

The Effect of Aerobic Exercise on Cognitive Function in People with Alzheimer’s Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Data Extraction
2.5. Methodological Quality Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Risk of Bias
3.4. Meta-Analysis Results
3.4.1. Effects of Aerobic Exercise on Cognitive Function in AD Patients
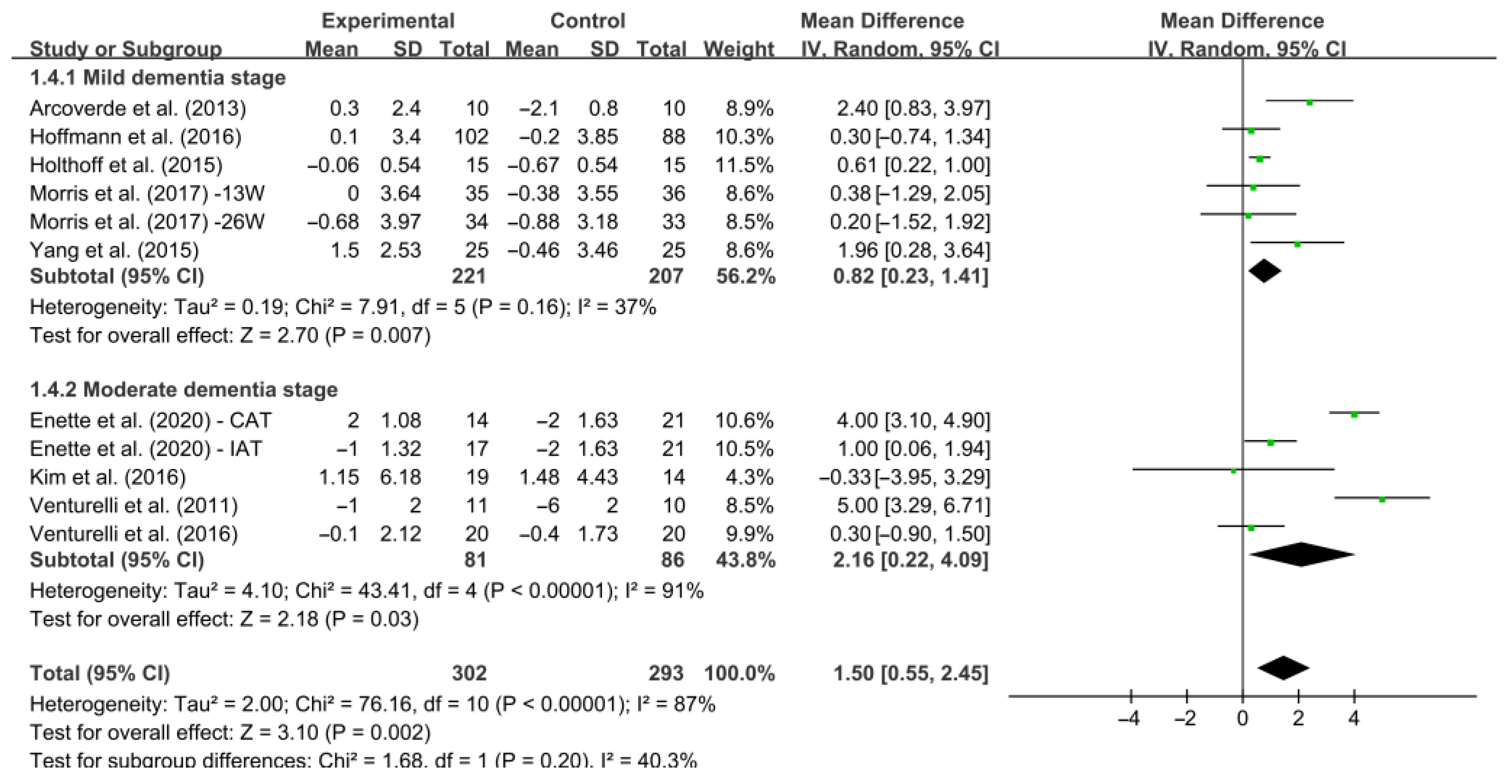
3.4.2. Subgroup Analysis
4. Discussion
4.1. Effects of Aerobic Exercise on Cognitive Function
4.2. Subgroup Analysis
4.3. Limitations of the Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the global burden of disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. 2021 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2021, 17, 327–406. [Google Scholar] [CrossRef] [PubMed]
- Brenowitz, W.D.; Hubbard, R.A.; Keene, C.D.; Hawes, S.E.; Longstreth, W.T., Jr.; Woltjer, R.L.; Kukull, W.A. Mixed neuropathologies and estimated rates of clinical progression in a large autopsy sample. Alzheimer’s Dement. 2016, 13, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Qiu, C.; Kivipelto, M.; von Strauss, E. Epidemiology of Alzheimer’s disease: Occurrence, determinants, and strategies toward intervention. Dialog-Clin. Neurosci. 2009, 11, 111–128. [Google Scholar] [CrossRef]
- Erkkinen, M.G.; Kim, M.-O.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2017, 10, a033118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrighi, H.M.; Neumann, P.J.; Lieberburg, I.M.; Townsend, R.J. Lethality of Alzheimer Disease and Its Impact on Nursing Home Placement. Alzheimer Dis. Assoc. Disord. 2010, 24, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Etters, L.; Goodall, D.; Harrison, B.E. Caregiver burden among dementia patient caregivers: A review of the literature. J. Am. Acad. Nurse Pract. 2008, 20, 423–428. [Google Scholar] [CrossRef]
- Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, A.M.; Winblad, B.; Jönsson, L.; Liu, Z.; Prince, M. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimer’s Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wolters, F.J.; Ikram, M.A. Epidemiology of Dementia: The Burden on Society, the Challenges for Research. Methods Mol. Biol. 2018, 1750, 3–14. [Google Scholar] [CrossRef]
- Jia, R.-X.; Liang, J.-H.; Xu, Y.; Wang, Y.-Q. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: A meta-analysis. BMC Geriatr. 2019, 19, 181. [Google Scholar] [CrossRef]
- Cedazo-Mínguez, A. Apolipoprotein E and Alzheimer’s disease: Molecular mechanisms and therapeutic opportunities. J. Cell. Mol. Med. 2007, 11, 1227–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Mendiola-Precoma, J.; Berumen, L.C.; Padilla, K.; Garcia-Alcocer, G. Therapies for Prevention and Treatment of Alzheimer’s Disease. BioMed Res. Int. 2016, 2016, 2589276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummings, J.L.; Tong, G.; Ballard, C. Treatment Combinations for Alzheimer’s Disease: Current and Future Pharmacotherapy Options. J. Alzheimer’s Dis. 2019, 67, 779–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossello, E.; Ballini, E. Management of patients with Alzheimer’s disease: Pharmacological treatment and quality of life. Ther. Adv. Chronic Dis. 2012, 3, 183–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.-T.; Etnier, J.L.; Wu, C.-H.; Cho, Y.-M.; Hung, T.-M.; Chang, Y.-K. Dose-Response Relationship between Exercise Duration and Executive Function in Older Adults. J. Clin. Med. 2018, 7, 279. [Google Scholar] [CrossRef] [Green Version]
