
Co-Design of an Educational Resource with Female Partners of Male Stroke Survivors to Support Physical Activity Participation


{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
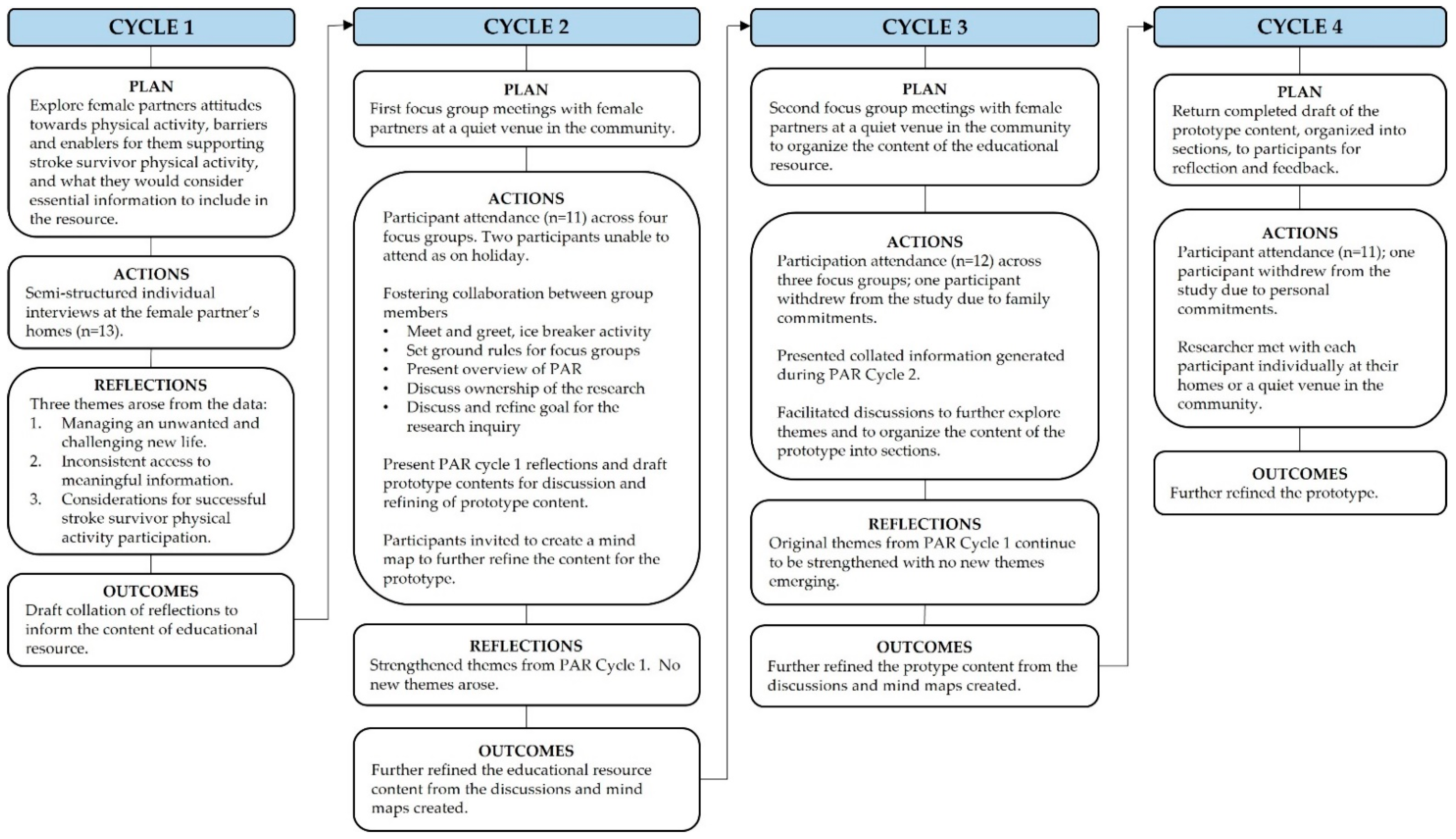
2.1. Study Design
2.2. Research Team and Reflexivity
2.3. Recruitment and Participants
2.4. Data Collection Procedures and Data Analysis
2.5. Ethics
3. Results
3.1. Theme 1: Managing an Unwanted and Challenging “New Life”
I’m trying to be all things. I’m not just being the housekeeper, housewife, I’m being the plumber, the painter, the lawn mower, the vege gardener, the taxi driver. The extra world is so demanding, unrelenting….it’s like running a train station. I was totally unprepared for it, and it was unrelenting, you never get a day off, you just can’t get out of it. You are absolutely out on your own….and you have got all the stress of this person…you are alone. (Participant 7, Individual Interview).
