
Comparison of Laparoscopic and Open Radical Cystectomy for Muscle-Invasive Bladder Cancer

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study and Control Groups
2.2. Group Comparison
2.3. Oncological Results
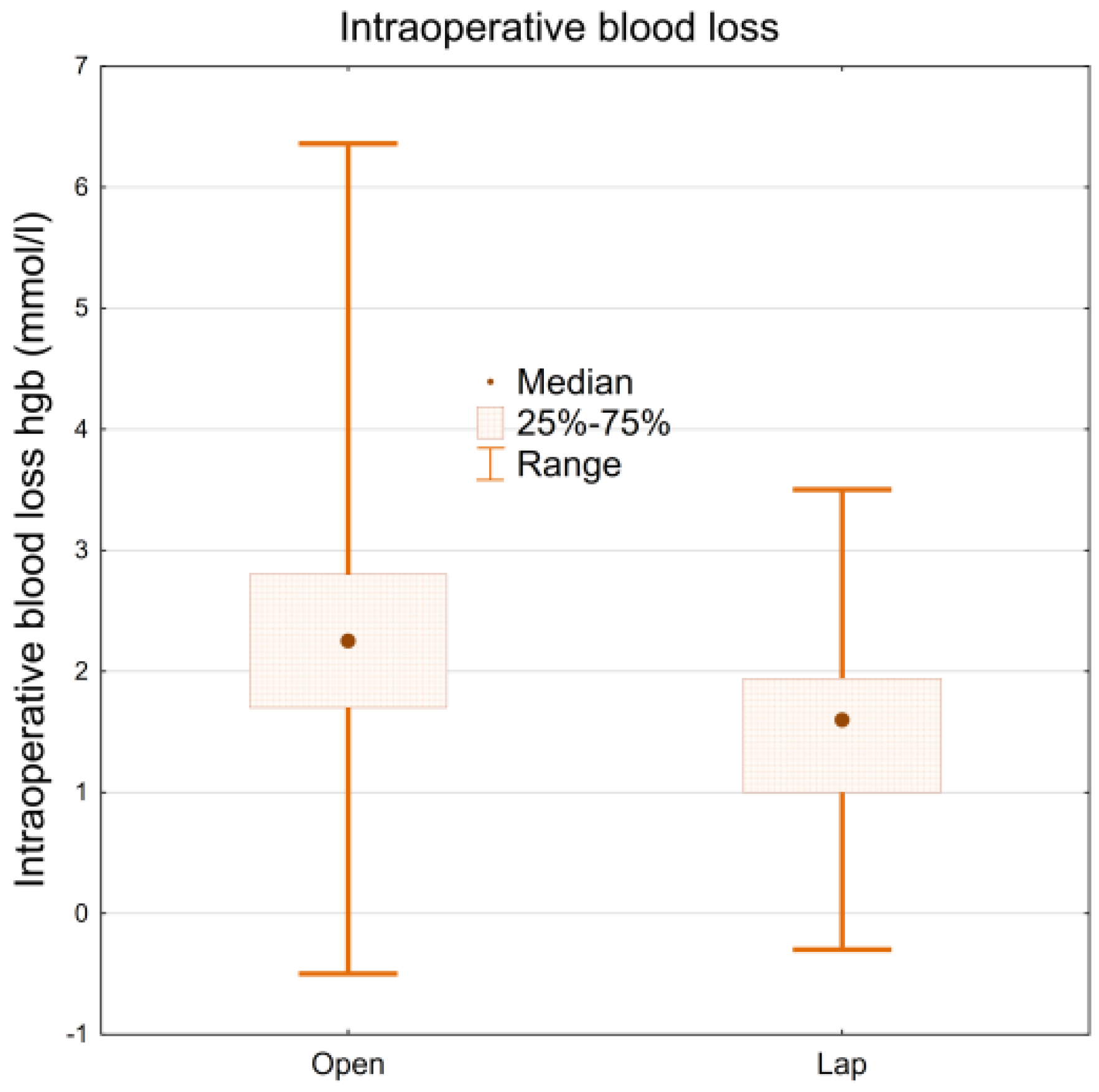
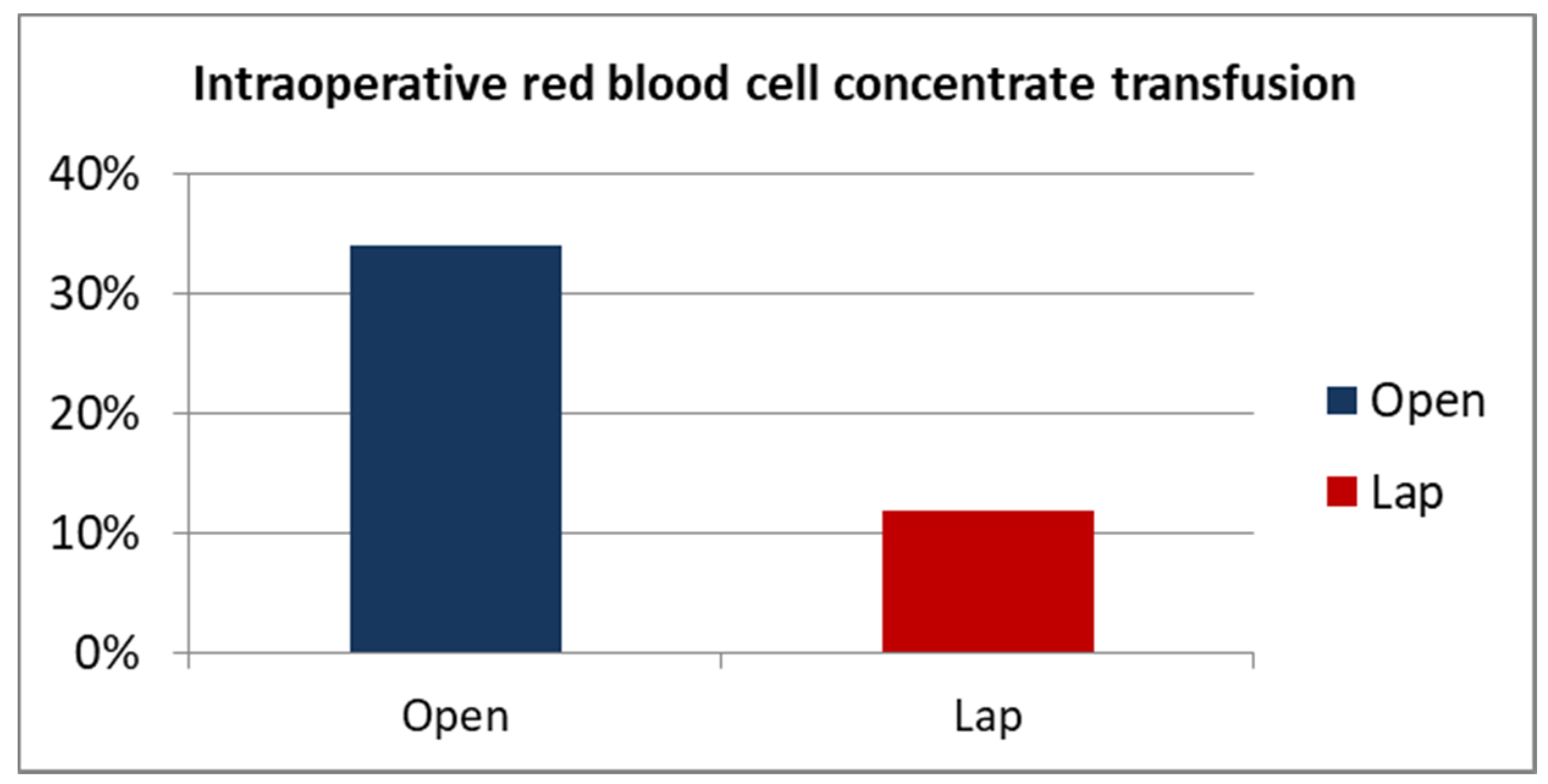
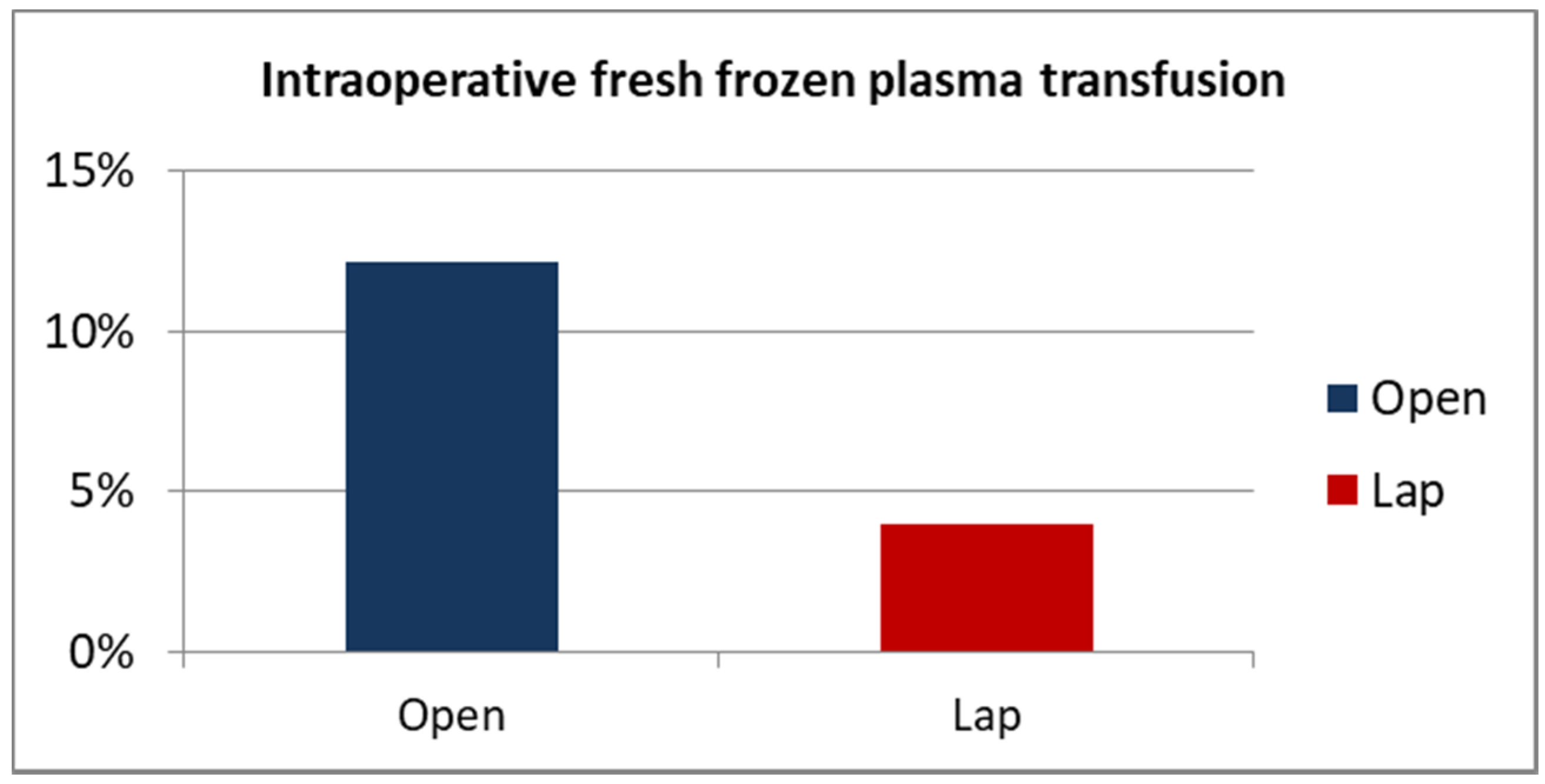
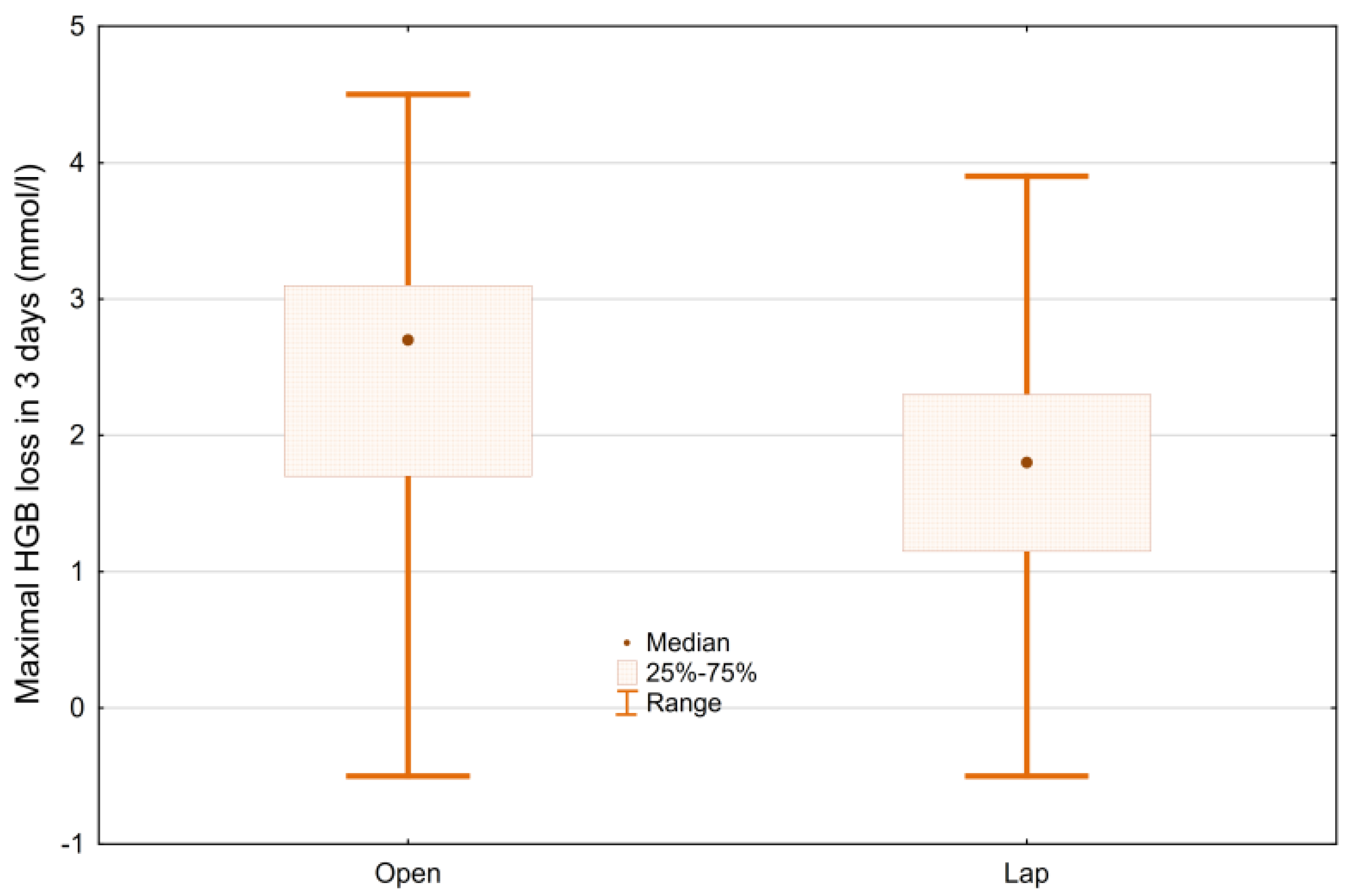
2.4. Blood Loss and Transfusion Rate
2.5. Complications
2.6. Other
2.7. Statistical Analysis
3. Results
3.1. Group Comparison
3.2. Oncological Results
3.3. Blood Loss and Transfusion Rate
3.4. Complications
3.5. Other
4. Discussion
5. Conclusions
- A radical cystectomy performed with the laparoscopic technique ensures comparable oncological results to the open approach in terms of overall survival, regardless of the stage of the disease. The percentage of positive surgical margins is comparable in the laparoscopic and the open cystectomy;
- The laparoscopic technique in radical cystectomy significantly reduces intraoperative and post-operative blood loss and the need for transfusion of blood products;
- There are no significant differences in the time of the surgery, time of post-operative hospitalization, time to the implementation of full oral alimentation between the laparoscopic, and the open cystectomy;
- The laparoscopic cystectomy shows no significant differences in terms of early post-operative complications compared to the open surgery. Some groups of patients, however, benefit from significantly fewer septic and ileus complications with laparoscopic cystectomy;
