
Sleep Problems and New Occurrence of Chronic Conditions during the COVID-19 Pandemic in the UK


Abstract
:1. Introduction
2. Materials and Methods
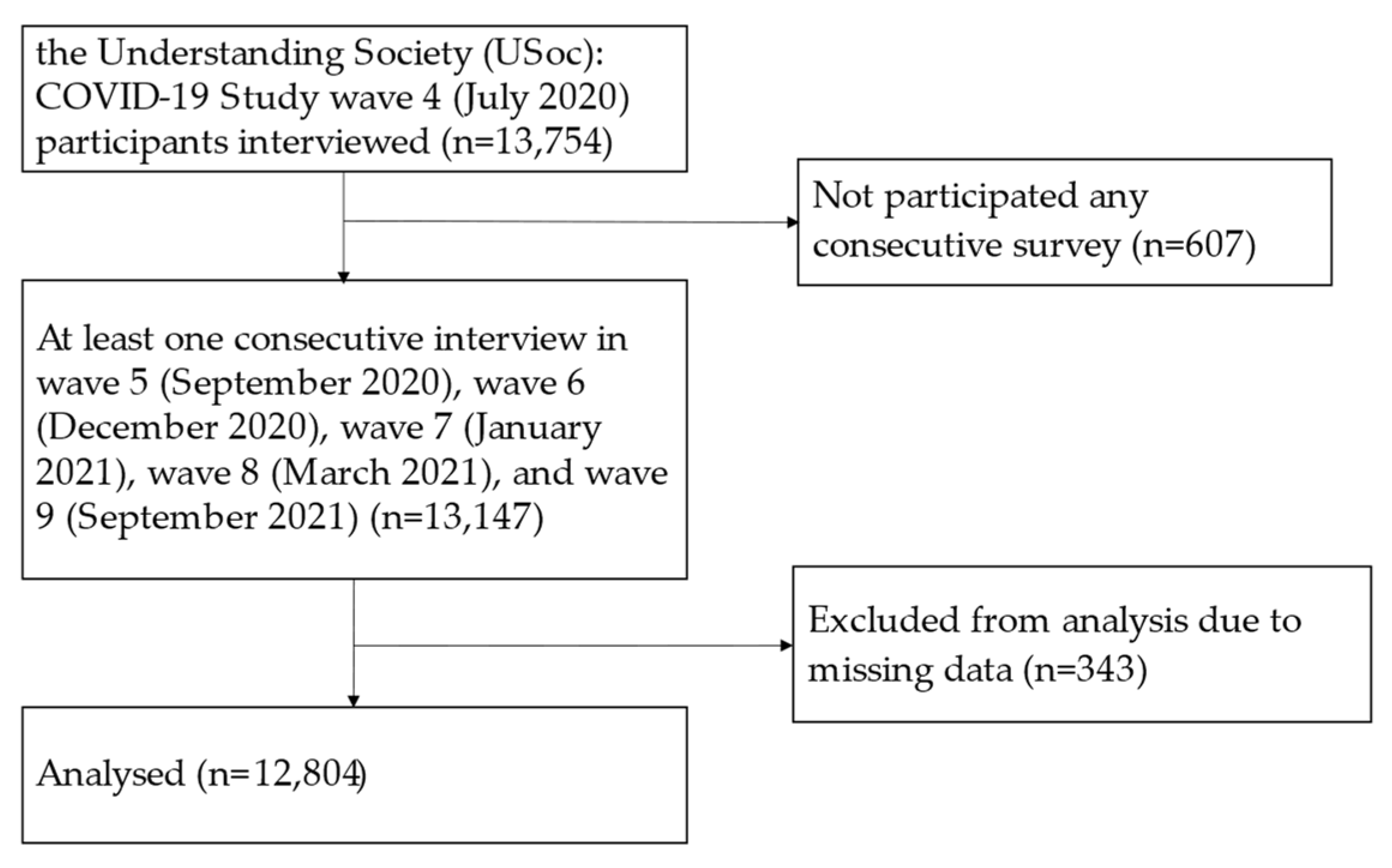
2.1. Study Design and Setting
2.2. Participants
2.3. Measures
2.3.1. Sleep Problems
- Not during the past month
- Less than once a week
- Once or twice a week
- Three or more times a week
- More than once most nights
- Not during the past month
- Less than once a week
- Once or twice a week
- Three or more times a week
- More than once most nights
- Not during the past month
- Less than once a week
- Once or twice a week
- Three or more times a week
- More than once most nights
- Not during the past month
- Less than once a week
- Once or twice a week
- Three or more times a week
- Not during the past month
- Less than once a week
- Once or twice a week
- Three or more times a week
- Very good
- Fairly good
- Fairly bad
- Very bad
2.3.2. Disease Incidence
2.3.3. Control Variables
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics and Bivariate Analysis Results
3.2. Logistic Regressions Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


{kind=link}
| CVD | Hypertension | Diabetes | Obesity | Arthritis | An Emotional, Nervous or Psychiatric Problem | |
|---|---|---|---|---|---|---|
| Sleep problems | p = 0.185 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| Good sleeper | 0.5 | 1.2 | 0.4 | 0.7 | 1.4 | 0.6 |
| Moderate sleep problems | 0.7 | 2.2 | 0.6 | 1.2 | 2.4 | 1.2 |
| Severe sleep problems | 1.2 | 3.2 | 1.5 | 2.1 | 3.8 | 4.1 |
| Age | p < 0.001 | p < 0.001 | p = 0.004 | p = 0.032 | p < 0.001 | p = 0.107 |
| 16–24 | 0.1 | - | - | 0.3 | 0.4 | 1.2 |
| 25–44 | 0.1 | 0.6 | 0.2 | 1.2 | 0.4 | 1.3 |
| 45–64 | 0.5 | 1.8 | 0.7 | 1.1 | 1.7 | 1.2 |
| 65–79 | 1.2 | 3.5 | 0.8 | 1.0 | 4.2 | 0.7 |
| 80+ | 4.4 | 2.9 | 1.2 | - | 6.7 | 0.3 |
| Gender | p = 0.003 | p = 0.941 | p = 0.970 | p = 0.008 | p = 0.123 | p = 0.156 |
