T.; Schuch, F.B. Is Physical Activity Associated with Less Depression and Anxiety during the COVID-19 Pandemic? A Rapid Systematic Review. Sports Med. 2021, 51, 1771–1783. [Google Scholar] [CrossRef]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef]
- Chtourou, H.; Trabelsi, K.; H’Mida, C.; Boukhris, O.; Glenn, J.M.; Brach, M.; Bentlage, E.; Bott, N.; Shephard, R.J.; Ammar, A.; et al. Staying Physically Active during the Quarantine and Self-Isolation Period for Controlling and Mitigating the COVID-19 Pandemic: A Systematic Overview of the Literature. Front. Psychol. 2020, 11, 1708. [Google Scholar] [CrossRef] [PubMed]
- Marconcin, P.; Werneck, A.O.; Peralta, M.; Ihle, A.; Gouveia, E.R.; Ferrari, G.; Sarmento, H.; Marques, A. The association between physical activity and mental health during the first year of the COVID-19 pandemic: A systematic review. BMC Public Health 2022, 22, 209. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, E.M.; Loukov, D.; Bowdish, D.M.E.; Heisz, J.J. Exercise reduces depression and inflammation but intensity matters. Biol. Psychol. 2018, 133, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Violant-Holz, V.; Gallego-Jiménez, M.G.; González-González, C.S.; Muñoz-Violant, S.; Rodríguez, M.J.; Sansano-Nadal, O.; Guerra-Balic, M. Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9419. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Tucker, L.; Wu, C.; Yang, L. Beneficial Effects of Exercise on Depression and Anxiety during the Covid-19 Pandemic: A Narrative Review. Front. Psychiatry 2020, 11, 587557. [Google Scholar] [CrossRef] [PubMed]
- Nie, Y.; Ma, Y.; Wu, Y.; Li, J.; Liu, T.; Zhang, C.; Lv, C.; Zhu, J. Association Between Physical Exercise and Mental Health during the COVID-19 Outbreak in China: A Nationwide Cross-Sectional Study. Front. Psychiatry 2021, 12, 722448. [Google Scholar] [CrossRef]
- Chang, Y.C.; Lu, M.C.; Hu, I.H.; Wu, W.I.; Hu, S.C. Effects of different amounts of exercise on preventing depressive symptoms in community-dwelling older adults: A prospective cohort study in Taiwan. BMJ Open 2017, 7, e014256. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.; Chi, X.; Liang, K.; Chen, S.T.; Huang, L.; Guo, T.; Jiao, C.; Yu, Q.; Veronese, N.; Soares, F.C.; et al. Moving More and Sitting Less as Healthy Lifestyle Behaviors are Protective Factors for Insomnia, Depression, and Anxiety among Adolescents during the COVID-19 Pandemic. Psychol. Res. Behav. Manag. 2020, 13, 1223–1233. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Quan, X.; Hui, S.S.; Hu, X.; Chan, J.S.M.; Wang, C.; Boyden, S.D.; Sun, L.; Wang, H. Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef] [Green Version]
- Aktug, Z.B.; Demir, N.A. An Exercise Prescription for COVID-19 Pandemic. Pak. J. Med. Sci. 2020, 36, 1732–1736. [Google Scholar] [CrossRef]
- Ai, X.; Yang, J.; Lin, Z.; Wan, X. Mental Health and the Role of Physical Activity during the COVID-19 Pandemic. Front. Psychol. 2021, 12, 759987. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, G.T.A.; Araújo, A.O.; Silva, L.; Linhares, M.; Pereira, L.C.; Lima, M.N.M.; Elsangedy, H.M. Exercise behavior patterns and associations with subjective well-being during the COVID-19 pandemic: A cross-sectional study in Brazil. Eur. J. Integr. Med. 2021, 46, 101374. [Google Scholar] [CrossRef] [PubMed]