- Further studies are needed to assess the long-term outcomes of laparoscopic cystectomy for MIBC.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologist Classification |
| BCG therapy | Bacillus Calmette-Guerin intravesical therapy |
| BMI | Body mass index |
| CI | Confidence interval |
| FFP | Fresh frozen plasma |
| Hgb | Hemoglobin |
| LNY | Lymph node yield |
| LRC | Laparoscopic radical cystectomy |
| MIBC | Muscle-invasive bladder cancer |
| NMIBC | Non-muscle-invasive bladder cancer |
| OR | Odds ratio |
| ORC | Open radical cystectomy |
| OS | Overall survival |
| RCC | Red blood cell concentrate |
| TNM | TNM Classification of Malignant Tumors |
| TURB | Transurethral bladder resection |
| WBC | White blood cells |
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Burger, M.; Catto, J.W.F.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L.A.; La Vecchia, C.; Shariat, S.; et al. Epidemiology and Risk Factors of Urothelial Bladder Cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Witjes, J.A.; Lebret, T.; Compérat, E.M.; Cowan, N.C.; De Santis, M.; Bruins, H.M.; Hernández, V.; Espinós, E.L.; Dunn, J.; Rouanne, M.; et al. Updated 2016 EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer. Eur. Urol. 2017, 71, 462–475. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between Smoking and Risk of Bladder Cancer Among Men and Women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.-C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical Cystectomy in the Treatment of Invasive Bladder Cancer: Long-Term Results in 1054 Patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, R.J.; van der Meijden, A.P.