Sometimes I feel guilty, like I’ve just started going to dance group again. It’s on a Monday night after work but I feel really bad because [husband] has been at home all day by himself. He wants me to do it and I do it, but I wish I could feel just that freedom…like in the past when he went to golf, and I went and did whatever [I wanted]. (Participant 2, Focus Group A-4).
3.2. Theme 2: Inconsistent Access to Meaningful Information
We get mixed messages. People [health professionals] say, “Oh you must walk more” and then yesterday the physio came, and she said, “Don’t overdo it.” (Participant 13, Individual Interview).
Focus Group B-2 discussion
Participant 3: You’ve got to ask questions and keep asking questions if you don’t know.
Participant 8: But there’s no one really to ask. They [medical team] never took me to a room, it was just told to me [about his stroke] in the hallway, amongst all these other people. I actually got more information from getting a few books. That was the best thing.
3.3. Theme 3: Considerations for Successful PA Participation for Stroke Survivors
[The physiotherapist] gave us a lovely list of exercises and realistically I think he [stroke survivor] did them twice. It’s about your home life and achieving it all. I knew what would click with his psyche and his determination factor. It was a mission [stroke survivor feeding his cattle] but it took him from walking to walking properly, because out in the paddock he had to learn to balance when he was putting this electric fence standard in, and he was walking on uneven ground. I also thought that his social aspect of life was very important to him, so it was a matter for both physical and socially integrating him…being part of people within and around him was very beneficial for his well-being. (Participant 4, Individual Interview).
One of the other challenges is [husband’s] tiredness. So you can’t force him out of bed if he can’t cope. You’ve got to take that into account how they’re feeling because if he just says he’s too tired, well…you have to go with it. (Participant 6, Individual Interview).
He [husband] had just started walking out in the garden and getting out of the wheelchair. It had snowed and I had to go back to work. I said, “Whatever you do there is going to be more snow so don’t go outside, stay inside, don’t go outside.” He decided to go and look at the trees and plants [while I was out] and I drove up the drive and there he was stuck by the clothesline, and I don’t know how long he had been there for, and he wasn’t that well-dressed. His planning wasn’t good. Yeah, I get worried. (Participant 8, Individual Interview).
Focus Group B-2 discussion
Participant 11: Like [Participant 9], every time she takes her husband out [into the community], she goes there first and checks out the access.
Participant 4: We had a prime example of that on Thursday night where I didn’t [check accessibility prior] and some friends took us for a drink at [restaurant]….and it was so unsuitable for my partner….there was a lack of chairs and cobbled concrete to get in. The stools were all the wrong height….you know I should have gone to have a look.
Participant 8: You would have been on edge the whole time I bet.
When he starts snapping, “You haven’t had a stroke.” I think I have to back off a wee bit. I just have to take that on the cheek if he’s going to say that to me. I have to let it go over my head. But if he says he’s not going to do it he won’t do it. End of story. There’s nothing else I can do. I’ve done lots of things. I’ve said, “Look if you walk every day, just around the block, we’ll go out to lunch. So, I used to give him incentives to do it…but there is a fine line. (Participant 12, Individual Interview).