| Men | 0.9 | 1.7 | 0.5 | 0.7 | 1.6 | 0.9 |
| Women | 0.4 | 1.7 | 0.6 | 1.2 | 2.2 | 1.2 |
| Ethnicity | p = 0.066 | p = 0.525 | p = 0.781 | p = 0.571 | p = 0.133 | p = 0.467 |
| British white | 0.7 | 1.7 | 0.6 | 1.0 | 2.0 | 1.1 |
| Other white | 0.6 | 1.7 | 0.4 | 1.1 | 2.7 | 0.6 |
| BAME | 0.1 | 1.7 | 0.6 | 1.2 | 1.3 | 0.8 |
| Education | p = 0.707 | p = 0.052 | p = 0.006 | p = 0.356 | p = 0.001 | p = 0.978 |
| No qualification | 0.6 | 2.1 | 0.6 | 0.9 | 2.9 | 1.0 |
| GCSE | 0.6 | 2.3 | 1.0 | 1.1 | 2.6 | 1.1 |
| A level | 0.7 | 1.8 | 0.4 | 1.3 | 2.2 | 1.0 |
| Degree or above | 0.7 | 1.4 | 0.4 | 0.9 | 1.6 | 1.1 |
| NS-SEC | p = 0.014 | p < 0.001 | p = 0.004 | p = 0.336 | p < 0.001 | p = 0.076 |
| Professional | 0.4 | 1.0 | 0.3 | 0.9 | 1.1 | 0.7 |
| Intermediate | 0.6 | 1.3 | 0.3 | 1.4 | 1.4 | 1.3 |
| Routine | 0.5 | 1.2 | 0.4 | 0.9 | 1.6 | 1.0 |
| Not working | 0.9 | 2.6 | 0.8 | 1.0 | 3.1 | 1.2 |
| Perceived current financial difficulty | p = 0.037 | p = 0.506 | p < 0.001 | p < 0.001 | p = 0.158 | p < 0.001 |
| Living comfortably | 1.0 | 1.6 | 0.4 | 0.6 | 1.9 | 0.6 |
| Doing all right | 0.5 | 1.6 | 0.4 | 0.8 | 1.8 | 0.9 |
| Just getting by | 0.6 | 2.0 | 1.1 | 1.8 | 2.5 | 1.9 |
| Difficulty or very difficult | 0.4 | 2.4 | 1.6 | 2.9 | 2.6 | 3.5 |
| Perceived future financial difficulty | p = 0.491 | p = 0.294 | p = 0.203 | p = 0.526 | p = 0.030 | p = 0.010 |
| No change | 0.7 | 1.8 | 0.5 | 1.0 | 2.0 | 1.0 |
| Better off | 0.4 | 1.0 | 0.5 | 1.0 | 0.9 | 1.1 |
| Getting worse | 0.8 | 1.4 | 1.0 | 0.9 | 2.4 | 2.1 |
| Living with a partner | p = 0.569 | p = 0.337 | p = 0.411 | p = 0.331 | p = 0.049 | p = 0.182 |
| No | 0.6 | 1.8 | 0.5 | 0.9 | 1.8 | 1.0 |
| Yes | 0.7 | 1.5 | 0.6 | 1.1 | 2.3 | 1.3 |
| Dependent child under 16 in the household | p < 0.001 | p < 0.001 | p = 0.555 | p = 0.980 | p < 0.001 | p = 0.467 |
| No | 0.8 | 2.0 | 0.6 | 1.0 | 2.4 | 1.0 |