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.; Kurth, K. Predicting Recurrence and Progression in Individual Patients with Stage Ta T1 Bladder Cancer Using EORTC Risk Tables: A Combined Analysis of 2596 Patients from Seven EORTC Trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Marshall, V.F. Transplantation of the Ureters and Total Cystectomy. J. Urol. 1947, 58, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Novotny, V.; Hakenberg, O.W.; Wiessner, D.; Heberling, U.; Litz, R.J.; Oehlschlaeger, S.; Wirth, M.P. Perioperative Complications of Radical Cystectomy in a Contemporary Series. Eur. Urol. 2007, 51, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Leminski, A.; Puszynski, M.; Kups, M.; Slojewski, M.; Sikorski, A. C27 results of surgical treatment of invasive bladder tumors in Poland—Single center observation of 402 patients after radical cystectomy. Eur. Urol. Suppl. 2012, 11, 88. [Google Scholar] [CrossRef]
- Tang, K.; Li, H.; Xia, D.; Hu, Z.; Zhuang, Q.; Liu, J.; Xu, H.; Ye, Z. Laparoscopic versus Open Radical Cystectomy in Bladder Cancer: A Systematic Review and Meta-Analysis of Comparative Studies. PLoS ONE 2014, 9, e95667. [Google Scholar] [CrossRef] [PubMed]
- Rochon, J.; Gondan, M.; Kieser, M. To test or not to test: Preliminary assessment of normality when comparing two independent samples. BMC Med. Res. Methodol. 2012, 12, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hautmann, R.E. The oncologic results of laparoscopic radical cystectomy are not (yet) equivalent to open cystectomy. Curr. Opin. Urol. 2009, 19, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Bi, J.; Dingwei, Y.; Han, P.; Song, D.; Shi, L.; Ye, D.; Shen, Y.; Gou, X.; He, W.; et