
Comparative Biomonitoring of Arsenic Exposure in Mothers and Their Neonates in Comarca Lagunera, Mexico
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
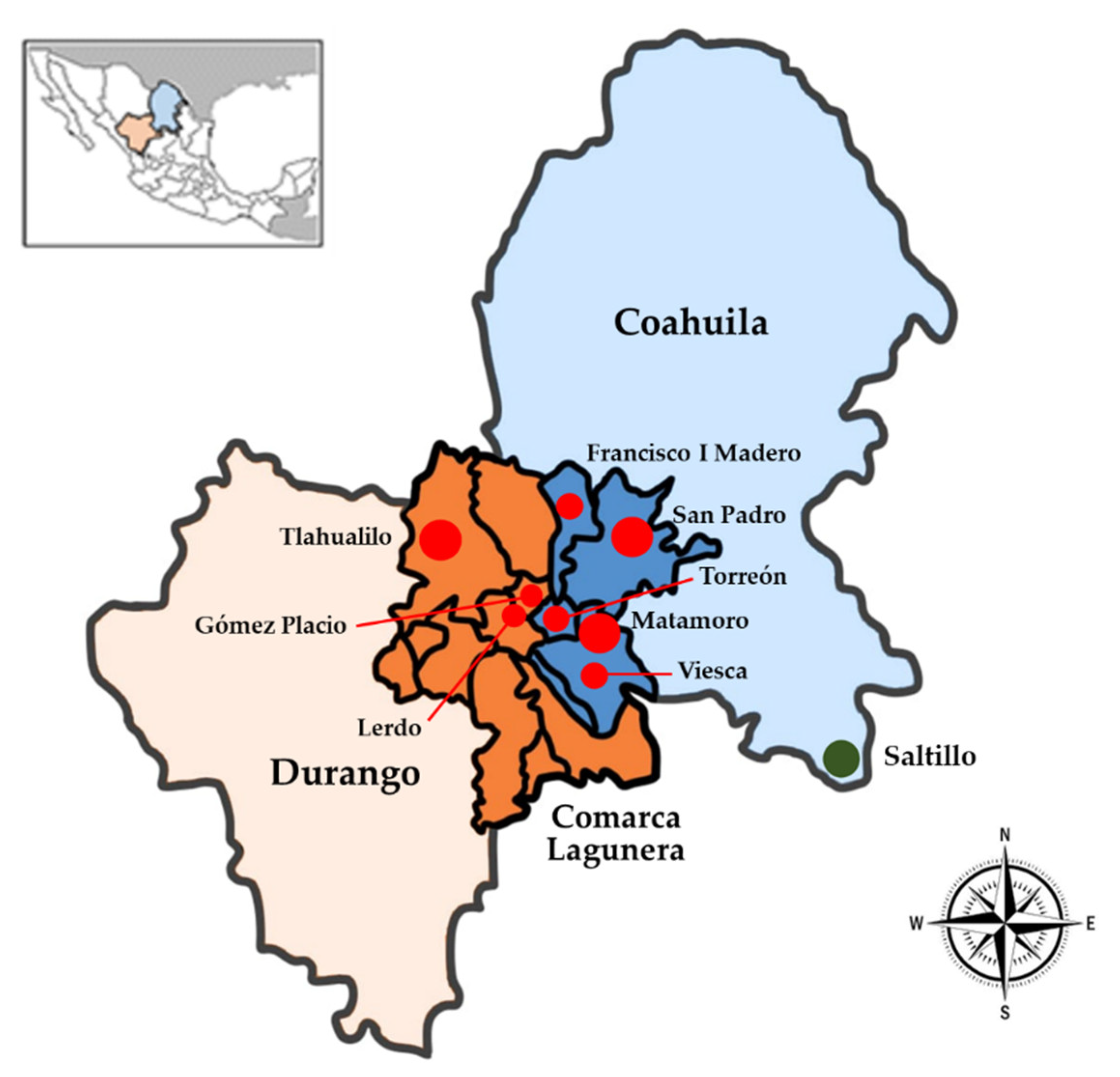
2.1. Study Location and Subjects
2.2. Sample Collection
2.3. Arsenic Determination
2.4. Ethical Considerations
2.5. Statistical Analysis
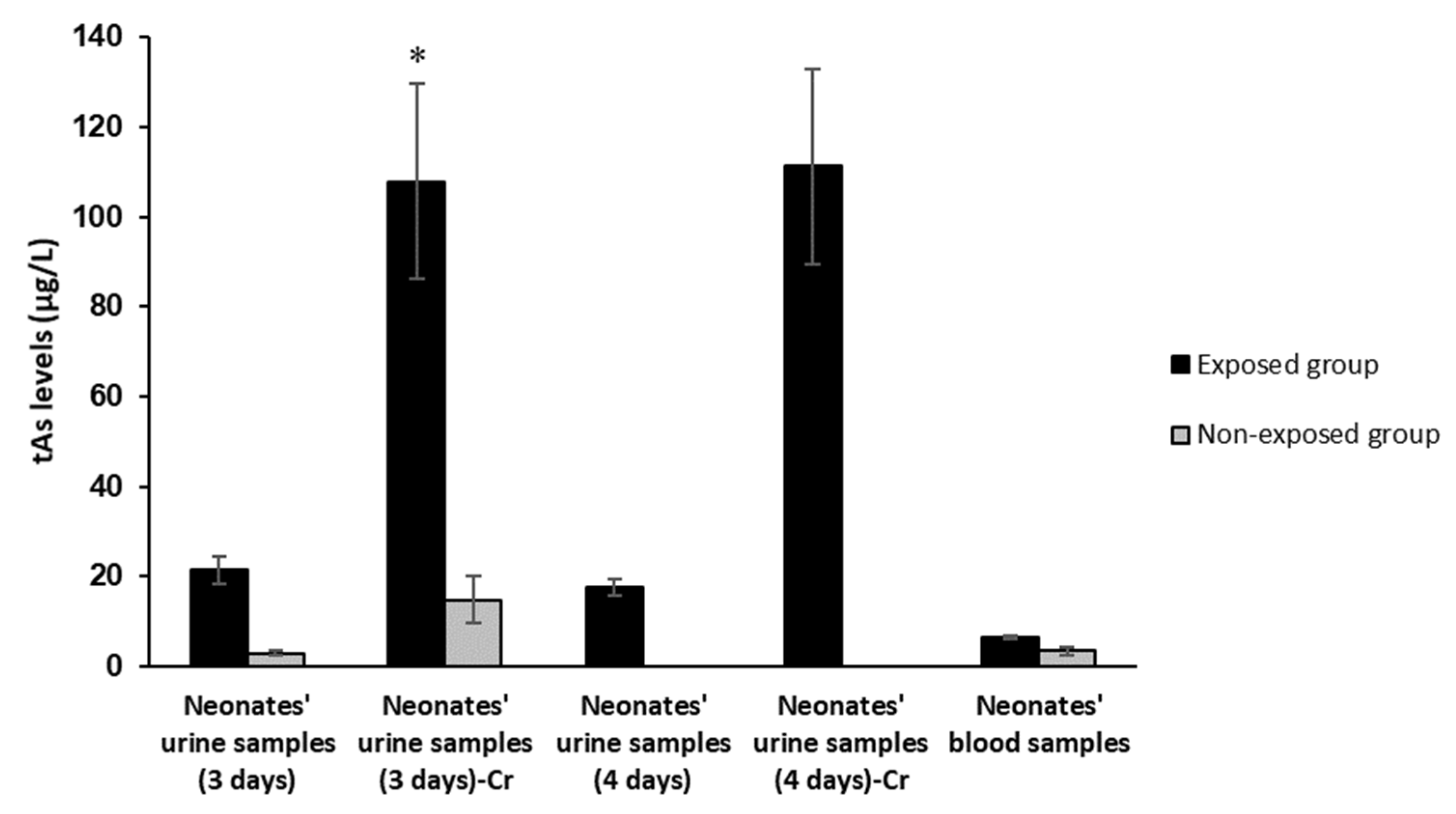
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cubadda, F.; Jackson, B.P.; Cottingham, K.L.; Van Horne, Y.O.; Kurzius-Spencer, M. Human exposure to dietary inorganic arsenic and other arsenic species: State of knowledge, gaps and uncertainties. Sci. Total. Environ. 2017, 579, 1228–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreccio, C.; Yuan, Y.; Calle, J.; Benítez, H.; Parra, R.L.; Acevedo, J.; Smith, A.H.; Liaw, J.; Steinmaus, C. Arsenic, Tobacco Smoke, and Occupation. Epidemiology 2013, 24, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Saadatzadeh, A.; Afzalan, S.; Zadehdabagh, R.; Tishezan, L.; Najafi, N.; SeyedTabib, M.; Noori, S.M.A. Determination of heavy metals (lead, cadmium, arsenic, and mercury) in authorized and unauthorized cosmetics. Cutan. Ocul. Toxicol. 2019, 38, 207–211. [Google Scholar] [CrossRef]
- Landrigan, P.J. The power of environmental protection: Arsenic in drinking water. Lancet Public Health 2017, 2, e488–e489. [Google Scholar] [CrossRef] [Green Version]
- Raessler, M. The Arsenic Contamination of Drinking and Groundwaters in Bangladesh: Featuring Biogeochemical Aspects and Implications on Public Health. Arch. Environ. Contam. Toxicol. 2018, 75, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackethal, C.; Kopp, J.F.; Sarvan, I.; Schwerdtle, T.; Lindtner, O. Total arsenic and water-soluble arsenic species in foods of the first German total diet study (BfR MEAL Study). Food Chem. 2021, 346, 128913. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.-Y.; Yu, S.-D.; Hong, Y.-S. Environmental Source of Arsenic Exposure. J. Prev. Med. Public Health 2014, 47, 253–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchounwou, P.B.; Yedjou, C.G.; Udensi, U.K.; Pacurari, M.; Stevens, J.J.; Patlolla, A.K.; Noubissi, F.; Kumar, S. State of the science review of the health effects of inorganic arsenic: Perspectives for future research. Environ. Toxicol. 2019, 34, 188–202. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Xi, S. A review on arsenic carcinogenesis: Epidemiology, metabolism, genotoxicity and epigenetic changes. Regul. Toxicol. Pharmacol. 2018, 99, 78–88. [Google Scholar] [CrossRef]