| Yes | 0.1 | 0.8 | 0.5 | 1.0 | 0.6 | 1.2 |
| COVID-19 symptoms | p = 0.798 | p = 0.303 | p = 0.721 | p = 0.755 | p = 0.871 | p = 0.104 |
| No | 0.6 | 1.7 | 0.6 | 1.0 | 1.9 | 1.1 |
| Yes | 0.8 | 2.5 | 0.4 | 1.2 | 2.1 | - |
| Baseline other chronic diseases | p < 0.001 | p < 0.001 | p = 0.002 | p < 0.001 | p < 0.001 | p = 0.015 |
| No | 0.2 | 1.0 | 0.4 | 0.6 | 0.9 | 0.8 |
| Yes | 0.8 | 2.7 | 0.8 | 1.4 | 3.3 | 1.3 |
| Total n who clears of baseline study disease | 12,123 | 10,420 | 11,895 | 12,229 | 11,085 | 12,052 |
| Study disease newly diagnosed n | 78 | 176 | 66 | 121 | 216 | 129 |
| % study disease incidence | 0.7 | 1.7 | 0.6 | 1.0 | 1.9 | 1.1 |
| Incidents of Chronic Disease | Total n | Sleep Problems | ||
|---|---|---|---|---|
| Good Sleeper | Moderate Sleep Problems | Severe Sleep Problems | ||
| CVD (n = 77) | 11,908 | |||
| Model 1 | 1.00 | 1.45 (0.90–2.35) | 2.42 * (1.19–4.92) | |
| Model 2 | 1.00 | 1.73 * (1.06–2.81) | 3.13 ** (1.52–6.47) | |
| Model 3 | 1.00 | 1.58 (0.97–2.58) | 2.74 * (1.30–5.78) | |
| Hypertension (n = 173) | 10,226 | |||
| Model 1 | 1.00 | 1.92 *** (1.39–2.66) | 2.92 *** (1.79–4.77) | |
| Model 2 | 1.00 | 2.02 *** (1.45–2.81) | 3.15 *** (1.91–5.20) | |
| Model 3 | 1.00 | 1.91 *** (1.37–2.66) | 2.61 *** (1.55–4.40) | |
| Diabetes (n = 66) | 11,682 | |||
| Model 1 | 1.00 | 1.54 (0.90–2.63) | 3.87 ***(1.94–7.71) | |
| Model 2 | 1.00 | 1.58 (0.92–2.71) | 3.95 *** (1.97–7.95) | |
| Model 3 | 1.00 | 1.41 (0.81–2.43) | 2.72 ** (1.29–5.73) | |
| Obesity (n = 118) | 12,008 | |||
| Model 1 | 1.00 | 1.89** (1.27–2.80) | 3.35 *** (1.90–5.89) | |
| Model 2 | 1.00 | 1.79** (1.20–2.67) | 3.08 *** (1.74–5.44) | |
| Model 3 | 1.00 | 1.63* (1.09–2.43) | 2.21 * (1.21–4.04) | |
| Arthritis (n = 212) | 10,881 | |||
| Model 1 | 1.00 | 1.73 *** (1.30–2.32) | 2.84 *** (1.81–4.46) | |
| Model 2 | 1.00 | 1.79 *** (1.33–2.41) | 3.14 *** (1.97–4.99) | |
| Model 3 | 1.00 | 1.64 *** (1.22–2.21) | 2.47 *** (1.53–3.99) | |