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Donnell, M.; Chin, S.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Reeves, M.; Bushnell, C.; Howard, G.; Gargano, J.; Duncan, P.; Lynch, G.; Khatiwoda, A.; Lisabeth, L. Sex differences in stroke: Epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol. 2008, 7, 915–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billinger, S.; Arena, R.; Bernhardt, J.; Eng, J.; Franklin, B.; Johnson, M.; MacKay-Lyons, M.; Macko, R.; Mead, G.; Roth, E.; et al. Physical activity and exercise recommendations for stroke survivors: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2532–2553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prior, P.; Suskin, N. Exercise for stroke prevention. Stroke Vasc. Neurol. 2018, 3, 59–68. [Google Scholar] [CrossRef]
- Rimmer, J.; Chen, M.; Hsieh, K. A conceptual model for identifying, preventing, and managing secondary conditions in people with disabilities. Phys. Ther. 2011, 91, 1728–1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sims-Gould, J.; Ahn, R.; Li, N.; Ottone, C.; Mackey, D.; McKay, H. “The social side is as important as the physical side”: Older men’s experiences of physical activity. Am. J. Mens Health 2018, 12, 2173–2182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtenay, W. Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Soc. Sci. Med. 2000, 50, 1385–1401. [Google Scholar] [CrossRef]
- Courtenay, W. Engendering health: A social constructionist examination of men’s beliefs and behaviours. Psychol. Men Masc. 2000, 1, 4–15. [Google Scholar] [CrossRef]
- Robertson, S. ‘Not living life in too much excess’: Lay men understand health and well-being. Health Interdiscip. J. Soc. Study Health Illn. Med. 2006, 10, 175–189. [Google Scholar] [CrossRef] [Green Version]
- Smith, B. Disability, sport and men’s narratives of health: A qualitative study. Health Psychol. 2013, 32, 110–119. [Google Scholar] [CrossRef]
- Ragonese, C.; Shand, T.; Barker, G. Masculine Norms and Men’s Health: Making the Connections; Promundo-US: Washington, DC, USA, 2019. [Google Scholar]
- Winstein, C.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.; Cramer, S.; Deruyter, F.; Eng, J.; Fisher, B.; Harvey, R.; et al. Guidelines for adult stroke rehabilitation and recovery. A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e2–e72. [Google Scholar] [CrossRef]
- Morris, J.; Oliver, T.; Kroll, T.; MacGillivray, S. The importance of psychological and social factors in influencing the uptake and maintenance of physical activity after stroke: A structured review of the empirical literature. Stroke Res. Treat. 2012, 2012, 195249. [Google Scholar] [CrossRef] [PubMed]
- Damush, T.; Plue, L.; Bakas, T.; Schmid, A.; Williams, L. Barriers and facilitators to exercise among stroke survivors. Rehabil. Nurs. 2007, 32, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Hebblethwaite, S.; Curley, L. Exploring the role of community recreation in stroke recovery using participatory action research and photovoice. Ther. Recreat. J. 2015, 49, 1–17. [Google Scholar]
- Nicholson, S.; Donaghy, M.; Johnston, M.; Sniehotta, F.; van Wijck, F.; Johnston, D.; Greig, C.; McMurdo, M.; Mead, G. A qualitative theory guided analysis of stroke survivors’ perceived barriers and facilitators to physical activity. Disabil. Rehabil. 2014, 36, 1857–1868. [Google Scholar] [CrossRef]
- Outermans, J.; Pool, J.; van de Port, I.; Bakers, J.; Wittink, H. What’s keeping people after stroke from walking outdoors to become physically active? A qualitative study, using an integrated biomedical and behavioural theory of functioning and disability. BMC Neurol. 2016, 16, 137. [Google Scholar] [CrossRef] [Green Version]