- Scales, K.; Zimmerman, S.; Miller, S.J. Evidence-Based Nonpharmacological Practices to Address Behavioral and Psychological Symptoms of Dementia. Gerontologist 2018, 58, S88–S102. [Google Scholar] [CrossRef] [Green Version]
- Sikkes, S.A.; Tang, Y.; Jutten, R.J.; Wesselman, L.M.; Turkstra, L.S.; Brodaty, H.; Clare, L.; Cassidy-Eagle, E.; Cox, K.L.; Chételat, G.; et al. Toward a theory-based specification of non-pharmacological treatments in aging and dementia: Focused reviews and methodological recommendations. Alzheimer’s Dement. 2020, 17, 255–270. [Google Scholar] [CrossRef]
- Venturelli, M.; Scarsini, R.; Schena, F. Six-Month Walking Program Changes Cognitive and ADL Performance in Patients With Alzheimer. Am. J. Alzheimer’s Dis. Other Dementiasr 2011, 26, 381–388. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M. Aerobic Exercise and Neurocognitive Performance: A Meta-Analytic Review of Randomized Controlled Trials. Psychosom. Med. 2010, 72, 239–252. [Google Scholar] [CrossRef]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Bs, S.B.H.; Zelinski, E.M. Extended Practice and Aerobic Exercise Interventions Benefit Untrained Cognitive Outcomes in Older Adults: A Meta-Analysis. J. Am. Geriatr. Soc. 2011, 60, 136–141. [Google Scholar] [CrossRef] [Green Version]
- Guadagni, V.; Drogos, L.L.; Tyndall, A.V.; Davenport, M.H.; Anderson, T.J.; Eskes, G.A.; Longman, R.S.; Hill, M.D.; Hogan, D.B.; Poulin, M.J. Aerobic exercise improves cognition and cerebrovascular regulation in older adults. Neurology 2020, 94, e2245–e2257. [Google Scholar] [CrossRef]
- Liu-Ambrose, T.; Best, J.R.; Davis, J.C.; Eng, J.J.; Lee, P.E.; Jacova, C.; Boyd, L.A.; Brasher, P.M.; Munkacsy, M.; Cheung, W.; et al. Aerobic exercise and vascular cognitive impairment: A randomized controlled trial. Neurology 2016, 87, 2082–2090. [Google Scholar] [CrossRef] [Green Version]
- Nocera, J.R.; Mammino, K.; Kommula, Y.; Wharton, W.; Crosson, B.; McGregor, K.M. Effects of Combined Aerobic Exercise and Cognitive Training on Verbal Fluency in Older Adults. Gerontol. Geriatr. Med. 2020, 6, 2333721419896884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.-Y.; Shan, C.-L.; Qing, H.; Wang, W.; Zhu, Y.; Yin, M.-M.; Machado, S.; Yuan, T.-F.; Wu, T. The Effects of Aerobic Exercise on Cognitive Function of Alzheimer’s Disease Patients. CNS Neurol. Disord.—Drug Targets 2015, 14, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Kemoun, G.; Thibaud, M.; Roumagne, N.; Carette, P.; Albinet, C.; Toussaint, L.; Paccalin, M.; Dugué, B. Effects of a Physical Training Programme on Cognitive Function and Walking Efficiency in Elderly Persons with Dementia. Dement. Geriatr. Cogn. Disord. 2010, 29, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Bernardo, T.; Marques-Aleixo, I.; Beleza, J.; Oliveira, P.; Ascensão, A.; Magalhães, J. Physical Exercise and Brain Mitochondrial Fitness: The Possible Role Against Alzheimer’s Disease. Brain Pathol. 2016, 26, 648–663. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: New York, NY, USA, 2008. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. (Engl. Ed.) 2021, 74, 790–799. [Google Scholar] [CrossRef]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef] [PubMed]