- Vahter, M.; Concha, G. Role of Metabolism in Arsenic Toxicity. Pharmacol. Toxicol. 2008, 89, 1–5. [Google Scholar] [CrossRef]
- Gao, S.; Lin, P.-I.; Mostofa, G.; Quamruzzaman, Q.; Rahman, M.; Rahman, M.L.; Su, L.; Hsueh, Y.-M.; Weisskopf, M.; Coull, B.; et al. Determinants of arsenic methylation efficiency and urinary arsenic level in pregnant women in Bangladesh. Environ. Health 2019, 18, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurzius-Spencer, M.; Burgess, J.L.; Harris, R.B.; Hartz, V.; Roberge, J.; Huang, S.; Hsu, C.-H.; O’Rourke, M.K. Contribution of diet to aggregate arsenic exposures—An analysis across populations. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 156–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McClintock, T.R.; Chen, Y.; Bundschuh, J.; Oliver, J.T.; Navoni, J.; Olmos, V.; Lepori, E.V.; Ahsan, H.; Parvez, F. Arsenic exposure in Latin America: Biomarkers, risk assessments and related health effects. Sci. Total Environ. 2012, 429, 76–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettinger, A.S.; Arbuckle, T.E.; Fisher, M.; Liang, C.L.; Davis, K.; Cirtiu, C.-M.; Bélanger, P.; LeBlanc, A.; Fraser, W.D. Arsenic levels among pregnant women and newborns in Canada: Results from the Maternal-Infant Research on Environmental Chemicals (MIREC) cohort. Environ. Res. 2017, 153, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Quansah, R.; Armah, F.; Essumang, D.K.; Luginaah, I.; Clarke, E.; Marfoh, K.; Cobbina, S.J.; Nketiah-Amponsah, E.; Namujju, P.B.; Obiri, S.; et al. Association of Arsenic with Adverse Pregnancy Outcomes/Infant Mortality: A Systematic Review and Meta-Analysis. Environ. Health Perspect. 2015, 123, 412–421. [Google Scholar] [CrossRef]
- Rahman, M.; Sohel, N.; Hore, S.K.; Yunus, M.; Bhuiya, A.; Streatfield, P.K. Prenatal arsenic exposure and drowning among children in Bangladesh. Glob. Health Action 2015, 8, 28702. [Google Scholar] [CrossRef] [Green Version]
- Valeri, L.; Mazumdar, M.M.; Bobb, J.F.; Henn, B.C.; Rodrigues, E.; Sharif, O.I.; Kile, M.L.; Quamruzzaman, Q.; Afroz, S.; Golam, M.; et al. The Joint Effect of Prenatal Exposure to Metal Mixtures on Neurodevelopmental Outcomes at 20–40 Months of Age: Evidence from Rural Bangladesh. Environ. Health Perspect. 2017, 125, 067015. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Liu, J.; Liu, B.; Liu, X.; Yu, X. Prenatal exposure to arsenic and neurobehavioral development of newborns in China. Environ. Int. 2018, 121, 421–427. [Google Scholar] [CrossRef]
