
Health-Related Quality of Life in Children: The Roles of Age, Gender and Interpersonal Trust

Abstract
:1. Introduction
The Present Study
2. Method
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Health-Related Quality of Life (HRQoL)
2.3.2. Interpersonal Trust
2.4. Data Analyses
3. Results
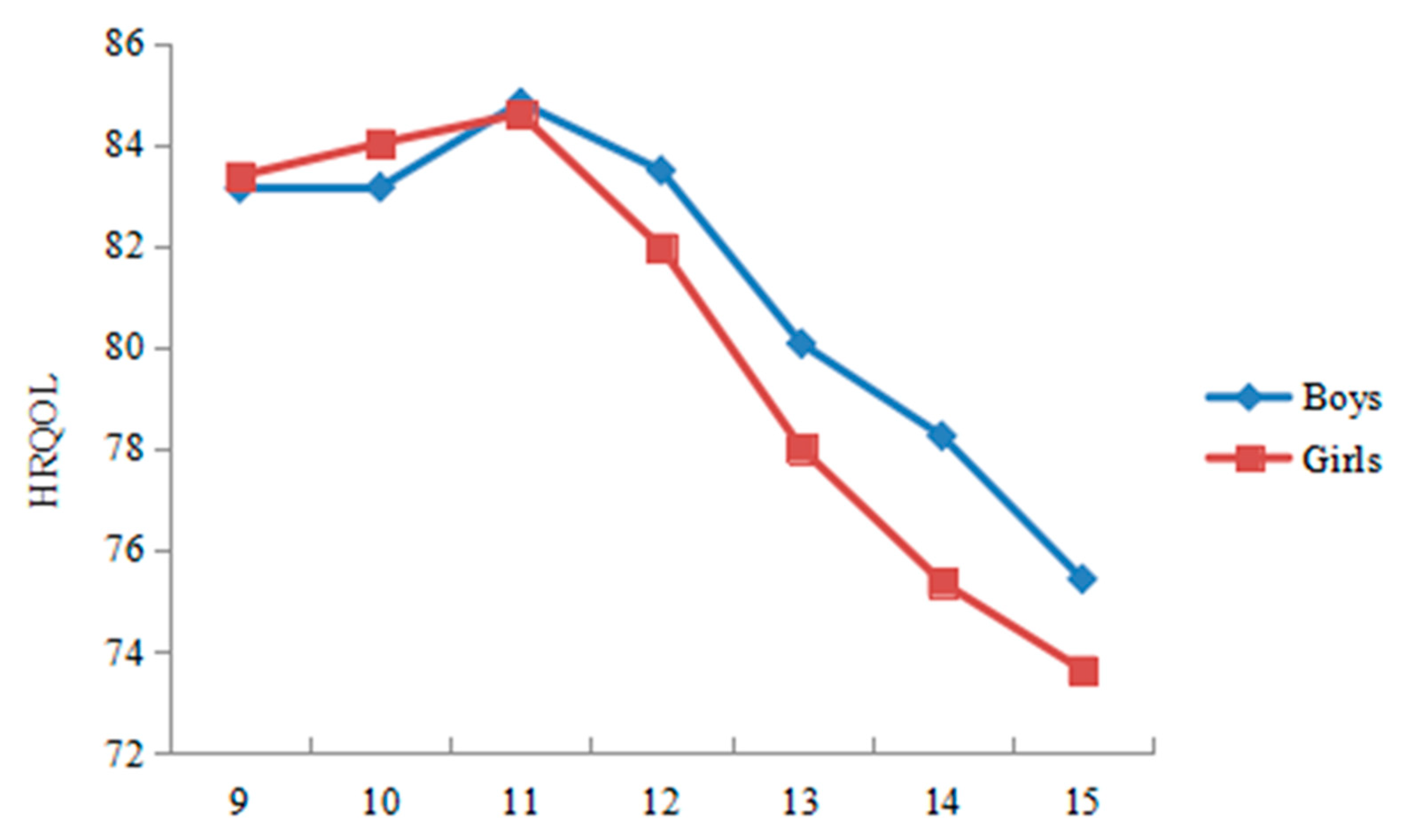
3.1. The Score of HRQoL and Interpersonal Trust following Child Development
3.2. Gender Differences
3.3. Correlations
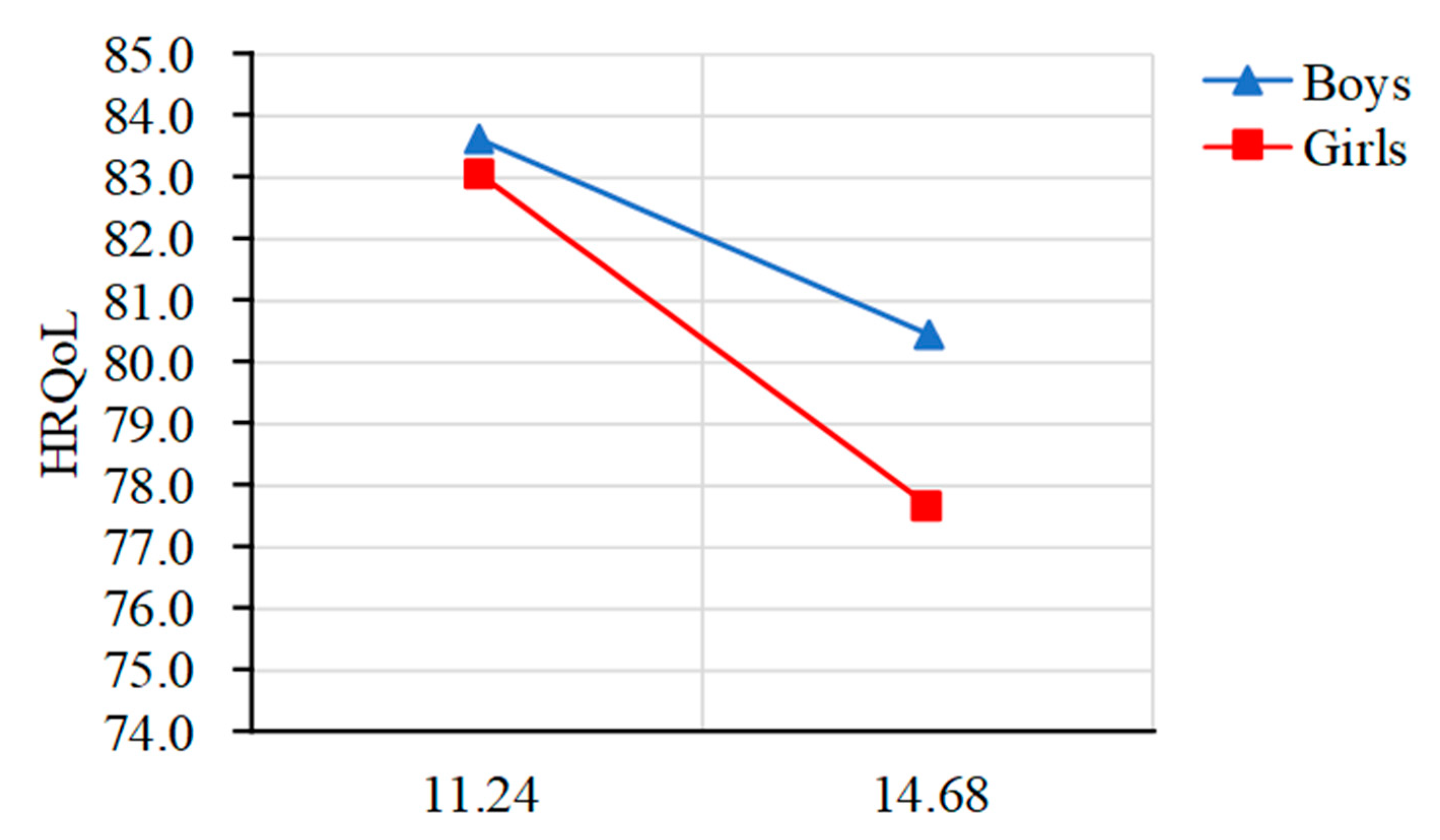
3.4. Moderated Mediation Effect Analyses
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tan, X.D.; Zhang, Y.N.; Shao, H.Y. Healthy China 2030, a breakthrough for improving health. Glob. Health Promot. 2019, 26, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Meade, T.; Dowswell, E. Health-related quality of life in a sample of Australia adolescents: Gender and age comparison. Qual. Life Res. 2015, 24, 2933–2938. [Google Scholar] [CrossRef]
- Michel, G.; Bisegger, C.; Fuhr, D.C.; Abel, T. Age and gender differences in health-related quality of life of children and adolescents in Europe: A multilevel analysis. Qual. Life Res. 2009, 18, 1147–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bevan, J.L.; Gomez, R.; Sparks, L. Disclosures about important life events on Facebook: Relationships with stress and quality of life. Comput. Hum. Behav. 2014, 39, 246–253. [Google Scholar] [CrossRef]
- Evans, D.R. Enhancing Quality of Life in the Population at Large. Soc. Indic. Res. 1994, 33, 47–88. [Google Scholar] [CrossRef]
- European Commission. Report on the State of Young People’s Health in the European Union: A Commission Services Working Paper. Available online: https://ec.europa.eu/health/ph_information/reporting/ke01_en.pdf (accessed on 7 November 2000).