| An emotional, nervous or psychiatric problem (n = 125) | 11,832 | |||
| Model 1 | 1.00 | 1.96 *** (1.30–2.94) | 6.67 *** (4.12–10.79) | |
| Model 2 | 1.00 | 1.93 *** (1.28–2.90) | 6.69 *** (4.11–10.89) | |
| Model 3 | 1.00 | 1.76 ** (1.17–2.67) | 4.92 *** (2.93–8.25) | |
| Incidents of Chronic Disease | Total n | Sleep Problems | |
|---|---|---|---|
| Good Sleeper | Poor Sleep Quality | ||
| CVD (n = 77) | 12,123 | ||
| Model 1 | 1.00 | 1.56 * (0.99–2.45) | |
| Model 2 | 1.00 | 1.90 ** (1.20–3.00) | |
| Model 3 | 1.00 | 1.72 * (1.08–2.74) | |
| Hypertension (n = 173) | 10,420 | ||
| Model 1 | 1.00 | 2.03 *** (1.50–2.76) | |
| Model 2 | 1.00 | 2.15 *** (1.57–2.94) | |
| Model 3 | 1.00 | 1.99 *** (1.45–2.73) | |
| Diabetes (n = 66) | 11,895 | ||
| Model 1 | 1.00 | 1.89 * (1.15–3.11) | |
| Model 2 | 1.00 | 1.94 ** (1.18–3.21) | |
| Model 3 | 1.00 | 1.63 (0.97–2.73) | |
| Obesity (n = 118) | 12,229 | ||
| Model 1 | 1.00 | 2.05 *** (1.42–2.96) | |
| Model 2 | 1.00 | 1.93 *** (1.33–2.79) | |
| Model 3 | 1.00 | 1.68 ** (1.15–2.46) | |
| Arthritis (n = 212) | 11,085 | ||
| Model 1 | 1.00 | 1.88 *** (1.43–2.47) | |
| Model 2 | 1.00 | 1.97 *** (1.49–2.60) | |
| Model 3 | 1.00 | 1.77 *** (1.33–2.35) | |
| An emotional, nervous or psychiatric problem (n = 125) | 12,052 | ||
| Model 1 | 1.00 | 2.64 *** (1.82–3.82) | |
| Model 2 | 1.00 | 2.59 *** (1.78–3.75) | |
| Model 3 | 1.00 | 2.24 *** (1.53–3.28) | |
References
- Alimoradi, Z.; Broström, A.; Tsang, H.W.; Griffiths, M.D.; Haghayegh, S.; Ohayon, M.M.; Lin, C.-Y.; Pakpour, A.H. Sleep problems during COVID-19 pandemic and its’ association to psychological distress: A systematic review and meta-analysis. eClinicalMedicine 2021, 36, 100916. [Google Scholar] [CrossRef]
- BBC News. Coronavirus: How the UK is Sleeping under Lockdown. 2021. Available online: https://www.bbc.co.uk/news/health-52911395 (accessed on 15 June 2020).