- You, Q.; Yu, L.; Li, G.; He, H.; Lv, Y. Effects of Different Intensities and Durations of Aerobic Exercise on Vascular Endothelial Function in Middle-Aged and Elderly People: A Meta-analysis. Front. Physiol. 2022, 12, 803102. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Li, Z.; Peng, X.; Xiang, W.; Han, J.; Li, K. The effect of resistance training on cognitive function in the older adults: A systematic review of randomized clinical trials. Aging 2018, 30, 1259–1273. [Google Scholar] [CrossRef]
- Cott, C.A.; Dawson, P.; Sidani, S.; Wells, D. The Effects of a Walking/Talking Program on Communication, Ambulation, and Functional Status in Residents with Alzheimer Disease. Alzheimer Dis. Assoc. Disord. 2002, 16, 81–87. [Google Scholar] [CrossRef]
- Enette, L.; Vogel, T.; Merle, S.; Valard-Guiguet, A.-G.; Ozier-Lafontaine, N.; Neviere, R.; Leuly-Joncart, C.; Fanon, J.L.; Lang, P.O. Effect of 9 weeks continuous vs. interval aerobic training on plasma BDNF levels, aerobic fitness, cognitive capacity and quality of life among seniors with mild to moderate Alzheimer’s disease: A randomized controlled trial. Eur. Rev. Aging Phys. Act. 2020, 17, 2. [Google Scholar] [CrossRef]
- Holthoff, V.A.; Marschner, K.; Scharf, M.; Steding, J.; Meyer, S.; Koch, R.; Donix, M. Effects of Physical Activity Training in Patients with Alzheimer’s Dementia: Results of a Pilot RCT Study. PLoS ONE 2015, 10, e0121478. [Google Scholar] [CrossRef] [Green Version]
- Venturelli, M.; Sollima, A.; Cè, E.; Limonta, E.; Bisconti, A.V.; Brasioli, A.; Muti, E.; Esposito, F. Effectiveness of Exercise- and Cognitive-Based Treatments on Salivary Cortisol Levels and Sundowning Syndrome Symptoms in Patients with Alzheimer’s Disease. J. Alzheimer’s Dis. 2016, 53, 1631–1640. [Google Scholar] [CrossRef]
- Arcoverde, C.; Deslandes, A.; Moraes, H. Treadmill training as an augmentation treatment for Alzheimer?s disease: A pilot randomized controlled study. Arq. De Neuro-Psiquiatr. 2014, 72, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, K.; Sobol, N.A.; Frederiksen, K.S.; Beyer, N.; Vogel, A.; Vestergaard, K.; Brændgaard, H.; Gottrup, H.; Lolk, A.; Wermuth, L.; et al. Moderate-to-High Intensity Physical Exercise in Patients with Alzheimer’s Disease: A Randomized Controlled Trial. J. Alzheimer’s Dis. 2016, 50, 443–453. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.-J.; Han, C.-W.; Min, K.-Y.; Cho, C.-Y.; Lee, C.