al. Survival after radical cystectomy for bladder cancer: Multicenter comparison between minimally invasive and open approaches. Asian J. Urol. 2020, 7, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Herr, H.; Lee, C.; Chang, S.; Lerner, S. Standardization of Radical Cystectomy and Pelvic Lymph Node Dissection for Bladder Cancer: A Collaborative Group Report. J. Urol. 2004, 171, 1823–1828. [Google Scholar] [CrossRef] [PubMed]
- Fonseka, T.; Ahmed, K.; Froghi, S.; Khan, S.A.; Dasgupta, P.; Khan, M.S. Comparing robotic, laparoscopic and open cystectomy: A systematic review and meta-analysis. Arch. Ital. Urol. Androl. 2015, 87, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaramillo, S.; Montane-Muntane, M.; Gambus, P.L.; Capitan, D.; Navarro-Ripoll, R.; Blasi, A. Perioperative blood loss: Estimation of blood volume loss or haemoglobin mass loss? Blood Transfus. 2020, 18, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Adamczyk, P.; Juszczak, K.; Kadłubowski, M.; Ostrowski, A.; Maciukiewicz, P.; Drewa, T. Can laparoscopic cystectomy become the method of choice in the treatment of invasive urothelial urinary bladder cancer? Adv. Clin. Exp. Med. 2020, 29, 301–304. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LRC n = 77 | ORC n = 82 | p-Value | |
|---|---|---|---|
| Age | 66 (44–84) | 65 (50–85) | 0.297 |
| Height | 1.7 (1.48–1.76) | 1.71 (1.5–1.89) | 0.985 |
| Weight | 77 (41–120) | 75 (44.5–114) | 0.558 |
| BMI | 25.88 (17.34–37.02) | 26.07 (17.9–34.48) | 0.582 |
| Male (sex) | 62 (80.5%) | 62 (75.6%) | 0.450 |
| Smoking: | |||
| - Yes | 25 (32.9) | 19 (24) | 0.380 |