- Falkingham, J.C.; Evandrou, M.; Qin, M.; Vlachantoni, A. Prospective longitudinal study of ‘Sleepless in Lockdown’: Unpacking differences in sleep loss during the coronavirus pandemic in the UK. BMJ Open 2022, 12, e053094. [Google Scholar] [CrossRef] [PubMed]
- Perlis, M.; Shaw, P.J.; Cano, G.; Espie, C.A. Models of insomnia. In Principles and Practice of Sleep Medicine: Fifth Edition; Kryger, M.H., Roth, T., Dement, W.C., Eds.; Elsevier Inc.: Philadelphia, PA, USA, 2010; pp. 850–865. [Google Scholar]
- Morin, C.M.; Benca, R. Chronic insomnia. Lancet 2012, 379, 1129–1141. [Google Scholar] [CrossRef] [PubMed]
- Medic, G.; Wille, M.; Hemels, M.E. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 2017, 151–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javaheri, S.; Redline, S. Insomnia and Risk of Cardiovascular Disease. Chest 2017, 152, 435–444. [Google Scholar] [CrossRef]
- Jarrin, D.C.; Alvaro, P.K.; Bouchard, M.-A.; Jarrin, S.D.; Drake, C.; Morin, C.M. Insomnia and hypertension: A systematic review. Sleep Med. Rev. 2018, 41, 3–38. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, E.S.; Smith, N.X.; Nichols, G.A.; Allison, M.J.; Clarke, G.N. Insomnia is associated with an increased risk of type 2 diabetes in the clinical setting. BMJ Open Diab. Res. Care 2018, 6, e000604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antza, C.; Kostopoulos, G.; Mostafa, S.; Nirantharakumar, K.; Tahrani, A. The links between sleep duration, obesity and type 2 diabetes mellitus. J. Endocrinol. 2021, 252, 125–141. [Google Scholar] [CrossRef]
- Gao, R.-C.; Sang, N.; Jia, C.-Z.; Zhang, M.-Y.; Li, B.-H.; Wei, M.; Wu, G.-C. Association Between Sleep Traits and Rheumatoid Arthritis: A Mendelian Randomization Study. Front. Public Health 2022, 10, 940161. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wu, C.; Gan, Y.; Qu, X.; Lu, Z. Insomnia and the risk of depression: A meta-analysis of prospective cohort studies. BMC Psychiatry 2016, 16, 375. [Google Scholar] [CrossRef]
- University of Essex, Institute for Social and Economic Research. Understanding Society: COVID-19 Study, 2020–2021, 11th ed.; Data collection; UK Data Service: Colchester, UK, 2021. [Google Scholar]
- Institute for Social and Economic Research. Understanding Society COVID-19 User Guide; Version 10.0; University of Essex: Colchester, UK, 2021. [Google Scholar]
- StataCorp. Stata Multiple Imputation Reference Manual Release Statistical Software; StataCorp LLC: College Station, TX, USA, 2021. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef] [PubMed]
- Backhausa, J.; Junghannsa, K.; Broocksa, A.; Riemannb, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Famodu, O.A.; Barr, M.L.; Holásková, I.; Zhou, W.; Morrell, J.S.; Colby, S.E.; Olfert, M.D. Shortening of the Pittsburgh Sleep Quality Index survey using factor analysis. Sleep Disord. 2018, 2018, 9643937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sancho-Domingo, C.; Carballo, J.L.; Coloma-Carmona, A.; Buysse, D.J. Brief version of the Pittsburgh Sleep Quality Index (B-PSQI) and measurement invariance across gender and age in a population-based sample. Psychol. Assess. 2021, 33, 111–121. [Google Scholar] [CrossRef]
- Morin, C.M.; Be’langer, L.; LeBlanc, M.; Ivers, H.; Savard, J.; Espie, C.A.; Me’rette, C.; Baillargeon, L.; Gre’goire, J. The natural history of insomnia. A population-based 3-year longitudinal study. Arch. Intern. Med. 2009, 169, 447–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.-C.; Hsu, N.-W.; Chou, P. Subgrouping Poor Sleep Quality in Community-Dwelling Older Adults with Latent Class Analysis—The Yilan Study, Taiwan. Sci. Rep. 2020, 10, 5432. [Google Scholar] [CrossRef] [Green Version]
- Cockerham, W.C.; Hamby, B.W.; Oates, G.R. The Social Determinants of Chronic Disease. Am. J. Prev. Med. 2017, 52, S5–S12. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M.; Bell, R. Social determinants and non-communicable diseases: Time for integrated action. Bmj 2019, 364, l251. [Google Scholar] [CrossRef]
- National Health Service (NHS). Insomnia. 2021. Available online: https://www.nhs.uk/conditions/insomnia/ (accessed on 15 September 2022).