- Tornbom, K.; Sunnerhagen, K.; Danielsson, A. Perceptions of physical activity and walking in an early stage after stroke or acquired brain injury. PLoS ONE 2017, 12, e0173463. [Google Scholar] [CrossRef] [Green Version]
- Lawerence, M.; Kerr, S.; Watson, H.; Paton, G.; Ellis, G. An exploration of lifestyle beliefs and lifestyle behaviour following stroke: Findings from a focus group study of patients and family members. BMC Fam. Pract. 2010, 11, 97. [Google Scholar] [CrossRef] [Green Version]
- Anderson, S.; Keating, N.; Wilson, D. Reconciling marriage and care after stroke. Can. J. Aging 2017, 36, 386–401. [Google Scholar] [CrossRef] [Green Version]
- Cameron, J.; Gignac, M. “Timing it right”: A conceptual framework for addressing the support needs of family caregivers to stroke survivors from the hospital to the home. Patient Educ. Couns. 2008, 70, 305–314. [Google Scholar] [CrossRef]
- Ekstam, L.; Johansson, U.; Guidetti, S.; Eriksson, G.; Ytterberg, C. The combined perceptions of people with stroke and their carers regarding rehabilitation needs 1 year after stroke: A mixed methods study. BMJ Open 2015, 5, e006784. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.; Glandon, G.; Elliott, T.; Giger, J.; Weaver, M. Problems and associated feelings experienced by family caregivers of stroke survivors the second and third month post discharge. Top. Stroke Rehabil. 2006, 13, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Hafsteinsdottir, T.; Vergunst, M.; Lindeman, E.; Schuurmans, M. Educational needs of patients with a stroke and their caregivers: A systematic review of the literature. Patient Educ. Couns. 2011, 85, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Larson, J.; Franzen-Dahlin, A.; Billing, E.; von Arbin, M.; Murray, V.; Wredling, R. The impact of gender regarding psychological well-being and general life situation among spouses of stroke patients during the first year after the patients’ stroke event: A longitudinal study. Int. J. Nurs. Stud. 2008, 45, 257–265. [Google Scholar] [CrossRef]
- Lou, S.; Carstensen, K.; Jorgensen, C.; Nielsen, C. Stroke patients’ and informal carers’ experiences with life after stroke: An overview of qualitative systematic reviews. Disabil. Rehabil. 2017, 39, 301–313. [Google Scholar] [CrossRef]
- Quinn, K.; Murray, C.; Malone, C. Spousal experiences of coping with and adapting to caregiving for a partner who has a stroke: A meta-synthesis of qualitative research. Disabil. Rehabil. 2014, 36, 185–198. [Google Scholar] [CrossRef]
- Saban, K.; Hogan, N. Female caregivers of stroke survivors: Coping and adapting to a life that once was. J. Neurosci. Nurs. 2012, 44, 2–14. [Google Scholar] [CrossRef]
- Satink, T.; Cup, E.; de Swart, B.; Nijhuis-van der Sanden, M. The perspectives of spouses of stroke survivors on self-management—A focus group study. Disabil. Rehabil. 2018, 40, 176–184. [Google Scholar] [CrossRef]
- Ytterberg, C.; von Koch, L.; Erikson, A. Abandoned to the strains of daily life: A qualitative study of the long-term experiences in partners to persons after a mild to moderate stroke. Disabil. Rehabil. 2017, 41, 649–655. [Google Scholar] [CrossRef]
- Zhang, J.; Lee, D. Meaning in stroke family caregiving: A literature review. Geriatr. Nurs. 2017, 38, 48–56. [Google Scholar] [CrossRef]
- Morris, J.; Williams, B. Optimising long-term participation in physical activities after stroke: Exploring new ways of working for physiotherapists. Physiotherapy 2009, 95, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Hammel, J.; Jones, R.; Gossett, A.; Morgan, E. Examining Barriers and Supports to Community Living and Participation after a Stroke from a Participatory Action Research Approach. Available online: http://find.galegroup.com/gtx/printdoc.do?contentSet=IAC-Documents&docType=IA (accessed on 15 April 2019).