-W.; Ogawa, Y.; Mori, E.; Kohzuki, M. Physical Exercise with Multicomponent Cognitive Intervention for Older Adults with Alzheimer’s Disease: A 6-Month Randomized Controlled Trial. Dement. Geriatr. Cogn. Disord. Extra 2016, 6, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.K.; Vidoni, E.D.; Johnson, D.K.; Van Sciver, A.; Mahnken, J.D.; Honea, R.A.; Wilkins, H.M.; Brooks, W.M.; Billinger, S.A.; Swerdlow, R.H.; et al. Aerobic exercise for Alzheimer’s disease: A randomized controlled pilot trial. PLoS ONE 2017, 12, e0170547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobol, N.A.; Dall, C.H.; Høgh, P.; Hoffmann, K.; Frederiksen, K.S.; Vogel, A.; Siersma, V.; Waldemar, G.; Hasselbalch, S.G.; Beyer, N. Change in Fitness and the Relation to Change in Cognition and Neuropsychiatric Symptoms After Aerobic Exercise in Patients with Mild Alzheimer’s Disease. J. Alzheimer’s Dis. 2018, 65, 137–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidoni, E.D.; Perales, J.; Alshehri, M.; Giles, A.-M.; Siengsukon, C.F.; Burns, J.M. Aerobic Exercise Sustains Performance of Instrumental Activities of Daily Living in Early-Stage Alzheimer Disease. J. Geriatr. Phys. Ther. 2019, 42, E129–E134. [Google Scholar] [CrossRef]
- Yu, F.; Salisbury, D.; Mathiason, M.A. Inter-individual differences in the responses to aerobic exercise in Alzheimer’s disease: Findings from the FIT-AD trial. J. Sport Health Sci. 2020, 10, 65–72. [Google Scholar] [CrossRef]
- Yu, F.; Vock, D.M.; Zhang, L.; Salisbury, D.; Nelson, N.W.; Chow, L.S.; Smith, G.; Barclay, T.R.; Dysken, M.; Wyman, J.F. Cognitive Effects of Aerobic Exercise in Alzheimer’s Disease: A Pilot Randomized Controlled Trial. J. Alzheimer’s Dis. 2021, 80, 233–244. [Google Scholar] [CrossRef]
- Cendoroglo, M.S. Exercise programs for people with dementia. Sao Paulo Med. J. 2014, 132, 195–196. [Google Scholar] [CrossRef] [Green Version]
- Yu, F.; Kolanowski, A.M.; Strumpf, N.E.; Eslinger, P.J. Improving cognition and function through exercise intervention in Alzheimer’s disease. J. Nurs. Sch. 2006, 38, 358–365. [Google Scholar] [CrossRef]
- Rao, A.K.; Chou, A.; Bursley, B.; Smulofsky, J.; Jezequel, J. Systematic Review of the Effects of Exercise on Activities of Daily Living in People With Alzheimer’s Disease. Am. J. Occup. Ther. 2014, 68, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, S.B.; Aslan, S.; Spence, J.S. Shorter term aerobic exercise improves brain, cognition, and cardiovascular fitness in aging. Front. Aging Neurosci. 2013, 5, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Praag, H.; Shubert, T.E.; Zhao, C.; Gage, F.H. Exercise Enhances Learning and Hippocampal Neurogenesis in Aged Mice. J. Neurosci. 2005, 25, 8680–8685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilckens, K.A.; Stillman, C.M.; Waiwood, A.M.; Kang, C.; Leckie, R.L.; Peven, J.C.; Foust, J.E.; Fraundorf, S.H.; Erickson, K.I. Exercise interventions preserve hippocampal volume: A meta-analysis. Hippocampus 2020, 31, 335–347. [Google Scholar] [CrossRef]
- Lange-Asschenfeldt, C.; Kojda, G. Alzheimer’s disease, cerebrovascular dysfunction and the benefits of exercise: From vessels to neurons. Exp. Gerontol. 2008, 43, 499–504. [Google Scholar] [CrossRef]
- Phillips, C.; Baktir, M.A.; Das, D.; Lin, B.; Salehi, A. The Link Between Physical Activity and Cognitive Dysfunction in Alzheimer Disease. Phys. Ther. 2015, 95, 1046–1060. [Google Scholar] [CrossRef] [Green Version]