- Lehmann, M.; Bruenahl, C.A.; Löwe, B.; Addo, M.M.; Schmiedel, S.; Lohse, A.W.; Schramm, C. Ebola and Psychological Stress of Health Care Professionals. Emerg. Infect. Dis. 2015, 21, 913. [Google Scholar] [CrossRef] [PubMed]
- Levin, J. Mental health care for survivors and healthcare workers in the aftermath of an outbreak. In Psychiatry of Pandemics; Huremovic, D., Ed.; Springer Nature: Switzerland, Switzerland, 2019; pp. 127–141. [Google Scholar]
- Sosso, F.A.E.; Kreidlmayer, M.; Pearson, D.; Bendaoud, I. Towards A Socioeconomic Model of Sleep Health among the Canadian Population: A Systematic Review of the Relationship between Age, Income, Employment, Education, Social Class, Socioeconomic Status and Sleep Disparities. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1143–1167. [Google Scholar] [CrossRef]
- Jean-Louis, G.; Grandner, M.A.; Seixas, A.A. Social determinants and health disparities affecting sleep. Lancet Neurol. 2022, 21, 864–865. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Broström, A.; Griffiths, M.D.; Pakpour, A.H. Investigating mediated effects of fear of COVID-19 and COVID-19 misunderstanding in the association between problematic social media use, psychological distress, and insomnia. Internet Interv. 2020, 21, 100345. [Google Scholar] [CrossRef]
- Perlis, M.L.; Posner, D.; Riemann, D.; Bastien, C.H.; Teel, J.; Thase, M. Insomnia. Lancet 2022, 400, 10357. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Social Care (DHSC); Office for National Statistics (ONS). Direct and Indirect Health Impacts of COVID-19 in England. 2021. Available online: https://www.gov.uk/government/publications/dhsc-direct-and-indirect-health-impacts-of-covid-19-in-england-long-paper-9-september-2021 (accessed on 12 November 2022).