- Backstrom, B.; Asplund, K.; Sundin, K. The meaning of middle-aged female spouses’ lived experience of the relationship with a partner who has suffered a stroke, during the first year post discharge. Nurs. Inq. 2010, 17, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Ellis-Hill, C.; Robison, J.; Wiles, R.; McPherson, K.; Hyndman, D.; Ashburn, A. Going home to get on with life: Patients and carers experiences of being discharged from hospital following stroke. Disabil. Rehabil. 2009, 31, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Green, T.; King, K. Experiences of male patients and wife-caregivers in the first year post-discharge following minor stroke: A descriptive qualitative study. Int. J. Nurs. Stud. 2009, 46, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, N.; MacKenzie, A. Informal caring for stroke survivors: Meta-ethnographic review of qualitative literature. Maturitas 2010, 66, 268–276. [Google Scholar] [CrossRef] [PubMed]
- White, C.; Korner-Bitensky, N.; Rodrigue, N.; Rosmus, C.; Sourial, R.; Lambert, S.; Wood-Dauphine, S. Barriers and facilitators to caring for individuals with stroke in the community: The family’s experience. Can. J. Neurosci. Nurs. 2007, 29, 5–12. [Google Scholar]
- Allison, R.; Evans, P.; Kilbride, C.; Campbell, J. Secondary prevention of stroke: Using the experiences of patients and carers to inform the development of an educational resource. Fam. Pract. 2008, 25, 355–361. [Google Scholar] [CrossRef] [Green Version]
- Eames, S.; Hoffman, T.; Worrall, L.; Read, S. Stroke patients’ and carers’ perception of barriers to accessing stroke information. Top. Stroke Rehabil. 2010, 17, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Gosman-Hedstrom, G.; Dahlin-Ivanoff, S. Mastering an unpredictable everyday life after stroke—Older women’s experiences of caring and living with their partners. Scand. J. Caring Sci. 2012, 26, 587–597. [Google Scholar] [CrossRef]
- Chen, L.; Dongxia, L.; Chamberlain, D.; Newman, P. Enablers and barriers in hospital-to-home transitional care for stroke survivors and caregivers: A systematic review. J. Clin. Nurs. 2021, 30, 2786–2807. [Google Scholar] [CrossRef]
- Eames, S.; Hoffman, T.; Worrall, L.; Read, S. Delivery styles and formats for different stroke information topics: Patient and carer preferences. Patient Educ. Couns. 2011, 84, e18–e23. [Google Scholar] [CrossRef] [PubMed]
- Plant, S.; Tyson, S.; Kirk, S.; Parsons, J. What are the barriers and facilitators to goal-setting during rehabilitation for stroke and other acquired brain injuries? A systematic review and meta-synthesis. Clin. Rehabil. 2016, 30, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Calder, A. Access to Physical Activity for Men Following Stroke. Ph.D. Thesis, University of Otago, Dunedin, New Zealand, 2019. [Google Scholar]
- Freeman, C.; Cassidy, B. Head Space: A Handbook on Brain Injury; New Zealand Spinal Trust: Christchurch, New Zealand, 2009. [Google Scholar]
- Stroke Foundation of New Zealand. Life after Stroke. A Guide for People with Stroke and Their Families, 2nd ed.; Stroke Foundation New Zealand: Wellington, New Zealand, 2013. [Google Scholar]
- Morris, J.; Oliver, T.; Kroll, T.; Joice, S.; Williams, B. From physical and functional to continuity with pre-stroke self and participation in valued activities: A qualitative exploration of stroke survivors’, carers’ and physiotherapists’ perceptions of physical activity after stroke. Disabil. Rehabil. 2014, 37, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Pearce, G.; Pinnock, H.; Epiphaniou, E.; Parke, H.; Heavey, E.; Griffiths, C.; Greenhalgh, T.; Sheikh, A.; Taylor, S. Experiences of self-management support following stroke. PLoS ONE 2015, 10, e0141803. [Google Scholar] [CrossRef]
- Rathnayake, S.; Moyle, W.; Jones, C.; Calleja, P. Co-design of an mHealth application for family caregivers of people with dementia to address functional disability care needs. Inform. Health Soc. Care 2021, 46, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Webber, R.; Partridge, R.; Grindell, C. The creative co-design of low back pain educational resources. Evid. Policy 2022, 18, 436–453. [Google Scholar] [CrossRef]
- Mountain, A.; Lindsay, M.; Teasell, R.; Salbach, N.; de Jong, A.; Foley, N.; Bhogal, S.; Bains, N.; Bowes, R.; Cheung, D.; et al. Canadian stroke best practice recommendations: Rehabilitation, recovery, and community participation following stroke. Part two: Transitions and community participation following stroke. Int. J. Stroke 2020, 15, 789–806. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.; Forster, A.; Young, J. Cochrane review: Information provision for stroke patients and their caregivers. Clin. Rehabil. 2009, 23, 195–206. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Jackson, C.; Shaw, S.; Janamian, T. Achieving research impact through co-creation in community-based health services: Literature review and case study. Milbank Q. 2016, 94, 392–429. [Google Scholar] [CrossRef] [Green Version]