- Eccles, J. The Development of Children Ages 6 to 14. Future Child. 1999, 9, 30–44. [Google Scholar] [CrossRef]
- Bisegger, C.; Cloetta, B.; von Rueden, U.; Abel, T.; Ravens-Sieberer, U. Health-related quality of life: Gender differences in childhood and adolescence. Soz.-Und Prav. 2005, 50, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Simon, A.E.; Chan, K.S.; Forrest, C.B. Assessment of children’s health-related quality of life in the United States with multidimensional index. Pediatrics 2008, 121, 118–126. [Google Scholar] [CrossRef]
- Jalali-Farahani, S.; Amiri, P.; Chin, Y.S. Are physical activity, sedentary behaviors and sleep duration associated with body mass index-for age and health-related quality of life among high school boys and girls? Health Qual. Life Outcomes 2016, 14, 30. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, L.; Morris, A.S. Adolescent development. Annu. Rev. Psychol. 2001, 52, 83–110. [Google Scholar] [CrossRef]
- Dou, D.M. A Study on Children’s Quality of Life in Urban and Country of HENAN. Master’s Thesis, Zhengzhou University, Zhengzhou, China, 2007. (In Chinese). [Google Scholar]
- Li, Y.; Lou, M.Y.; Chen, Q.; Xing, H.Y. Study on the correlation between quality of life and social support among migrant children and the influencing factors. Matern. Child Health Care China 2015, 30, 5027–5029. (In Chinese) [Google Scholar]
- Jiang, X.Y. Linguistic Validation and Measurement Properties of Chinese Version of Youth Quality of Life Instrument (YQOL-R). Master’s Thesis, Zhejiang University, Hangzhou, China, 2014. [Google Scholar]
- Herten, M.H.; Bai, G.N.; Hafkamp, E.; Landgraf, J.M.; Raat, H. Determinants of health-related quality of life in school-aged children: A general population study in Netherlands. PLoS ONE 2015, 10, e0125083. [Google Scholar]
- Jonason, P.K.; Krause, L. The emotional deficits associated with the dark triad traits: Cognitive empathy, affective empathy, and alexithymia. Personal. Individ. Differ. 2013, 55, 532–537. [Google Scholar] [CrossRef]
- Jonason, P.K.; Lyons, M.; Bethell, E.J.; Ross, R. Different routes to limited empathy in the sexes: Examining the links between the dark triad and empathy. Personal. Individ. Differ. 2013, 54, 572–576. [Google Scholar] [CrossRef]
- Wu, X.Y.; Ohinmaa, A.; Veugelers, P.J. Sociodemographic and neighbourhood determinants of health-related quality of life among grade-five students in Canada. Qual. Life Res. 2010, 16, 969–976. [Google Scholar] [CrossRef]
- Liang, Y. Correlations between health-related quality of life and interpersonal trust: Comparisons between two generations of Chinese rural-to-urban migrants. Soc. Indic. Res. 2015, 123, 677–700. [Google Scholar] [CrossRef]
- Tokuda, Y.; Jimba, M.; Yanai, H.; Fujii, S.; Inoguchi, T. Interpersonal trust and quality of life: A cross-sectional study in Japan. PLoS ONE 2008, 3, e3985. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.L.; Li, Y.P.; Tu, Y.D. Linking proactive personality to life satisfaction in the Chinese context: The mediation of interpersonal trust and moderation of positive reciprocity beliefs. J. Happiness Stud. 2019, 20, 2471–2488. [Google Scholar] [CrossRef]
- Jin, X.; Li, Y.M.; Li, X.S.; Yang, L.Q.; Lao, Y.C. Relationship among online social attitude, online trust, interpersonal trust, social anxiety and loneliness (in Chinese). Chin. J. Clin. Psychol. 2017, 25, 185–187. [Google Scholar]