- Rahman, A.; Vahter, M.; Ekström, E.-C.; Persson, L. Arsenic Exposure in Pregnancy Increases the Risk of Lower Respiratory Tract Infection and Diarrhea during Infancy in Bangladesh. Environ. Health Perspect. 2011, 119, 719–724. [Google Scholar] [CrossRef]
- Farzan, S.F.; Karagas, M.R.; Chen, Y. In utero and early life arsenic exposure in relation to long-term health and disease. Toxicol. Appl. Pharmacol. 2013, 272, 384–390. [Google Scholar] [CrossRef]
- Roh, T.; Steinmaus, C.; Marshall, G.; Ferreccio, C.; Liaw, J.; Smith, A.H. Age at Exposure to Arsenic in Water and Mortality 30–40 Years After Exposure Cessation. Am. J. Epidemiol. 2018, 187, 2297–2305. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.H.; Marshall, G.; Roh, T.; Ferreccio, C.; Liaw, J.; Steinmaus, C. Lung, Bladder, and Kidney Cancer Mortality 40 Years After Arsenic Exposure Reduction. Gynecol. Oncol. 2017, 110, 241–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punshon, T.; Davis, M.A.; Marsit, C.; Theiler, S.K.; Baker, E.R.; Jackson, B.P.; Conway, D.C.; Karagas, M.R. Placental arsenic concentrations in relation to both maternal and infant biomarkers of exposure in a US cohort. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 599–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samiee, F.; Leili, M.; Faradmal, J.; Torkshavand, Z.; Asadi, G. Exposure to arsenic through breast milk from mothers exposed to high levels of arsenic in drinking water: Infant risk assessment. Food Control 2019, 106, 106669. [Google Scholar] [CrossRef]
- Islam, R.; Attia, J.; Alauddin, M.; McEvoy, M.; McElduff, P.; Slater, C.; Islam, M.; Akhter, A.; D’Este, C.; Peel, R.; et al. Availability of arsenic in human milk in women and its correlation with arsenic in urine of breastfed children living in arsenic contaminated areas in Bangladesh. Environ. Health 2014, 13, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sternowsky, H.-J.; Moser, B.; Szadkowsky, D. Arsenic in breast milk during the first 3 months of lactation. Int. J. Hyg. Environ. Health 2002, 205, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Armienta, M.A.; Segovia, N. Arsenic and fluoride in the groundwater of Mexico. Environ. Geochem. Health 2008, 30, 345–353. [Google Scholar] [CrossRef]
- Fisher, A.T.; López-Carrillo, L.; Gamboa-Loira, B.; Cebrián, M.E. Standards for arsenic in drinking water: Implications for policy in Mexico. J. Public Health Policy 2017, 38, 395–406. [Google Scholar] [CrossRef] [Green Version]