- Walsh, N.P.; Gleeson, M.; Pyne, D.B.; Nieman, D.C.; Dhabhar, F.S.; Shephard, R.J.; Oliver, S.J.; Bermon, S.; Kajeniene, A. Position statement. Part two: Maintaining immune health. Exerc. Immunol. Rev. 2011, 17, 64–103. [Google Scholar]
- Coelho, F.G.D.M.; Vital, T.M.; Stein, A.M.; Arantes, F.J.; Rueda, A.V.; Camarini, R.; Teodorov, E.; Santos-Galduróz, R.F. Acute Aerobic Exercise Increases Brain-Derived Neurotrophic Factor Levels in Elderly with Alzheimer’s Disease. J. Alzheimer’s Dis. 2014, 39, 401–408. [Google Scholar] [CrossRef]
- Cotman, C.W. Exercise: A behavioral intervention to enhance brain health and plasticity. Trends Neurosci. 2002, 25, 295–301. [Google Scholar] [CrossRef]
- Stigger, F.S.; Marcolino, M.A.Z.; Portela, K.M.; Plentz, R. Effects of Exercise on Inflammatory, Oxidative, and Neurotrophic Biomarkers on Cognitively Impaired Individuals Diagnosed With Dementia or Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 74, 616–624. [Google Scholar] [CrossRef]
- Aberg, M.A.; Åberg, N.D.; Hedbäcker, H.; Oscarsson, J.; Eriksson, P.S. Peripheral Infusion of IGF-I Selectively Induces Neurogenesis in the Adult Rat Hippocampus. J. Neurosci. 2000, 20, 2896–2903. [Google Scholar] [CrossRef] [PubMed]
- Homolak, J.; Mudrovčić, M.; Vukić, B.; Toljan, K. Circadian Rhythm and Alzheimer’s Disease. Med. Sci. 2018, 6, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albinet, C.T.; Abou-Dest, A.; André, N.; Audiffren, M. Executive functions improvement following a 5-month aquaerobics program in older adults: Role of cardiac vagal control in inhibition performance. Biol. Psychol. 2016, 115, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Albinet, C.T.; Boucard, G.; Bouquet, C.A.; Audiffren, M. Increased heart rate variability and executive performance after aerobic training in the elderly. Eur. J. Appl. Physiol. 2010, 109, 617–624. [Google Scholar] [CrossRef]
- Schwarck, S.; Busse, N.; Ziegler, G.; Glanz, W.; Becke, A.; Düzel, E. Heart Rate Variability During Physical Exercise Is Associated With Improved Cognitive Performance in Alzheimer’s Dementia Patients—A Longitudinal Feasibility Study. Front. Sports Act. Living 2021, 3, 684089. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Hearth Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.-K.; Etnier, J.L. Chronic exercise and cognitive function: An update of current findings. Int. J. Sport Exerc. Psychol. 2016, 17, 85–88. [Google Scholar] [CrossRef]
- Cai, Z.; Wang, X.; Yin, J.; Song, D.; Chen, Z. Effects of physical exercise on working memory in older adults: A systematic and meta-analytic review. Eur. Rev. Aging Phys. Act. 2021, 18, 18. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Groot, C.; Hooghiemstra, A.M.; Raijmakers, P.G.H.M. The effect of physical activity on cognitive function in patients with dementia: A meta-analysis of randomized control trials. Ageing Res. Rev. 2016, 25, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, B.M.; Tijhuis, M.A.; Kalmijn, S.; Giampaoli, S.; Nissinen, A.; Kromhout, D. Physical activity in relation to cognitive decline in elderly men. FINE Study 2004, 63, 2316–2321. [Google Scholar] [CrossRef] [PubMed]
- Kruger, J.; Buchner, D.M.; Prohaska, T.R. The Prescribed Amount of Physical Activity in Randomized Clinical Trials in Older Adults. Gerontologist 2009, 49, S100–S107. [Google Scholar] [CrossRef] [PubMed]