- Phongsavan, P.; Chey, T.; Bauman, A.; Brooks, R.; Silove, D. Social capital, socio-economic status and psychological distress among Australian adults. Soc. Sci. Med. 2006, 63, 2546–2561. [Google Scholar] [CrossRef]
- Pollack Evan, C.; Knesebeck, V.D.; Olaf. Social capital and health among the aged: Comparisons between the United States and Germany. Health Place 2004, 10, 383–391. [Google Scholar] [CrossRef]
- Yu, Z.J.; Xu, L.Z.; Sun, L.; Zhang, J.; Qin, W.Z.; Li, J.J.; Ding, G.; Wang, Q.; Zhu, J.; Xie, X. Association between interpersonal trust and suicidal ideation in older adults: A cross-sectional analysis of 7070 subjects in Shandong, China. BMC Psychiatry 2019, 19, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Z.X.; Vlachantoni, A.; Liu, X.T.; Jones, K. Social trust, interpersonal trust and self-rated health in China: A multi-level study. Int. J. Equity Health 2016, 15, 180. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.P.; Eberly, M.B.; Chiang, T.J.; Farh, J.L.; Cheng, B.S. Affective trust in Chinese leaders: Linking paternalistic leadership to employee performance. J. Manag. 2014, 40, 796–819. [Google Scholar] [CrossRef]
- Pender, N.J.; Murdaugh, C.L.; Parsons, M.A. Health promotion in nursing practice. Nurs. Stand. 2010, 5, 37. [Google Scholar]
- Bradbury-Golas, K. Health promotion and prevention strategies. Nurs. Clin. North Am. 2013, 48, 469–483. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Campbell, R.; Brown, J.; Gainforth, H. ABC of Behaviour Change Theories. Available online: https://silverbackpublishing.org/products/abc-of-behaviour-change-theories (accessed on 2 June 2014).
- Laranjo, L. Chapter 6—Social Media and Health Behavior Change. In Participatory Health through Social Media; Syed-Abdul, S., Gabarron, E., Lau, A.Y.S., Eds.; Academic Press: Cambridge, MA, USA, 2016; pp. 83–111. [Google Scholar]
- Barlett, C.P.; Barlett, N.D. The young and the restless: Examining the relationship between age, emerging adulthood variables, and the dark triad. Personal. Individ. Differ. 2015, 86, 20–24. [Google Scholar] [CrossRef]
- Kavanagh, P.S.; Signal, T.D.; Taylor, N. The dark triad and animal cruelty: Dark personality, dark attitudes, and dark behaviors. Personal. Individ. Differ. 2013, 55, 666–670. [Google Scholar] [CrossRef]
- Carter, G.L.; Campell, A.C.; Muncer, S. The dark triad personality: Attractiveness to women. Personal. Individ. Differ. 2014, 56, 57–61. [Google Scholar] [CrossRef]
- Carter, G.L.; Campell, A.C.; Muncer, S. The dark triad: Beyond a ‘male’ mating stragey. Personal. Individ. Differ. 2014, 56, 159–164. [Google Scholar] [CrossRef]
- Geng, Y.G.; Yang, Z.H.; Zhang, R.X.; Fan, W.J.; Yan, F.Y.; Sai, X.Y.; Liu, Y.N. Relations between Machiavellianism, internalizing and externalizing behavior problems in adolescents: A one-year longitudinal study. Personal. Individ. Differ. 2017, 119, 296–300. [Google Scholar] [CrossRef]
- Sutton, J.; Keogh, E. Components of Machiavellian beliefs in children: Relationships with personality. Personal. Individ. Differ. 2001, 30, 137–148. [Google Scholar] [CrossRef]
- Wu, Y.; Hall, A.; Siehl, S.; Grafman, J.; Krueger, F. Neural signatures of gender differences in interpersonal trust. Front. Hum. Neurosci. 2020, 14, 225. [Google Scholar] [CrossRef]