- García-Alvarado, F.J.; Neri-Meléndez, H.; Armendáriz, L.P.; Guillen, M.R. Polimorfismos del gen Arsénico 3 Metiltransferasa (As3MT) y la eficiencia urinaria del metabolismo del arsénico en una población del norte de México. Rev. Peru Med. Exp. Salud Publica 2018, 35, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Laine, J.; Bailey, K.A.; Rubio-Andrade, M.; Olshan, A.F.; Smeester, L.; Drobná, Z.; Herring, A.H.; Stýblo, M.; García-Vargas, G.G.; Fry, R.C. Maternal Arsenic Exposure, Arsenic Methylation Efficiency, and Birth Outcomes in the Biomarkers of Exposure to ARsenic (BEAR) Pregnancy Cohort in Mexico. Environ. Health Perspect. 2015, 123, 186–192. [Google Scholar] [CrossRef]
- Ortega-Morales, N.B.; Cueto-Wong, J.A.; Barrientos-Juárez, E.; García-Vargas, G.; Salinas-González, H.; Garcia, A.B.; Martínez, J.M. Toxicity in Goats Exposed to Arsenic in the Region Lagunera, Northern Mexico. Vet. Sci. 2020, 7, 59. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.H. Arsine Evolution-Electrothermal Atomic Absorption Method for the Determination of Nanogram Levels of Total Arsenic in Urine and Water. J. Anal. Toxicol. 1980, 4, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Junge, W.; Wilke, B.; Halabi, A.; Klein, G. Determination of reference intervals for serum creatinine, creatinine excretion and creatinine clearance with an enzymatic and a modified Jaffé method. Clin. Chim. Acta 2004, 344, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Diaz, O.P.; Arcos, R.; Tapia, Y.; Pastene, R.; Velez, D.; Devesa, V.; Montoro, R.; Aguilera, V.; Becerra, M. Estimation of Arsenic Intake from Drinking Water and Food (Raw and Cooked) in a Rural Village of Northern Chile. Urine as a Biomarker of Recent Exposure. Int. J. Environ. Res. Public Health 2015, 12, 5614–5633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloom, M.S.; Neamtiu, I.A.; Surdu, S.; Pop, C.; Anastasiu, D.; Appleton, A.A.; Fitzgerald, E.F.; Gurzau, E.S. Low level arsenic contaminated water consumption and birth outcomes in Romania—An exploratory study. Reprod. Toxicol. 2016, 59, 8–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Shimoda, Y.; Wang, S.; Wang, Z.; Liu, J.; Liu, X.; Jin, H.; Gao, F.; Tong, J.; Yamanaka, K.; et al. Total arsenic and speciation analysis of saliva and urine samples from individuals living in a chronic arsenicosis area in China. Environ. Health Prev. Med. 2017, 22, 45. [Google Scholar] [CrossRef] [Green Version]
- Welch, B.; Smit, E.; Cardenas, A.; Hystad, P.; Kile, M.L. Trends in urinary arsenic among the U.S. population by drinking water source: Results from the National Health and Nutritional Examinations Survey 2003–2014. Environ. Res. 2018, 162, 8–17. [Google Scholar] [CrossRef]