- Marcus, B.; Selby, V.; Niaura, R.; Rossi, J. Self-efficacy and the stages of exercise behaviour change. Res. Q. Exerc. Sport 1992, 63, 60–66. [Google Scholar] [CrossRef]
- Thomas, D. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Stewart, D.; Shamdasani, P.; Rook, D. Focus Groups Theory and Practice, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Hoffman, T.; McKenna, K. Analysis of stroke patients’ and carers’ reading ability and the content and design of written materials: Recommendations for improving written stroke information. Patient Educ. Couns. 2006, 60, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Cao, V.; Chung, C.; Ferreira, A.; Nelken, J.; Brooks, D.; Cott, C. Changes in activities of wives caring for their husbands following stroke. Physiother. Can. 2010, 62, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visser-Meily, A.; Post, M.; Gorter, J.; Berlekom, S.; van den Bos, T.; Lindeman, E. Rehabilitation of stroke patients needs a family-centred approach. Disabil. Rehabil. 2006, 28, 1557–1561. [Google Scholar] [CrossRef] [PubMed]
- Creasy, K.; Lutz, B.; Young, M.; Stacciarini, J. Clinical implications of family-centered care in stroke rehabilitation. Rehabil. Nurs. 2015, 40, 349–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robison, J.; Wiles, R.; Ellis-Hill, C.; McPherson, K.; Hyndman, D.; Ashburn, A. Resuming previously valued activities post-stroke: Who or what helps? Disabil. Rehabil. 2009, 31, 1555–1566. [Google Scholar] [CrossRef] [PubMed]
- Krishman, S.; Pappadis, M.; Weller, S.; Stearnes, M.; Kumar, A.; Ottenbacher, K.; Reistetter, T. Needs of stroke survivors as perceived by their caregivers. Am. J. Phys. Med. Rehabil. 2017, 96, 487–505. [Google Scholar] [CrossRef]
- Northcott, S.; Moss, B.; Harrison, K.; Hilari, K. A systematic review of the impact of stroke on social support and social networks: Associated factors and patterns of change. Clin. Rehabil. 2015, 30, 811–831. [Google Scholar] [CrossRef]
- Teasel, R.; Hussein, N.; Viana, R.; Madady, M.; Donaldson, S.; McClure, A.; Richardson, M. Stroke Rehabilitation Clinician Handbook. Available online: www.ebrsr.com/clinician-handbook (accessed on 30 June 2019).
- Foster, A.; Armstrong, J.; Buckley, A.; Sherry, J.; Young, T.; Foliaki, S.; James-Hohaia, T.; Theadom, A.; McPherson, K. Encouraging family engagement in the rehabilitation process: A rehabilitation provider’s development of support strategies for family members of people with traumatic brain injury. Disabil. Rehabil. 2012, 34, 1855–1862. [Google Scholar] [CrossRef]
- Mulligan, H.; Wilkinson, A.; Lusty, A.; Delorme, A.; Bong, S. Consumers and health professionals’ perceptions of participatory action research in developing a health resource. N. Z. J. Physiother. 2015, 43, 93–97. [Google Scholar] [CrossRef]
- Kuluski, K.; Kokorelias, K.; Peckham, A.; Goldhar, J.; Petrie, J.; Alloway, C. Twelve principles to support caregiver engagement in health care systems and health research. Patient Exp. J. 2019, 6, 141–148. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calder, A.; Sole, G.; Mulligan, H. Co-Design of an Educational Resource with Female Partners of Male Stroke Survivors to Support Physical Activity Participation. Int. J. Environ. Res. Public Health 2022, 19, 16856. https://doi.org/10.3390/ijerph192416856
Calder A, Sole G, Mulligan H. Co-Design of an Educational Resource with Female Partners of Male Stroke Survivors to Support Physical Activity Participation. International Journal of Environmental Research and Public Health. 2022; 19(24):16856. https://doi.org/10.3390/ijerph192416856
Chicago/Turabian StyleCalder, Allyson, Gisela Sole, and Hilda Mulligan. 2022. "Co-Design of an Educational Resource with Female Partners of Male Stroke Survivors to Support Physical Activity Participation" International Journal of Environmental Research and Public Health 19, no. 24: 16856. https://doi.org/10.3390/ijerph192416856
APA StyleCalder, A., Sole, G., & Mulligan, H. (2022). Co-Design of an Educational Resource with Female Partners of Male Stroke Survivors to Support Physical Activity Participation. International Journal of Environmental Research and Public Health, 19(24), 16856. https://doi.org/10.3390/ijerph192416856