- Belcher, B.R.; Zink, J.; Azad, A.; Campbell, C.E.; Chakravartti, S.P.; Herting, M.M. The Roles of Physical Activity, Exercise, and Fitness in Promoting Resilience during Adolescence: Effects on Mental Well-Being and Brain Development. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Santi, G.; di Fronso, S.; Montesano, C.; Di Gruttola, F.; Ciofi, E.G.; Morgilli, L.; Bertollo, M. Athletes and adversities: Athletic identity and emotional regulation in time of COVID-19. Sport Sci. Health 2020, 16, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Callow, D.D.; Arnold-Nedimala, N.A.; Jordan, L.S.; Pena, G.S.; Won, J.; Woodard, J.L.; Smith, J.C. The Mental Health Benefits of Physical Activity in Older Adults Survive the COVID-19 Pandemic. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2020, 28, 1046–1057. [Google Scholar] [CrossRef]
- Moldofsky, H.; Patcai, J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. 2011, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- McMurray, R.; Forsythe, W.; Mar, M.; Hardy, C.J. Exercise intensity-related responses of beta-endorphin and catecholamines. Med. Sci. Sports Exerc. 1987, 19, 570–574. [Google Scholar] [CrossRef]
- Paryab, N.; Taheri, M.; H’Mida, C.; Irandoust, K.; Mirmoezzi, M.; Trabelsi, K.; Ammar, A.; Chtourou, H. Melatonin supplementation improves psychomotor and physical performance in collegiate student-athletes following a sleep deprivation night. Chronobiol. Int. 2021, 38, 753–761. [Google Scholar] [CrossRef]
- Xu, C.; Dong, Y.; Yu, X.; Wang, H.; Tsamlag, L.; Zhang, S.; Chang, R.; Wang, Z.; Yu, Y.; Long, R.; et al. Estimation of reproduction numbers of COVID-19 in typical countries and epidemic trends under different prevention and control scenarios. Front. Med. 2020, 14, 613–622. [Google Scholar] [CrossRef]
- Chang, J.J.; Ji, Y.; Li, Y.H.; Pan, H.F.; Su, P.Y. Prevalence of anxiety symptom and depressive symptom among college students during COVID-19 pandemic: A meta-analysis. J. Affect. Disord. 2021, 292, 242–254. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Studies with Controlled Experimental Groups | 1. Irretrievable literature |
| 2. Studies include measures of depression and anxiety | 2. Repeated research |
| 3. The research object is university students | 3. Review and observational or cross-sectional studies |
| 4. All physical activity interventions are eligible, i.e., “any physical movement produced by skeletal muscle that results in energy expenditure above resting levels” [73] | 4. Report with no valid results |
| 5. Articles published between 1 January 2020 and 4 October 2022 | |
| 6. Experiments conducted during the outbreak of COVID-19 | |
| Trial ID | Country | N | Age Mean (Range) | Gender, % Female | T | C | Recruitment Setting | Depression and Anxiety Inclusion Criteria | Scale Validity Value | Depression and Anxiety Outcome Measures | Research Type |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wang et al., 2021 [58] | China | 200 | 19–21 | 51 | 100 | 100 | College freshman | Depression ≥ 3 | SCL Cronbach’s coefficient α = 0.79~0.99 | SCL-90 | RCT |
| Liu et al., 2020 [59] | China | 192 | NR | 100 | 128 | 64 | Undergraduate | Anxiety Score ≥ 50 Depression Score ≥ 50 | SAS Cronbach’s coefficient α = 0.912 SDS Cronbach’s coefficient α = 0.818 | SAS SDS | RCT |