- Komorowicz, I.; Barałkiewicz, D. Determination of total arsenic and arsenic species in drinking water, surface water, wastewater, and snow from Wielkopolska, Kujawy-Pomerania, and Lower Silesia provinces, Poland. Environ. Monit. Assess. 2016, 188, 504. [Google Scholar] [CrossRef] [Green Version]
- Bommarito, P.A.; Beck, R.; Douillet, C.; Del Razo, L.M.; Garcia-Vargas, G.-G.; Valenzuela, O.L.; Sanchez-Peña, L.C.; Styblo, M.; Fry, R.C. Evaluation of plasma arsenicals as potential biomarkers of exposure to inorganic arsenic. J. Expo. Sci. Environ. Epidemiol. 2019, 29, 718–729. [Google Scholar] [CrossRef]
- Moon, K.A.; Oberoi, S.; Barchowsky, A.; Chen, Y.; Guallar, E.; Nachman, K.E.; Navas-Acien, A. A dose-response meta-analysis of chronic arsenic exposure and incident cardiovascular disease. Int. J. Epidemiol. 2017, 46, 1924–1939. [Google Scholar] [CrossRef]
- Feseke, S.K.; St-Laurent, J.; Anassour-Sidi, E.; Ayotte, P.; Bouchard, M.; Levallois, P. Arsenic exposure and type 2 diabetes: Results from the 2007–2009 Canadian Health Measures Survey. Health Promot. Chronic Dis. Prev. Can. 2015, 35, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Wade, T.J.; Xia, Y.; Mumford, J.; Wu, K.; Le, X.C.; Sams, E.; E Sanders, W. Cardiovascular disease and arsenic exposure in Inner Mongolia, China: A case control study. Environ. Health 2015, 14, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farzan, S.F.; Chen, Y.; Rees, J.R.; Zens, M.S.; Karagas, M.R. Risk of death from cardiovascular disease associated with low-level arsenic exposure among long-term smokers in a US population-based study. Toxicol. Appl. Pharmacol. 2015, 287, 93–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Esquinas, E.; Pollán, M.; Umans, J.G.; Francesconi, K.A.; Goessler, W.; Guallar, E.; Howard, B.; Farley, J.; Best, L.G.; Navas-Acien, A. Arsenic Exposure and Cancer Mortality in a US-Based Prospective Cohort: The Strong Heart Study. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1944–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karagas, M.R.; Gossai, A.; Pierce, B.L.; Ahsan, H. Drinking Water Arsenic Contamination, Skin Lesions, and Malignancies: A Systematic Review of the Global Evidence. Curr. Environ. Health Rep. 2015, 2, 52–68. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Guo, Y.-L.L.; Su, H.-J.; Hsueh, Y.-M.; Smith, T.J.; Ryan, L.; Lee, M.-S.; Chao, S.-C.; Lee, J.Y.-Y.; Christiani, D.C. Arsenic Methylation and Skin Cancer Risk in Southwestern Taiwan. J. Occup. Environ. Med. 2003, 45, 241–248. [Google Scholar] [CrossRef]