- Kosfeld, M.; Heinrichs, M.; Zak, P.; Fischbacher, U.; Fehr, E. Oxytocin increases trust in humans. Nature 2005, 435, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.V.; Jackson, E.F. Is trust in others declining in America? An age–period–cohort analysis. Soc. Sci. Res. 2001, 30, 117–145. [Google Scholar] [CrossRef]
- Zhu, X.L.; Wang, F.; Geng, Y.G. Machiavellianism on quality of life: The role of lifestyle, age, gender, social support. Personal. Individ. Differ. 2021, 173, 110609. [Google Scholar] [CrossRef]
- Christie, R.; Geis, F.L. Studies in Machiavellianism; Academic Press: New York, NY, USA, 1970; p. 76. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Gu, H.L.; Fu, D.D.; Lu, X.Y.; Xia, T.S. The relationship between negative life events and non-suicidal self-injury among junior middle school students: Moderated mediation effect (in Chinese). Psychol. Dev. Educ. 2018, 34, 229–238. [Google Scholar]
- Brett, C.E.; Dykiert, D.; Starr, J.M.; Deary, I.J. Predicting change in quality of life from age 79 to in the Lothian Birth Cohort 1921. Qual. Life Res. 2019, 28, 737–749. [Google Scholar] [CrossRef] [Green Version]
- Von Rueden, A.; Gosch, L.R.; Bisegger, C.; Ravens-Sieberer, U. Socioeconomic determinants of health-related quality of life in childhood and adolescence: Results from a European study. J. Epidemiol. Community Health 2006, 60, 130–135. [Google Scholar] [CrossRef]
- Waters, E.; Davis, E.; Nicolas, C.; Wake, M.; Lo, S.K. The impact of childhood conditions and concurrent morbidities on child health and well-being. Child Care Health Dev. 2008, 34, 418–429. [Google Scholar] [CrossRef]
- Poulin, M.J.; Haase, C.M. Growing to trust: Evidence that trust increases and sustains well-being across the life span. Soc. Psychol. Personal. Sci. 2015, 6, 614–621. [Google Scholar] [CrossRef]
- Cherepanov, D. Gender Differences in Health-Related Quality of Life. Ph.D. Thesis, University of Wisconsin–Madison, Madison, WI, USA, 2009. [Google Scholar]
- Eccles, J.S.; Lord, S.; Buchanan, C.M. School transitions in early adolescence: What are we doing to our young people? In Transitions through Adolescence: Interpersonal Domains and Context; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1996; pp. 251–284. [Google Scholar]
- Agnieszka, L.; Katarzyna, T.; Sandra, B. Empathy, resilience, and gratitude—Does gender make a difference? An. De Psicol. 2020, 36, 521–532. [Google Scholar] [CrossRef]
- Layard, R. Happiness: Lessons from a New Science; Penguin Press: New York, NY, USA, 2005; pp. 310–315. [Google Scholar]
- Werner, N.E.; Hill, L.G. Individual and peer group normative beliefs about relational aggression. Child Dev. 2010, 81, 826–836. [Google Scholar] [CrossRef] [PubMed]
- Jonason, P.K.; Icho, A.; Ireland, K. Resources, harshness, and unpredictability: The socioeconomic conditions associated with the dark triad traits. Evol. Psychol. 2016, 14, 1474704915623699. [Google Scholar] [CrossRef] [Green Version]
- Ravens-Sieberer, U.; Gosch, A.; Rajmil, L.; Erhart, M.; Bruil, J.; Power, M.; Duer, W.; Auquier, P.; Cloetta, B.; Czemy, L.; et al. The KIDSCREEN-52 quality of life measure for children and adolescents: Psychometric results from a cross-cultural survey in 13 European countries. Value Health 2008, 11, 645–658. [Google Scholar] [CrossRef]
- Mansour, M.E.; Kogatal, U.; Rose, B.; Ho, M.; Brewer, D.; Roy-Chaudhury, A.; Hornung, R.W.; Wade, T.J.; DeWitt, T.G. Health-related quality of life in urban elementary schoolchildren. Pediatrics 2003, 111, 1372–1381. [Google Scholar] [CrossRef]