| Chang et al., 2022 [60] | America | 273 | NR | NR | 114 | 159 | Undergraduate students aged ≥18 attending a 4-year college in the U.S. who did not graduate before May 2020 | NR | PHQ-4 Anxiety Cronbach’s coefficient α = 0.83, Depression = 0.82 PANAS positive Cronbach’s coefficient α = 0.90, negative = 0.87 PSS-10 Cronbach’s coefficient α = 0.89 | PANAS PHQ-4 PSS-10 | RCT |
| Li et al., 2022 [61] | China | 387 | 20–30 | 49.8 | 195 | 192 | 1. Between 20 and 30 years old. 2. Study or work in school for more than two months | NR | CAS Cronbach’s coefficient α = 0.793. PWBS Cronbach’s coefficient α = 0.93 | CAS PWBS | RCT |
| Hamed et al., 2021 [62] | Saudi Arabia | 54 | 18–25 | 70.3 | 27 | 27 | Undergraduate | NR | NR | DASS21 | RCT |
| Chawla et al., 2022 [63] | India | 30 | 23–26 | 70 | 15 | 15 | Undergraduate | Depression > 10 Anxiety > 8 | DASS Anxiety Cronbach’s coefficient α = 0.84 Depression = 0.91 | DASS SF-36 | RCT |
| BarĞi, et al., 2021 [64] | Turkey | 31 | 18–21 | 90.3 | 15 | 16 | 1. Undergraduate 2. aged ≥18 years 3. Having a smartphone or pedometer | Depression > 14 Anxiety > 8 | NR | PA BAI BDI QOL, SF-36 | RCT |
| Philippot, Arnaud, et al., 2022 [65] | Belgium | 28 | 19–25 | 89.2 | 13 | 15 | 1. Undergraduate 2. Between 18 and 25 years old. | GAD-7 ≥ 5 | NR | DASS-21 GAD-7 | RCT |
| Trial ID | Physical Activity Arms and Content | Aerobic/ Resistance | Setting | Duration (Weeks) | Session (Min) | Sessions per Week | Intensity (MET) * | Control Arm |
|---|---|---|---|---|---|---|---|---|
| Wang et al., 2021 [58] | 1. Baduanjin | NR | S Q G | 18 weeks | 90 min | 3 | Mod (3 < 6) | NT |
| Liu et al., 2020 [59] | 1. physical training@ HR (60~69%) 2. Taijiquan | Aerobic | S Q G | 5 weeks | 40 min | 3 | Vig (6 < 9) | Prevented from doing sports |
| Chang et al., 2022 [60] | 1. Yoga Namaskar 2. Nadi Shuddhi | NR | NR NR I | 12 weeks | 40–45 min | 3 | Mod (3 < 6) | WL = 1. complete the weekly surveys 2. At Week 4 learn the same yoga practices |
| Li et al., 2022 [61] | 1. Baduanjin | NR | NR Q I | 12 weeks | 45 min | ≥5 | Mod (3 < 6) | Learning health knowledge |
| Hamed et al., 2021 [62] | 1. treadmill running 2. high-pace stationary cycling 3.weight-bearing aerobic exercises@HR (70% to 90%) | Aerobic | S NR I | 8 weeks | 80 min | 5 | Vig (6 < 9) | CBT |
| Chawla et al., 2022 [63] | Do static and dynamic squats from different angles + WBV (Whole-Body Vibrating Platform) | NR | U NR I | 4 weeks | 30 min | 2 | Vig (6 < 9) | Do static and dynamic squats from different angles |
| BarĞi, et al., 2021 [64] | 1. 5000–10,000 steps/day 2. Doing leisure activities and/or doing housework | Aerobic | S Q I | 4 weeks | 30–60 min | 3 | Mod (3 < 6) | NT |
| Philippot, Arnaud et al., 2022 [65] | HIIT@HRmax (80% < 90%) | Aerobic | S Q I | 4 weeks | ≥10 min | 3 | Vig (6 < 9) | NT |
| _ES | Coef. | Std. Err. | t | p > |t| | [95% Conf. Interval] |
|---|---|---|---|---|---|
| Met | −0.7531876 | 0.3061729 | −2.46 | 0.091 | −1.727567 to 0.2211914 |
| Frequency (week) | −0.0706776 | 0.129785 | −0.54 | 0.624 | −0.4837114 to 0.3423562 |
| Time (min) | −0.1395257 | 0.1319966 | −1.06 | 0.368 | −0.559598 to 0.2805465 |
| Duration (weeks) | 0.2457894 | 0.2962629 | 0.83 | 0.468 | −0.6970513 to 1.18863 |