- Panza, G.A.; Taylor, B.A.; MacDonald, H.; Johnson, B.T.; Zaleski, A.L.; Livingston, J.; Thompson, P.D.; Pescatello, L.S. Can Exercise Improve Cognitive Symptoms of Alzheimer’s Disease? J. Am. Geriatr. Soc. 2018, 66, 487–495. [Google Scholar] [CrossRef] [Green Version]
- Doody, R.S.; Massman, P.; Dunn, J.K. A Method for Estimating Progression Rates in Alzheimer Disease. Arch. Neurol. 2001, 58, 449–454. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Std_EFF | Coef. | Std. Err. | t | p > |t| | 95% CI |
|---|---|---|---|---|---|
| Slope | 0.5688279 | 0.7304694 | 0.78 | 0.456 | −1.083609, 2.221265 |
| Bias | 1.409892 | 1.53018 | 0.92 | 0.381 | −2.051615, 4.871399 |
| Study | A | B | C | D | E | F | G | H | I | J | K | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arcoverde et al. (2013) [42] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7/10 |
| Kim et al. (2016) [44] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7/10 |
| Hoffmann et al. (2016) [43] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7/10 |
| Yu et al. (2020) [48] | Y | Y | N | Y | N | N | Y | N | N | Y | Y | 5/10 |
| Yang et al. (2015) [27] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6/10 |
| Fang Yu et al. (2021) [49] | Y | Y | N | Y | N | N | Y | N | N | Y | Y | 5/10 |
| Sobol et al. (2018) [46] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6/10 |
| Vidoni et al. (2019) [47] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7/10 |
| Morris et al. (2017) [45] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7/10 |
| Cott et al. (2002) [38] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7/10 |
| Holthoff et al. (2015) [40] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6/10 |
| Kemoun et al. (2010) [28] | Y | Y | N | Y | N | N | N | N | Y | Y | Y | 5/10 |
| Venturelli et al. (2011) [20] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7/10 |
| Venturelli et al. (2016) [41] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7/10 |
| Enette et al. (2020) [39] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, S.; Zhen, K.; Su, Q.; Chen, Y.; Lv, Y.; Yu, L. The Effect of Aerobic Exercise on Cognitive Function in People with Alzheimer’s Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 15700. https://doi.org/10.3390/ijerph192315700
Zhang S, Zhen K, Su Q, Chen Y, Lv Y, Yu L. The Effect of Aerobic Exercise on Cognitive Function in People with Alzheimer’s Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(23):15700. https://doi.org/10.3390/ijerph192315700
Chicago/Turabian StyleZhang, Shiyan, Kai Zhen, Qing Su, Yiyan Chen, Yuanyuan Lv, and Laikang Yu. 2022. "The Effect of Aerobic Exercise on Cognitive Function in People with Alzheimer’s Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 23: 15700. https://doi.org/10.3390/ijerph192315700
APA StyleZhang, S., Zhen, K., Su, Q., Chen, Y., Lv, Y., & Yu, L. (2022). The Effect of Aerobic Exercise on Cognitive Function in People with Alzheimer’s Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 19(23), 15700. https://doi.org/10.3390/ijerph192315700