| - Former | 44 (57.8) | 49 (62) | |
| - Never | 7 (9.2) | 11 (13.9) | |
| Hydronephrosis | |||
| - No | 46 (60.5%) | 46 (56.1%) | 0.800 |
| - Unilateral | 22 (28.9%) | 25 (30.5%) | |
| - Bilateral | 8 (10.5%) | 11 (13.4%) | |
| Waiting time for operation (days) | 89 (0–510) | 82 (14–208) | 0.107 |
| WBC (103) | 8.37 (3.01–34.02) | 8.18 (3.47–32.82) | 0.117 |
| Creatinine | 1.07(0.6–3.89) | 0.99(0.56–8.45) | 0.318 |
| Albumin in serum | 42.5 (29–49) | 43 (21–49) | 0.700 |
| Total protein in serum | 71 (53–78) | 71 (51–78) | 0.550 |
| Hgb (mmol/L) | 7.6 (5–10) | 8 (4.7–10.8) | 0.026 |
| RBC (mln/µL) | 4.07 (2.7–6.42) | 4.33 (2.7–5.41) | 0.053 |
| Hct (%) | 36.5 (24.4–48.6) | 37.9 (24.1–48.2) | 0.070 |
| No. comorbidities | 2 (0–6) | 1 (0–8) | 0.025 |
| ASA | 2 (1–4) | 2 (1–3) | 0.320 |
| ASA ≥ 2 | 71 (93.4%) | 72 (90%) | 0.630 |
| ASA ≥ 3 | 19 (25%) | 16 (20%) | 0.580 |
| cT3–4 (operator evaluation) | 35 (46%) | 47 (57.3%) | 0.150 |
| pT3–4 | 37 (48.7%) | 50 (61%) | 0.120 |
| pN+ | 16 (23.5%) | 30 (38%) | 0.060 |
| Urinary diversion: | |||
| - Ureterocutaneostomy | 39 (51.3%) | 43 (53.1%) | |
| - Ileal conduit (Bricker) | 37 (48.7%) | 33 (40.8%) | |
| - Studer neobladder | 0 | 5 (6.1%) | 0.070 |
| Urinary diversion: | |||
| - Ureterocutaneostomy | 39 (51.3%) | 43 (53.1%) | |
| - Ileal urinary diversion | 37 (48.7%) | 38 (46.9%) | 0.820 |
| N = 158 | Relative Risk | Standard Error | Hazard Ratio (95%) Upper | Hazard Ratio (95%) Lower | p-Value |
|---|---|---|---|---|---|
| Open/laparoscopic (0/1) | 1.408 | 0.242 | 0.876 | 2.261 | 0.157 |
| pT0–2: 0; pT3–4: 1 | 3.024 | 0.294 | 1.701 | 5.378 | <0.001 |