- Sung, T.-C.; Huang, J.-W.; Guo, H.-R. Association between Arsenic Exposure and Diabetes: A Meta-Analysis. BioMed Res. Int. 2015, 2015, 368087. [Google Scholar] [CrossRef] [Green Version]
- Tofail, F.; Vahter, M.; Hamadani, J.D.; Nermell, B.; Huda, S.N.; Yunus, M.; Rahman, M.; Grantham-McGregor, S.M. Effect of Arsenic Exposure during Pregnancy on Infant Development at 7 Months in Rural Matlab, Bangladesh. Environ. Health Perspect. 2009, 117, 288–293. [Google Scholar] [CrossRef]
- Kahn, L.G.; Trasande, L. Environmental Toxicant Exposure and Hypertensive Disorders of Pregnancy: Recent Findings. Curr. Hypertens. Rep. 2018, 20, 87. [Google Scholar] [CrossRef]
- Navasumrit, P.; Chaisatra, K.; Promvijit, J.; Parnlob, V.; Waraprasit, S.; Chompoobut, C.; Binh, T.T.; Hai, D.N.; Bao, N.D.; Hai, N.K.; et al. Exposure to arsenic in utero is associated with various types of DNA damage and micronuclei in newborns: A birth cohort study. Environ. Health 2019, 18, 51. [Google Scholar] [CrossRef]
- Rudge, C.V.; Röllin, H.B.; Nogueira, C.M.; Thomassen, Y.; Rudge, M.C.; Odland, J.Ø. The placenta as a barrier for toxic and essential elements in paired maternal and cord blood samples of South African delivering women. J. Environ. Monit. 2009, 11, 1322–1330. [Google Scholar] [CrossRef] [Green Version]
- Hamadani, J.D.; Grantham-McGregor, S.M.; Tofail, F.; Nermell, B.; Fängström, B.; Huda, S.N.; Yesmin, S.; Rahman, M.; Vera-Hernández, M.; E Arifeen, S.; et al. Pre- and postnatal arsenic exposure and child development at 18 months of age: A cohort study in rural Bangladesh. Int. J. Epidemiol. 2010, 39, 1206–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert-Diamond, D.; Emond, J.A.; Baker, E.R.; Korrick, S.A.; Karagas, M.R. Relation between in Utero Arsenic Exposure and Birth Outcomes in a Cohort of Mothers and Their Newborns from New Hampshire. Environ. Health Perspect. 2016, 124, 1299–1307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchet, J.P.; Lauwerys, R.; Roels, H. Urinary excretion of inorganic arsenic and its metabolites after repeated ingestion of sodium metaarsenite by volunteers. Int. Arch. Occup. Environ. Health 1981, 48, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.F. Biomarkers of Exposure: A Case Study with Inorganic Arsenic. Environ. Health Perspect. 2006, 114, 1790–1796. [Google Scholar] [CrossRef] [Green Version]