| Row % of Sleep Problems | p Value | % Among All Respondents | |||
|---|---|---|---|---|---|
| Good Sleeper | Moderate Sleep Problems | Severe Sleep Problems | |||
| Total | 52.8 (6948) | 39.1 (4950) | 8.1 (906) | 100.0 (12,804) | |
| Mean age | 48.5 | 49.2 | 50.1 | 0.022 | 48.9 years |
| Age group | <0.001 | ||||
| 16–24 | 60.2 | 35.0 | 4.7 | 12.7 | |
| 25–44 | 51.1 | 40.5 | 8.4 | 28.4 | |
| 45–64 | 50.4 | 40.1 | 9.5 | 35.9 | |
| 65–79 | 54.3 | 38.7 | 7.0 | 18.9 | |
| 80+ | 55.7 | 36.3 | 8.0 | 4.1 | |
| Gender | <0.001 | ||||
| Men | 59.2 | 34.8 | 6.0 | 47.0 | |
| Women | 47.1 | 43.0 | 9.9 | 52.9 | |
| Ethnicity | <0.001 | ||||
| British white | 52.4 | 39.8 | 7.8 | 86.3 | |
| Other white | 52.9 | 37.2 | 9.9 | 3.4 | |
| BAME | 54.4 | 35.6 | 10.0 | 7.8 | |
| Education | <0.001 | ||||
| No qualification | 39.2 | 44.5 | 16.3 | 6.7 | |
| GCSE | 50.4 | 41.5 | 8.1 | 28.4 | |
| A level | 53.0 | 38.6 | 8.3 | 21.0 | |
| Degree or above | 56.2 | 37.1 | 6.7 | 38.6 | |
| NS-SEC | <0.001 | ||||
| Professional | 56.4 | 38.7 | 5.0 | 23.3 | |
| Intermediate | 56.0 | 38.5 | 5.5 | 12.1 | |
| Routine | 50.7 | 41.4 | 7.9 | 18.5 | |
| Not working | 50.2 | 38.9 | 10.9 | 40.7 | |
| Perceived current financial difficulty | <0.001 | ||||
| Living comfortably | 63.4 | 31.7 | 4.9 | 26.5 | |
| Doing all right | 55.5 | 39.5 | 5.0 | 46.3 | |
| Just getting by | 39.3 | 47.3 | 13.4 | 19.1 | |
| Difficulty or very difficult | 15.7 | 54.5 | 29.8 | 6.2 | |
| Perceived future financial difficulty | <0.001 | ||||
| No change | 53.7 | 38.9 | 7.4 | 79.1 | |
| Better off | 55.3 | 39.7 | 5.0 | 9.0 | |
| Getting worse | 36.1 | 47.1 | 16.8 | 10.0 | |
| Living with a partner | <0.001 | ||||
| No | 50.2 | 38.1 | 11.7 | 40.2 | |
| Yes | 54.5 | 39.9 | 5.6 | 59.8 | |
| Dependent child under 16 in the household | <0.001 | ||||
| No | 53.3 | 38.2 | 8.5 | 78.1 | |
| Yes | 50.9 | 42.6 | 6.5 | 21.9 | |
| COVID-19 symptoms | <0.001 | ||||
| No | 53.2 | 38.9 | 7.9 | 97.8 | |
| Yes | 37.1 | 49.3 | 13.6 | 2.2 | |
| Baseline chronic disease | |||||
| CVD | 48.7 | 35.9 | 15.4 | <0.001 | 5.6 |
| Without CVD | 53.1 | 39.3 | 7.6 | 94.4 | |
| Hypertension | 46.9 | 42.2 | 10.9 | <0.001 | 16.0 |
| Without Hypertension | 53.9 | 38.6 | 7.5 | 84.0 | |
| Diabetes | 43.2 | 39.8 | 17.0 | <0.001 | 6.9 |
| Without Diabetes | 53.5 | 39.1 | 7.4 | 93.1 | |
| Obesity | 28.7 | 51.4 | 19.9 | <0.001 | 4.5 |
| Without Obesity | 53.9 | 38.6 | 7.5 | 95.5 | |
| Arthritis | 38.4 | 45.1 | 16.4 | <0.001 | 12.0 |
| Without Arthritis | 54.8 | 38.3 | 6.9 | 88.0 | |
| An emotional, nervous or psychiatric problem | 33.2 | 41.8 | 25.0 | <0.001 | 6.2 |
| Without An emotional, nervous or psychiatric problem | 54.1 | 39.0 | 6.9 | 93.8 | |
| Incidents of Chronic Disease | Total n | Sleep Problems | ||
|---|---|---|---|---|
| Good Sleeper | Moderate Sleep Problems | Severe Sleep Problems | ||
| CVD (n = 78) | 12,123 | |||