| Resection margin(0/1) | 2.25 | 0.276 | 1.31 | 3.862 | 0.003 |
| ASA ≥ 3 | 2.059 | 0.249 | 1.264 | 3.356 | 0.004 |
| Sex (female 0, male 1) | 0.965 | 0.257 | 0.583 | 1.598 | 0.889 |
| Age | 1.026 | 0.015 | 0.996 | 1.056 | 0.089 |
| BMI | 0.948 | 0.028 | 0.896 | 1.002 | 0.057 |
| Neoadjuvant chemotherapy | 0.962 | 0.303 | 0.531 | 1.744 | 0.899 |
| cT0–2: 0; cT3–4: 1 | 1.24 | 0.249 | 0.761 | 2.02 | 0.388 |
| N(-): 0, N(+): 1 | 1.718 | 0.303 | 0.949 | 3.11 | 0.074 |
| No. of N(+) | 1.055 | 0.053 | 0.952 | 1.17 | 0.309 |
| LRC n = 77 | ORC n = 82 | p-Value | |
|---|---|---|---|
| Clavien–Dindo > 2 | 24 (31.6%) | 26 (31.7%) | 0.98 |
| Clavien–Dindo > 3b | 12 (16%) | 12 (14.6%) | 0.81 |
| Prolonged drain leak | 23 (30.3%) | 36 (43.9%) | 0.07 |
| Ileus (conservative treatment) | 7 (9.2%) | 11 (13.4%) | 0.41 |
| Need of blood transfusions | 37 (48.7%) | 60 (73.2%) | 0.001 |
| Need of parenteral nutrition | 9 (11.8%) | 19 (23.2%) | 0.06 |
| SIRS/sepis | 22 (28.9%) | 33 (40.2%) | 0.13 |
| Ileus (surgical treatment), eventration | 5 (6.6%) | 13 (15.9%) | 0.11 |
| Gastrointestinal hemorrhage | 2 (2.63%) | 2 (2.44%) | 0.67 |
| Need of PCN drainage | 6 (7.9%) | 5 (6.1%) | 0.89 |
| Haemodialysis | 6 (7.9%) | 5 (6.1%) | 0.89 |
| Thromboembolism | 1 (1.32%) | 3 (3.66%) | 0.66 |
| Abscess/hematoma requiring drainage | 2 (2.6%) | 4 (4.9%) | |
| Hemorrhage requiring urgent reoperation | 0 | 1 (1.22%) | 0.96 |
| Colostomy | 0 | 2 (2.44%) | 0.51 |
| Limb amputation | 0 | 1 (1.22%) | 0.96 |
| ICU admission | 7 (9.2%) | 8 (9.8%) | 0.90 |
| Death | 5 (6.5%) | 8 (9.8%) | 0.66 |
| LRC n = 77 | ORC n = 82 | p-Value | |