- Carignan, C.C.; Cottingham, K.L.; Jackson, B.P.; Farzan, S.F.; Gandolfi, A.J.; Punshon, T.; Folt, C.L.; Karagas, M.R. Estimated Exposure to Arsenic in Breastfed and Formula-Fed Infants in a United States Cohort. Environ. Health Perspect. 2015, 123, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Samanta, G.; Das, D.; Mandal, B.K.; Chowdhury, T.R.; Chakraborti, D.; Pal, A.; Ahamed, S. Arsenic in the breast milk of lactating women in arsenic-affected areas of West Bengal, India and its effect on infants. J. Environ. Sci. Health Part A 2007, 42, 1815–1825. [Google Scholar] [CrossRef]
- Gürbay, A.; Charehsaz, M.; Eken, A.; Sayal, A.; Girgin, G.; Yurdakök, M.; Yiğit, S.; Erol, D.D.; Şahin, G.; Aydın, A. Toxic Metals in Breast Milk Samples from Ankara, Turkey: Assessment of Lead, Cadmium, Nickel, and Arsenic Levels. Biol. Trace Elem. Res. 2012, 149, 117–122. [Google Scholar] [CrossRef]
- Fängström, B.; Moore, S.; Nermell, B.; Kuenstl, L.; Goessler, W.; Grandér, M.; Kabir, I.; Palm, B.; El Arifeen, S.; Vahter, M. Breast-feeding Protects against Arsenic Exposure in Bangladeshi Infants. Environ. Health Perspect. 2008, 116, 963–969. [Google Scholar] [CrossRef] [Green Version]
- Chao, H.-H.; Guo, C.-H.; Huang, C.-B.; Chen, P.-C.; Li, H.-C.; Hsiung, D.-Y.; Chou, Y.-K. Arsenic, Cadmium, Lead, and Aluminium Concentrations in Human Milk at Early Stages of Lactation. Pediatr. Neonatol. 2014, 55, 127–134. [Google Scholar] [CrossRef]
- Milton, A.H.; Hussain, S.; Akter, S.; Rahman, M.; Mouly, T.A.; Mitchell, K. A Review of the Effects of Chronic Arsenic Exposure on Adverse Pregnancy Outcomes. Int. J. Environ. Res. Public Health 2017, 14, 556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelmann, E.R.; Gurzau, E.; Gurzau, A.; Goessler, W.; Kunrath, J.; Yeckel, C.W.; McCarty, K.M. A pilot study: The importance of inter-individual differences in inorganic arsenic metabolism for birth weight outcome. Environ. Toxicol. Pharmacol. 2013, 36, 1266–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, W.-C.; Chung, Y.-T.; Chen, H.-Y.; Wang, C.-J.; Ying, T.-H.; Chuang, C.-Y.; Tseng, Y.-C.; Wang, S.-L. Maternal Arsenic Exposure and DNA Damage Biomarkers, and the Associations with Birth Outcomes in a General Population from Taiwan. PLoS ONE 2014, 9, e86398. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Region | Total No. | No. with Detectable Arsenic in Breast Milk (%) | Mean (µg/L) | Range (µg/L) |
|---|---|---|---|---|
| Non-Exposed | 39 | 5 (13) | 5.3 | ND 1–7.3 |
| Exposed | 75 | 25 (33) 2 | 8.5 | ND–26.0 |
| Medium | N | Mean | SD | Range |