| Model 1 | 1.00 | 1.41 (0.87–2.27) (p = 0.159) | 2.34 (1.15–4.75) (p = 0.019) | |
| Model 2 | 1.00 | 1.68 (1.04–2.73) (p = 0.035) | 3.01 (1.46–6.20) (p = 0.003) | |
| Model 3 | 1.00 | 1.54 (0.95–2.51) (p = 0.083) | 2.64 (1.25–5.54) (p = 0.011) | |
| Hypertension (n = 176) | 10,420 | |||
| Model 1 | 1.00 | 1.88 (1.37–2.60) (p < 0.001) | 2.81 (1.73–4.58) (p < 0.001) | |
| Model 2 | 1.00 | 1.99 (1.43–2.75) (p < 0.001) | 3.01 (1.83–4.95) (p < 0.001) | |
| Model 3 | 1.00 | 1.88 (1.35–2.61) (p < 0.001) | 2.54 (1.51–4.26) (p < 0.001) | |
| Diabetes (n = 66) | 11,895 | |||
| Model 1 | 1.00 | 1.54 (0.90–2.63) (p = 0.115) | 3.86 (1.94–7.67) (p < 0.001) | |
| Model 2 | 1.00 | 1.58 (0.92–2.71) (p = 0.096) | 3.94 (1.96–7.91) (p < 0.001) | |
| Model 3 | 1.00 | 1.41 (0.82–2.44) (p = 0.219) | 2.72 (1.29–5.72) (p = 0.009) | |
| Obesity (n = 121) | 12,229 | |||
| Model 1 | 1.00 | 1.83 (1.24–2.70) (p = 0.002) | 3.19 (1.82–5.59) (p < 0.001) | |
| Model 2 | 1.00 | 1.73 (1.17–2.56) (p = 0.006) | 2.92 (1.66–5.14) (p < 0.001) | |
| Model 3 | 1.00 | 1.58 (1.06–2.35) (p = 0.023) | 2.13 (1.08–3.61) (p = 0.014) | |
| Arthritis (n = 216) | 11,085 | |||
| Model 1 | 1.00 | 1.73 (1.30–2.30) (p < 0.001) | 2.76 (1.76–4.33) (p < 0.001) | |
| Model 2 | 1.00 | 1.79 (1.34–2.40) (p < 0.001) | 3.07 (1.93–4.87) (p < 0.001) | |
| Model 3 | 1.00 | 1.65 (1.23–2.21) (p = 0.001) | 2.42 (1.50–3.91) (p < 0.001) | |
| An emotional, nervous or psychiatric problem (n = 129) | 12,052 | |||
| Model 1 | 1.00 | 1.98 (1.33–2.95) (p < 0.001) | 6.69 (4.16–10.76) (p < 0.001) | |
| Model 2 | 1.00 | 1.94 (1.30–2.91) (p < 0.001) | 6.69 (4.14–10.82) (p < 0.001) | |
| Model 3 | 1.00 | 1.79 (1.19–2.69) (p = 0.005) | 5.01 (3.02–8.34) (p < 0.001) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falkingham, J.; Evandrou, M.; Vlachantoni, A.; Qin, M. Sleep Problems and New Occurrence of Chronic Conditions during the COVID-19 Pandemic in the UK. Int. J. Environ. Res. Public Health 2022, 19, 15664. https://doi.org/10.3390/ijerph192315664
Falkingham J, Evandrou M, Vlachantoni A, Qin M. Sleep Problems and New Occurrence of Chronic Conditions during the COVID-19 Pandemic in the UK. International Journal of Environmental Research and Public Health. 2022; 19(23):15664. https://doi.org/10.3390/ijerph192315664
Chicago/Turabian StyleFalkingham, Jane, Maria Evandrou, Athina Vlachantoni, and Min Qin. 2022. "Sleep Problems and New Occurrence of Chronic Conditions during the COVID-19 Pandemic in the UK" International Journal of Environmental Research and Public Health 19, no. 23: 15664. https://doi.org/10.3390/ijerph192315664
APA StyleFalkingham, J., Evandrou, M., Vlachantoni, A., & Qin, M. (2022). Sleep Problems and New Occurrence of Chronic Conditions during the COVID-19 Pandemic in the UK. International Journal of Environmental Research and Public Health, 19(23), 15664. https://doi.org/10.3390/ijerph192315664