|---|---|---|---|
| Hospitalization (days) | 7 (3–34) | 7 (5–71) | 0.263 |
| Operation time (minutes) | 240 (120–425) | 225 (135–360) | 0.140 |
| Antibiotic therapy (days) | 6 (2–27) | 6 (1–70) | 0.807 |
| Time to implementation of liquid diet (days) | 1 (1–6) | 1 (1–4) | 0.901 |
| Time to implementation of full oral alimentation (days) | 4 (2–25) | 4 (2–15) | 0.339 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lisiński, J.; Kienitz, J.; Tousty, P.; Kaczmarek, K.; Lemiński, A.; Słojewski, M. Comparison of Laparoscopic and Open Radical Cystectomy for Muscle-Invasive Bladder Cancer. Int. J. Environ. Res. Public Health 2022, 19, 15995. https://doi.org/10.3390/ijerph192315995
Lisiński J, Kienitz J, Tousty P, Kaczmarek K, Lemiński A, Słojewski M. Comparison of Laparoscopic and Open Radical Cystectomy for Muscle-Invasive Bladder Cancer. International Journal of Environmental Research and Public Health. 2022; 19(23):15995. https://doi.org/10.3390/ijerph192315995
Chicago/Turabian StyleLisiński, Janusz, Jakub Kienitz, Piotr Tousty, Krystian Kaczmarek, Artur Lemiński, and Marcin Słojewski. 2022. "Comparison of Laparoscopic and Open Radical Cystectomy for Muscle-Invasive Bladder Cancer" International Journal of Environmental Research and Public Health 19, no. 23: 15995. https://doi.org/10.3390/ijerph192315995
APA StyleLisiński, J., Kienitz, J., Tousty, P., Kaczmarek, K., Lemiński, A., & Słojewski, M. (2022). Comparison of Laparoscopic and Open Radical Cystectomy for Muscle-Invasive Bladder Cancer. International Journal of Environmental Research and Public Health, 19(23), 15995. https://doi.org/10.3390/ijerph192315995