| _cons | 0.5127189 | 0.8040718 | 0.64 | 0.569 | −2.046196 to 3.071634 |
| _ES | Coef. | Std. Err. | t | p > |t| | [95% Conf. Interval] |
|---|---|---|---|---|---|
| Met | −0.8071271 | 0.4329666 | −1.86 | 0.203 | −2.670032 to 1.055778 |
| Frequency (week) | 0.9779419 | 0.6021712 | 1.62 | 0.246 | −1.612992 to 3.568875 |
| Time (min) | 0.0014643 | 0.2964396 | 0.00 | 0.997 | −1.274012 to 1.276941 |
| Duration (weeks) | 0.0314791 | 0.4857233 | 0.06 | 0.954 | −2.05842 to 2.121378 |
| _cons | −0.6500254 | 1.14621 | −0.57 | 0.628 | −5.581768 to 4.281717 |
| Group | Sub-Group | K | N | SMD | 95% CI | p | I2 |
|---|---|---|---|---|---|---|---|
| Met | 3 < 6 | 5 | 919 | −0.171 | −0.301 to −0.040 | 0.010 | 0.0% |
| 6 < 9 | 3 | 276 | −1.124 | −1.387 to −0.860 | 0.000 | 0.0% | |
| Frequency (week) | <4 | 6 | 754 | −0.473 | −0.907 to −0.038 | 0.033 | 85.1% |
| ≥4 | 2 | 441 | −0.626 | −1.558 to 0.306 | 0.188 | 89.3% | |
| Time (min) | ≤30 | 2 | 58 | −0.598 | −1.127 to −0.070 | 0.027 | 0.0% |
| 30 < 60 | 4 | 883 | −0.401 | −0.914 to 0.112 | 0.126 | 91.3% | |
| ≥60 | 2 | 254 | −0.673 | −1.515 to 0.169 | 0.117 | 85.7% | |
| Duration (weeks) | ≤8 | 5 | 335 | −−0.807 | −1.213 to −0.402 | 0.017 | 57.8% |
| >8 | 3 | 860 | −0.163 | −0.298 to −0.029 | 0.000 | 0.0% |
| Group | Sub-Group | K | N | SMD | 95% CI | p | I2 |
|---|---|---|---|---|---|---|---|
| Met | 3 < 6 | 4 | 532 | −0.419 | −0.592 to −0.246 | 0.000 | 0.0% |
| 6 < 9 | 3 | 276 | −0.859 | −1.634 to −0.085 | 0.030 | 85.0% | |
| Frequency (week) | <4 | 6 | 754 | −0.674 | −1.088 to −0.260 | 0.001 | 83.0% |
| ≥4 | 1 | 54 | −0.273 | −0.809 to 0.263 | 0.319 | 0.0% | |
| Time (min) | ≤30 | 2 | 58 | −0.798 | −1.335 to −0.261 | 0.004 | 0.0% |
| 30 < 60 | 3 | 496 | −0.709 | −1.467 to 0.048 | 0.067 | 91.8% | |
| ≥60 | 2 | 254 | −0.349 | −0.597 to −0.101 | 0.006 | 0.0% | |
| Duration (weeks) | ≤8 | 5 | 335 | −0.716 | −1.286 to −0.145 | 0.014 | 79.1% |
| >8 | 2 | 473 | −0.417 | −0.600 to −0.233 | 0.000 | 0.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, Q.; Zhang, P.; Liu, Y.; Ma, X.; Jennings, G. Intervention of Physical Activity for University Students with Anxiety and Depression during the COVID-19 Pandemic Prevention and Control Period: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15338. https://doi.org/10.3390/ijerph192215338
Luo Q, Zhang P, Liu Y, Ma X, Jennings G. Intervention of Physical Activity for University Students with Anxiety and Depression during the COVID-19 Pandemic Prevention and Control Period: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(22):15338. https://doi.org/10.3390/ijerph192215338
Chicago/Turabian StyleLuo, Qingyuan, Peng Zhang, Yijia Liu, Xiujie Ma, and George Jennings. 2022. "Intervention of Physical Activity for University Students with Anxiety and Depression during the COVID-19 Pandemic Prevention and Control Period: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 22: 15338. https://doi.org/10.3390/ijerph192215338
APA StyleLuo, Q., Zhang, P., Liu, Y., Ma, X., & Jennings, G. (2022). Intervention of Physical Activity for University Students with Anxiety and Depression during the COVID-19 Pandemic Prevention and Control Period: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(22), 15338. https://doi.org/10.3390/ijerph192215338