- Du, A.Z.; Gu, C.W.; Ding, G.F. A review of significance and methods mediation analysis in psychological researches. Chinese Ment. Health J. 2014, 28, 578–583. (In Chinese) [Google Scholar]
- Gan, Y.Q. The new trend of mediating effect research. Chinese Ment. Health J. 2014, 28, 584–585. (In Chinese) [Google Scholar]
- Allik, J. National differences in personality. Personal. Individ. Differ. 2012, 53, 114–117. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Age | ||
| 9 | 378 | 6.0 |
| 10 | 1036 | 16.6 |
| 11 | 1363 | 21.8 |
| 12 | 1106 | 17.7 |
| 13 | 996 | 15.9 |
| 14 | 852 | 13.6 |
| 15 | 517 | 8.3 |
| Gender | ||
| Male | 2938 | 47.0 |
| Female | 3310 | 53.0 |
| Total | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | t | df | |
| Interpersonal trust | 37.52 | 9.80 | 38.24 | 9.95 | 36.69 | 9.55 | 6.25 ** | 6215.54 |
| HRQoL | 81.24 | 12.32 | 81.75 | 12.17 | 80.70 | 12.45 | 3.24 ** | 6162.01 |
| Physical function | 82.46 | 14.12 | 83.49 | 13.88 | 81.32 | 14.29 | 6.00 ** | 6135.22 |
| Emotional function | 72.81 | 19.79 | 73.72 | 19.35 | 71.82 | 20.21 | 3.76 ** | 6110.26 |
| Social function | 88.46 | 13.92 | 88.04 | 14.12 | 88.92 | 13.69 | −2.47 * | 6246.00 |
| School function | 79.72 | 15.10 | 79.64 | 15.25 | 79.79 | 14.93 | −0.38 | 6246.00 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1 Age | 1 | |||||||
| 2 Gender | −0.02 | 1 | ||||||
| 3 Interpersonal trust | 0.25 ** | −0.08 ** | 1 | |||||
| 4 HRQoL | −0.24 ** | −0.04 ** | −0.33 ** | 1 | ||||
| 5 Physical function | −0.14 ** | −0.08 ** | −0.24 ** | 0.85 ** | 1 | |||
| 6 Emotional function | −0.22 ** | −0.05 ** | −0.27 ** | 0.81 ** | 0.54 ** | 1 | ||
| 7 Social function | −0.14 ** | 0.03 * | −0.26 ** | 0.74 ** | 0.51 ** | 0.50 ** | 1 | |
| 8 School function | −0.27 ** | 0.01 | −0.28 ** | 0.75 ** | 0.51 ** | 0.49 ** | 0.46 ** | 1 |
| Variables | Interpersonal Trust | 95% CI | HRQoL | 95% CI |
|---|---|---|---|---|
| Age | 0.26 ** | 0.23, 0.28 | −0.17 ** | −0.20, −0.15 |
| Gender | −0.08 ** | −0.10, −0.05 | −0.07 * | 0.05, 0.09 |
| Interpersonal trust | −0.29 ** | −0.31, −0.26 | ||
| Age × Gender | −0.03 * | −0.06, −0.01 | −0.05 ** | −0.07, −0.02 |
| Interpersonal trust × Gender | 0.02 | −0.04, 0.06 | ||
| R2 | 0.07 | 0.14 | ||
| F | 151.00 ** | 192.21 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Jin, W.; Shi, L.; Geng, Y.; Zhu, X.; Hu, W. Health-Related Quality of Life in Children: The Roles of Age, Gender and Interpersonal Trust. Int. J. Environ. Res. Public Health 2022, 19, 15408. https://doi.org/10.3390/ijerph192215408
Wang J, Jin W, Shi L, Geng Y, Zhu X, Hu W. Health-Related Quality of Life in Children: The Roles of Age, Gender and Interpersonal Trust. International Journal of Environmental Research and Public Health. 2022; 19(22):15408. https://doi.org/10.3390/ijerph192215408
Chicago/Turabian StyleWang, Jing, Wenjing Jin, Liping Shi, Yaoguo Geng, Xueli Zhu, and Wanying Hu. 2022. "Health-Related Quality of Life in Children: The Roles of Age, Gender and Interpersonal Trust" International Journal of Environmental Research and Public Health 19, no. 22: 15408. https://doi.org/10.3390/ijerph192215408
APA StyleWang, J., Jin, W., Shi, L., Geng, Y., Zhu, X., & Hu, W. (2022). Health-Related Quality of Life in Children: The Roles of Age, Gender and Interpersonal Trust. International Journal of Environmental Research and Public Health, 19(22), 15408. https://doi.org/10.3390/ijerph192215408