|---|---|---|---|---|
| Exposed Region | ||||
| Placenta | 83 | 7.80 µg/kg * | 6.30 | 0.3–33 |
| Blood | 80 | 4.96 µg/L | 2.90 | ND–12.4 |
| Urine | 79 | 54.92 µg/L ** | 39.07 | 4.1–190 |
| Urine-Cr | 80 | 77.04 µg/g-Cr ** | 56.03 | 15.3–306.5 |
| Breast Milk | 75 | 4.30 µg/L * | 10.50 | ND–24.7 |
| Non-Exposed Region | ||||
| Placenta | 13 | 2.17 µg/kg | 2.57 | 0.1–8.8 |
| Blood | 14 | 3.85 µg/L | 2.64 | ND–9.7 |
| Urine | 13 | 4.60 µg/L | 3.09 | 0.8–9.4 |
| Urine-Cr | 13 | 6.71 µg/g-Cr | 5.73 | 0.7–18.4 |
| Breast Milk | 13 | 0.87 µg/L | 1.71 | ND–7.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García Salcedo, J.J.; Roh, T.; Nava Rivera, L.E.; Betancourt Martínez, N.D.; Carranza Rosales, P.; San Miguel Salazar, M.F.; Rivera Guillén, M.A.; Serrano Gallardo, L.B.; Niño Castañeda, M.S.; Guzmán Delgado, N.E.; et al. Comparative Biomonitoring of Arsenic Exposure in Mothers and Their Neonates in Comarca Lagunera, Mexico. Int. J. Environ. Res. Public Health 2022, 19, 16232. https://doi.org/10.3390/ijerph192316232
García Salcedo JJ, Roh T, Nava Rivera LE, Betancourt Martínez ND, Carranza Rosales P, San Miguel Salazar MF, Rivera Guillén MA, Serrano Gallardo LB, Niño Castañeda MS, Guzmán Delgado NE, et al. Comparative Biomonitoring of Arsenic Exposure in Mothers and Their Neonates in Comarca Lagunera, Mexico. International Journal of Environmental Research and Public Health. 2022; 19(23):16232. https://doi.org/10.3390/ijerph192316232
Chicago/Turabian StyleGarcía Salcedo, José Javier, Taehyun Roh, Lydia Enith Nava Rivera, Nadia Denys Betancourt Martínez, Pilar Carranza Rosales, María Francisco San Miguel Salazar, Mario Alberto Rivera Guillén, Luis Benjamín Serrano Gallardo, María Soñadora Niño Castañeda, Nacny Elena Guzmán Delgado, and et al. 2022. "Comparative Biomonitoring of Arsenic Exposure in Mothers and Their Neonates in Comarca Lagunera, Mexico" International Journal of Environmental Research and Public Health 19, no. 23: 16232. https://doi.org/10.3390/ijerph192316232
APA StyleGarcía Salcedo, J. J., Roh, T., Nava Rivera, L. E., Betancourt Martínez, N. D., Carranza Rosales, P., San Miguel Salazar, M. F., Rivera Guillén, M. A., Serrano Gallardo, L. B., Niño Castañeda, M. S., Guzmán Delgado, N. E., Millán Orozco, J., Ortega Morales, N., & Morán Martínez, J. (2022). Comparative Biomonitoring of Arsenic Exposure in Mothers and Their Neonates in Comarca Lagunera, Mexico. International Journal of Environmental Research and Public Health, 19(23), 16232. https://doi.org/10.3390/ijerph192316232